
Abstract
Background:
Hamstring injuries are common in sports involving rapid acceleration and directional changes. Despite extensive research, management remains primarily dependent on clinical judgment, owing to the absence of standardized, evidence-based protocols.
Purpose:
To compare the outcomes of operative versus nonoperative treatments, focusing on patient satisfaction, muscle strength, range of motion (ROM), activity level, and return to sport.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, the authors performed a systematic search of the PubMed, Google Scholar, Web of Science, and ScienceDigest databases from January 2000 to May 2024. Reported outcomes measured were muscle strength, ROM, functional activity, pain levels, return to preinjury activity levels, and patient satisfaction. Additionally, any complications related to the intervention were documented. The authors identified 13 eligible studies involving adults with acute hamstring injuries, including 526 patients. Eleven studies specifically investigated operative treatment, 1 examined nonoperative management, and 1 directly compared both approaches.
Result:
Surgical intervention was consistently associated with superior outcomes across multiple domains. Postoperatively, the Lower Extremity Functional Scale score often exceeded 74, and strength recovery commonly approached 90.0% of the contralateral limb. ROM was preserved after surgery but was not evaluated in nonoperative cohorts. Functional activity was generally higher after operative treatment (mean Tegner Activity Scale [TAS] scores: 4.7 ± 0.8, 6.0 ± 1.47, 5.1, and 8.5 ± 2.4; Marx Activity Rating Scale scores: 3.5 ± 4.3 and 4.4 ± 4.4), whereas nonoperative treatment showed a decline in TAS score (6.9 ± 1.7 to 6.1 ± 1.9; P = .030). Pain levels were low overall (visual analog scale score: 0.7 ± 0.9 to 4.0 ± 4.0). Complications were more frequent after surgery (4.2%-36.6%, including hematomas, neurapraxia, and superficial infections), although mostly minor. Nonoperative complications were limited to ecchymosis.
Conclusion:
This study demonstrated that operative treatment was associated with good functional recovery, muscle strength, and high return-to-sport rates. Complications rates within the operative group were mostly minor and not statistically significant when compared to nonoperative management, which yielded good outcomes in the limited available data. Further prospective studies using standardized outcome measures and clear subtype definitions are required to determine which patients benefit most from operative versus nonoperative management.
The hamstring muscle group, located on the posterior aspect of the thigh, comprises the semimembranosus, semitendinosus, and biceps femoris. They originate mainly from the ischial tuberosity, except the short head of the biceps femoris, which arises from the femur. Functionally, the hamstrings facilitate knee flexion and hip extension, with the biceps femoris contributing to external rotation, while the semimembranosus and semitendinosus support internal rotation. 24 Their biarticular characteristics make them susceptible to injuries, particularly the biceps femoris, due to its dual innervation. 26 Key risk factors for recurrence include a previous hamstring injury, advanced age, and elevated muscle torque. 34 Moreover, ethnicity and sport-specific factors, such as participation in high-level competition and engagement in sports that require frequent high-intensity accelerations, have been shown to increase injury susceptibility.13,14
Soft tissue injuries are classified into 3 grades based on clinical severity. Grade 1 involves minimal structural disruption with mild pain and tenderness, typically elicited only during activity. Grade 2 represents partial tissue disruption with moderate to severe pain and functional limitation, while grade 3 indicates complete rupture or avulsion with marked functional loss; paradoxically, pain may be absent due to tissue discontinuity. Although grading is primarily clinical, magnetic resonance imaging (MRI) and ultrasound are often used to confirm the diagnosis, particularly in grades 2 and 3. 20 This system is similarly applied to hamstring injuries. 16
Management is largely guided by clinical judgment, as no universally accepted evidence-based protocol exists. Grades 1 and 2 are generally treated nonoperatively with rest, ice, short-term nonsteroidal anti-inflammatory drugs, and structured rehabilitation. The use of platelet-rich plasma and other biological therapies remains controversial given limited supporting evidence and potential World Anti-Doping Agency restrictions related to insulin-like growth factor-1.4,11 Initial care emphasizes hemorrhage, edema, and pain control, followed by assisted ambulation and postural correction. 23
In contrast, grade 3 injuries often necessitate surgical intervention, particularly when tendon retraction exceeds 2.0 cm, as nonoperative approaches may result in persistent pain, weakness, and long-term functional deficits. Early surgical repair—ideally within 4 to 6 weeks—is recommended to reduce complications such as sciatic nerve scarring. 10 Adjunct modalities, including therapeutic ultrasound and shockwave therapy, have demonstrated limited or no significant clinical benefit in this context. 27
This systematic review evaluates and compares operative and nonoperative treatments for acute hamstring injuries by analyzing outcomes related to muscle strength, range of motion (ROM), functional activity, pain levels, return to preinjury activity, patient satisfaction, and treatment-related complications. We hypothesized that operative and nonoperative treatments for acute hamstring injuries would demonstrate differences in patient satisfaction, functional recovery (hamstring ROM, muscle strength, and functional activities), return to preinjury activity levels, and complication rates.
Methods
This systematic review was conducted from January 2000 to May 2024 in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 25 All stages of the review process followed the methodological framework outlined in the Cochrane Handbook for Systematic Reviews of Interventions. 17 The study protocol was prospectively registered in PROSPERO (International Prospective Register of Systematic Reviews) under the identification number CRD42024567841 (https://www.crd.york.ac.uk/PROSPERO/view/CRD42024567841).
Eligibility Criteria
Studies were included if they met the following criteria:
Included patients aged ≥18 years with acute hamstring muscle injuries, classified by anatomic location as ischial tuberosity avulsions, intramuscular tears, or musculotendinous junction injuries, treated either operatively or nonoperatively;
Reported treatment-related outcomes, including patient satisfaction, functional outcomes (hamstring ROM, muscle strength, and functional activity), and return to preinjury activity levels;
Included interventions initiated within 6 weeks of injury, with the acute nature of the injury clearly stated6,28;
Published in the English language;
Were a randomized controlled trial, observational study, or case series with a minimum of 10 patients.
Exclusion criteria were as follows: studies that did not report outcomes of interest; injuries classified as chronic (ie, treated >6 weeks after onset) or where acute versus chronic injury was not clearly distinguished; non–hamstring-specific injuries; and articles published in languages other than English or outside the specified time frame.
Search Strategy
A comprehensive literature search was conducted in the PubMed, Google Scholar, Web of Science, and ScienceDirect databases. The search strategy used Boolean operators and relevant keywords, including “Hamstring muscle injury,”“Operative treatment,” and “Conservative treatment” (Appendix 1).
The Rayyan web-based tool (www.rayyan.ai), which utilizes artificial intelligence for screening and deduplication, was used to manage the selection process. Each step was independently verified manually by 2 reviewers (D.O.S. and A.A.Alshammary) to ensure accuracy and minimize selection bias.
The initial search yielded 1205 articles. After duplicate removal via Rayyan and manual verification, 815 unique articles remained for screening. A 2-stage screening process was conducted: titles and abstracts were screened first, followed by full-text review. Discrepancies were resolved by a third reviewer (A.A.Alharbi) in a blinded manner. Studies that fulfilled the predefined inclusion criteria were selected for final analysis.
Data Extraction
Data were extracted from full-text articles and systematically recorded in a Microsoft Excel spreadsheet. Each study was analyzed across several domains.
Study characteristics included article title, author names, country of origin, study design, sample size, participant age, sex distribution, body mass index, inclusion criteria, and group categorization (if applicable).
Injury-related variables included anatomic site, operational definition of acute injury, intervention protocol, follow-up duration, and time from injury to surgery. Reported outcomes included muscle strength, ROM, pain, return to preinjury activity, patient satisfaction, and functional activity. Functional recovery was evaluated using validated instruments, including the Lysholm score, passive straight-leg raise (PSLR), modified Harris Hip Score (HHS), Marx Activity Rating Scale (MARS) score, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), straight-leg raise test score, limb symmetry index (LSI) for flexor strength, Lower Extremity Functional Scale (LEFS) score, Perth Hamstring Assessment Tool (PHAT) score, International Hip Outcome Tool-12 (iHOT-12) score, and Kerlan-Jobe Orthopaedic Clinic (KJOC) score. Functional activity after both operative and nonoperative treatments was assessed using the Short Form-12 (SF-12) score, Tegner Activity Scale (TAS) score, and MARS score. Pain levels were consistently assessed using the visual analog scale (VAS) score.
Complications related to the interventions were also recorded. All data were independently reviewed by 2 authors (R.H.A. and O.H.A.), and any discrepancies during data extraction were resolved by a third reviewer (S.D.A.) through blinded adjudication to ensure objectivity and minimize bias.
Quality Assessment
The methodological quality of the included studies was independently assessed by 2 reviewers (R.H.A. and D.O.S.), with a third reviewer (K.M.A.) performing a final evaluation (Figure 1) and resolving any discrepancies. For nonrandomized cohort studies, the Newcastle-Ottawa Scale was used, categorizing studies into predefined quality levels: high quality (7-9 stars), moderate quality (4-6 stars), and low quality (0-3 stars). 32 In case series, a validated checklist was applied to classify studies as high quality (8-10 “yes” responses), moderate quality (5-7 “yes” responses), and low quality (0-4 “yes” responses). 7
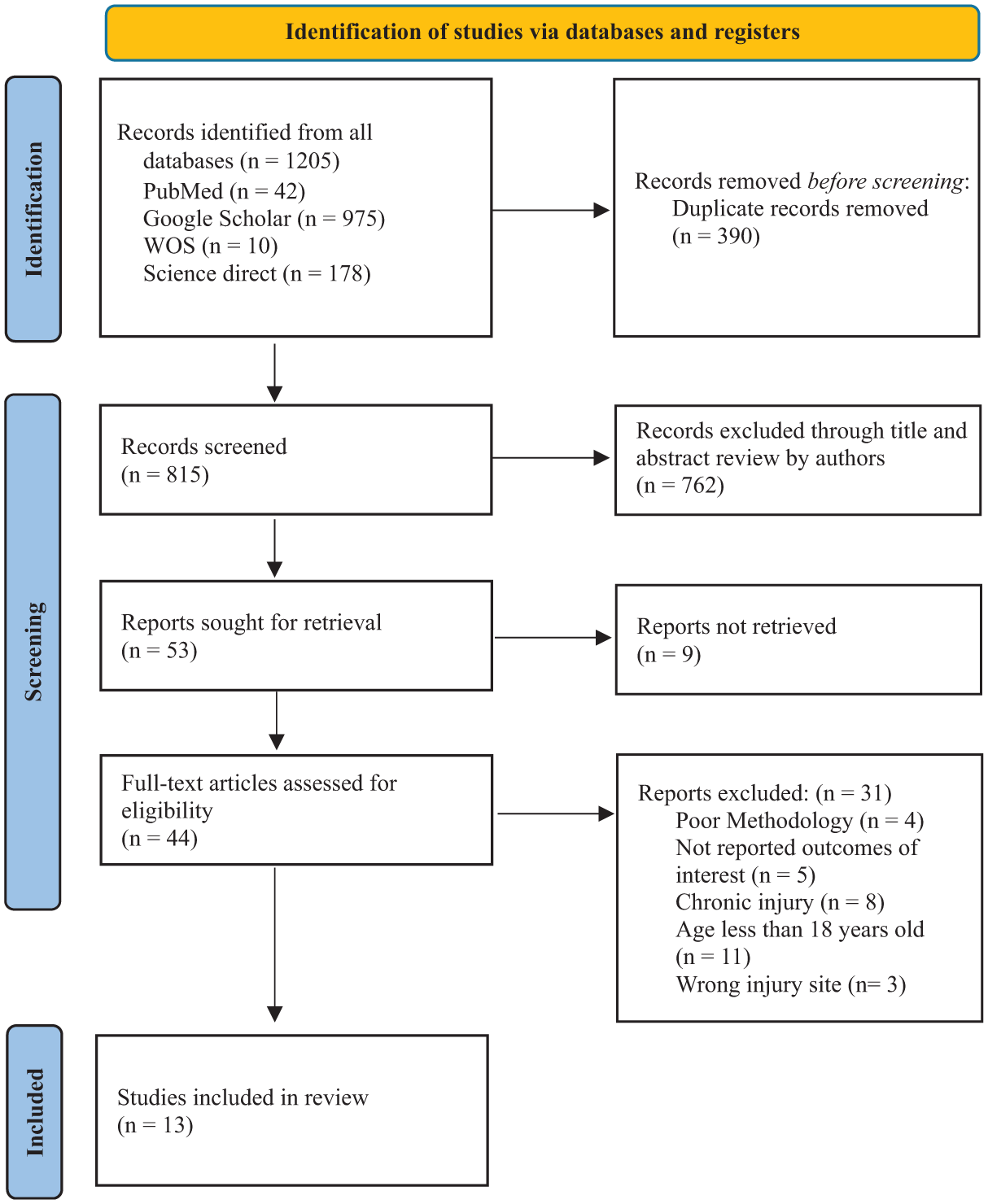
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of included articles. WOS, Web of Science.
Results
Characteristics of Included Studies
A total of 13 articles # were included, addressing various operative and nonoperative interventions for acute hamstring ruptures, whether partial or complete. A summary of study characteristics is provided in Table 1, while the baseline features are detailed in Table 2.
Summary Characteristics of Included Studies a

BAMIC, British Athletics Muscle Injury Classification; BMI, body mass index; HHS, Harris Hip Score; iHOT-12, International Hip Outcome Tool-12; KJOC, Kerlan-Jobe Orthopaedic Clinic; LEFS, Lower Extremity Functional Scale; LSI, limb symmetry index; MARS, Marx Activity Rating Scale; MTJ-BFlh, musculotendinous junction of the long head of the biceps femoris; MRI, magnetic resonance imaging; NFL, National Football League; PHAI, proximal hamstring tendon avulsion injury; PHAT, Perth Hamstring Assessment Tool; PSLR, passive straight-leg raise; PHCI, proximal hamstring complex injury; PHTR, proximal hamstring free tendon rupture; RTP, return to play; RTS, return to sport; RTW, return to work; SF-12, Short Form-12; SANE, Single Assessment Numeric Evaluation; TAS, Tegner Activity Scale; UCLA, University of California, Los Angeles; VAS, visual analog scale; WC, workers’ compensation; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; wk, weeks; mo, months; y, years.
Baseline Features of the Included Studies a

BMI, body mass index; MTJ-BFlh, musculotendinous junction of the long head of the biceps femoris; NR, not reported; PHCI, proximal hamstring complex injury; ROM, range of motion; SM, semimembranosus; ST, semitendinosus.
Presented as mean ± SD or median (range).
Presented as mean ± SD or mean (range) unless otherwise indicated.
Results Synthesis
Within the included studies, 11 investigated surgical repairs, ** 1 focused exclusively on nonoperative management, 12 and 1 study compared both surgical and nonoperative treatments 30 (Table 3).
Outcomes of the Included Studies a

ADL, activities of daily living; BMI, body mass index; HHS, Harris Hip Score; iHOT-12, International Hip Outcome Tool-12; KJOC, Kerlan-Jobe Orthopaedic Clinic; LEFS, Lower Extremity Functional Scale; LSI, limb symmetry index; MARS, Marx Activity Rating Scale; MTJ-BFlh, musculotendinous junction of the long head of the biceps femoris; NR, not reported; NS, not significant; PHAT, Perth Hamstring Assessment Tool; PSLR, passive straight-leg raise; ROM, range of motion; RTS, return to sport; SF-12, Short Form-12; SANE, Single Assessment Numeric Evaluation; TAS, Tegner Activity Scale; UCLA, University of California, Los Angeles; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Functional Recovery
Operative Treatment
Across the included studies, 458 patients were analyzed. One study reported a mean postoperative LEFS score of 74.9 ± 7.8 (range, 59-80) and HHS of 90.7 ± 13.9 (range, 67-100). 8 Another study reported a mean Lysholm score of 90.2 ± 3.4, a mean WOMAC score of 96.3 ± 2.4, and a mean University of California, Los Angeles (UCLA) activity score of 8.1 ± 0.9. 29 The iHOT-12 (mean, 99) and KJOC (mean, 77) scores were also reported, with 78.0% of patients demonstrating good or excellent outcomes. 5 Additional reports described a mean Lysholm score of 85.7 ± 18.3 and a mean modified HHS of 91.0 ± 12.6. 33 Functional recovery over time was assessed using the PSLR, MARS score, and LEFS score, all of which showed significant improvement by the 3-month follow-up. 1 At 2 years, 30.0% of patients achieved LEFS scores of 80.0, and 45.0% had MARS scores of 75.0. 1 Among 64 surgically treated musculotendinous junction injuries of the long head of the biceps femoris, LEFS and MARS scores improved significantly at 3 months, 1 year, and 2 years. 2 LEFS scores of 80.3 ± 20.2 and 94.3 ± 10.1 were observed in 2 postoperative groups. 19 The median EQ-5D-5L score was 0.94 (0.83-1.00), with an LEFS score of 88.8 (range, 61.6-100.0), PHAT score of 78.8 (range, 54.6-99.8), and LSI score of 95.6% (range, 71.7%-135.6%). 9
Nonoperative Treatment
Only 1 study assessed nonoperative management for unilateral proximal hamstring rupture, including 16 patients. It reported a mean LEFS score of 76.6 ± 3.9 and a UCLA activity score of 37.5 ± 2.2. 12
Operative Versus Nonoperative Treatment
In the study by Shambaugh et al, 30 comparisons between the operative group (n = 14) and the nonoperative group (n = 11) demonstrated higher mean LEFS scores in the operative group (74.71 ± 5.38 vs 68.50 ± 7.92). Additionally, the mean single-leg hop distance was significantly greater in the operative group (119.1 ± 27.7 cm) than in the nonoperative group (56.1 ± 31.2 cm). 30
Muscle Strength
Operative Treatment
In 1 study, a mean postoperative hamstring strength recovery of 78.0% ± 6.1% (range, 74.0%-88.0%) was observed compared with the contralateral side. 8 In another study, strength restoration >90.0% was observed at the 1-year follow-up, 1 with significant improvement from preoperative to postoperative levels confirmed. 2 Mean muscle strength values of 80.6 ± 20.1 and 91.8 ± 10.6 were reported in 2 operative cohorts. 19 In the study by Chocholáč et al, 9 the median maximum flexor strength was 0.82 Nm/kg (range, 0.33-1.42 Nm/kg) on the operated side compared with 0.72 Nm/kg (range, 0.41-1.89 Nm/kg) on the contralateral side (P = .807), with a median LSI of 95.6% (range, 71.7%-135.6%).
Nonoperative Treatment
In 1 study, a concentric strength deficit of 40% ± 25.0% was observed at 4 months, decreasing to 25.0% ± 12% at 2 years. 12 However, the eccentric strength deficit persisted over time.
Operative Versus Nonoperative Treatment
In the study by Shambaugh et al, 30 the mean perceived strength was 86.07% ± 12.12% in the operative group compared with 83.64% ± 14.16% in the nonoperative group. 30 The mean isokinetic strength in the operative group was 90.87% ± 16.3%. In contrast, isometric testing in the nonoperative group revealed marked weakness at 45° (57.54% ± 7.8%) and 90° (67.73% ± 18.8%) of flexion compared to the uninjured side. 30 The mean follow-up duration was 3.56 ± 2.11 years for the operative group and 2.48 ± 3.66 years for the nonoperative group. 30
Range of Motion
No studies assessed the ROM after nonoperative treatment; however, 4 studies evaluated ROM after surgery. Biarticular and monoarticular hip flexibility showed mean values of 86.6°± 8.6° and 127.8°± 12°, respectively, in the work of Sandmann et al. 29 In the study by Chocholáč et al, 9 median passive hip flexion with the knee bent was 120° (range, 115°-140°) on the operated side and 120° (115°-150°) on the contralateral side (P = .581). With the knee straight, median passive hip flexion was 90° (range, 60°-120°) on the operated side and 90° (70°-110°) on the contralateral side (P > .999). 9
Functional Activities
Operative Treatment
Postoperative TAS scores were reported as 4.7 ± 0.8, 29 6.0 ± 1.47, 33 and 5.1. 5 Higher mean TAS scores of 8.5 ± 2.4 21 and 8.5 ± 2.4 19 were also documented in other studies.
Nonoperative Treatment
A significant decline in TAS score from 6.9 ± 1.7 to 6.1 ± 1.9 was observed after nonoperative treatment (P = .030). 12
Operative Versus Nonoperative Treatment
No significant differences were found between groups in SF-12 mental and physical component scores, indicating comparable functional outcomes. 30
Patient Satisfaction
Operative Treatment
All patients were reported to be extremely satisfied postoperatively. 8 High satisfaction scores of 93.1 ± 13.1 and 96.7 ± 5.3 were documented in 1 study. 19 Median satisfaction rates were 94.0%, 5 95.0%, 1 and 100.0%. 9 Although 2 patients were unsatisfied at the 1-year follow-up in the study by Ayuob et al, 2 satisfaction improved at 2 years, with 81.2% reporting “very satisfied” and 18.8% reporting “satisfied.”
Nonoperative Treatment
Fifteen of 16 patients were either very satisfied or satisfied, with high subjective outcome scores. 12
Return to Preinjury Activity Levels
Operative Treatment
Chahal et al 8 found a mean Single Assessment Numeric Evaluation score of 93.6% ± 7.5% (range, 75.0%-100.0%), although only 16 of 27 (59.3%) patients fully returned to preinjury activity. In 1 study, 90.0% (9/10) resumed play despite full strength recovery in all cases. 22 A return-to-sport (RTS) rates of 98.7% (77 patients) was reported in another study, 31 and 14 of 15 patients resumed their preinjury level in the study by Sandmann et al. 29 In their work, Willinger et al 33 found that RTS outcomes varied, with 50.0% returning to the same level, 41.7% returning to a reduced level, and 8.3% ceasing participation in sport. Bowman et al 5 reported an RTS rate of 88.0% at a mean of 7.6 months, with 72.0% (42/58) resuming at their prior level. In their work, Ayuob et al1,2 observed RTS rates of 95.0% (19/20) at a mean of 11.9 ± 5.7 weeks and 100.0% at a mean of 13.4 ± 5.1 weeks. In the study by Lefèvre et al, 21 63 (98.4%) patients returned to sport, with 78.1% maintaining and 18.8% reducing their performance level.
Operative Versus Nonoperative Treatment
All surgically treated patients returned to their preinjury activities, compared with 8 of 11 in the nonoperative group. 30
Pain Levels
Among the 7 articles that addressed pain levels, the lowest mean VAS score was 0.7 ± 0.9, 29 whereas the highest was 4.0 ± 4.0 after surgical intervention. 19
Adverse Effects or Complications
Operative Treatment
In 1 study, 6 cases of postoperative stiffness and 1 case of numbness/tingling were reported. 8 In the study by Subbu et al, 31 6 complications were noted, including 4 superficial infections and 2 neural symptoms. In another study, 3 (4.2%) complications and sitting discomfort in 36.6% of patients were documented. 33 A 15.0% complication rate was reported by Bowman et al, 5 including 1 major complication (wound dehiscence) and 8 minor complications. In the work by Ayuob et al, 1 4 (20.0%) patients developed hematomas, and 1 had a superficial infection. The same group also observed 12 hematomas, 3 recurrences, and 4 cases of neurapraxia. 2 Two additional postoperative complications were reported in the work of Chocholáč et al. 9
Nonoperative Treatment
Ecchymosis was observed in 14 patients managed nonoperatively. 12
Operative Versus Nonoperative Treatment
In the study by Shambaugh et al, 30 2 patients in the operative group developed postoperative complications. One patient experienced a hematoma, which required a reoperation, while the other patient developed incisional numbness, which resolved within 3 months after surgery. 30
Risk of Bias
Cohort Studies
Quality assessment indicated that 2 studies19,30 were of overall good quality. The study by Johnson et al 19 achieved the highest score (7/9), reflecting a strong methodology across the selection, comparability, and outcome domains. The study by Shambaugh et al 30 scored 6 of 9, with adequate performance in selection and outcome assessment, but limited comparability (Table 4).
NOS Quality Assessment Results a

NOS, Newcastle-Ottawa Scale.
Case Series Studies
Eleven case series were assessed using a 9-item standardized checklist. Nine studies1,2,5,8,9,12,21,31,33 each scored 7 of 9, demonstrating strong reporting across inclusion criteria, valid measurements, and follow-up data. One study 29 scored 6 of 9, with limitations in inclusion clarity and site data. The study by Mansour et al 22 had the lowest score (5/9), showing deficiencies in inclusion criteria and demographic reporting (Table 5).
Case Series Checklist Quality Assessment Results

Discussion
The major findings of our study demonstrated that proximal hamstring avulsions are significant lower limb injuries leading to impaired strength, reduced function, and limitations in both daily and athletic activities. 24 We found that the 2 primary management approaches for these injuries are operative and nonoperative treatment. Surgical repair typically involves reattaching the avulsed tendon to the ischial tuberosity, while nonoperative treatment emphasizes physical therapy and gradual return to function.24,26 Despite the availability of both approaches in clinical practice, their comparative effectiveness remains an area of ongoing investigation and debate.
The major findings of our review demonstrated that surgical intervention was frequently associated with favorable outcomes in terms of functional recovery, strength, and return to activity. Across several validated scoring systems, including the LEFS score, HHS, Lysholm score, WOMAC, and UCLA score, patients in the surgical groups generally reported higher scores and greater recovery, although direct comparisons with nonoperative management were limited in several studies.1,2,5,8,9,15,19,21,29 These trends were observed in both short-term and long-term follow-ups, particularly in studies reporting LEFS and MARS scores,1,2 suggesting sustained postoperative function. However, due to incomplete reporting of comparative nonoperative outcomes in many studies, definitive conclusions regarding the superiority of surgical management could not be drawn.
In contrast, nonoperative treatment produced moderate improvements. While LEFS scores approached those of surgical cohorts, overall functional gains were less pronounced, and activity-specific outcomes, such as hop performance and UCLA scores, remained inferior. 12 Better LEFS and strength values were observed in surgically treated patients. 30 It is important to note that these comparisons rely on a significantly unequal distribution of data—11 operative studies compared with only 1 nonoperative cohort—thereby limiting the validity and generalizability of direct comparisons. These differences reflect a recurring pattern in the literature, where nonoperative management yields acceptable but suboptimal results, particularly in high-demand populations.3,18
Muscle strength recovery was also superior in the surgical group. Most studies reported that patients regained ≥75.0% to 90.0% of contralateral leg strength, primarily when surgery was performed acutely.1,2,8,15,19 Balanced flexor strength and high LSI values were also reported, further supporting the role of surgical repair in restoring muscle function. 9 This trend is reinforced by findings of significantly higher strength outcomes in operative patients (85.0%) compared with nonoperative ones (64.0%). 3
In contrast, nonoperative cohorts experienced persistent strength deficits, particularly in eccentric and isometric contraction. 12 Delayed or nonoperative management was associated with poorer strength recovery. 15 Furthermore, heterogeneity in strength testing protocols (eg, isokinetic vs isometric) across studies limits direct comparison. 30
Regarding ROM, surgical patients generally maintained near-normal joint mobility, with no significant differences between the injured and uninjured sides. This indicates that early surgical repair does not appear to compromise joint flexibility and may facilitate an early return to activity.9,15,29 Comparable passive hip flexion was reported on both operated and nonoperated sides (P = .581 and P > .999), reinforcing the preservation of ROM after repair. 9 However, no data were available for ROM after nonoperative treatment, highlighting a notable gap in the literature. Future studies should address whether nonoperative treatment affects passive or active ROM.
Postoperative functional activity levels were generally favorable after surgical repair. Most studies reported a return to moderate to high activity levels, with TAS scores ranging from 4.7 to 6.5,29,33 Higher performance was also observed, with a mean TAS score of 8.5 ± 2.4. 21
In contrast, nonoperative treatment resulted in a statistically significant decline in activity level. 12 While comparable SF-12 mental and physical scores were reported, objective performance and RTS rates favored the operative group. 30 These inconsistencies between subjective and objective measures underscore the need for standardized activity assessments.
Complications were more frequent in surgical cases but were largely minor, including transient stiffness, hematomas, or superficial infections.1,2,5,8,31 Lower complication rates were observed in acute compared with chronic repairs.15,18 A complication rate of 23.2% was reported among surgically treated patients, underscoring the importance of careful patient selection. 3 Overall, the safety profile is considered acceptable when weighed against functional benefits. Although nonoperative management is less invasive, complications such as prolonged bruising or soft tissue issues were reported. 12 However, underreporting remains a possibility. Longitudinal studies may better capture delayed complications, including chronic weakness or reinjury.
Implications for Clinical Practice and Future Research
The findings of this systematic review suggest that operative treatment is associated with better functional, strength, and RTS outcomes compared with nonoperative management, especially in active individuals or athletes. However, treatment decisions should be personalized, taking into account patient goals, comorbidities, and risk profiles.
To improve clinical decision-making and evidence quality, future research should prioritize prospective comparative studies using standardized outcome measures, including consistent assessment of ROM, strength, and functional activity. Moreover, further investigation into the long-term effects and efficacy of nonoperative management is essential to clarify its role and identify patient populations most likely to benefit from nonoperative approaches.
Limitations
This review has several limitations that should be acknowledged. Many included studies had small sample sizes and lacked control groups, reducing external validity. There was substantial heterogeneity in outcome measures, follow-up durations, and strength assessment protocols, making meta-analysis unfeasible. Most of the included studies were observational, and only English-language articles were considered, introducing language bias. It is also important to note that these comparisons rely on a significantly unequal distribution of data—11 operative studies compared with only 1 nonoperative cohort—thereby limiting the validity and generalizability of direct comparisons. Furthermore, the specific tear patterns in each group were not clearly reported; therefore, it is unclear whether the operative series included only complete proximal tendon tears or whether muscle injuries were also represented. This limits the ability to make direct comparisons between operative and nonoperative cohorts. The relatively small number of nonoperative cases, particularly for muscle-related injuries, further reduces the strength of any conclusions drawn and highlights the need for caution in interpretation, including consideration of whether the title should more accurately reflect the available evidence base. Additionally, the exclusion of gray literature, unpublished data, and studies published before 2000 may have introduced publication bias. Taken together, these factors indicate that strong conclusions are difficult to make, and the findings of this review should be interpreted with appropriate caution.
Conclusion
Our study demonstrated that operative treatment resulted in generally good functional outcomes, substantial muscle strength recovery, high patient satisfaction, and a high rate of RTS, although with a higher incidence of mostly minor complications that were not statistically significant. Nonoperative management also showed good outcomes in the few studies available. Given the limited quantity and heterogeneity of available studies, particularly for nonoperative treatment, the current literature does not allow definitive recommendations favoring one approach over the other. Prospective studies with standardized outcome measures and clear subtype definitions are needed to clarify which patients derive the most benefit from operative versus nonoperative treatment.
Footnotes
Appendix 1
The following Boolean search strings and MeSH terms were used across the included databases:
Final revision submitted September 21, 2025; accepted September 30, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not required, as this study is a systematic review of previously published studies and did not involve new data collection from human or animal subjects.