
Abstract
Background:
The kneeling stress radiograph is valuable for quantifying posterior cruciate ligament (PCL) injuries. However, this method presents drawbacks, including patient discomfort during filming, radiation exposure, variability attributable to patient cooperation, and technician skill requirements. The modified Lachmeter technique offers an alternative approach. Its notable advantages are reproducibility, less patient pain or discomfort, and reduction of radiographic exposure.
Purpose:
To compare and find the correlation of the side-to-side difference (SSD) value between the modified Lachmeter technique and the kneeling stress radiograph.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
A total of 33 patients with isolated PCL injury were measured for the SSD value using a modified Lachmeter technique and a kneeling stress radiograph. Demographic data and SSDs were collected from each method and analyzed.
Results:
The sample entailed 26 men and 7 women, with a mean of 37.58 years (range, 15-65 years). There were 14 patients with right knee injuries and 19 patients with left knee injuries. The mean difference in absolute values between the 2 methods was 2.32 ± 2.29 mm. Interobserver and intraobserver intraclass correlation coefficients of the modified Lachmeter showed almost perfect agreement (0.909 and 0.977, respectively).
Conclusion:
The SSD showed an excellent correlation between the modified Lachmeter technique and kneeling stress radiographs. Consequently, the modified Lachmeter technique holds promise as an alternative to stress radiography for patients with isolated PCL injuries.
Keywords
Isolated posterior cruciate ligament (PCL) injuries are relatively uncommon. Diagnosis of PCL injuries remains challenging and prone to missed diagnoses due to its reliance on operator-dependent physical examinations.6,13 Consequently, some patients may lose a chance to receive proper management, potentially leading to adverse outcomes such as osteoarthritis or meniscal injury.1,14,18,20 However, numerous studies4,5,9-11 have developed and proposed alternative methods for diagnosing and quantifying PCL injuries. Stress radiography techniques have gained popularity due to their reproducibility and reliability. Various stress radiographic techniques, including kneeling, Telos (Telos GmbH), and weighted gravity stress techniques, have been developed to evaluate PCL injuries.4,5,9
Some studies support the benefit of stress radiographs (either instrumented knee devices or kneeling) being the gold standard for quantifying PCL injury.5,11,19 However, stress radiography has some drawbacks, including pain and discomfort during the procedure, radiation exposure, the requirement for skilled radiographic technique, and the need for patient cooperation.
The Lachmeter (Lachmeter Co) is an instrument initially proposed to aid in quantifying anterior cruciate ligament (ACL) injuries by measuring the anterior displacement of the tibia. Numerous studies3,17 have established a correlation between ACL injury and Lachmeter measurement. One advantage of this instrument is that it minimizes discomfort and eliminates the need for radiation exposure.
No specialized instrument is available for measuring posterior displacement in PCL injuries. Due to this limitation, a modification technique was developed for the Lachmeter to measure posterior displacement in PCL injuries. This is referred to here as “the modified Lachmeter technique.”
The objective of our study was to compare the side-to-side difference (SSD) values between the modified Lachmeter technique and the kneeling stress radiograph.
Methods
The study included patients who presented at Thammasat University Hospital between January 2018 and December 2022 with suspected isolated PCL injuries. The research was approved by the ethics committee of Thammasat University Hospital (registration No. MTU-EC-OT-0-238/65). The inclusion criteria were patients with unilateral, isolated PCL injuries without meniscal injury confirmed by physical examination and magnetic resonance imaging. Patients with bilateral knee injuries, a history of previous knee surgeries, associated fractures, or multiligamentous injuries were excluded from the study. Demographic details such as age, sex, side of injury, onset of injury, and any previous treatments received were recorded.
The modified Lachmeter technique was performed by applying the Lachmeter to measure the posterior displacement of the tibia to the femur. The modified Lachmeter technique was performed in all patients by 2 independent orthopaedic sports medicine fellows (V.S., C.J.) (Figure 1). The Lachmeter principle is based on measuring the anterior translation of the knee in patients with ACL injuries.

The Lachmeter device, which was used as the measurement tool in this study.
This study used the Lachmeter to evaluate the posterior tibial translation in patients with PCL injury by modifying the standard Lachmeter test. In the modified Lachmeter technique, this principle is measured in the posterior translation of the knee in patients with PCL injuries. The process began with the patient lying supine with the knee flexed at a 90° angle. The proximal support of the Lachmeter was placed at the lower pole of the patella, the distal support was put at the anterior aspect of the distal leg, and the measurement bar was level-adjusted at 1 cm below the most proximal aspect of the tibial tuberosity with the foot held securely in a neutral position. A posterior translation force was applied to create the maximum posterior translation. After force was applied, the device was reset to zero (Figure 2A). Then, the knee was manually pulled forward to achieve maximum anterior translation (Figure 2B). The same measurement steps were repeated on the opposite side. Two independent orthopaedic sports medicine fellows (V.S. and C.J.) performed 3 measurements on each side. Subsequently, mean data were calculated for each side to determine the SSD. The modified Lachmeter technique assesses the motion from the posterior endpoint to the anterior endpoint and could also include native anterior laxity in the measurement. Therefore, the total motion should be greater than the posterior stress. However, the SSD between both knees can eliminate the effect of native anterior laxity.

Modified Lachmeter technique for the left knee in 90° of knee flexion. (A) The tester created manual maximum posterior translation and then set the device to zero value. (B) The tester pulled the tibial to maximal anterior translation and measured the value.
The 3-time measurement was summarized to obtain a mean value on each side, and then SSDs were calculated using the mean value of the affected knee minus the normal knee. Subsequently, the patients underwent standard anteroposterior (AP) and lateral views of the knee and kneeling stress radiographs of both knees.
Kneeling Stress Radiograph Technique
Posterior stress radiography with Telos and kneeling stress radiography are reliable methods for evaluating PCL laxity. 5 Kneeling stress radiographs were performed on each knee to assess PCL laxity and evaluate a posterior translation on the same day as the modified Lachmeter measurement. The patient's knee was placed in a kneeling position on a smooth-padded surface, flexed at 90° to create a posteriorly directed force on the tibial tubercle by the body weight. The radiographic beam was positioned laterally, as depicted in Figure 3.

Demonstration of the kneeling stress radiograph technique on the right knee.
Stress Radiographic Measurement
We used the measurement method described by Jackman et al. 10 A line was drawn parallel to the posterior tibial cortex. Then, another line was drawn that paralleled the first line to the most posterior point along the Blumensaat line. The distance between these 2 lines represented the posterior tibial translation. Displacement of the posterior tibial cortex line (yellow line) anterior or posterior to the posterior aspect of the Blumensaat line (red line) was given a positive or negative value, respectively (Figure 4). The measurement was done on both knees by 2 independent orthopaedic fellows (V.S. and C.J.) who performed 2-time measurements on each side. Subsequently, mean data were calculated for each side to determine the SSD. The repeated measurement was made from the previous radiographs, 2 weeks after the first measurement.

Measurement of posterior tibial translation on the lateral knee radiographs using the technique of Jackman et al. 10 First, a line was drawn parallel to the posterior tibial cortex (yellow line). Then, another line was drawn that paralleled the first line to the most posterior point along the Blumensaat line (red line), which typically should be placed posterior to the yellow line in the normal knee. The distance between these 2 lines represented the posterior tibial translation. Displacement of the posterior tibial cortex line anterior or posterior to the posterior aspect of the Blumensaat line was given a positive or negative value, respectively.
Statistical Analysis
Statistical analyses were conducted using Stata Version 14.2. Categorical data were reported as percentages. Continuous data were reported as mean, standard deviation, and range (minimum-maximum).
From a previous study, 8 the standard deviation of the stress radiographic and instrumented laxity measurements was 3.2 mm. Based on the testing of 2 dependent means calculations, the delta (difference in data between 2 groups) was set as 2, the significance level (alpha) was .05, and the power was 80%. The output of the sample size calculation from n4Studies 16 was 21 samples.
To assess the reliability of measurements, the intraobserver and interobserver reliabilities were evaluated using single-measure intraclass correlation coefficients (ICCs) in a 2-way random-effects model. ICCs are statistical measures that help determine the level of agreement between different observers regarding a specific question or measurement. The ICC values <0.5, 0.5-0.75, 0.75-0.9, and >0.90 indicate poor, moderate, good, and excellent reliability, respectively. 12
Correlation between the SSD of the stress radiographic measurements and the modified Lachmeter measurement was tested using the Pearson correlation coefficient.
Results
A total of 33 patients with isolated PCL injuries were enrolled in this study. The mean age of the patients was 37.58 years, ranging from 15 to 65 years. The onset of injury to the index test was about 28 weeks. The demographic data of the patients are presented in Table 1.
Demographic Data of the Study Population (N = 33) a

Data are expressed as mean (min-max), n (%), or mean ± SD.
The modified Lachmeter and stress radiographic SSDs are plotted in Figure 5, showing good correlation and calculated with a Pearson coefficient of 0.858.

Graph showing the correlation of side-to-side differences between modified Lachmeter and stress radiographic measurements.
The mean and standard deviation were calculated between the kneeling stress radiographs and the modified Lachmeter (Table 2). The SSD values measured from the stress radiographic and modified Lachmeter measurements demonstrated a strong correlation. The mean difference in absolute values between the 2 methods was 2.32 ± 2.29 mm.
Comparison of the Side-to-Side Difference (SSD) Between the Modified Lachmeter Technique and Kneeling Radiographic Measurement a

Negative values represent a posterior translation of the tibia related to the Blumensaat line.
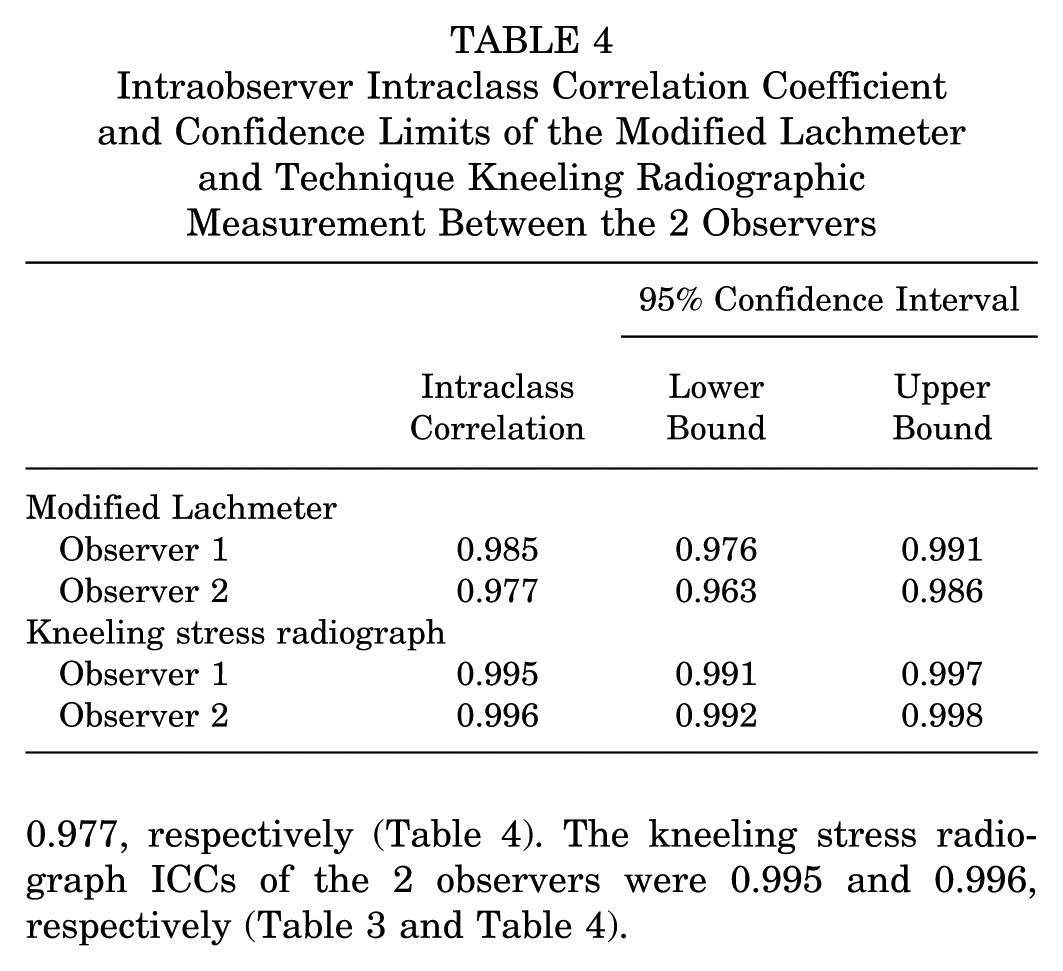
The modified Lachmeter and kneeling stress radiographs had almost perfect agreement of intraobserver and interobserver reliability for evaluating PCL injuries. Interobserver ICCs of the modified Lachmeter and the kneeling stress radiograph were 0.909 and 0.988, respectively (Table 3). The intraobserver ICCs of the modified Lachmeter measured by 2 observers were 0.985 and 0.977, respectively (Table 4). The kneeling stress radiograph ICCs of the 2 observers were 0.995 and 0.996, respectively (Table 3 and Table 4).
Interobserver Intraclass Correlation Coefficient and Confidence Limits of the Modified Lachmeter Technique and Stress Radiographic Measurement

Intraobserver Intraclass Correlation Coefficient and Confidence Limits of the Modified Lachmeter and Technique Kneeling Radiographic Measurement Between the 2 Observers
Discussion
This study found a high correlation (r = 0.858) between the modified Lachmeter technique and kneeling stress radiograph for detecting posterior tibial translation in patients with PCL injury, with a mean difference between the 2 methods of 2.32 ± 2.29 mm.
Stress radiographs are options for evaluating posterior tibial translation in PCL-injured patients. Hewett et al 7 determined that stress radiography was superior to arthrometer (KT-1000) and clinical posterior drawer testing for determining PCL injury, with the value of 8 mm indicating complete PCL rupture. Margheritini et al 15 found that stress radiography was superior to KT-2000 arthrometry in measuring posterior tibial translation. However, both studies used a measurement method that showed poor reliability. 2
Höher et al 8 proposed a technique for measuring AP translation using the Rolimeter compared with Telos stress radiography. The results demonstrated a favorable comparability of the measurement between the Rolimeter and the stress radiograph. However, the limitations of this study were the retrospective study design and the lack of reliability tests.
In this study, we assessed the inter- and intraobserver reliability of the modified Lachmeter technique, which has not been previously studied before and showed almost perfect agreement of reliability. Additionally, we examined the inter- and intraobserver reliability of kneeling stress radiography, which showed almost perfect agreement. The kneeling stress radiograph was described by Jackman et al, 10 who reported the reproducibility of the kneeling technique of stress radiography to quantify the posterior knee instability.
This modified Lachmeter technique offers several advantages, including avoiding patient discomfort and imposing no radiation exposure. Nevertheless, the measurement values obtained using this technique may show variation due to multifactorial factors, including the lack of experience of the surgeon or multiligament injuries.
Limitations
This study has several limitations. The first, this study focused on patients with isolated PCL injuries, minimizing potential outliers or variations in measurements that could arise from concomitant collateral ligament or ACL injuries. Even though we focused on isolated PCL injury, some patients may have varying amounts of anterior translation that could cause a misdiagnosis of bicruciate ligament injury. However, we minimized this by scanning magnetic resonance images to confirm an intact ACL in every case. Second, generalization may vary depending on the population, high body mass index, skin diseases such as scleroderma or scars, and measurement techniques that might be operator dependent. Third, inconsistent force application during modified Lachmeter testing can lead to variable results, affecting diagnostic reliability. Prospective multicenter studies and larger sample sizes may be needed to validate the technique in broader clinical practice, specifically for sports-related applications. Fourth, the study population had an onset of injury at about 28 weeks (minimum 12 weeks); acute PCL injury could not be included in this study. Fifth, a contralateral knee with an intact ACL and PCL was required to evaluate the SSD. Sixth, despite the good correlation with kneeling radiographs, there are still no specific measurements using the modified Lachmeter that correlate with varying degrees of PCL tear, such as partial or complete tear. Seventh, we compared the modified Lachmeter test with the kneeling stress radiograph, which is not the gold standard in evaluating posterior translation of the tibia. The Telos was not used due to limited resources and cost-effectiveness. However, several studies showed good reliability of kneeling stress radiography compared with Telos or KT-arthrometer testing.
Conclusion
The SSD showed an almost perfect correlation between the modified Lachmeter technique and kneeling stress radiography. Consequently, the modified Lachmeter technique holds promise as an alternative to stress radiography for patients with isolated PCL injuries.
Footnotes
Acknowledgements
We would like to thank all participants in the study. We would like to thank the Department of Orthopaedics, Faculty of Medicine, Thammasat University; Thammasat University Hospital; and the Thai Orthopaedic Society for Sports Medicine (TOSSM) for their kind support.
Final revision submitted May 27, 2025; accepted July 26, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Thammasat University Hospital (registration No. MTU-EC-OT-0-238/65).