
Abstract
Background:
The utility of indeterminate magnetic resonance (MR) imaging findings in identifying shoulder pathology in overhead throwing athletes is yet to be determined. The assessment of capsular redundancy on MR arthrography, specifically in the abduction external rotation (ABER) position, could help accurately distinguish between throwing disorders involving internal impingement and those involving anterior instability.
Purpose:
To compare MR arthrography findings in the ABER position between patients with internal impingement with anterior instability and those with traumatic shoulder dislocation.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This study included patients who had subtle glenohumeral instability, as indicated by a positive anterior apprehension test and relocation test results. Those with voluntary and multidirectional instability and with large glenoid bone loss (>25%) were excluded. In total, 95 shoulders (86 male, 9 female; mean age, 23.9 ± 9.4 years) that had undergone arthroscopic procedures were divided into 2 groups: 35 shoulders in the throwing group with internal impingement with anterior instability and 60 in the traumatic dislocation group. We classified the anterior glenohumeral capsular ligaments on MR arthrography in the ABER position into the following 4 types based on a previous report: taut, avulsion, crescent, and fluctuation sign. Compared with arthroscopy, MR arthrography in the side position was evaluated for its accuracy in detecting rotator cuff and labral injuries.
Results:
MR arthrography in the ABER position revealed that the fluctuation sign in 71% of shoulders in the throwing group was significantly greater than that in 12% of shoulders in the dislocation group (P < .001). MR arthrography revealed that rotator cuff and posterosuperior labral injuries were present in 83% and 71% of shoulders in the throwing group, which was significantly greater than the 20% and 23% of shoulders in the dislocation group (P < .001).
Conclusion:
The fluctuation sign on MR arthrography in the ABER position could potentially detect characteristic lesions in throwing athletes with internal impingement with anterior instability.
Keywords
Magnetic resonance (MR) imaging (MRI) is a crucial imaging modality for identifying shoulder disorders; however, its usefulness for identifying shoulder pathology in overhead throwing athletes is yet to be determined. Superior labrum anterior and posterior (SLAP) lesions and internal impingement are characteristic findings in MRI for overhead throwing disorders.24,27,39 However, previous studies demonstrated that MRI abnormalities consistent with internal impingement could be observed in asymptomatic patients.13,26 Among overhead throwing athletes, including those with rotator cuff tears, biceps tears, and labral lesions, symptoms were poorly correlated with abnormalities observed on MRI. 24 Furthermore, another study reported that MRI findings were not predictive of future placement on an injury list or duration of placement. 1
Glenohumeral stability is important for overhead throwing athletes.5,20,23,35,41 Jobe and Bradley 19 stated that a lack of shoulder stability can lead to common disorders in young athletes. However, most throwing athletes who present symptomatic internal impingement with anterior instability do not experience shoulder dislocation and show positive painful apprehension and relocation test results, while athletes with recurrent anterior shoulder instability show positive loose apprehension test results.14,21 A recent study suggested that the physiopathology of internal impingement with anterior instability in throwing athletes might be related to the dysfunction of the anterosuperior GHL, including the middle glenohumeral ligament (MGHL) rather than the inferior glenohumeral ligament (IGHL), as in traumatic anterior shoulder dislocations. 11 Therefore, MR findings of the anterior capsular ligament, including the MGHL and IGHL, would help in identifying the physiopathology of shoulder disorders in overhead throwing athletes.
Assessment of ligamentous structures in the shoulders of overhead throwing athletes is challenging primarily due to the relaxed state of the anterior glenohumeral ligament (GHL) in neutral position and the complex variation in anterior GHL anatomy, making it difficult to obtain reliable evaluations.6,15,38 The main stabilizers of the shoulder at the end range of movement when mimicking overhead throwing motion are the capsuloligamentous structures. 16 At the end range of movement, a part of the shoulder capsule is tight, which prevents translation of the humeral head. 17 The abduction external rotation (ABER) position complements conventional sequences by enabling further assessment of the MGHL, which may appear lax and difficult to fully evaluate on conventional sequences. 40 Schaeffeler etal 42 described that evaluating capsular redundancy on MR arthrography, including ABER, allowed for accurate differentiation between patients with atraumatic multidirectional instability (MDI) of the shoulder and those with clinically stable shoulders. Therefore, we considered that MR arthrography in the ABER position, which simulates the throwing position, would provide important information for assessing the conditions of the capsular ligament in throwing athletes.
This study aimed to compare MR arthrography findings in the ABER position between patients with internal impingement with anterior instability and those with traumatic shoulder dislocation. We hypothesized that GHL disruption patterns on MR arthrography in the ABER position would be different between the 2 groups based on their similar characteristics of positive apprehension and relocation test results.
Methods
Patients and Methods
This study was approved by the institutional review board of Keiyu Orthopaedic Hospital, and all patients provided informed consent for the participation in and publication of this study. Data from consecutive patients who were treated in our hospitals were retrospectively reviewed. Between August 2017 and December 2024, 163 patients underwent MR arthrography in the ABER position and surgery for shoulder instability, including overhead throwing disorders (throwing group) and traumatic dislocation (dislocation group). Shoulder instability was diagnosed based on traumatic episodes, physical examination, plain radiography, and MRI. Although the pathologies of overhead throwing disorders vary, the current study focused on internal impingement with anterior shoulder instability. The present study defined internal impingement with anterior instability as positive outcomes in painful or loose anterior apprehension and relocation tests (Jobe relocation test),14,25,29 alongside negative or improved glenohumeral internal rotation deficit. Additionally, internal impingement was identified between a partial tear of the supraspinatus tendon and the posterosuperior glenoid labrum on MRI scans. Traumatic shoulder dislocation was defined as shoulder instability involving >1 traumatic dislocation. Operated shoulders were included regardless of whether symptoms were present in the ipsilateral or bilateral shoulders. The inclusion criterion was symptomatic shoulder instability requiring surgical treatment, including throwing or dislocation. The throwing group only included the throwing side. The indications for surgery included true apprehension consistent with gross instability of the shoulder, evidence of anterior instability on imaging, lack of improvement with nonoperative treatment, and MR arthrography in the ABER position. The exclusion criteria were previous shoulder surgeries, voluntary instability, extensive glenoid bone loss (>25%), age >50 years, and poor-quality MR arthrography in the ABER position (Figure 1).

Flowchart of patient selection. MR, magnetic resonance.
MR Arthrography
MR arthrography was performed using a 1.5-T scanner (Vantage Orian; Canon Medical Systems) with a flexible surface coil (16-channel speeder large). All examinations were started within 15 minutes after intra-articular injection of a total of 18.1 mL (10 cc of saline, 5 cc of xylocaine, 3 cc of iotrolan 240 mg/mL, and 0.1 mL of gadoteridol [ProHance: Eisai] as the contrast medium via a rotator interval approach under fluoroscopic guidance). Standard MRI was performed with the shoulder in a neutral position. With patients in the supine neutral position, coronal oblique, sagittal oblique, and transverse T1-weighted images (repetition time/echo time = 650-700 ms/15 ms; section thickness = 3.5 mm; field of view = 200 × 200 mm; matrix = 288 × 416; 3 echo factors) were performed. Once MRI in a neutral position was completed, patients were instructed to place the ipsilateral hand behind the head or neck with the elbow flexed to obtain the ABER position. If patients did not tolerate this positioning, it was also acceptable to place the hand of the affected extremity above the head with the elbow flexed. Oblique axial T1-weighted images (repetition time/echo time = 650-700 ms/15 ms; section thickness = 3.5 mm; field of view = 200 × 200 mm; matrix = 288 × 416; 3 echo factors) were obtained parallel to the glenoid cavity using a T1-weighted coronal localizer image for placement.
Image Interpretation
MR arthrograms were randomly evaluated by 2 observers with experience in musculoskeletal radiology (T.F., S.M.) and did not contain any patient information. Images of the side position sequences were evaluated for cuff tears, SLAP, and labral injury, which included heterogeneity or hyperintensity of the lesions. Axial images of the ABER position sequences were evaluated for the anterior GHL. According to Schaeffeler classification, 42 we classified the following 4 types of the anterior GHLs, including the MGHL and IGHL.
Taut appearance of the GHL: taut GHL serves as the primary soft tissue stabilizer for the humeral head during ABER (Figure 2A)
Avulsion of the GHL: the GHL being loose with an avulsed or displaced anteroinferior labrum from the glenoid (Figure 2B)
Crescent sign of the GHL: presence of a crescent-shaped layer of intra-articular contrast material between the humeral head and GHL (Figure 2C)
Fluctuation sign of the GHL: presence of fluctuating GHL beside the labrum despite the GHL’s being taut on the humeral head (Figure 2D)
The anterior GHL was evaluated at the 2, 3, and 4 o’clock positions of the glenoid (Figure 3).

T1-weighted magnetic resonance arthrograms in the abduction external rotation position. (A) Taut appearance: the taut glenohumeral ligament (GHL) (white arrow) serves as primary soft tissue stabilization for the humeral head (HH) in abduction and external rotation. (B) Avulsion appearance: the GHL is loose with an avulsed or displaced anteroinferior labrum from the glenoid (white arrow). (C) Crescent sign: presence of a crescent-shaped layer (white arrow) of intra-articular contrast material between the HH and GHL. (D) Fluctuation sign: presence of fluctuating GHL (white arrow) beside the labrum despite the GHL’s being taut on the HH. G, glenoid.

T1-weighted magnetic resonance arthrograms in the ABER position at the 2, 3, and 4 o’clock positions of the glenoid. (A) Three-dimensional computed tomography: lines at the 2, 3, and 4 o’clock positions. (B) Two o’clock: the glenohumeral ligament (GHL) is vaguely loose without avulsed labrum. (C) Three o’clock: presence of fluctuating GHL. (D) Four o’clock: the GHL is loose but not injured. G, glenoid; HH, humeral head.
MR images were assessed to determine interobserver reliability and intraclass correlation coefficients. The interobserver reliability was calculated from the classification of 2 same observers experienced in musculoskeletal radiology. The intraclass correlation coefficients for interobserver reproducibility were reassessed in 2 weeks.
Intraoperative Arthroscopic Findings
Anterior GHL reconstruction (AGCR) surgeries were performed in the beach-chair position using a spider limb positioner (Smith & Nephew). Surgeries for Bankart lesions or SLAP repair were performed in the lateral decubitus position using 4.5 kg of traction. A 4-mm arthroscope with 30° and 70° angulations was inserted through a standard posterior portal in all patients. An arthropump was used to deliver a saline solution at a constant pressure (30 mmHg). Systematic arthroscopic examination was performed without traction to visualize the internal structures, and the arm was placed in the ABER position until contact rim was observed between the articular surface of the supraspinatus tendon and posterior superior glenoid. Arthroscopic findings showed anteroinferior labroligamentous complex lesions as detachment of the IGHL and labrum from the anterior glenoid with or without a ruptured periosteum, including Bankart lesion. In addition, rotator cuff injury and SLAP lesions were evaluated as positive or negative using the Ellman classification and the Snyder and Maffet classification.7,28,37,43 These findings were assessed by a single surgeon (T.F.).
Statistical Analysis
The Kruskal-Wallis test, Fisher exact test, Tukey test, Steel-Dwass test, and 1-way analysis of variance were performed to compare the 2 groups with respect to age, body mass index (BMI), sex, height, body weight, and evaluation of categorical groups. Fisher exact test was performed to compare the 2 groups with respect to MR arthrography and arthroscopic findings. P values of <.05 were considered statistically significant. All statistical data were analyzed using R, Version 4.0.2 (R Foundation for Statistical Computing).
Results
Patients
In total, 95 patients with 95 shoulders (86 male individuals and 9 female individuals; mean age, 23.9 ± 9.4 years) who underwent arthroscopic procedures were divided into 2 groups: 35 shoulders in the throwing group and 60 shoulders in the dislocation group (Table 1). The throwing group included 33 baseball players, 1 tennis player, and 1 badminton player. Collegiate-level players had the highest proportion in the throwing and dislocation groups (65.7% and 30%, respectively). All patients in the throwing group experienced shoulder pain at maximal external rotation during the throwing motion without an evident traumatic shoulder dislocation episode. The dislocation group included 7 patients with 1 dislocation and 53 with >1 dislocation. All patients tested positive in the painful or apprehension test. In total, 54 (90%) shoulder dislocations occurred during sports activity. The remaining cases involved 6 (10%) work-related injuries. Table 1 summarizes the demographic data of the 95 shoulders. The patients in the throwing group were significantly more likely to be male, have a larger physique, and use the dominant side more frequently than those in the dislocation group.No significant differences were noted between the throwing and dislocation groups in terms of age or BMI. In the throwing group, 2 SLAP repairs, 2 labral repairs, and 31 AGCRs are shown in Table 1.
Patient Demographic Variables a

Data are presented as n or mean ± SD unless otherwise indicated. ABR, arthroscopic Bankart repair; AGCR, anterior glenohumeral capsular ligament reconstruction; SLAP, superior labrum anterior and posterior.
MR Arthrography Interpretation
MR arthrography in the ABER position revealed the ratio of the 4 types of anterior GHLs at the 2, 3, and 4 o’clock positions of the glenoid. Although the fluctuation in the throwing group was significantly greater than that in the dislocation group at the 2, 3, and 4 o’ clock positions of the glenoid, the odds ratio of the fluctuation sign was highest at the 3 o’ clock position of the glenoid (Table 2). Therefore, the fluctuation sign was evaluated at the 3 o’ clock position of the glenoid in the current study. MR arthrography in the ABER position revealed that the fluctuation sign in 71% of shoulders in the throwing group was significantly greater than that in 12% of shoulders in the dislocation group (P < .001) (Tables 2 and 3).
Comparison of Anterior Glenohumeral Ligament in MR Arthrography Findings Between Dislocation and Throwing Groups a
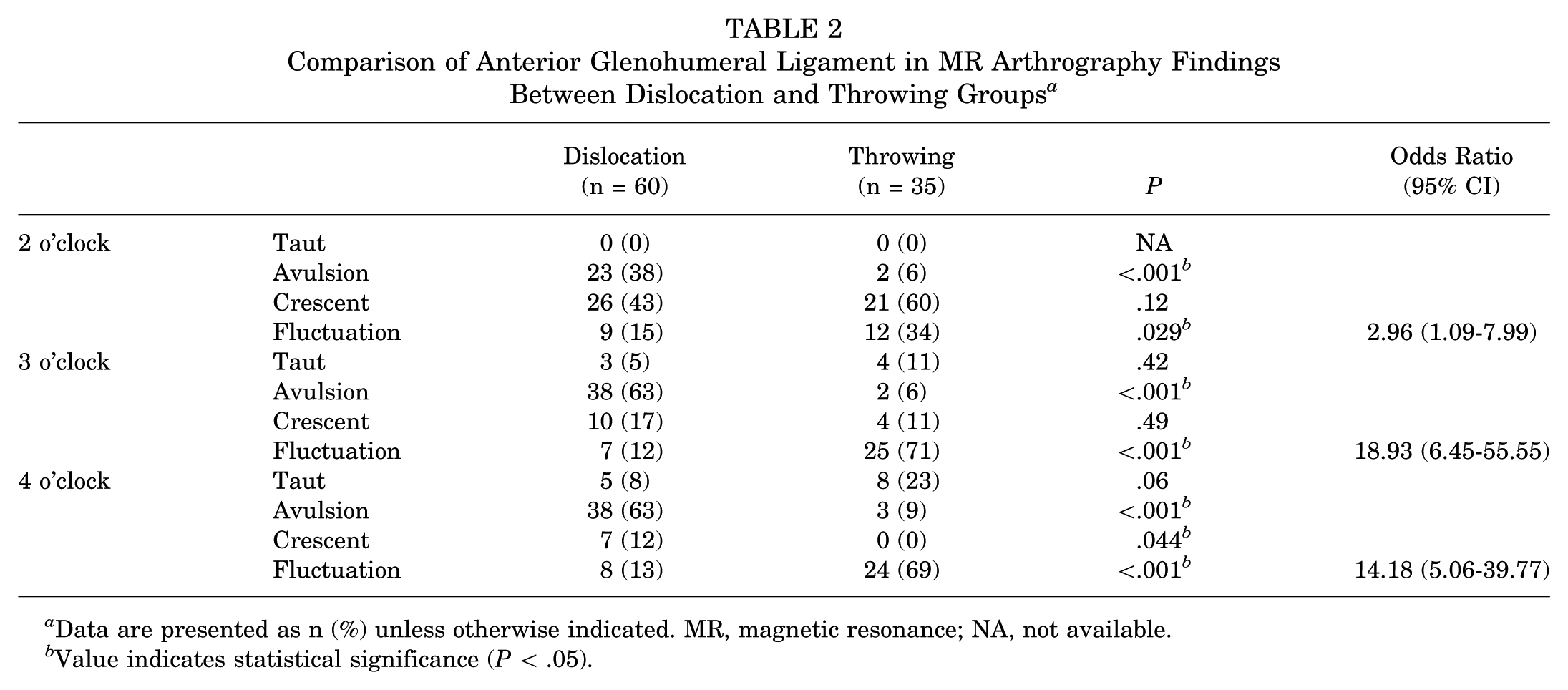
Data are presented as n (%) unless otherwise indicated. MR, magnetic resonance; NA, not available.
Value indicates statistical significance (P < .05).
Comparison of MR Arthrography Findings Between the Dislocation and Throwing Groups a

Data are presented as n (%). AGHL, anterior glenohumeral ligament; AI, anteroinferior; AS, anterosuperior; MR, magnetic resonance; PI, posteroinferior; PS, posterosuperior; SLAP, superior labrum anterior and posterior.
Value indicates statistical significance.
The intraclass correlation coefficients and interobserver reliability of the fluctuation sign were in high agreement (Kappa coefficient = 0.817 [95% CI, 0.72-0.91]) and 0.73 ([95% CI, 0.71-0.88]), respectively.
MR arthrography revealed that cuff tears (supraspinatus and/or infraspinatus tendon) in 83% of shoulders in the throwing group were significantly greater than those in 12% of shoulders in the dislocation group (P < .001). There were no significant differences in the SLAP lesion between the throwing and dislocation groups. In the dislocation group, the avulsion sign was observed in 63% of shoulders, significantly greater than 6% in the throwing groups. The characteristic findings of MR arthrography in the throwing group were cuff tears, posterosuperior labral tears, and the fluctuation sign compared with those in the dislocation group (Table 3).
Arthroscopic Evaluation
Arthroscopic evaluation revealed anteroinferior labroligamenotus complex lesions (Bankart lesions) in 90% and 9% of shoulders in the dislocation and throwing groups, respectively (Table 4). In addition, arthroscopic findings showed significantly greater cuff tears in the throwing group than in the dislocation group.On the other hand, there were no significant differences in SLAP lesion between the throwing and dislocation groups.
Comparison of Arthroscopic Findings Between Dislocation and Throwing Groups a

SLAP, superior labrum anterior and posterior.
Accuracy of MR Arthrography
Compared with the arthroscopic findings, the positive and negative predictive value and accuracy of MR arthrography for detecting Bankart lesion were 97%, 97%, and 97%, respectively (Table 5).
Accuracy of MR-A and Arthroscopy in Diagnosing Bankart Lesions, Cuff Tears, and SLAP Lesions a

Data are presented as n. MR-A, magnetic resonance arthrography; SLAP, superior labrum anterior to posterior.
Discussion
Our study demonstrates that MR arthrography of the shoulder in the ABER position has the potential to identify patients with overhead throwing disorders. The incidence of the fluctuation sign on MR arthrography in the ABER position was significantly higher in the throwing group, observed in 71% of shoulders, than in the dislocation groups at 12% (P < .001). In addition, MR arthrography revealed that cuff tears and posterosuperior labral tears in the throwing group were significantly greater than those in the dislocation group.An important finding of the current study was that the characteristic pattern of MR arthrography in the ABER position in overhead throwing athletes with instability was the fluctuation sign of the anterior GHL.
We suppose that the relaxed tension of the anterior GHL is a cause of the decentering of the humeral head, leading to the appearance of the fluctuation sign on MR arthrography in the ABER position. The fluctuation of the anterior GHL on MR arthrography in the ABER position was defined as a fluctuating anterior GHL. While the anterior GHL was clearly visible on MR arthrography in the ABER position, the majority of GHLs (71%) in the throwing group were categorized as having the fluctuation sign. The fluctuation sign is important because it may help identify individual pathologies of complicated throwing disorders, including capsular redundancy. The dominant shoulder of throwing athletes develops an adaptive increase in external rotation and horizontal abduction through both soft tissue and osseous changes. Previous biomechanical studies support the notion that hyperangulation during horizontal abduction causes symptomatic internal impingement.30-32 Mihata etal 31 indicated that excessive glenohumeral horizontal abduction might cause internal impingement, reporting that increased anterior capsular laxity significantly increased horizontal abduction and contact pressure at the posterosuperior glenohumeral joint. 32 Thus, repetitive microtrauma or mechanical stress can lead to the conversion of these adaptive changes to pathologic injury. Burkhart and Lo 3 and Burkhart and Morgan 4 indicated that the relative redundancy in the anteroinferior shoulder capsule may have clinical implications in the pathology of the disabled throwing shoulder. Funakoshi etal 11 reported that the physiopathology of internal impingement with anterior instability in throwing athletes may be related to the dysfunction of the anterosuperior GHL, including the MGHL, rather than that of the IGHL as in traumatic anterior shoulder dislocations. In the current study, arthroscopic findings demonstrated that the anteroinferior labroligamentous complex lesions in the throwing group were significantly less damaged than those in the dislocation group, as previously reported.11,35 Despite an intact anteroinferior labrum and anteroinferior GHL, the glenohumeral joint showed subtle instability in throwing athletes with internal impingement and anterior instability. The fluctuation sign of the anterior GHL would indicate a relaxed but not injured GHL. In addition, the capsular redundancy and instability of the shoulder on MR findings could aid in the appropriate treatment decision. Jobe and Bradley 19 stated that most pervasive disorders in young athletes were due to a lack of shoulder stability. Several surgical outcomes indicate the importance of stability and satisfactory results in overhead throwing athletes after shoulder stabilization.5,20,23,35,41 Jobe etal 20 reported satisfactory results following anterior capsulolabral reconstruction in overhead throwing athletes. Funakoshi etal 10 reported that AGCR may represent a solution for internal impingement with anterior instability in overhead throwing athletes. We consider that the fluctuation sign of the anterior GHL would be involved in the clinical application for an appropriate surgical strategy.
In the current study, we were unable to distinguish between the MGHL and IGHL using MR arthrography in the ABER position. This was due to the various attachments of the GHL, which included underdeveloped, disappeared, and cord-like MGHLs.6,15,38 Since Flood 9 described the 3 GHLs, including the superior GHL, MGHL, and IGHL, several anatomic and biomechanical studies have shown that the anterosuperior GHL is an important stabilizer when shoulder abduction is <90°.2,8,12,33,34,44,45 Conversely, in a morphologic cadaveric study, Pouliart and Gagey 36 reported that the MGHL and IGHL were clearly observed as bands defined by arthroscopy in the resting position and that when the arm was moved into full ABER, all bands progressively disappeared. This finding suggests that the MGHL and IGHL may be difficult to divide on the ABER position. In addition, interpretation of the obtained 2-dimensional slices would be difficult for the entire anterior capsular ligament. Gohlke etal 12 also described a complex cross-linking pattern visible in the superior capsule and a system of fiber bundles spiraling across each other in the anteroinferior capsule. For these reasons, the current study assessed the entire anterior GHL without dividing the MGHL and IGHL.
The term shoulder instability encompasses various mechanisms and clinical presentations, such as symptomatic general joint laxity, subluxation, dislocation, and microinstability. Jobe and Pink 22 introduced generalized ligamentous laxity, including the shoulder, elbow, knee, finger, and thumb, as group 3. Several pathologies associated with throwing disorders including injured or underdeveloped GHL can result in various shapes of the GHL on MR arthrography in the ABER position. The crescent sign also suggests that a concept of humeral head decentralization might help identify shoulder pathology in throwing athletes, including patients with generalized ligamentous laxity. Schaeffeler etal 42 indicated that the crescent sign can be interpreted as an expression of the anteroinferior GHL, if noted in patients with clinically diagnosed atraumatic MDI. They stated that elongation of the inferior joint capsule might allow hyperabduction and decentering of the humeral head. Therefore, the crescent sign could indicate the elongation of the anterior GHL and decentering of the humeral head in patients with throwing disorders, similar to that in patients with MDI.
On the other hand, the fluctuation signs on MR arthrography may be present in asymptomatic loose shoulders of overhead throwing athletes. As we have previously described, the dominant shoulder of throwing athletes develops an adaptive increase in external rotation and horizontal abduction. This study revealed that rotator cuff tears in the throwing group were larger than those in the dislocation group.Therefore, a combined assessment including the fluctuation sign, cuff tears, and posterosuperior labral tears may allow for a more accurate diagnosis. A previous study described the characteristic lesions of internal impingement with anterior instability in throwing athletes, including partial-thickness rotator cuff tears, SLAP lesions, posterosuperior labral tears, and hypoplastic MGHLs. 11 We believe the whole anterior capsular function should be considered for stabilization of the shoulder in throwing athletes because throwing disorders involve several conditions: acquired repetitive microtrauma, congenital ligamentous laxity, and traumatic dislocation, as classified by Jobe. 22 The current study showed that the fluctuation signs on MR arthrography in the ABER position were highly accurate in identifying throwing athletes who have internal impingement with anterior instability. Nonetheless, assessing the anterior GHL conditions via MRI remains challenging. We recommend that multiple factors, including patient history, clinical presentation, and other MR findings, should be considered for the correct diagnosis and treatment of disabled shoulders in overhead throwing athletes.
Limitations
This study has certain limitations. First, the sample size was small, and the study design was retrospective. Second, contrast injection has the inherent disadvantages of being a painful procedure, requiring extended time, and having a risk of iatrogenic extravasation. The imaging time was extended by 5 minutes or 25% of the time of the routine protocol.18,40 Third, the ABER position was remarkably apprehensive in some patients, especially those with acute traumatic dislocation. The ABER position reflects the appearance of the GHL. Although the ABER position would mimic the throwing motion better than the conventional position, the ABER position is not considered the same as the throwing motion. Fourth, selection bias of the divided groups should be considered. We divided the patients into 2 groups based on their history and clinical presentation in terms of the shoulder dislocation episodes, the anterior apprehension test, and relocation test. Pathologies, including congenital ligamentous laxity or acquired injury, may overlap in several patients. More than half of the patients in the dislocation group also participated in overhead sports. Fifth, it did not include healthy controls. Given that the evaluation of MR arthrography findings in the ABER position was too invasive to ascertain the absence of pathological lesions in a healthy throwing athlete, we compared these findings with those of patients in the dislocation group.Disabled throwing athletes without anterior instability may be candidates for controls. Last, the fluctuation sign on MR arthrography in the ABER position could not be confirmed on arthroscopy in terms of the ABER position, volume of intrajoint fluid, and limitation of narrow space in the anterior evaluation from posterior viewing.
Conclusion
The fluctuation sign on MR arthrography findings in the ABER position was found more frequently in overhead throwing athletes with internal impingement and anterior instability than in patients with traumatic shoulder dislocation. Our study indicated that MR arthrography in the ABER position could potentially detect capsular redundancy of the anterior GHL as a characteristic lesion of internal impingement with anterior instability in throwing athletes. These findings may be useful for the correct diagnosis and selection of an appropriate treatment strategy for disabled overhead throwing athletes with internal impingement and anterior instability.
Footnotes
Final revision submitted June 4, 2025; accepted July 15, 2025.
Presented as a poster at the annual meeting of the AOSSM, Nashville, Tennessee, July 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Keiyu Orthopaedic Hospital (No. 3630).