
Abstract
Background:
While ulnar collateral ligament (UCL) injuries have been widely studied, no investigations have characterized the kinematics of acutely presenting UCL injuries or examined the pitch-by-pitch sequence leading up to ligamentous failure.
Purpose:
To use Statcast pitch-tracking metrics from Major League Baseball (MLB) games to identify potential warning signs for acute UCL injury.
Study Design:
Retrospective case-control; Level of evidence, 3.
Methods:
Seven MLB pitchers who sustained acute UCL injuries on a single pitch between 2020 and 2025 were retrospectively identified. Statcast data from the injury game and 4 prior outings were analyzed for each player. Five pitch-tracking metrics (velocity, spin rate, release extension, arm angle, and acceleration magnitude) were extracted for each pitch. For each pitcher and pitch type, a principal component model was trained on control outings; Mahalanobis distance (MD) was calculated to quantify multivariate deviation from baseline. To assess short-term variability, MD values from the 5 fastballs before injury were summed and compared with control-derived thresholds. Pitch-to-pitch trends in MD and individual features were analyzed for progressive changes. Matched controls were selected according to age, handedness, starting versus relief pitcher, and season pitch count. The same process was then completed for a 5-game sample window of pitches for these matched controls. Outlier pitches and periods of elevated short-term variability were identified when MD values exceeded a 95th percentile threshold derived from each pitcher's control data; statistical significance for performance trends was set at P < .05.
Results:
Principal component analysis and MD analysis revealed 3 principal findings: (1) every injury pitch was a mechanical outlier based on MD exceeding the 95th percentile of the control distribution (all P < .05), (2) velocity was suppressed by a mean of 2.1 SD and arm angle reduced by a mean of 1.5 SD at the injury pitch, and (3) 86% of pitchers (6 of 7) showed elevated cumulative deviation across the 5 fastballs preceding injury, compared with 7% of matched controls (1 of 14) (P < .001).
Conclusion:
This study demonstrated that acute UCL injuries in MLB pitchers are often preceded by identifiable changes in key pitch-tracking metrics. Rather than a prolonged deterioration across outings, acute UCL failure may reflect a distinct biomechanical pattern marked by short-term variability and abrupt decompensation within the injury game. These findings provide the first pitch-level characterization of UCL failure and may support future in-game risk-monitoring strategies. However, future studies are needed to help understand these warning signs and prevent UCL injury.
Ulnar collateral ligament (UCL) injury is among the leading causes of extended absence in Major League Baseball (MLB) pitchers and one of the most impactful injuries in professional sports. 7 Epidemiologic studies suggest that approximately 25% of MLB pitchers will undergo UCL reconstruction (UCLR) during their careers, a rate that has risen steadily from youth through professional levels, especially over the past decade.4,12 Although newer surgical techniques, such as primary repair with internal brace augmentation, have shortened return-to-play timelines (9.2 vs 13.4 months), 10 UCL injuries still result in prolonged absences and impose significant financial burdens on players and teams. 27
During the overhand pitching motion, the elbow experiences extreme valgus torque, particularly during the late cocking and early acceleration phases.15,36 Peak torque values up to 120 N·m have been recorded, far exceeding the tensile strength of the UCL, estimated at 30 to 40 N·m in cadaveric studies.28,33,36 This mismatch necessitates dynamic stabilization from surrounding musculature, primarily the flexor-pronator mass.28,35,38 Over time, repetitive high-stress pitching induces microtrauma and progressive ligamentous degeneration. 15 These chronic changes often manifest as reduced velocity, diminished command, or vague medial elbow pain. 20
Not all injuries follow this gradual course. A significant subset of UCL tears occurs acutely, with pitchers reporting a sudden “pop” and immediate pain on a single pitch.26,38 In some surgical cohorts, these abrupt failures account for nearly half of all reconstructions. 3 Although such injuries appear instantaneous, they are widely considered “acute-on-chronic,” final ruptures of structurally degenerated ligaments. 11 Imaging studies have backed this notion, revealing evidence of chronic damage even in first-time tears.18,21
Despite their frequency and distinctive presentation, the pitch-level mechanics of acutely presenting UCL failure in pitchers remain unstudied. Prior studies have aggregated injuries across types and time frames, limiting insight into whether acute tears are preceded by measurable changes in mechanical variables such as velocity, arm angle, or release extension.24,25,26
Since 2015, MLB's Statcast system has enabled the release of high-resolution pitch-tracking metrics, including velocity, acceleration, spin rate, extension, and release point. 24 Studies using these data have identified long-term predictors of UCL surgery—such as elevated mean velocity, increased offspeed pitch usage, release location, and overall pitching ability. ‖ One study noted gradual velocity and spin declines in the weeks preceding reconstruction, 26 but otherwise these patterns describe season-level trends, not the kinematic profile of the pitch sequence immediately preceding injury. No known study to date has evaluated whether the injury pitch, or the sequence leading up to it, deviates from a pitcher's mechanical baseline.
Therefore, the primary objective of this study was to evaluate if acute UCL failure is preceded by detectable changes in pitch-tracking metrics such as velocity, spin rate (rpm), release extension (feet), arm angle (degrees), and acceleration, or if it occurs without biomechanical warning. First, we hypothesized that the injury pitch itself would represent a clear mechanical outlier relative to each pitcher's recent baseline. Second, we hypothesized that the cumulative mechanical deviation of the 5 fastballs before the injury pitch would be significantly greater than the pitcher's typical variability.
Methods
Study Design and Participant Selection
This study was deemed exempt from institutional review board approval, as it involved no interaction with human participants and utilized only publicly available data. A retrospective analysis was performed on MLB pitchers who underwent UCL surgery between 2020 and 2025, using a publicly available database. 31 Each case was manually reviewed to identify injuries with a clearly documented acute onset—defined as symptoms occurring on a single pitch during a regular season game, followed by immediate removal from the game. Injury acuity was confirmed by cross-referencing official MLB transactions, postgame updates, and reputable media sources. We specifically searched for language suggesting acute presentation (eg, “felt a pop”). Pitchers were excluded if they were removed between innings, had vague or progressive symptoms, or lacked sufficient Statcast data. Statcast is MLB's advanced pitch-tracking system, which provides high-resolution measures of velocity, spin rate, extension, and release point. 25 Inclusion criteria required (1) symptoms attributable to a single pitch, (2) immediate in-game removal, and (3) complete Statcast data for the injury outing and ≥2 prior appearances. Of the 146 eligible pitchers, 7 met all criteria and were included in the final analysis. Player identities were anonymized (eg, pitcher 1-7) to protect privacy. Statcast data from the injury game were analyzed in comparison with a pitcher-specific multivariate control model derived from 4 prior outings, enabling pitch-level assessment of mechanical deviation at or leading up to the moment of injury. Pitch counts varied across pitchers and analyses, and all models were constructed independently for each case.
Each case was then assigned 2 matched controls who were matched according to age, handedness, starting versus relief pitcher, and season pitch count. A 5-game best possible sample window of pitches aligned with year and time of season was then selected and the same pitch-tracking analysis process was run as performed on case data. A total of >900 pitches were then analyzed for controls.
Pitch Type Classification and Control Definition
Each injury pitch was assigned a pitch type using MLB Statcast classifications, including 4-seam fastball (FF), sinker (SI), slider (SL), and changeup (CH). For each pitcher, control pitches were defined as pitches of the same type thrown during the 4 most recent outings preceding the injury game. The total number of these control pitches is denoted by N control, and N injury represents the number of that pitch type thrown in the injury game. Three pitchers had <4 control appearances because of data availability (2 pitchers had 3, and 1 had 2). All analyses accounted for these discrepancies by modeling each pitcher's baseline mechanics using only the player's available control data. Because all statistical procedures were performed within pitcher and within pitch type, differing control sample sizes did not affect the validity of the models or the interpretation of injury deviations. Only pitch types that were listed as the injury pitch in our cohort were included in our analysis.
Feature Extraction and Mahalanobis Distance
For each pitch, the following kinematic features were extracted from Statcast tracking data: velocity (mph), spin rate (rpm), extension (feet), arm angle (degrees), and 3 orthogonal acceleration components (horizontal [ax], vertical [ay], and lateral [az]; in ft/s2). 1 Kinematic features were extracted specifically for the injured pitcher and for the injury pitch type. Velocity was defined as the release speed of the ball in mph, while spin rate represented the ball's rpm at release. Extension referred to the distance from the pitching rubber to the release point, capturing how far down the mound the ball was released. Arm angle was defined as the horizontal angle between the pitcher's throwing shoulder and the ball at release. 1
The 3 acceleration components quantified the linear acceleration of the ball at release along the ax, ay, and az axes. To summarize overall force imparted to the ball, a scalar measure of total linear acceleration—acceleration magnitude—was calculated √(ax2+ay2+az2).
All features were standardized (z-scored) within pitcher and pitch type using only the control period data. Principal component analysis (PCA) was applied to each control data set, retaining components sufficient to explain ≥95% of the variance. PCA is a dimensionality reduction technique that transforms correlated features into uncorrelated principal components, ordered by the variance they explain. Each injury-game pitch was projected into this PCA-defined space, and Mahalanobis distance (MD) was computed to quantify multivariate deviation from the pitcher's baseline. MD accounts for correlations between variables and identifies how far a pitch lies from the center of the control distribution. Higher MD values reflect greater departure from typical mechanics.
For each pitcher, only pitches of the same type as the injury pitch were included in the analysis, leading to 387 pitches being included in the PCA. PCA was applied to control period pitches from the 4 most recent outings, retaining components that collectively explained ≥95% of the variance. Each injury-game pitch was then projected into this PCA space, and MD was calculated to quantify deviation from baseline. An injury pitch was labeled an outlier if its MD exceeded the 95th-percentile threshold of the control distribution.
Variability Detection Analysis (Fastballs Only)
To assess preinjury variability, analysis was restricted to each pitcher's primary fastball type—either FF or SI—depending on which pitch he threw most frequently. Some pitchers primarily throw an SI as their fastball, and thus we wanted to make sure we were capturing each pitcher's primary fastball type. Fastballs were selected because of their prevalence in MLB (comprising >50% of all pitches in recent seasons) 17 and their established use as a biomechanical reference point due to consistent mechanics and high joint loading.22,23
For each pitcher, ≤5 fastballs immediately preceding the injury pitch were identified, and the MDs of these pitches were summed to produce an observed lead-up MD sum. To establish a reference threshold for abnormal variability, all control period fastball MDs were extracted and ordered chronologically across the 4 most recent outings. A 5-pitch rolling window was applied to this sequence to generate control 5-pitch MD sums, and the 95th percentile of this distribution defined the variability threshold. Lead-up MD sums exceeding this threshold were classified as unstable.
In addition, to evaluate whether MD progressively increased in the pitches immediately preceding injury, Spearman rank-correlation coefficient (ρ) was calculated between MD and the pitch sequence index (1–5) for each pitcher. A positive and statistically significant ρ would indicate progressive mechanical drift prior to ligament failure. Group differences in the proportion of pitchers exceeding the cumulative deviation threshold were compared between injury and control groups using Fisher exact test.
Biomechanical Trend Exploration
Feature-wise z-scores were computed for each pitch and pitch type in the injury game using the control period as the reference. For each pitcher, directional changes over the final 5 preinjury pitches were examined in 5 core metrics: velocity, spin rate, extension, arm angle, and acceleration magnitude. z-scores examine all pitch types, but scores are normalized between each pitch type.
Statistical Analysis
All data processing, statistical analyses, and visualizations were performed in R (Version 4.3.1; RStudio) using the packages FactoMineR, stats, ggplot2, and custom scripts developed for reproducibility. Given that the case and control samples were individualized models, no direct comparisons could be made.
Results
Demographics
Demographics of the injured pitchers are described in Table 1. Mean age of injured pitchers was 25.8 ± 2.0 years, with a majority (71%) being right-handed. On average, injured MLB pitchers had already played over 3 MLB seasons, and pitch count in the season prior to injury was 1011.4 ± 786.7 and 381.7 ± 262.7 in the index season of injury. Finally, 3 (42.9%) pitchers were starters and 4 (57.1%) were relievers. All were primary UCL injuries without any previous UCL injury or associated procedure reported.
Demographics of MLB Players Who Sustained an Acute UCL Injury a
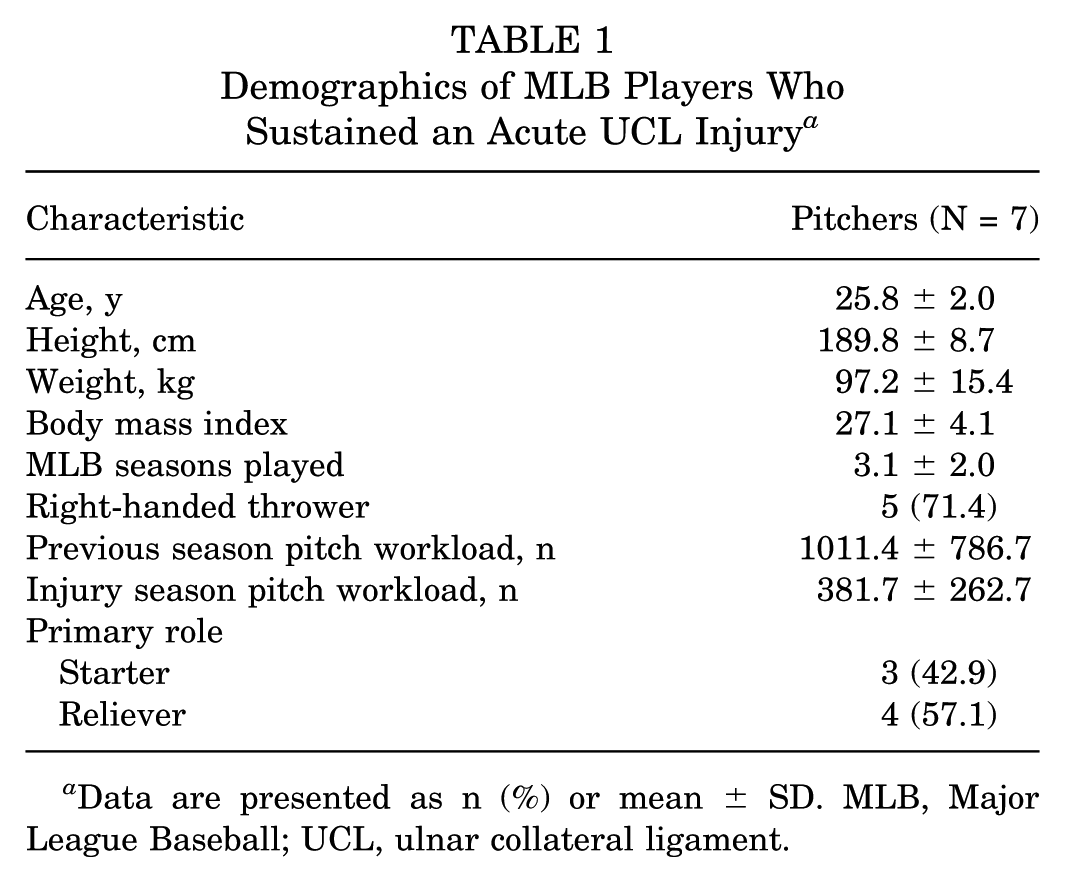
Data are presented as n (%) or mean ± SD. MLB, Major League Baseball; UCL, ulnar collateral ligament.
Pitch-Specific Mechanical Variability-Injury Pitch
In all 7 pitchers, the injury pitch cleared the 95th percentile variability threshold (Table 2), confirming a statistically significant multidimensional deviation at the moment of injury. This was in contrast to the matched controls who had none out of the 14 pitchers with an outlier final pitch (Table 3).
MD Analysis for Injury Pitches a

This table quantifies the multidimensional deviation of the specific pitch on which each acute UCL injury occurred (n = 7). For each pitcher, a baseline model was built using individualized PCA on five kinematic features (velocity, spin rate, extension, arm angle, and acceleration magnitude) from pitches of the same type thrown during a control period (up to four prior outings). N injury indicates the number of pitches of that type thrown in the injury game, and N control indicates the number of pitches used to construct each pitcher's baseline model. The injury MD represents the Mahalanobis distance of the injury pitch relative to that baseline distribution, and the 95th percentile of the control MD distribution defines the individualized threshold used to identify outliers. A pitch was classified as an outlier (“Yes”) if its injury MD exceeded this threshold. Note: Limited control counts for some cases reduce threshold stability; however, the analysis is within pitcher and within pitch type. CH, changeup; FF, four-seam fastball; MD, Mahalanobis distance; PCA, principal component analysis; SL, slider.
MD Analysis of the Final Pitch for Matched Control Pitchers a

This table provides the comparative analysis for the 14 matched controls, quantifying the multidimensional deviation of the final pitch of a representative outing. For each control pitcher, a baseline model was built using PCA on five kinematic features (velocity, spin rate, extension, arm angle, and acceleration magnitude) from their most frequently thrown pitch type during the four outings preceding the reference game. N index indicates the number of pitches of that type thrown in the final game, and N control indicates the number of pitches used to construct each pitcher's baseline model. The final-pitch MD represents the Mahalanobis distance of the final pitch (from the fifth sample game, serving as the methodological analog to the injury pitch) relative to that baseline. The 95th percentile of the control MD distribution defines the individualized threshold used to identify outliers. The Outlier column indicates whether the final pitch's MD exceeded its individualized threshold. FF, four-seam fastball; MD, Mahalanobis distance; SI, sinker.
To visualize mechanical trajectories throughout the injury game, MD values were plotted across pitch sequences for each pitcher (Figure 1, A and B).

MD trajectories across injury games for case pitchers. This figure visualizes the individualized MD analyses, plotting per-pitch MD values for the injury-specific pitch type across both the control period and the injury game to allow direct visual comparison of the injury outing (red) with the pitcher's baseline mechanics (black). MD per pitch is computed from an individualized PCA model trained on that pitcher's control data (features: velocity, spin rate, extension, arm angle, and acceleration magnitude); thus, larger MD values indicate greater multivariate deviation from the pitcher's baseline. The x-axis represents the chronological pitch number within an outing, and the y-axis represents per-pitch MD. Red and black dots denote individual pitches from the injury and control periods, respectively, while corresponding LOESS lines show smoothed trends across those pitches. The gray dashed line marks the pitcher-specific 95th percentile of the control MD distribution, and the red dashed line marks the injury pitch. Panel A shows pitchers injured on fastballs (FF), and Panel B shows those injured on off-speed pitches (SL or CH). CH, changeup; FF, four-seam fastball; MD, Mahalanobis distance; SL, slider.
Fastballs Variability Detection Analysis
Overall, 339 pitches were included in the PCA. Six of 7 pitchers exhibited cumulative MD sums exceeding the 95th percentile variability threshold of their control distributions, indicating significant short-term mechanical variability prior to injury (P < .001) (Table 4). Pitcher 3 was the only exception, with a lead-up MD sum that remained below the threshold. This was in contrast to the matched controls who exhibited only 1 out of 14 pitchers with elevated cumulative mechanical deviation across the 5 preceding Fastballs with 938 pitches included in the PCA (Table 5).
Cumulative MD Analysis of the Five-Pitch Lead-Up Sequence for Case Pitchers (Fastballs Only) a

This table quantifies short-term mechanical variability in the five fastballs immediately preceding each pitcher's UCL injury. For each case pitcher, MD values for the five fastballs immediately preceding the injury pitch were summed to form a cumulative lead-up MD, which was compared with an individualized threshold derived from a rolling five-pitch MD distribution across control-period fastballs. “Above threshold” indicates whether the observed cumulative lead-up MD exceeded that pitcher-specific control 95th-percentile benchmark. Each pitcher's primary fastball was determined by their most commonly thrown type. Cumulative MD = sum of MD across the last five fastballs; Control MD 95% = 95th percentile of rolling five-pitch cumulative MD from controls; Above Threshold = Yes/No. FF, four-seam fastball; MD, Mahalanobis distance; SI, sinker.
Cumulative MD Analysis of the Five-Pitch Lead-Up Sequence for Control Pitchers (Fastballs Only) a
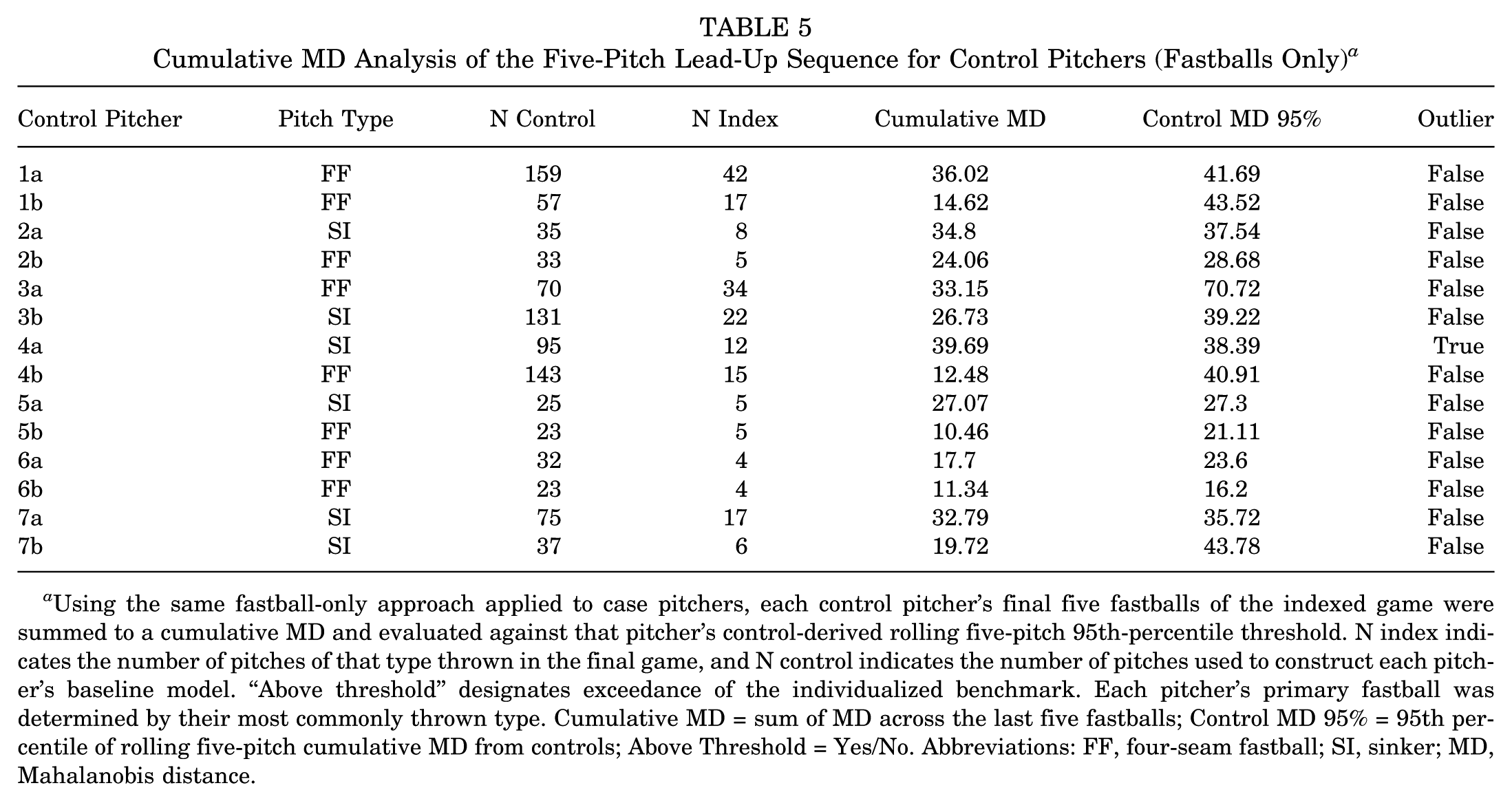
Using the same fastball-only approach applied to case pitchers, each control pitcher's final five fastballs of the indexed game were summed to a cumulative MD and evaluated against that pitcher's control-derived rolling five-pitch 95th-percentile threshold. N index indicates the number of pitches of that type thrown in the final game, and N control indicates the number of pitches used to construct each pitcher's baseline model. “Above threshold” designates exceedance of the individualized benchmark. Each pitcher's primary fastball was determined by their most commonly thrown type. Cumulative MD = sum of MD across the last five fastballs; Control MD 95% = 95th percentile of rolling five-pitch cumulative MD from controls; Above Threshold = Yes/No. Abbreviations: FF, four-seam fastball; SI, sinker; MD, Mahalanobis distance.
None of the 6 pitchers with ≥3 qualifying fastballs in the injury game demonstrated a statistically significant trend (all P > .05; Table 6). Pitcher 7, who threw only 2 fastballs prior to the injury pitch, did not meet the minimum requirement for correlation analysis and was therefore excluded from statistical testing (P value reported as not applicable). These findings indicate that, although cumulative variability (Table 4) is frequently elevated, it does not consistently present as a monotonic increase in MD on a pitch-by-pitch basis.
Spearman Correlation (ρ) Between MD and Pitch Order in the Five-Pitch Lead-Up Sequence (Fastballs Only) a

This table evaluates whether mechanical deviation progressively increased across the pitches immediately preceding UCL injury. Spearman's rank correlation coefficient (ρ) was calculated between MD and pitch order (1-5) for each case pitcher with at least three qualifying fastballs. Pitcher 7 threw only two qualifying fastballs and was therefore excluded from correlation testing (p = NA). FF, four-seam fastball; MD, Mahalanobis distance; SI, sinker.
Biomechanical Trends Preceding Injury
z-scores were calculated for 5 key biomechanical features—velocity, spin rate, release extension, arm angle, and acceleration magnitude—standardized independently by pitcher and pitch type, using control period baselines. These standardized metrics are summarized in Figures 2 and 3 for the injury game.

Pitch-by-pitch mechanical Z-score heatmaps leading to acute UCL injury. This figure visualizes pitch-by-pitch mechanical deviations for the seven case pitchers in the sequence immediately preceding and including the injury pitch. Each of the seven panels represents a single pitcher. The y-axis (mechanical feature) lists the five core kinematic metrics, and the x-axis (pitch sequence) is chronological, from T-5 (five pitches prior to injury) through the injury pitch itself. Each cell value is a Z-score quantifying deviation from the pitcher's baseline for that specific feature. Z-scores were calculated by standardizing each pitch relative to the pitcher's control period, within pitch type (e.g., a fastball was compared only to other fastballs) to normalize for type-specific variability. Red shading indicates positive deviations from baseline; blue shading indicates negative deviations.

Mechanical z-score profile at the injury pitch for case pitchers. This figure summarizes per-feature mechanical deviations at the specific injury pitch for each of the seven case pitchers (Pitchers 1-7). Each column represents one of the five core kinematic features, and each cell displays the Z-score for that feature on the injury pitch. Z-scores were computed relative to each pitcher's individualized control baseline derived from the four most recent pre-injury outings and standardized within pitch type. Red shading indicates positive deviations from baseline; blue shading indicates negative deviations.
In the 5 pitches preceding injury, each pitcher displayed a distinct trajectory across the 5 analyzed features, with no consistent directional trends. No systematic progressive increases or decreases were observed in any of the measured variables. Instead, preinjury kinematic data exhibited multidimensional variability without a uniform pattern across players.
Despite the lack of consistent progressive trends, substantial deviations were consistently observed between the final preinjury pitch (T-1) and the injury pitch. All 7 pitchers showed marked velocity suppression at the injury pitch (mean drop, 2.1 SD from the preceding pitch). A consistent acute decrease in arm angle was also observed at the injury pitch across all pitchers (mean decrease, 1.5 SD from the preceding pitch).
At the moment of injury, velocity and arm angle consistently deviated from the pitcher's baseline, while other features varied considerably: velocity was universally suppressed, with 6 of 7 pitchers >1.5 SD below baseline. Arm angle was also more often decreased, with 2 of 7 pitchers exceeding a 1.5-SD reduction. Four pitchers exhibited notably reduced extension (>1.5 SD below baseline), while 2 showed moderate increases. Acceleration magnitude ranged widely (–2.1 to +3.0 SD), with only 2 pitchers exceeding ±1.5 SD. For spin rate, there were minimal deviations overall, except for 1 pitcher (pitcher 5; –4.1 SD).
Discussion
The major findings of our study demonstrated 3 consistent biomechanical patterns at the moment of acute UCL rupture. First, every injury pitch (7/7; 100%) was a mechanical outlier, exceeding the 95th percentile MD threshold derived from each pitcher's control distribution. Second, cumulative variability was elevated in 6 of 7 pitchers (86%), as their 5 fastballs preceding injury surpassed the control-derived threshold for instability. Third, the injury pitch itself was consistently characterized by suppressed velocity (6/7; >1.5 SD below baseline) and reduced arm angle (mean, 1.5-SD drop from the previous pitch). In contrast, none of the matched controls exhibited an outlier final pitch, and only 1 of 14 (7%) showed elevated cumulative variability across the 5 preceding fastballs. Collectively, these findings suggest that acute UCL failure represents a distinct biomechanical phenotype characterized by abrupt in-game decompensation, rather than a gradual decline over multiple prior outings.
Velocity suppression on the injury pitch (6/7 pitchers >1.5 SD below their baseline) likely reflects kinetic chain disruption following ligament rupture. The UCL provides critical medial-elbow stability and resists valgus stress during throwing. 32 Loss of this support, especially during the late cocking and early acceleration phase, may impair force transmission, resulting in decreased pitch speed. Simultaneously, every pitcher exhibited a lower-than-baseline arm angle on his injury pitch, averaging a 1.5-SD drop from the previous pitch. Such an acute decrease could represent neuromuscular compensation for sudden joint instability or, alternatively, a final kinematic deviation that precipitated the tear. Prior work has linked chronically lower arm angles to elevated UCLR risk,6,9,29,37 but those studies used season- or career-level data rather than pitch-level resolution.
Whiteside et al 37 found reduced horizontal release and higher mean pitch speed to predict UCLR, while Portney et al 29 showed that more horizontal release points independently raise reconstruction risk. Mastroianni et al, 24 performed the most recent and comprehensive analysis on pitch-tracking data, finding no difference in horizontal release points or horizontal approach angles between cases and uninjured matched controls. However, these metrics are mostly a proxy of arm angle, measuring the ball's location at the time of release relative to home plate, and thus do not directly analyze the pitcher's arm angle. Arm angle data were not released publicly by MLB at the time. Dong et al 9 demonstrated that each 10° increase in arm angle adds roughly 4.23 N·m of varus torque. While causality cannot be confirmed, pitch-tracking findings in our study suggest that an acute drop in arm angle, possibly due to fatigue, motor breakdown, or mechanical compensation, may be an indicator of UCL injury. 2 This is in contrast to pitchers with more subacute or chronic presentations who demonstrate a trend of higher arm angles immediately prior to injury list placement (Supplementary Table 1), perhaps as a compensatory mechanism that results in decreased valgus stress and improvement of symptoms.
Intriguingly, even though a CH normally produces far less valgus stress than FF, SL, or curveball,13,16 2 of the 7 pitchers in this cohort sustained UCL injuries on a CH rather than on a higher-stress FF thrown earlier in the same outing. This paradox suggests that once the ligament is primed for failure, even a “lower-stress” pitch can trigger failure. This is supported by previous pitch-specific research, with Mastroianni et al 25 finding pitch-specific associations with UCL surgery compared with uninjured matched controls. Higher velocity, superior ability, and command of CH were all found to be risk factors for UCL injury. 25 Our study suggests that even lower stress pitches such as the CH can potentially contribute to injury.
Beyond the moment of failure, acute UCL injuries frequently appeared to follow a period of short-term mechanical variability. In 6 of 7 pitchers, the cumulative MD across the 5 FFs preceding injury exceeded the 95th-percentile threshold derived from control distributions. The absence of a linear trend across those 5 pitches indicates that volatility, rather than monotonic drift, characterizes the lead-up to injury. This aligns with broader performance declines reported before UCLR: Mayo et al 26 documented drops in velocity and spin over the 15 games before surgery, whereas the present analysis compresses that decline into a single outing. Moreover, workload and variability studies support this concept: Fleisig et al 14 reported that younger pitchers throwing >100 innings per year face significantly higher injury risk. DeFroda et al 8 reported that small increases in FF velocity drive higher tear rates, especially early in the season. Van Trigt et al 34 used simulations to demonstrate that pitchers with greater within-participant load variability under fatigue are more likely to exceed the UCL injury threshold. Collectively, these data suggest that short-term mechanical volatility, when superimposed on chronic stressors, may precipitate ligament overload.
While recent investigations into nonpitch metrics, such as a pitcher's control and success,17,24 have also been tied to elevated UCL risk, most existing research emphasizes long-term risk factors. Without distinguishing acute and chronic injury presentation, these studies cannot detect sudden in-game biomechanical deviations and often yield conflicting conclusions in terms of predictive trends. For example, while increased FF velocity is widely accepted as a major driver of UCL injuries,5,26,30 Chalmers et al 5 found that even when combined with secondary predictors such as higher weight and younger age, only 7% of variance in UCLR rates could be explained. Keller et al 19 concluded that pitch velocity alone is not a risk factor for UCLR. These inconsistencies, even around what is considered the primary contributor to injury, highlight the need for more definitive explanations into the mechanism of injury. Mastroianni et al 24 analyzed pitching trends in the years prior to injury finding that yearly increases in overall pitching ability (pitching+) were associated with UCL surgery, providing insight into how changes even on a seasonal level can predispose to injury. Analyzing pitching trends immediately before injury gives us potentially even more valuable insight into how acute changes in a pitcher's repertoire can influence injury risk.
By focusing exclusively on pitchers with acute injury presentation and leveraging Statcast's high-resolution pitch-tracking data, the present analysis identified immediate, multidimensional deviations at the failure moment—insights not observable when acute and chronic cases were mixed. Real-time deviation from an individual's baseline may thus offer a complementary risk signal, especially when such deviations accumulate across multiple pitches. Because variables such as velocity, spin rate, release extension, and arm angle are already tracked in real time during every MLB game, this framework could form the basis for in-game surveillance tools. By continuously comparing each pitch with a pitcher's recent baseline, automated alerts could flag patterns of mechanical variability, such as cumulative MD exceeding a defined threshold, enabling medical or coaching staff to intervene before injury occurs. Although still preliminary, this individualized approach holds promise for early warning systems capable of detecting risk within a single outing.
Limitations
This study has several limitations that warrant consideration. First, the sample size of overall pitchers was small (N = 7), although the sample size of total pitches was more reasonable, reflecting the strict inclusion criteria required to isolate acute, in-game UCL injuries with complete Statcast data. While the consistent findings across cases support internal validity, the limited cohort size constrains generalizability and precludes subgroup analysis. These results should be interpreted as descriptive rather than predictive. Very short control sets (eg, pitcher 6 CH analysis, n = 5; pitcher 5 CH analysis, n = 13) reduce the stability of MD thresholds. Although sensitivity analyses using stricter outlier cutoffs confirmed each injury pitch as an outlier, larger data sets are needed to validate these findings.
Additionally, Statcast data capture only external kinematic features and does not provide direct insight into internal joint loading or ligamentous strain. Although MD offers a sensitive composite measure of mechanical deviation, it remains an indirect proxy for tissue-level stress. Additional tools, such as wearable sensors, on-field motion capture, or kinetic modeling, may enhance future interpretations.
Finally, although the present study focused on acute injury events, many UCL injuries evolve along a continuum from chronic degeneration to sudden failure. Reliance on publicly reported injury details may introduce misclassification bias, particularly in distinguishing acute from subacute presentations. The extent to which short-term mechanical instability can detect progressive or evolving UCL pathology remains unclear. Further research is needed to determine whether the patterns observed in this cohort extend to other types of UCL injury.
Conclusion
Our study demonstrated that acute UCL injuries in MLB pitchers are often preceded by identifiable changes in key pitch-tracking metrics. Rather than a prolonged deterioration across outings, acute UCL failure may reflect a distinct biomechanical pattern marked by short-term variability and abrupt decompensation within the injury game. These findings provide the first pitch-level characterization of UCL failure and may support future in-game risk-monitoring strategies. However, future studies are needed to help understand these warning signs and prevent UCL injury.
Supplemental Material
sj-docx-1-ojs-10.1177_23259671251389226 – Supplemental material for Using Pitch-Tracking Metrics to Identify Warning Signs Immediately Prior to Acute Ulnar Collateral Ligament Injuries in Major League Baseball Players
Supplemental material, sj-docx-1-ojs-10.1177_23259671251389226 for Using Pitch-Tracking Metrics to Identify Warning Signs Immediately Prior to Acute Ulnar Collateral Ligament Injuries in Major League Baseball Players by Morgan R. Dillon, Michael A. Mastroianni, Nicholas Frappa, Kristen Nicholson, Matthew R. LeVasseur, Andrew J. Luzzi, Frank J. Alexander, Robert Ablove and Christopher S. Ahmad in The Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted August 30, 2025; accepted September 2, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.S.A. receives royalties and consulting fees from Arthrex; he also serves as the head team physician of the New York Yankees. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study was deemed exempt from the need for ethical approval.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.