
Abstract
Background:
Acute traumatic patellar dislocations may cause intra-articular derangements of the knee in the setting of acute and chronic instability which may not always be appropriately identified on magnetic resonance imaging (MRI).
Purpose:
To determine the rates of coexisting intra-articular pathology in patients with patellar instability requiring medial patellofemoral ligament (MPFL) reconstruction and to report discrepancies between preoperative magnetic resonance imaging (MRI) findings and diagnostic arthroscopy results.
Study Design:
Cohort study (Diagnosis); Level of evidence, 3.
Methods:
Patients who underwent MPFL reconstruction at a single institution between 2010 and 2023 were identified. Operative reports and preoperative MRIs were reviewed. Records without full MRI reports as read by a radiologist or cases in which a diagnostic arthroscopy was not conducted were excluded. Intra-articular pathologies noted on MRI and confirmed by arthroscopy were documented. MRI findings were considered to be discordant from arthroscopic findings if a lesion was identified on diagnostic arthroscopy that was not present in the full MRI report and that lesion resulted in additional surgical procedures.
Results:
There were 331 arthroscopic procedures conducted within the study population of 508 patients who underwent diagnostic arthroscopy at the time of their patellar stabilization procedures. These procedures included 180 loose body removals, 95 osteochondral lesions treated via a variety of interventions including open reduction and internal fixation (26 cases), particulated allograft chondral grafting (30 cases), osteochondral allograft transplantation (9 cases), and microfracture (30 cases), and 39 meniscal tears resulting in 33 partial meniscectomies and 6 meniscal repairs. Among these 508 patients, 105 (21%) demonstrated discordance of preoperative MRI and arthroscopic findings that necessitated additional procedures. This discordance was responsible for a total of 109 (33%) of the 331 arthroscopic procedures. These included 75 loose body removals, 2 osteochondral fracture fixation procedures, 2 microfractures for full-thickness cartilage loss, 16 partial meniscectomies, and 2 meniscal repairs, among others.
Conclusion:
Among patients undergoing patellar stabilization, 21% had intra-articular lesions not identified on preoperative MRI detected at the time of diagnostic arthroscopy that resulted in surgical intervention. This study, representing the largest cohort to date of patellar stabilization surgeries with both MRI and arthroscopy findings, underscores the importance of diagnostic arthroscopy for improving diagnostic accuracy and addressing associated intra-articular pathology.
Acute traumatic patellar dislocations can lead to recurrent symptoms of patellar instability in 15% to 80% of patients. 12 Preoperative magnetic resonance imaging (MRI) reveals rupture of the medial patellofemoral ligament (MPFL) and provides a static snapshot of articular derangements sustained from dislocation events before the study date. 3 However, patellar instability patients often have recurrent subluxations, which are described as “collapsing or shifting” events that provide ongoing potential for further damage.3,12 A 2007 cohort study of 38 adolescent patients with patellar instability 5 reported on diagnostic arthroscopy for patients undergoing patellar stabilization procedures. They recommended routine arthroscopic evaluation, as 20% of patients had nonpatellofemoral diagnoses at the time of arthroscopy that resulted in 5 additional procedures being conducted (4 partial meniscectomies and 1 meniscal repair). A study conducted by Shultz and associates 10 found that among patients with patellar instability undergoing isolated MPFL reconstruction without MRI findings of intra-articular pathology, 35% had findings on diagnostic arthroscopy that were not identified on preoperative MRI. However, the sample size was limited, patients who underwent tibial tubercle osteotomy at the time of MPFL reconstruction were excluded, imaging was reviewed by treating surgeons and not radiologists, and discordance between MRI and arthroscopic findings was not the primary focus.
Therefore, the purpose of the present study was to determine the rates of coexisting intra-articular pathology in patients with patellar instability undergoing patellar stabilization surgery, elucidate any discordance between preoperative MRI findings and diagnostic arthroscopic findings that led to additional procedures performed at the time of index surgery, and identify if the discordance rate is affected by the time from MRI to surgery.
Methods
In this retrospective case series, chart review was conducted to identify all patients with patellar instability who underwent primary MPFL reconstruction at a tertiary care center between 2010 and 2023. The full MRI report, the date the MRI was obtained, and the findings on the MRI report were documented. The operative note was queried, and findings and procedures conducted during the diagnostic arthroscopy were recorded and documented. Patients were included if they had an MPFL reconstruction performed by a fellowship-trained sports surgeon within the study dates. Patients were excluded if they did not have a preoperative MRI with a full imaging report from a radiologist or if a diagnostic arthroscopy was not conducted at the time of MPFL reconstruction. Arthroscopic findings were compared with MRI findings, and discordance was defined as cases where an additional procedure was conducted to address intra-articular pathology identified during diagnostic arthroscopy that was not included on the formal MRI report. The quantity and types of these discordant events were recorded. Given the ambiguity and surgeon-to-surgeon variability in the conducting of shaving chondroplasties, this procedure was excluded. To mitigate bias, any questionable discordant findings were flagged for review by another author (A.J.T. or V.R.T). MRIs were categorized as those taken ≤90 days prior to the date of surgery and those obtained >90 days from the surgical date. The 90-day grouping was selected in line with previous papers evaluating MRI and arthroscopic discordance. 13 Rates of discordance were identified within each of these groups and compared with the overall rate of discordance in MRI and arthroscopic findings within the study population. A chi-square test was used to identify any significant difference in discordance rates between these 2 groups, with significance defined as P < .05.
Results
Of a total of 640 patients identified between 2010 and 2023, 508 patients met our inclusion criteria. Median age was 20, and 65% of patients were female. Of the initial 640 patients, 132 were excluded, as no full MRI report from an attending radiologist was present in the chart. Additional arthroscopic procedures were common at the time of MPFL reconstruction, which reflected the frequency of concomitant pathology with patellar instability; these additional procedures were characterized as planned if they were supported by the preoperative MRI and discordant if the pathology addressed was not identified on the preoperative imaging report. This cohort of 508 patients had a total of 331 arthroscopic procedures conducted. The most common procedure was loose body removal (n = 180). Osteochondral lesions were treated with open reduction and internal fixation in 26 cases, particulated allograft chondral grafting with Denovo NT Graft (Zimmer Biomet) in 30 cases, osteochondral allograft transplantation in 9 cases, and microfracture of a chondral defect in 30 cases. Partial meniscectomy was performed in 33 cases, meniscal repair was performed in 6 cases (including a repair of a bucket-handle meniscal tear, a repair of a medial meniscus root tear, and a repair of bilateral posterior horn tears). Finally, in 17 cases a limited synovectomy was performed (Table 1).
Total Arthroscopic Procedures Conducted and Procedures Missed With MRI Read Alone a
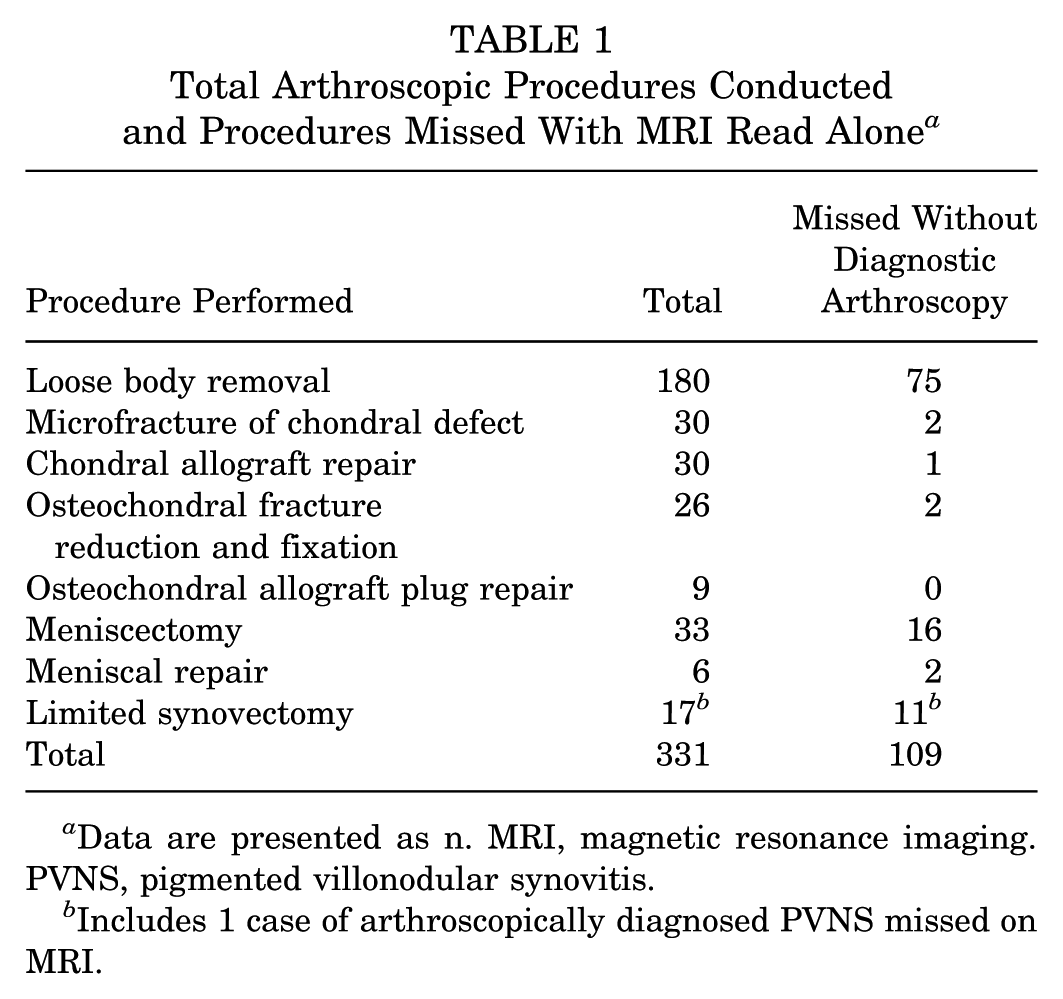
Data are presented as n. MRI, magnetic resonance imaging. PVNS, pigmented villonodular synovitis.
Includes 1 case of arthroscopically diagnosed PVNS missed on MRI.
Among these 508 patients, 105 (21%) were identified in which 109 unplanned additional procedures were performed at the time of diagnostic arthroscopy to treat pathology not identified on preoperative MRI. These 109 arthroscopic procedures consisted of 75 loose body removals, 2 osteochondral fracture fixation procedures (one located on the lateral femoral condyle and the other on the patella), 1 particulated allograft chondral grafting procedure (conducted as unplanned treatment for a second lesion on the medial femoral condyle not identified on preoperative MRI), 2 microfractures for full-thickness cartilage loss (lateral femoral condylar 10 × 3–mm lesion; lateral femoral condylar undocumented size), 16 partial meniscectomies (3 medial, 13 lateral), 2 meniscal repair procedures (1 horizontal cleavage tear and 1 vertical tear at the root/posterior horn junction both conducted on lateral menisci), and 10 limited synovectomies conducted for impinging synovium (directly anterior in 3 cases, anterolateral or lateral in 4 cases, and anteromedial in 3 cases), as well as 1 arthroscopic diagnosis of pigmented villonodular synovitis who ultimately required 3 additional procedures (1 manipulation under anesthesia and 2 extensive synovectomies) (Table 1).
Among the 508 patients included in the study, 49 patients had MRI reports with no intra-articular pathology documented. Of these patients, 12 (24%) had findings on diagnostic arthroscopy that resulted in intervention. These procedures included 9 loose body removals and 3 limited synovectomies.
Patients who underwent an MRI within 90 days of surgery (62/321; 19%) and those who obtained an MRI >90 days from their date of surgery (46/187; 25%) did not demonstrate a statistically significant difference in rates of discordant findings (P = .03 and P = .16, respectively). Discordant findings identified among MRIs obtained >90 days from the day of surgery included 32 of 75 loose bodies not identified on MRI and 8 of 16 meniscal tears resulting in partial meniscectomy not identified on MRI. All discordant chondral pathology requiring arthroscopic intervention was identified in patients who had an MRI ≤90 days before their reconstruction.
Discussion
In 21% of patients with patellar instability undergoing patellar stabilization surgery, the MRI report did not identify intra-articular pathology that resulted in surgical intervention that would not have been addressed without utilization of diagnostic arthroscopy. Additionally, there was no significant difference in MRI and arthroscopic discordance between MRIs obtained ≤90 days before surgery and those obtained >90 days before surgery.
Among the 508 patients who underwent MPFL reconstruction for patellar instability, the most common associated pathology was loose bodies, present in 180 patients among the cohort of 508 (35%). Other studies describing arthroscopic findings at time of MPFL reconstruction also documented a high rate of loose bodies with rates reaching as high as 81%. 10 In our cohort, intervention for chondral damage that was more significant than shaving chondroplasty was the second most common arthroscopic procedure performed when aggregated, resulting in 95 of the 331 procedures performed.
Chondral damage, specifically patellar and trochlear chondral damage in patients with patellar instability, is a well-known lesion identified in 95% to 97% of patients with diagnostic arthroscopy at the time of MPFL reconstruction.4,7 Our findings are consistent with work conducted by previous studies, such as that from Sallay and associates, 8 who found osteochondral lesions involving the patella and lateral femoral condyle in 68% of patients with documented patellar dislocations. Other studies provided more granularity and demonstrated that in patients with documented patellar dislocation, 40% of patients had osteochondral lesions of the lateral condyle and >60% of patients had chondral or osteochondral lesions of the medial patella. 9 In a systematic review of patients with recurrent patellar dislocations, nearly 85% of patients demonstrated patellar chondral defects and nearly 28% of patients demonstrated trochlear chondral defects. 6 Cartilage damage found in our patients was variable in severity, demonstrating the importance of direct inspection to determine need for treatment, and the possibility of an osteochondral fragment amenable to repair.
While meniscal tears were rare within our cohort, there were 33 patients (6%) undergoing partial meniscectomy and 6 patients (1%) who underwent meniscal repair, suggesting that the meniscus should be critically evaluated at the time of surgery. Our study cohort had a lower rate of meniscal injury than previous literature, which documents the rate of meniscal tear as high as 11% to 21%.1,2 Recurrent patellar instability events may manifest for the patient as a major “giving way” of the knee with collapse and falls. This mechanism can put the meniscus at risk for tear. It is not uncommon for patients to report repeat events between timing of an office visit to review MRI findings and the actual surgical date. Obtaining repeat MRI scans between surgery scheduling and surgery would add cost and scheduling challenges, while still potentially providing a high rate of false negative findings based on the available literature, including the present study. 10
Previous studies that have characterized the pathology associated with patellar instability have reported similar results with much smaller sample sizes. Stanitski and Paletta 11 reviewed 48 adolescents with acute patellar dislocation and identified articular damage in 34 of 48 patients (71%) and loose bodies in 8 of 28 (29%) patients. A similar categorization of arthroscopic findings in adolescents with patellar instability was conducted in 2007 by Luhmann and associates, 5 which reviewed 38 patients and found patellar osteochondral lesions in 78%, loose bodies in 15%, and meniscal injuries resulting in either meniscectomy (n = 2) or meniscal repair (n = 1). In our study, we identified 95 cartilage procedures, which included microfracture, osteochondral fracture repair, osteochondral allograft plug transplantation, and use of particulated allograft chondral grafting. When loose body removals were included, that number increased to 109 of 331 procedures conducted within this cohort. The present study adds the largest cohort of patients to date reporting on concomitant procedures at the time of patellar stabilization surgery.
Within the present study, preoperative MRI findings failed in >20% of cases to identify pathology that required additional procedures performed at the time of patellar stabilization surgery. Failure to conduct a diagnostic arthroscopy at the time of patellar stabilization would have resulted in missing 42% of all loose bodies (75/180), 33% of all meniscal repairs (2/6), and 48% of meniscectomies conducted in this population (16/33). Similarly, 2 of 26 (8%) of the osteochondral fractures that underwent reduction and fixation and 1 of 30 (3%) of the particulated allograft chondral grafting (second lesion identified intraoperative not previously seen on MRI) would not have been conducted if MRI alone was utilized as a diagnostic tool. A salient point to note is that in the 49 patients identified without intra-articular pathology on preoperative MRI, 12 (24%) had arthroscopic findings requiring intervention. Relying on MRI alone would have resulted in missed ongoing intra-articular pathology for these patients at an unacceptably high rate. Shultz and associates 10 identified a discordance rate of 35% among patients undergoing isolated MPFL reconstruction who underwent diagnostic arthroscopy without intra-articular pathology identified on preoperative MRI. However, that study excluded patients undergoing associated tibial tubercle osteotomy and only included 41 patients in the diagnostic arthroscopy group.
Limitations
The present study is not without limitations. This study was conducted at a single institution, which limits the generalizability of these results. There are limitations given the retrospective nature of the study which limited data collection to what was recorded at the time of the procedure. As a result, other intra-articular pathology that may have also been missed on preoperative MRI but did not rise to the level of requiring surgical intervention may not have been documented. Furthermore, pathology that was treated and deemed to “require intervention” was based on the judgment of the treating surgeon and predicated on the belief that a failure to treat would have compromised the surgical outcome. For some treated lesions, including loose body removals, the size and characteristics of the loose bodies were not fully documented, which limits granular analysis of the treated pathology. This surgeon-to-surgeon variability and the lack of consistent documentation of all lesion sizes represents a limitation of the current study.
Conclusion
The most important finding of the present study is that 21% of patients had findings at the time of diagnostic arthroscopy that resulted in additional procedures that would not have been conducted based on the preoperative MRI alone. The present study demonstrates these findings in the largest cohort to date of patients undergoing patellar stabilization surgery examined with both MRI and diagnostic arthroscopic findings. The findings of the present study underscore the importance of performing a diagnostic arthroscopy at the time of patellar stabilization surgery to improve diagnostic accuracy and address associated intra-articular pathology.
Footnotes
Final revision submitted July 27, 2025; accepted August 26, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.R.D. has received royalties from Smith & Nephew; consulting fees from DePuy Synthes and OsteoCentric Technologies; and a grant from Zimmer, Moximed, and Aesculap. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Virginia Institutional Review Board for Health Sciences Research (study No. 16911).