
Abstract
Background:
Osgood-Schlatter Disease (OSD) is an overuse injury causing pain and inflammation at the tibial tubercle, usually in skeletally immature patients. Various treatments are available, including surgical and nonsurgical approaches.
Purpose:
To review the literature focusing on the clinical outcomes of different treatments for OSD.
Study Design:
Scoping review; Level of evidence, 4.
Methods:
Under PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a search was performed in June 2024 with PubMed, Embase, and Cochrane Trials, totaling 349 initial articles. Data were collected on patient demographics, treatments, clinical outcomes, and complication rates. Bias was assessed using the methodological index for non-randomized studies and risk of bias 2.0 tools.
Results:
Fifteen studies encompassing 712 patients were included and categorized into nonoperative (n = 7), injection-based (n = 4), and surgical (n = 6) treatment groups. Among injection studies, full recovery rates ranged from 31.8% to 84.3%, with the Knee injury and Osteoarthritis Outcome Score and Tegner Activity Scale (TAS) scores as high as 94.3 and 6.3, respectively, after treatment. Dextrose and platelet-rich plasma injections demonstrated no reported complications. Nonoperative treatments, including physical therapy, immobilization, and supportive care, showed full recovery of activities of daily living (ADL) in 14.3% to 100% of cases. Complication rates for nonoperative treatments ranged from 0% to 66.7%, most commonly involving quadriceps atrophy and skin irritation. Surgical treatments were typically reserved for refractory cases and achieved return to ADL in 79% to 100% of patients. Postoperative Lysholm scores ranged from 96.9 to 99.0, and TAS scores ranged from 6.2 to 8.5. However, complications were reported in 5 of 6 surgical studies, with rates ranging from 0% to 75.8%, including infections, hypertrophic scarring, and residual pain.
Conclusion:
Our systematic review showed that nonoperative treatments are effective for managing OSD. Surgery, while rare, seems reserved for patients with closed growth plates who have persistent symptoms. This review highlights the need for additional studies to better identify the best nonsurgical treatment.
Osgood-Schlatter Disease (OSD) has a global incidence rate of 3.8 per 1000 people per year, commonly affecting adolescents and involving symptomatic pain in the anterior knee.15,35 It is a condition characterized by inflammation of the tibial tubercle, caused by repeated stress and chronic avulsion from the patellar tendon. OSD can result in serious complications, including increased posterior tibial slope, which may alter knee biomechanics, and secular recurvatum, often displayed in surgical cases.15,32 It was recently discovered that OSD may lead to permanent structural changes in young athletes, specifically at the proximal tibia, where reports have demonstrated an increased posterior tibial slope.10,27 While OSD is typically described as self-limiting and resolves as adolescents reach skeletal maturity, persistent cases may require intervention. 15 Nonsurgical treatments, including analgesics and physical therapy, are typically the first line of management, 9 although surgical procedures, including open techniques, may be considered for refractory cases. 3
Currently, there are gaps in the literature regarding the most effective treatment options for OSD, with no clear consensus on the best approach. This poses a challenge for primary care providers and sports medicine physicians to determine the optimal management strategy for their patients, especially when comparing nonoperative treatments with more invasive options. While surgical procedures such as ossicular excision are available, they are less frequently discussed because of the rare need for surgery in this patient population. 13 Although OSD often resolves once patients reach skeletal maturity, it is important to evaluate treatment strategies to ensure the optimal outcomes for patients.
This study aims to clarify the most effective treatment options for OSD through a systematic review of the available literature, focusing on both nonsurgical and surgical approaches. We will evaluate the clinical outcomes associated with various treatment modalities, with particular attention to randomized controlled trials (RCTs). We hypothesize that nonsurgical treatments are most effective in managing OSD symptoms, with surgical intervention reserved for patients who fail nonoperative and injection-based therapies, as supported by the rarity of surgical cases in the literature.
Methods
This systematic review adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 22 This review is original, as it was not previously registered with the International Prospective Register of Systematic Reviews.
Eligibility Criteria
We selected original research articles that provided outcomes for patients diagnosed with and treated for OSD. Exclusion criteria were as follows: duplicate studies, non-English publications, reviews or meta-analyses, case reports with <10 patients, commentaries, articles without full text, animal or cadaveric studies, letters to the editor, and protocols.
Search Strategy
In June 2024, 2 reviewers (L.C.M.N. and I.A.) conducted searches in PubMed, Embase, and Cochrane Trials. We initially included all articles from these databases since their inception. The search terms used included the following Boolean query: “Osgood-Schlatter AND treatment NOT review.” If there was remaining conflict or uncertainty among the 2 reviewers regarding inclusion, a third reviewer (D.W.G.) was consulted before making a final decision.
Data Collection
Data extraction and screening was carried out by 2 reviewers (A.A. and A.T.K.) using a standardized form. During the full-text review, various variables were collected, including the country of origin, level of evidence, total number of patients, outcomes/patient conditions before and after treatment, treatment specifics, treatment duration, and patient demographics. Bias was assessed according to the methodological index for non-randomized studies (MINORS) and the revised Cochrane risk-of-bias tool for randomized trials (RoB 2.0) criteria. The MINORS scale is out of 16 for noncomparative studies and 24 for comparative studies, where each individual item ranges from 0 to 2. 28 The RoB 2.0 framework assesses the quality of randomized studies based on 5 domains: bias arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each RoB 2.0 domain is rated as low risk, some concern, or high risk of bias. 30
Statistical Analysis
The study characteristics are outlined descriptively with reported means and ranges. All data are presented in a narrative manner.
Results
Search and Study Characteristics
A total of 349 articles were collected using the search criteria. After abstract screening, 33 full texts were reviewed for eligibility. Ultimately, 15 articles ¶ were included in this study (Figure 1). The MINORS and RoB 2.0 results demonstrated overall moderate-to-good quality and low bias for the included studies (Figure 2, Table 1).28,30 According to Table 2, 712 total patients of OSD were included in this systematic review. Of these, there were 490 male patients and 222 female patients, ranging in age from 12.3 to 23 years. The type of study varied, with 4 RCTs,18,31,32,36 2 prospective cohort studies,11,16 5 retrospective cohort studies,1,3,5,6,8 1 prospective case series, 23 and 3 retrospective case series.7,14,20 Only 12 studies reported a mean clinical follow-up, ranging from 6 to 66.1 months. # There were 9 studies that reported physical activities prior to injury,1,3,7,14,18,23,31,32,36 as listed in Table 2.
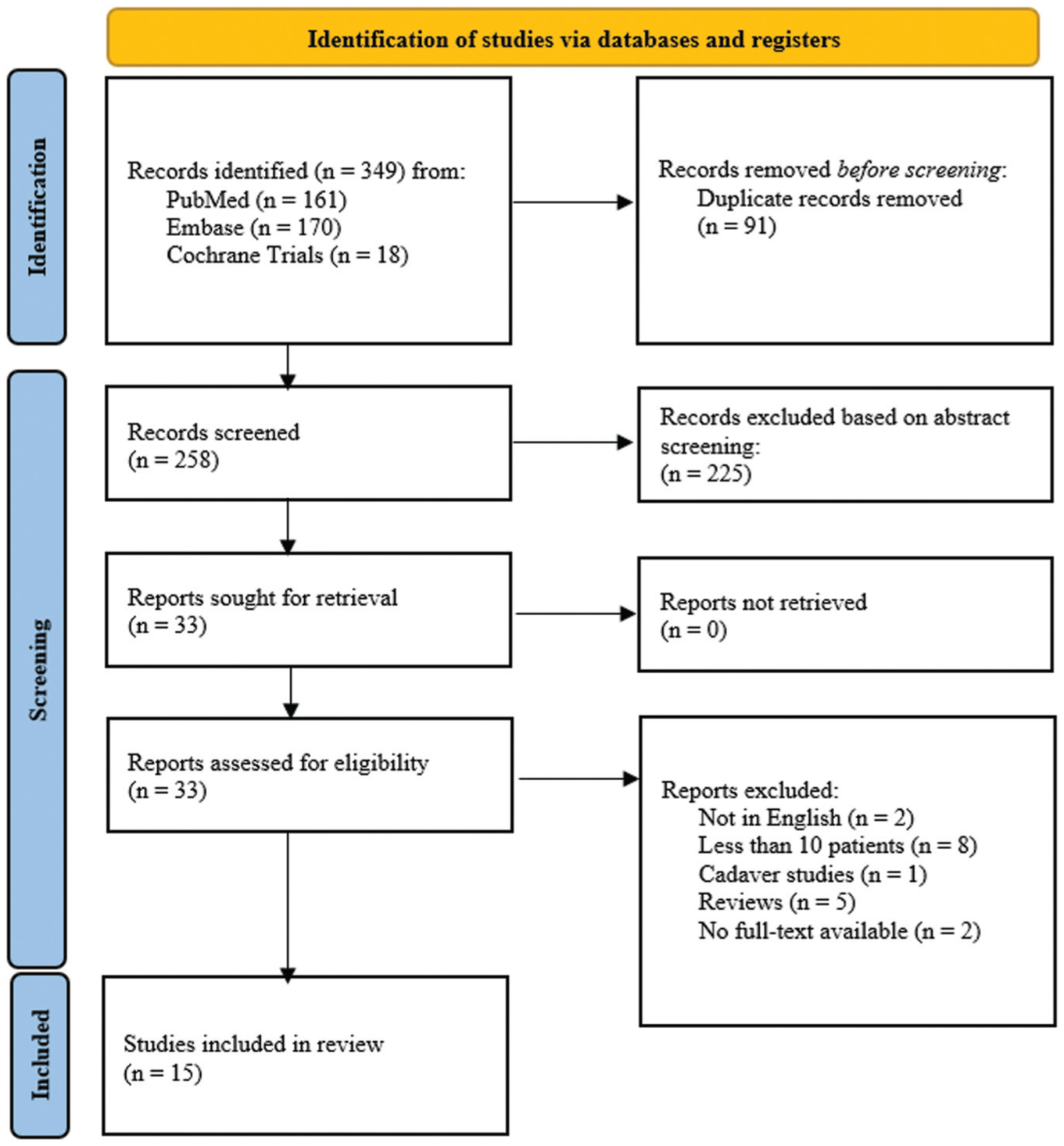
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of article identification, 22 exclusions in article screenings, and final inclusions for systematic review on comparing Osgood-Schlatter Disease treatments.

The revised Cochrane risk-of-bias tool for randomized trials results for the 4 randomized studies of this systematic review on Osgood-Schlatter Disease treatments. 3

MINORS, methodological index for non-randomized studies; dashes indicate no value reported.
Study Characteristics and Patient Demographics a

OSD, Osgood-Schlatter Disease; NR, not reported.
Surgical Treatments for OSD
Surgical approaches to OSD typically include removing or smoothing down the raised area of the tibial tubercle, removing the bursa and nearby irritated tissues, and/or removing loose ossicles and free cartilaginous pieces (sequestrectomy). In our review, 6 studies reported surgical treatment outcomes (Table 3).3,6-8,20,32 One study evaluated partial tibial tubercle excision, 8 1 examined a tibial sequestrectomy, 32 3 reviewed ossicular excisions,3,7,20 and 1 study involved a combination of patients who underwent either ossicular excisions or tibial tubercleplasty. 6 The studies involved 3 arthroscopic,3,20,32 1 bursoscopic, 7 and 2 open surgeries.6,8 Postoperative radiographic findings were reported in 5 studies,3,6,7,20,32 where 3 demonstrated successful ossicular removal3,6,20 and 2 did not7,32. Based on all 6 studies, the percentage of surgical patients who fully returned to activities of daily living (ADL) ranged from 79% to 100%. Arthroscopic techniques3,20 were associated with fewer complications and faster return to ADL compared with open procedures,6,8 which had higher rates of scarring and residual pain. In terms of patient-reported outcome measures, there were 2 surgical studies that reported a postoperative Lysholm Knee Score and Tegner Activity Scale (TAS) score,3,7 ranging on average from 96.9 to 99.0 and 6.2 to 8.5, respectively. The complication rate for surgical treatment, according to all 6 studies, ranged from 0% to 75.8%. From our radiographic findings, the OSD-related complications included ossicular separation in 23 knees after ossicular excision surgery, 20 then a prominent tubercle in 7 knees and sequestrae in 4 knees both after a tibial sequestrectomy (Table 3). 32 Complications were reported in 5 of the 6 surgical studies, ranging from superficial infections and hypertrophic scars to functional limitations such as recurvatum and loss of flexion. The majority of the studies on surgical treatment included in this review had a nonzero complication rate.6-8,20,32 Most common among these complications were infections at the surgical site as well as mobility and aesthetic issues related to postoperative scarring. El-Husseini and Abdelgawad 6 observed 1 case of a hypertrophic scar causing discomfort during kneeling, another case of a superficial wound infection that resolved with antibiotics, and 3 cases of persistent mild pain (2 of which had additional pathologies such as patellofemoral osteoarthritis and lateral patellar tilt). Similarly, Nierenberg et al 20 reported 1 keloid scar, residual pain in 1 patient, and temporary numbness at the surgical site in 3 patients. Eun et al 7 noted 1 superficial infection; 4 patients in their study reported difficulty kneeling postoperatively. One patient in the study performed by Flowers and Bhadreshwar 8 developed a superficial drain-site infection, which was resolved with antibiotics. Last, the patients in the surgical group of the study performed by Trail 32 included an enlargement of the bony prominence in 55% of the patients. Four of these patients had tubercles sufficiently large that they required subsequent surgical revision and shaving. One patient lost 10° of flexion in the operated knee as compared with the contralateral knee. Another patient developed 10° recurvatum (hyperextension of the knee joint). Additional complications included slight wound dehiscence at the surgical site in 1 case and superficial wound infection in another that left the patient with an unsightly scar. 32
Patient Outcomes After Surgical Treatment of OSD a

ADL, activities of daily living; NR, not reported; OSD, Osgood-Schlatter Disease.
Statistical significance compared with preoperative.
Injection Treatments for OSD
Injections for OSD were intended to reduce inflammation and pain by stimulating a healing response within irritated tissues. Options typically included hyperosmolar dextrose solution or platelet-rich plasma (PRP). The injections were administered at the tibial tubercle, typically under ultrasound guidance to ensure accurate placement at the patellar tendon insertion site, as described in the protocols by Nakase et al 18 and Wu et al. 36 In this systematic review, we discovered 4 studies involving injections11,18,31,36 (Table 4). Nakase et al recommended injection for patients with insufficient improvement in OSD symptoms after over a month of nonoperative treatments such as physical therapy, medication, and padding. Topol et al 31 focused on sports-related OSD pain persisting for ≥3 months despite following protocols such as structured and gradual hamstring stretching and quadriceps strengthening. Guszczyn et al 11 included children who underwent nonoperative treatment with persisting symptoms for ≥12 months, as surgery was not an option given unfused growth plates. Wu et al focused on adults and older adolescents with unresolved OSD symptoms after ≥1 month of nonoperative treatment. Three studies used hyperosmolar dextrose solution,18,31,36 and 1 used a leukocyte-rich PRP (LR-PRP) injection (Table 5). 11 Among injection types, PRP demonstrated the highest Knee injury and Osteoarthritis Outcome Score (KOOS) 24 at 94.3 and TAS score at 6.3, while dextrose injections18,36 showed comparable improvements with saline in the Victorian Institute of Sport Assessment for Patellar Tendon (VISA-P) questionnaire, suggesting the mechanical effect of needling may contribute to symptom relief. Lidocaine-only injections 31 were less effective, with a 46.2% recovery rate compared with 84.2% in the dextrose group. Nakase et al and Wu et al compared dextrose solution with saline injections, whereas Topol et al used both a lidocaine control and a supervised care group. Among all injection studies, 1 reported postinjection radiographic findings 11 ; radiographs continued to demonstrate an ossicle at the site of the tibial tubercle. The percentage of knees treated with dextrose, lidocaine, and LR-PRP injections that made a full recovery ranged from 31.8% to 84.3%,11,18,31 whereas those treated with saline fully recovered in 23.8% of cases. 18 Guszczyn et al reported mean KOOS and TAS scores after treatment as 94.3 and 6.3, respectively.
Criterion for recommending injections a

NSAID, nonsteroidal anti-inflammatory drug; OSD, Osgood-Schlatter Disease.
Patient Outcomes After Nonsurgical Treatment of OSD a

ADL, activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; LR-PRP, leukocyte-rich platelet-rich plasma; NR, not reported; OSD, Osgood-Schlatter Disease; RICE, rest ice compression elevation; VAS, visual analog scale; VISA-P, Victorian Institute of Sport Assessment for Patellar Tendon.
Statistical significance compared with pretreatment.
Two studies reported patient results with VISA-P after treatment.18,36 The VISA-P score measures a patient's freedom from pain and lack of disability due to afflictions of the patellar tendon, ranging from 0 to 100, where 100 represents optimal health and function. 12 They reported a mean posttreatment VISA-P score ranging from 50.8 to 83.2 for the saline injections and 76.2 to 85.7 for dextrose injections.18,36 Of the 3 injection studies that reported complication rates,11,18,36 patients who underwent injections had zero reported complications.
Nonoperative Treatments for OSD
Seven studies implemented nonsurgical treatments.1,5,14,16,23,31,32 Methods included immobilization,5,16,32 physical therapy,1,23,31 and other supportive measures,14,32 with recovery rates ranging from 67% to 100% across studies. The wide range in recovery rates is likely attributed to study differences in treatment duration, patient adherence, and adjunct therapies—for instance, Bezuglov et al 1 incorporated cryotherapy and magnetic field therapy, while Topol et al 31 relied solely on home-based stretching protocols.
There were 2 RCTs with nonoperative OSD treatments.31,32 Topol et al 31 reported nonoperative treatment with physical therapy for 3 months in children with a mean age of 13.3. Clinical follow-up was observed 12 months following treatment and full recovery of ADL of 14.3%. 31 Trail 32 treated participants with a mean age of 12.6 with extension plaster cast, ice, and physical therapy. This study reported clinical follow-up within a mean of 66 months following treatment and full recovery of ADL of 91%. A retrospective cohort method was used in 2 nonoperative studies.1,5 Bezuglov et al 1 utilized physical therapy for 1 month in participants with a mean age of 12.9, and clinical follow-up was reported within a mean of 6 months after treatment, with 100% full recovery of ADL. Duperron et al 5 included immobilization with resin cast in participants with mean age of 11.9 and indicated 67% full recovery of ADL following treatment. Case series were used in 2 nonoperative studies retrospectively and prospectively.14,23 Kireti et al 14 utilized a retrospective case series study in which participants with a mean age of 12.8 were treated with the RICE (rest-ice-compression-elevation) protocol and topical/oral analgesics. Clinical follow-up was reported within a mean of 12 months following treatment, with 86% full recovery of ADL. Rathleff et al 23 conducted a prospective case series study reporting participants with mean age of 12.7, treated with physical therapy for 3 months, and 69% full recovery of ADL following treatment. Levine and Kashyap 16 conducted a prospective cohort study on participants with mean age of 12.8, treated with an infrapatellar strap for 6 to 8 weeks. Outcomes indicated 79.1% full recovery of ADL, and clinical follow-up was not reported.
Immobilization protocols varied across studies. For instance, Duperron et al 5 used a cruromalleolar synthetic resin cast for 4 weeks, while Trail 32 applied an extension plaster cast combined with ice and physical therapy for a mean of 66 months of follow-up. Such immobilization methods aim to reduce strain on the knee. Physical therapy and exercise-based treatments involved structured programs with stretching, strengthening exercises, and a gradual return to activity. Rathleff et al 23 implemented a 12-week program divided into phases of activity reduction and progressive rehabilitation. Topol et al 31 provided individualized instruction on stretching and strengthening exercises with follow-up sessions. Bezuglov et al 1 incorporated quadriceps stretching exercises into therapy. Trail included physical therapy as part of an unspecified treatment protocol. Supportive measures for managing OSD included the use of rest, analgesics, and the RICE protocol (Kireti et al 14 ) and cryotherapy for inflammation and symptom relief (Bezuglov et al). Radiographs in some studies reported persistent ossicles after treatment (Duperron et al, Kireti et al, Trail), and complications such as quadriceps muscle atrophy or skin irritation from casting were documented in 4 studies, ranging from 0% to 66.7%. Table 6 summarizes the heterogeneous details of all nonsurgical treatments that did not involve injections.
Overview of Nonsurgical Treatment Options Without Injections a

RICE, rest ice compression elevation; OSD, Osgood-Schlatter Disease.
Three studies on nonoperative therapy included in this review had a nonzero complication rate.5,14,32 Duperron et al, 5 Kireti et al, 14 and Trail 32 reported complication rates of 66.7, 14.3, and 26.1, respectively. In Duperron et al’s study, muscle atrophy of the quadriceps occurred in 14 out of 30 patients, and dermabrasion or skin irritation was reported in 4 patients as a result of the immobilization device (a cruromalleolar synthetic resin cast). Excessive itching, skin erosion, and patellofemoral pain syndrome were also observed in the same study. 5 In Kireti et al’s study including nonoperative treatments such as the RICE protocol and topical and oral analgesics, 5 patients out of 35 experienced worsening OSD symptoms after treatment and elected to proceed with surgical intervention after the study. Trail noted that 6 out of 23 knees included in the nonoperative group treated with ice, physical therapy, and plaster casts appeared to have bony prominences at the tubercule at the follow-up (5 years and 6 months after treatment on average). It should be noted that Trail's study did not include a control group without nonoperative treatment, so it cannot be verified that the nonoperative treatment led to this prominence.
Discussion
The major finding of this systematic review demonstrated that nonsurgical treatments, especially injection-based ones, seem to have promising success in treating OSD. Nonoperative treatments, such as physical therapy and immobilization, demonstrated variable success, with full recovery rates ranging from 14.3% (Topol et al 31 ) to 100% (Bezuglov et al 1 ). Injection-based therapies, particularly LR-PRP, showed promising results with KOOS scores averaging 94.3 and no reported complications. 11 Surgical interventions, while effective in resolving symptoms in recalcitrant cases, were associated with higher complication rates, ranging from 0% (Circi and Beyzadeoglu 3 ) to 75.8% (Trail 32 ), and were primarily reserved for skeletally mature patients with persistent symptoms. The only previous systematic review of OSD reviewed studies published prior to 2019, and it did not review studies on surgical treatments or injections. 19
Injection Treatments
In our review, we found that injections can successfully improve OSD symptoms and have low complication rates. A 2021 systematic review concluded that the outcomes for injection-based management of OSD were unclear. 19 However, newer studies included in this review demonstrated improved outcomes for injection therapy.11,36 The previous systematic review highlighted conflicting results from RCTs conducted by Topol et al 31 and Nakase et al. 18 Topol et al found that hyperosmolar dextrose injections improve symptoms more effectively than lidocaine or usual care. Nakase et al found that both dextrose and saline improved OSD symptoms, with no significant differences in outcomes between the 2. Nakase et al proposed that the traumatic needling procedure of injections—rather than the type of solution injected—may promote a healing response via local inflammation.
In a more recent RCT, Wu et al 36 found similar results to Nakase et al. 18 Both the dextrose group and the control group who received saline injection experienced significant improvement in symptoms and function throughout the study without finding a statistically significant difference between the efficacy of hyperosmolar dextrose injections and the control solution. Wu et al and Nakase et al noted significant improvements in VISA-P scores after injections of either dextrose or saline. Wu et al found dextrose and saline to produce VISA-P scores of 50.8 and 76.2, respectively, whereas Nakase et al found values of 85.7 and 83.2, respectively. In both studies, these scores represented significant improvements in patellar tendon function compared with the pretreatment values. These studies indicated that the inflammatory response to the injection, rather than the specific therapeutic effect of the dextrose, may have contributed to the observed improvements.
A study by Guszczyn et al 11 intended to alleviate OSD symptoms by injecting LR-PRP. The therapeutic effects of LR-PRP are driven by the release of growth factors that promote tendon repair, collagen synthesis, and inflammation modulation. In a cohort of 152 knees, the injection group treated nonoperatively (with nonsteroidal anti-inflammatory drugs and physical therapy) and with LR-PRP outperformed the noninjection group receiving only standard nonoperative treatment. Patients treated with LR-PRP showed significant improvements in KOOS. At follow-up, which on average was 40 months after the initial injection, the mean KOOS score was 94.3, which is considered excellent.2,11 Additionally, the TAS scores for these patients also showed significant improvement. 26 The TAS scores of patients who received LR-PRP injections in Guszczyn et al improved significantly from 5.58 before treatment to 6.30 afterwards (Table 5). Overall, Guszczyn et al demonstrated that PRP combined with nonoperative therapy significantly outperformed standard care alone, with KOOS scores of 94.3 and a 72% full recovery rate, compared with lower recovery rates in noninjection nonoperative cohorts. 11
Guszczyn et al 11 found these significant improvements in OSD symptoms despite the persistence of ossicles on radiographic evaluation. Indeed, injections may work to improve OSD by improving degeneration at the patellar tendon without directly affecting the apophysis or ossicles that may be present. 31 Previous studies have demonstrated that some patients with OSD have become asymptomatic despite the persistence of nonunified ossicles. 25 These findings underscore the potential of injections as an effective treatment for OSD, perhaps best when combined with nonoperative treatments.
Our review demonstrated that injection therapy has lower complication rates compared with surgical treatment or nonoperative management (Tables 3 and 5). We found nonzero complication rates in 5 of 6 studies on surgical treatments,6-8,20,32 and 3 of the 7 studies on noninjection nonoperative treatments (which will be outlined in the following sections).5,14,32 In contrast, the 3 injection studies that reported complication rates had none.11,18,36
Nonoperative Treatments
In addition to injections, there are various nonsurgical treatments for OSD. These include physical therapy to strengthen quadriceps and improve flexibility and mobility, 23 immobilization of the knee to reduce strain on the tibial tubercle, 34 and the RICE protocol paired with analgesics to reduce acute inflammation and pain. 14 There were positive trends in patients returning to ADL across all of these protocols (Table 5). However, physical therapy literature displayed the greatest range in patient outcomes, boasting the highest and lowest ADL rates compared with other studies in this category. Specifically, patients in the Topol et al 31 study found a full recovery of ADL in just 14.3% of cases, compared with the 100% of cases that achieved this in Bezuglov et al 1 ’s study. One factor that may have led to this discrepancy is the follow-up period. Topol et al’s patients had a mean follow-up period of 12 months, whereas Bezuglov et al’s patients were assessed after only 6 months. These data suggest that the benefits of therapy may diminish after treatment. More research is needed on the long-term impact of physical therapy in treating OSD and the duration of sustained improvement.
Six of the 7 available studies on nonoperative treatment in our review did not report essential metrics of knee health,1,5,14,16,31,32 such as the KOOS, TAS, and VISA-P scores (Table 5), making it challenging to evaluate and compare the efficacy of any single technique. Despite our limited data set, the differences in outcome may likely be attributed to treatment duration, patient adherence, and whether protocols included supervised physical therapy or adjunct modalities such as cryotherapy.
Surgical Treatment
As shown in Table 7, surgery was indicated for skeletally mature individuals with persistent pain unresolved with nonoperative treatment with painful bursitis, radiographic evidence of a separated mobile issues fragment, and failure of nonsurgical management. 20 Athletes with unresolved OSD symptoms after 6 months of nonoperative treatment, particularly those with tibial tubercle and distal patellar tendon pain, were also candidates for surgical treatment. 3 A study recommended surgery for young, active patients, especially military recruits, with high visual analog scale pain score, focal tenderness over the tibial tubercle, anterior knee pain, and radiographic evidence of an ossicle, following a nonoperative treatment. 7 Another study recommended surgery for adults with persistent OSD symptoms such as anterior knee pain, presence of an ossicle, difficulty kneeling, and patellar ligament impingement by a tibial tubercle, despite nonoperative treatment. 6 Flowers and Bhadreshwar 8 recommended surgery for adults and adolescents whose OSD symptoms did not improve after 13.3 months on average of nonoperative treatments such as immobilization, analgesics, and restricted sports participation. According to our review, current literature on surgical treatment of OSD focuses on rare cases that do not resolve after a year or so of symptoms. A Johns Hopkins article 21 states that surgery for adolescent OSD patients is ill-advised because proximal tibial physeal closure is likely to resolve symptoms naturally. 4 A recent study reported that 90% of OSD nonoperative cases do not have symptoms into adulthood. 29
Criteria for Recommending Surgery a

NSAID, nonsteroidal anti-inflammatory drug; VAS, visual analog scale.
Most surgical studies in our review, 4 out of 63,6,7,20 (67%) contained patients with a mean age of ≥18 years. The surgical patients included in the studies conducted by Flowers and Bhadreshwar 8 and Trail 32 had mean ages of 17.4 and 13.8 years, respectively. However, these studies were published >20 years prior to the current review, which may explain their surgical focus—recent clinical protocols disfavor surgery in younger OSD patients. 21
While surgical treatment for OSD is rarely needed, it may be required when OSD symptoms recur after growth plate closure as seen in similar case reports of a 30-year-old woman and a 26-year-old male soccer player.17,33 As shown in Table 3, the surgical outcomes for Lysholm Knee and TAS scores were ≥85% in the Circi and Beyzadeoglu 3 study, with all patients having a successful arthroscopic ossicular excision and a total return to their previous ADL. This finding highlights the positive outcomes of surgery for OSD in adults. However, adults remain in the minority (10%) of those symptomatic with OSD. 29
Arthroscopic ossicular excision, as reported by Circi and Beyzadeoglu 3 and Nierenberg et al, 20 demonstrated the most favorable outcomes, with 100% return to ADL and no reported complications in Circi and Beyzadeoglu's cohort. These procedures were minimally invasive, allowed for precise removal of ossicles, and were associated with high Lysholm Knee (96.9) and TAS (8.5) scores. In contrast, open procedures such as those described by El-Husseini and Abdelgawad 6 and Flowers and Bhadreshwar, 8 while effective in symptom resolution, were associated with higher complication rates including hypertrophic scarring, residual pain, and superficial infections. Trail 32 reported the highest complication rate (75.8%) in patients undergoing tibial sequestrectomy, with issues such as recurvatum, loss of flexion, and wound dehiscence, suggesting that this technique may carry greater risk, particularly in younger patients.
While there were a variety of postoperative protocols, they were generally underreported. Studies with arthroscopic approaches, however, often emphasized early mobilization and shorter rehabilitation periods, which may have contributed to better functional outcomes.3,20 For example, Eun et al 7 used a bursoscopic approach and reported a 79% return to ADL with minimal complications, suggesting that less invasive techniques may reduce soft tissue trauma and facilitate recovery. In contrast, open procedures often required longer immobilization and were more likely to result in cosmetic or functional complications.6,8
Surgical management of OSD demonstrated a wide range of complication rates, from 0% to 75.8%, across our reported studies (Table 3). The most common surgical complications in our study included superficial infections,6,7 scar-related issues such as hypertrophic or keloid scars,6,20 and localized pain or tenderness. 32 Less frequent complications included numbness, 20 mild residual pain, 6 loss of knee flexion, 32 and recurvatum. 32 This variability in complications and rates highlights the complexity of surgical management and the need for refining these techniques to improve outcomes.
Limitations
This systematic review is not without limitations. Most of the included studies were retrospective in nature, which limited overall quality and introduced some bias. Due to heterogeneity in study design and outcome reporting, direct comparisons between surgical and nonsurgical treatments are limited to observable trends among the groups, but more high-quality articles on this topic are necessary for future meta-analyses and generalizability. Some studies also lacked standard deviations and ranges for their mean values, which limited the scope of our data. The patient demographics varied across studies and were not standardized by a meta-analysis. This prevented our ability to make definitive claims when comparing OSD treatments. Many studies did not report treatment outcomes (in particular, the nonsurgical studies), which further limited our analysis of the literature.
Conclusion
Our systematic review showed that nonoperative treatments are effective for managing OSD. Surgery, while rare, seems reserved for patients with closed growth plates and persistent symptoms. This review highlights the need for additional studies to better identify the best nonsurgical treatment.
Footnotes
Final revision submitted June 28, 2025; accepted July 16, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.W.G. has received consulting fees from OrthoPediatrics, nonconsulting fees from Arthrex and Synthes, and royalties from Arthrex and OrthoPediatrics Canada and serves as a consultant for Arthrex Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.