
Abstract
Background:
Medicaid coverage is associated with longer appointment wait times, poorer health outcomes, and decreased access to care compared with private insurance across multiple medical specialties. Currently, there is a paucity of data assessing the effect of Medicaid coverage on new patient access to care and appointment wait times for orthopaedic sports medicine surgeons.
Purpose:
To assess the effect of insurance status on patient access to care and appointment wait times for sports medicine–trained orthopaedic surgeons specializing in hip, knee, and shoulder arthroscopy.
Study Design:
Cross-sectional study.
Methods:
Sports medicine–trained orthopaedic surgeons were identified using the American Academy of Orthopaedic Surgeons patient-facing database, and physicians were categorized by joint specialization (hip, knee, or shoulder). Mystery callers posing as either Medicaid or Blue Cross/Blue Shield (BCBS) insured patients with a textbook presentation of a nonurgent hip, knee, or shoulder injury contacted physicians to request the next available new patient appointment. The number of business days until the first available new patient appointment was recorded and analyzed using a linear mixed model of Poisson regression.
Results:
A total of 1046 telephone calls were made to 523 unique orthopaedic sports medicine clinics in 48 states. Of the 385 included physicians, 129 (34%) did not accept Medicaid. Patients with Medicaid experienced a 20% longer wait time for a new patient appointment compared with patients with BCBS (incidence rate ratio [IRR], 1.20 [95% CI, 1.14-1.26]; P < .001), with median wait times of 13 days (IQR, 7-23 days) and 12 days (IQR, 6-20 days), respectively. Additionally, patients with Medicaid experienced increased wait times in specific geographic locations (P < .05) and a greater increase in wait times at academic institutions compared with private practices (IRR, 1.36 [95% CI, 1.13-1.62]; P = .001), with median wait times of 19 days (IQR, 15-22 days) and 14 days (IQR, 12-15 days), respectively. No significant difference in access to care or wait time was identified between hip, knee, and shoulder arthroscopic surgeons (P = .68). Our model achieved an R2 value of 0.93, demonstrating strong explanatory power.
Conclusion:
Patients with Medicaid experienced decreased access to care, with 34% of sports medicine–trained orthopaedic surgeons declining to accept Medicaid insurance. Among surgeons who accepted Medicaid, patients with Medicaid experienced slightly longer wait times for a new patient appointment compared with patients with private (BCBS) insurance. Additionally, patients with Medicaid experienced significantly longer wait times at academic institutions and in specific geographic locations. The present findings highlight a critical disparity in care, further underscoring the need for additional research to identify the cause and implement solutions.
The United Nations Department of Economic and Social Affairs has identified the expansion of health coverage and equitable access to quality health care as one of its priorities. 30 In the United States, states provide cost-effective health care to people with limited resources through a federally funded public insurance program called Medicaid. As of May 2024, nearly 73.8 million people are enrolled in Medicaid, with 40 states offering expanded benefits to adults aged <65 years with an annual income <133% of the federal poverty level. 19 Despite the large number of patients covered by Medicaid insurance, patients with Medicaid are less likely to use preventive health services and have decreased access to primary care physicians. 18 Additionally, patients with Medicaid are 3.3-fold less likely to have success when scheduling an appointment with a specialist compared with patients with private insurance. 16
Previous work assessing this issue in orthopaedic surgery has demonstrated decreased access to care and increased wait times for patients with Medicaid compared with their privately insured counterparts. A 2022 survey on physician appointment wait times and Medicaid acceptance rates for nonemergency diagnoses found that the mean Medicaid acceptance rate for orthopaedic surgeons in 15 metropolitan areas was 53%, with a mean appointment wait time of 16.9 days, a 33% increase from a previous survey in 2017. 21 In orthopaedic sports medicine, the current literature suggests that 31% to 54% of sports medicine–trained orthopaedic surgeons do not accept Medicaid, and patients with Medicaid experience increased wait times when presenting with emergent and nonurgent abnormalities.12,27,28,32
Audit studies, commonly referred to as “mystery caller” or “secret shopper” studies, effectively acquire objective data and insight into the challenges that patients face when accessing health care.17,26 Although audit studies have been previously conducted within the orthopaedic sports medicine realm to assess patient access to care and wait times based on insurance status, existing studies are dated and often confined to specific geographic locations or limited to individual clinical scenarios.12,27,28,32 To our knowledge, no study has evaluated new patient appointment wait times for sports medicine–trained orthopaedic surgeons to examine the effect of Medicaid insurance on access to treatment of hip, knee, and shoulder musculoskeletal abnormalities.
As a result, the present study aimed to assess the effect of insurance status on patient access to care and appointment wait times for sports medicine–trained orthopaedic surgeons specializing in hip, knee, and shoulder arthroscopy. We hypothesized that patients with Medicaid would experience decreased access to care and increased appointment wait times compared with patients with private insurance. Additionally, we hypothesized that there would be no difference in access to care or appointment wait times between hip, knee, and shoulder scenarios when controlling for insurance status. By examining the effect of insurance type on access to hip, knee, and shoulder arthroscopic surgeons, we aimed to identify inequities in access to care and propose solutions to ensure efficient and equitable care for all.
Methods
In this mystery caller investigation, we identified sports medicine fellowship–trained orthopaedic surgeons using the American Academy of Orthopaedic Surgeons (AAOS) patient-facing database. 2 Physician information was compiled from the AAOS patient-facing database, and physicians were categorized by joint specialization (hip, shoulder, or knee) and the United States Census Bureau division. Joint specialization was determined via a manual review of each physician's personal website. Surgeons were classified into the hip, shoulder, or knee group based on explicit statements indicating that they performed arthroscopy on the respective joint. Surgeons listing arthroscopy for >1 joint were randomly assigned to one of the eligible groups. Duplicate telephone numbers and addresses were removed. If physicians shared the same office location, only one physician was randomly selected to be included in the study to minimize administrative burden. Overall, 3 authors (N.A.F., E.G.-C., M.M.F.) screened each of the 672 randomly assigned physicians before starting data collection to weed out personal telephone numbers, confirm that physicians were currently practicing, and identify their respective joint specialization. After initial screening, 523 unique offices were identified and included for further data collection. There were 2 sets of calls made to each physician using the same scripted clinical vignette based on their respective joint specialization. During one call, the caller claimed to have private insurance from Blue Cross/Blue Shield (BCBS). In the other call, the caller asserted to be a Medicaid beneficiary. The caller's identity and the order in which the calls were made (BCBS vs Medicaid) were randomized. Clinical vignettes for each joint were selected based on common nonurgent diagnoses (Appendix 1).
A total of 10 callers participated in this study to conduct 1046 telephone calls. Each call aimed to ascertain the earliest available appointment time under the given scenario at the specified address. No appointments were scheduled, and no patient names or identifying information were used during telephone calls. The telephone calls were conducted during standard working hours, from 8:00 AM to 5:00 PM (excluding the 12:00-1:00 PM lunch hour) local time, for 1 week from July 29, 2024, to August 2, 2024. This 1-week call window was chosen to ensure that estimated appointment times were not influenced by prolonged intervals between calls or by potential seasonality in medical care.
Physicians were included if they were a practicing orthopaedic sports medicine surgeon and a fellow of the AAOS. Physicians were excluded if a telephone call to their office went to voicemail after 2 call attempts, the mystery caller was on hold for >5 minutes after 2 call attempts, the physician did not treat the condition described in the clinical vignette, the physician was not accepting new patients, incomplete physician information was obtained from the AAOS patient-facing database, an advanced practice provider appointment was required before a physician appointment, the physician belonged to a closed medical system, or the telephone call went to the physician's personal telephone number. Notably, we excluded physicians if an advanced practice provider appointment was required before a physician appointment to accommodate for variance in the number of advanced practitioners in any given practice, thus simplifying the study methodology.
Callers recorded the date of the earliest appointment time for each insurance type, hold time, total call time, and number of transfers. In addition, callers recorded if telephone calls were not answered, if the physician was no longer practicing, if the physician did not treat the conditions depicted in our vignettes, if they did not take Medicaid insurance, or if they required a formal referral before scheduling. If the caller was on hold for >5 minutes, a second call was attempted 24 hours later. If the caller remained on hold for >5 minutes on the second attempt, the call was deemed “unreachable” and excluded. If a call was not answered on the first attempt, a second call was attempted 24 hours later before the physician was deemed “unreachable.” The study design was standardized across all telephone calls, and caller training was performed before the onset of data collection to ensure that the results accurately reflect the target population. The 5-minute hold time was also chosen based on the “passing criteria” for Medicare organizations and Medicare/Medicaid insurers per the Centers for Medicare and Medicaid Services guidelines. 5
The mystery caller study received approval from the Colorado Multiple Institutional Review Board, which granted an exemption for obtaining informed consent. This exemption aligns with the mystery caller protocol, which restricts participants from providing informed consent before their involvement. However, after each call, a debriefing letter was dispatched to the participating practices (Appendix 2). This letter conveyed details about the call and its objectives, as well as the measures taken to ensure privacy, and provided contact information for the investigator and the Colorado Multiple Institutional Review Board.
Statistical Analysis
All analyses were conducted using R (Version 4.3.3; www.r-project.org). The time until the first available appointment was quantified as the number of business days elapsed from the initial call. A Poisson generalized linear mixed model with a log link was used to analyze the factors associated with the amount of time until the first available appointment. This model was chosen for its suitability in counting data. Physicians were considered random effects, allowing each physician to receive up to 2 calls with valid data.
Additionally, insurance type was included as a fixed effect while controlling for subspecialty, physician sex, age group, United States Census Bureau division, day of the week, and physician medical degree. A second model was created using an interaction term between joint specialization and insurance type to better understand the effect of insurance type. The choice of reference categories was based on the frequency of the category. These models were executed using the R package “lme4,” and estimated marginal means were calculated with the assistance of the “emmeans” package.
Results
Physician Characteristics
A total of 1046 telephone calls were made to 523 sports medicine–trained orthopaedic surgeons in 48 states who belonged to the AAOS. Of the 1046 telephone calls, 888 (84.9%) successfully reached a representative, while 158 (14.9%) were deemed unsuccessful because of prolonged hold times or no answer after 2 repeated attempts. Of the successful telephone calls, 55 (6.2%) did not correspond to the correct office location or physician specialty, 43 (4.8%) were not accepting new patients, 27 (3.0%) required a physician referral before scheduling an appointment, 6 (0.7%) required a patient to see an advanced practice provider before scheduling an appointment with the physician, and 2 (0.2%) were part of a closed medical system. For these reasons, 291 telephone calls resulted in 138 of 523 physicians meeting exclusion criteria (Appendix 3). Of the remaining 385 physicians meeting inclusion criteria, 129 (33.5%) did not accept Medicaid. Ultimately, 256 physicians provided a date for the first available new patient appointment.
Of the 385 physicians included, 120 (31.2%) specialized in hip surgery, 127 (33.0%) specialized in knee surgery, and 138 (35.8%) specialized in shoulder surgery. The median age of the physicians was 55 years (IQR, 48-62 years), they were primarily male (n = 368 [95.6%]), and most had graduated from an allopathic medical school (n = 377 [97.9%]) (Table 1).
Characteristics of Included Physicians a
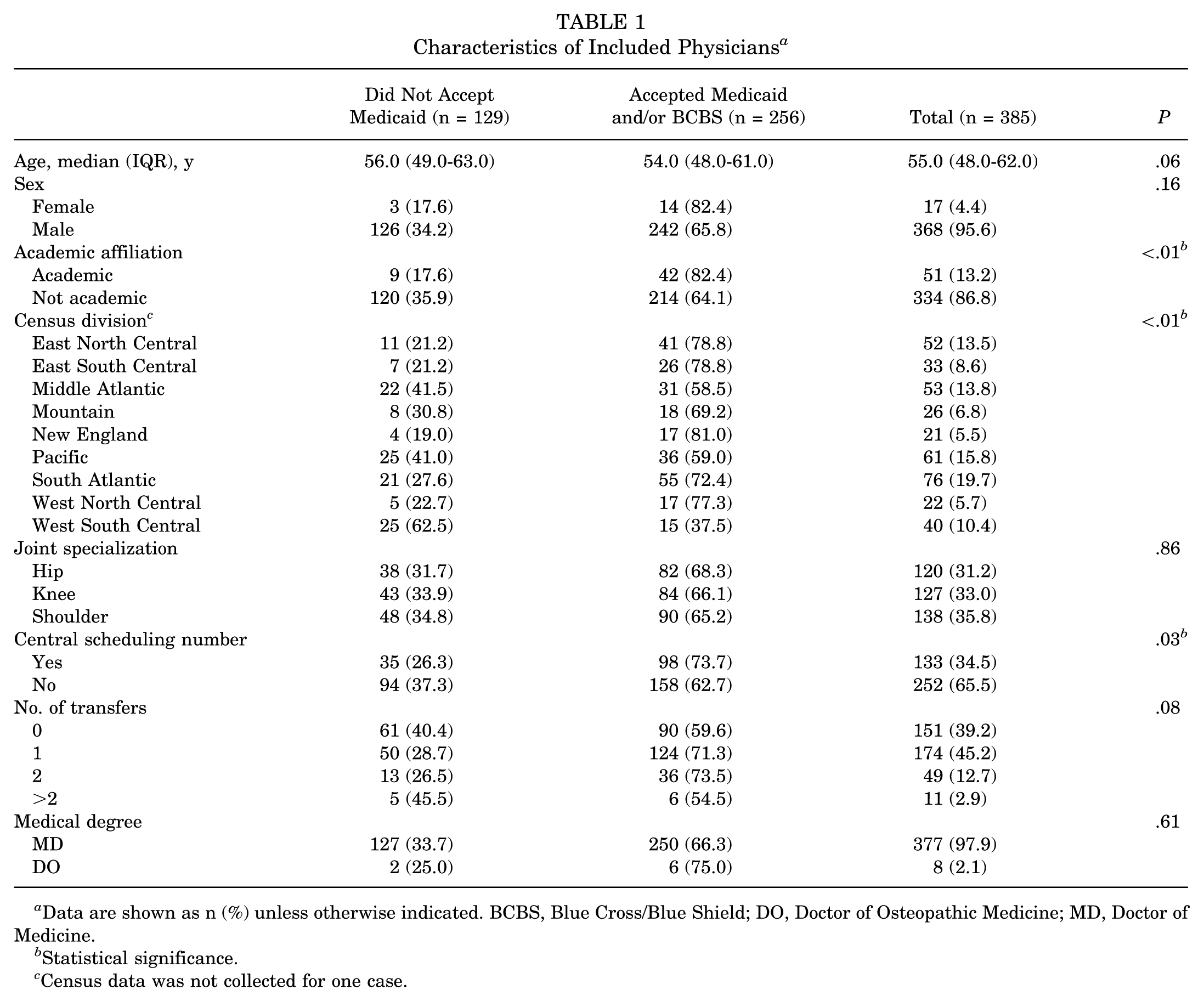
Data are shown as n (%) unless otherwise indicated. BCBS, Blue Cross/Blue Shield; DO, Doctor of Osteopathic Medicine; MD, Doctor of Medicine.
Statistical significance.
Census data was not collected for one case.
Univariate Analysis
Physicians who did not accept Medicaid were less likely to be affiliated with an academic institution compared with physicians who accepted Medicaid (P < .01) (Table 1). Additionally, certain geographic regions were associated with more physicians not accepting Medicaid (P < .01), and physicians who did not accept Medicaid were less likely to utilize a central call center (P = .03). No significant differences were observed in provider age (P = .06), medical degree (P = .61), joint specialization (P = .86), or number of transfers (P = .08) between physicians who accepted Medicaid and those who did not (Table 1).
Multivariate Analysis
The multivariate analysis encompassed data from 385 physicians who met the inclusion criteria for the study. This analysis aimed to identify factors significantly associated with the wait time for the first available new patient appointment with sports medicine–trained orthopaedic surgeons (Table 2). Notably, insurance type played a crucial role, with patients having Medicaid experiencing a 20% longer wait time compared with those with BCBS insurance (incidence rate ratio [IRR], 1.20 [95% CI, 1.14-1.26]; P < .001), with median wait times of 13 days (IQR, 7-23 days) and 12 days (IQR, 6-20 days), respectively (Table 2 and Figure 1). Patients seeking care at academic institutions experienced a median wait time of 19 days (IQR, 15-22 days), which was 36% longer than the median wait time of 14 days (IQR, 12-15 days) at private practices (IRR, 1.36 [95% CI, 1.13-1.62]; P = .001). Geographic location also significantly influenced appointment availability. Orthopaedic surgeons practicing in the New England division had wait times 3.15 times longer than the reference region (IRR, 3.15 [95% CI, 2.27-4.35]; P < .001). Orthopaedic surgeons practicing in the New England division had the longest wait time (IRR, 3.15 [95% CI, 2.27-4.35]; P < .001), followed by those in the West North Central (IRR, 2.94 [95% CI, 2.11-4.09]; P < .001), Pacific (IRR, 2.70 [95% CI, 2.17-3.37]; P < .001), and Middle Atlantic (IRR, 2.37 [95% CI, 1.86-3.02]; P < .001) divisions. The model demonstrated robust explanatory power, achieving an R2 value of 0.93, indicating that 93% of the variability in wait times was accounted for by the factors included in the model.
Multivariate Analysis of Factors Affecting Wait Time

Statistical significance.

Dot plot comparing the median number of business days until an appointment for patients with Blue Cross/Blue Shield insurance and patients with Medicaid insurance.
Discussion
Primary Findings and Current Literature
The most important finding in the present study was that 34% of sports medicine–trained orthopaedic surgeons did not accept Medicaid insurance. Among surgeons who did accept Medicaid, patients with Medicaid experienced a 20% longer wait for a new patient appointment compared with those with BCBS insurance. Secondary findings were that there was no significant difference in wait times between hip, knee, and shoulder arthroscopic surgeons; physicians affiliated with academic institutions had longer wait times than their private practice counterparts; and certain regions of the United States were associated with longer wait times for a new patient appointment.
Our findings suggest that patients with Medicaid experience a 20% longer wait time for a new patient appointment, which is consistent with the current literature. Previous studies assessing patient wait times for sports medicine–trained orthopaedic surgeons have demonstrated a 20% to 58% longer wait time for patients with Medicaid compared with those with private insurance, similar to the present study's findings.12,27,32 Extending beyond orthopaedics, similar disparities have been documented in fields such as otorhinolaryngology, obstetrics and gynecology, primary care, dermatology, urology, and oncology, highlighting a pervasive issue across multiple medical specialties.1,9,10,15,24
Not only did patients with Medicaid seeking care from a sports medicine–trained orthopaedic surgeon experience an increased wait time compared with privately insured patients, but they were also much more likely to be denied an appointment. Our results found that 34% of surgeons did not accept Medicaid insurance, a rate consistent with those reported by Shi et al, 27 Wiznia et al, 32 and Felan et al, 12 with Medicaid denials of about 31%, 54%, and 50%, respectively. Notably, our observed Medicaid acceptance rate was higher than the 53% acceptance rate reported for general orthopaedic surgeons in the 2022 Merritt Hawkins survey. 21 However, direct comparisons are limited, as previous studies assessed fewer clinics over a broader time period, evaluated only a single joint, or were restricted to smaller geographic regions.
Among the factors examined, academic affiliation was the most significant predictor of prolonged wait times for new patient appointments among patients with Medicaid coverage. Although the present study did not directly evaluate the underlying causes of this association, it is plausible that the broader scope of academic physicians’ responsibilities, including research, education, and administrative duties, constrains clinical capacity. 8 Additionally, academic institutions are generally more inclined to accept Medicaid, which may result in a disproportionately high volume of patients with Medicaid seeking care.12,29 The confluence of reduced provider availability and increased patient demand may contribute to extended delays in access to initial appointments. These findings highlight a potential systemic imbalance within academic settings that warrants further investigation to inform policies and operational strategies aimed at improving timely access for publicly insured populations.
Implications of Findings
The present study did not assess the clinical significance of decreased access to care experienced by patients with Medicaid; however, poor outcomes due to delayed care are well documented in the orthopaedic literature.6,14,23,31,33 George et al 14 found that patients seeking treatment for hip fractures had an increase in mortality if their surgery was delayed for >6 days. Similarly, uninsured patients presenting with ankle fractures to a level 1 trauma center experienced a significant delay in surgical treatment and a subsequent increased risk of postoperative infections. 23 In sports medicine, delayed elective surgery significantly increased stress and decreased mental health in adolescent patients. 6 These findings are further corroborated by studies demonstrating an increased failure rate after delayed rotator cuff repair.7,31 Although the 20% increase in wait times—approximately 1 business day—for patients with Medicaid reported in the present study may not be clinically significant in the context of the clinical scenarios presented, in some instances, even minor delays could have significant consequences on outcomes.
Potential Causes and Policy Recommendations
The underlying reason for decreased access to care experienced by patients with Medicaid is difficult to identify based on the study design. However, we suspect that reduced reimbursement rates compared with private insurance may be a factor. 25 Medicaid reimbursement is often linked to Medicare reimbursement rates, which, when adjusting for inflation, have declined by 23% to 38% since 2000. Casper et al 4 reported a mean Medicaid reimbursement rate of 81.9% that of Medicare reimbursement for common orthopaedic procedures. For standard sports medicine procedures, Medicaid reimbursement may be as low as 20.6% that of Medicare. 4 For physicians operating a private practice, these reduced reimbursement rates may be a significant factor in patient selection that was not present in the past. Medicaid serves a critical function in expanding insurance coverage and facilitating access to care for millions who would otherwise remain uninsured. Proposed reductions in Medicaid services may lengthen wait times for patients who lose eligibility, while declining reimbursement rates may further compound the substantial barriers to access already experienced by this vulnerable population.
The broader implementation of telehealth may be another solution to overcome the barriers that patients with Medicaid face in orthopaedics. Telehealth can effectively increase efficiency and access to care while decreasing patient costs. 3 Additionally, patients have demonstrated similar satisfaction and improved follow-up rates when using telemedicine compared with traditional visits.11,13,20,22 Despite inherent limitations, including the potential lack of access to Wi-Fi or wireless devices and the inability to conduct comprehensive physical examinations and imaging, the broader implementation of telemedicine may help mitigate new patient wait times and improve access disparities for patients seeking care from sports medicine–trained orthopaedic surgeons.
Limitations
It is essential to acknowledge the limitations of the present study. First, the clinical scenarios utilized were designed to represent elective, nonurgent cases. As a result, the current findings may be more applicable to patients seeking care for elective rather than urgent abnormalities. Additionally, although each caller underwent training before study onset, it is possible that some callers were more uncomfortable during their telephone calls, which may have led to unnatural encounters, resulting in telephone calls ending prematurely before the provision of an appointment date. Lastly, using a public directory to obtain contact information and physician characteristics resulted in difficulties in correctly identifying physicians because of factors such as incorrect telephone numbers, incorrect practice addresses, and physicians no longer practicing at their publicly listed locations.
Conclusion
Patients with Medicaid experienced decreased access to care, with 34% of sports medicine–trained orthopaedic surgeons declining to accept Medicaid insurance. Among surgeons who accepted Medicaid, patients with Medicaid experienced slightly longer wait times for a new patient appointment compared with patients with private (BCBS) insurance. Additionally, patients with Medicaid experienced significantly longer wait times at academic institutions and in specific geographic locations. The present findings highlight a critical disparity in care, further underscoring the need for additional research to identify the cause and implement solutions.
Footnotes
Appendix
Appendix 1
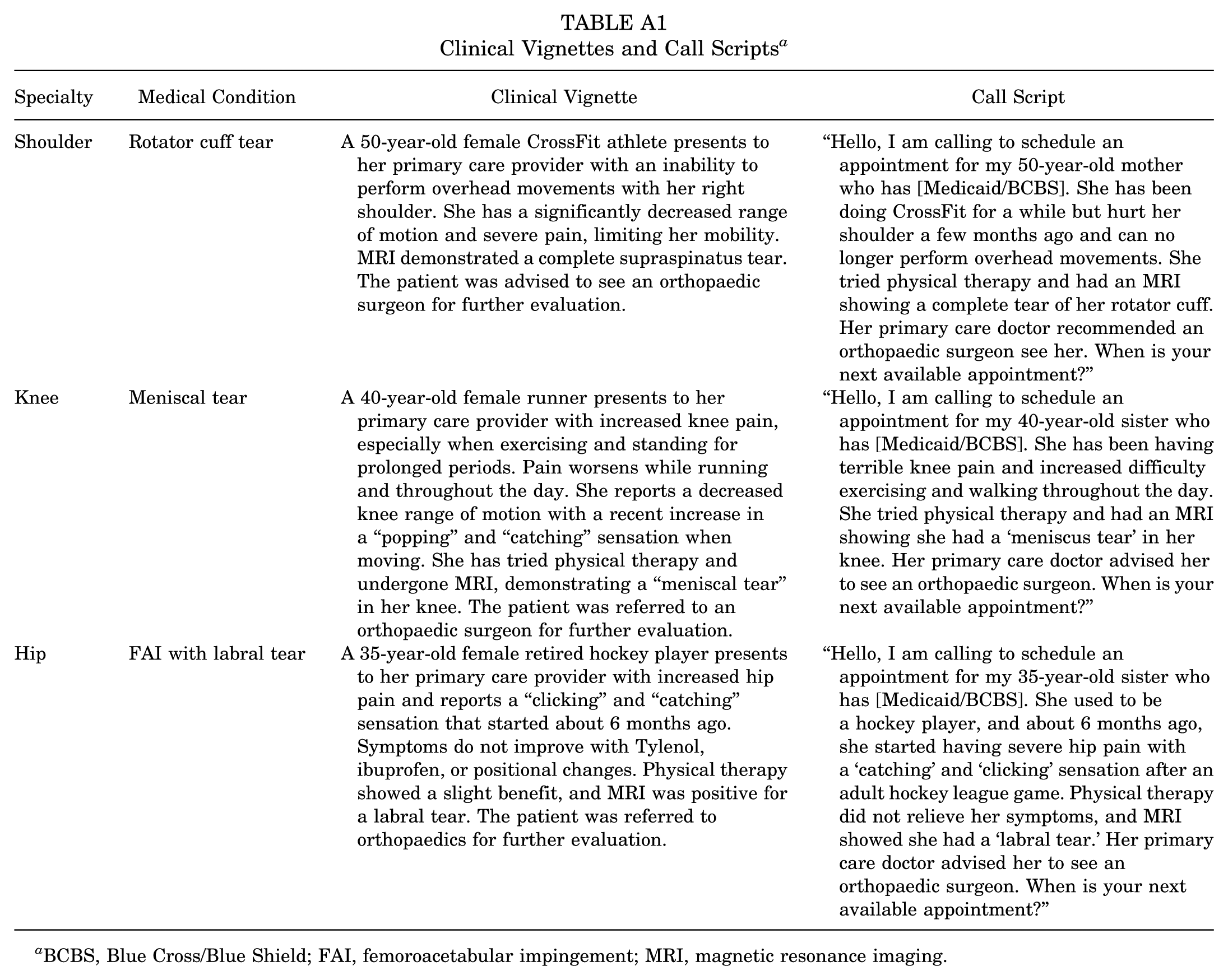
Clinical Vignettes and Call Scripts a
| Specialty | Medical Condition | Clinical Vignette | Call Script |
|---|---|---|---|
| Shoulder | Rotator cuff tear | A 50-year-old female CrossFit athlete presents to her primary care provider with an inability to perform overhead movements with her right shoulder. She has a significantly decreased range of motion and severe pain, limiting her mobility. MRI demonstrated a complete supraspinatus tear. The patient was advised to see an orthopaedic surgeon for further evaluation. | “Hello, I am calling to schedule an appointment for my 50-year-old mother who has [Medicaid/BCBS]. She has been doing CrossFit for a while but hurt her shoulder a few months ago and can no longer perform overhead movements. She tried physical therapy and had an MRI showing a complete tear of her rotator cuff. Her primary care doctor recommended an orthopaedic surgeon see her. When is your next available appointment?” |
| Knee | Meniscal tear | A 40-year-old female runner presents to her primary care provider with increased knee pain, especially when exercising and standing for prolonged periods. Pain worsens while running and throughout the day. She reports a decreased knee range of motion with a recent increase in a “popping” and “catching” sensation when moving. She has tried physical therapy and undergone MRI, demonstrating a “meniscal tear” in her knee. The patient was referred to an orthopaedic surgeon for further evaluation. | “Hello, I am calling to schedule an appointment for my 40-year-old sister who has [Medicaid/BCBS]. She has been having terrible knee pain and increased difficulty exercising and walking throughout the day. She tried physical therapy and had an MRI showing she had a ‘meniscus tear’ in her knee. Her primary care doctor advised her to see an orthopaedic surgeon. When is your next available appointment?” |
| Hip | FAI with labral tear | A 35-year-old female retired hockey player presents to her primary care provider with increased hip pain and reports a “clicking” and “catching” sensation that started about 6 months ago. Symptoms do not improve with Tylenol, ibuprofen, or positional changes. Physical therapy showed a slight benefit, and MRI was positive for a labral tear. The patient was referred to orthopaedics for further evaluation. | “Hello, I am calling to schedule an appointment for my 35-year-old sister who has [Medicaid/BCBS]. She used to be a hockey player, and about 6 months ago, she started having severe hip pain with a ‘catching’ and ‘clicking’ sensation after an adult hockey league game. Physical therapy did not relieve her symptoms, and MRI showed she had a ‘labral tear.’ Her primary care doctor advised her to see an orthopaedic surgeon. When is your next available appointment?” |
BCBS, Blue Cross/Blue Shield; FAI, femoroacetabular impingement; MRI, magnetic resonance imaging.
Appendix 2
Appendix 3
Final revision submitted July 16, 2025; accepted August 1, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was supported by a National Institutes of Health/National Center for Advancing Translational Sciences Clinical and Translational Science Award grant (No. UL1 TR002535). E.C.M. has received research support from Arthrex, Breg, DJ Orthopedics, Mitek, Ossur, and Smith & Nephew; is a paid consultant for Biomet and Bioventus; and receives royalties from Biomet, Zimmer, and Elsevier. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Colorado Multiple Institutional Review Board: 23-1303.