
Abstract
Background:
Arthroscopic lateral ligament repair is widely performed to treat chronic lateral ankle instability (CLAI), with good clinical outcomes. However, some patients show residual or recurrent instability after surgery. Although some risk factors of recurrent instability have been reported, the morphological characteristics of lateral ankle ligament injuries with residual or recurrent instability remain unclear.
Hypothesis:
Characteristic patterns of anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) injuries may be observed in patients with CLAI who have residual instability after isolated ATFL repair or recurrent instability after arthroscopic lateral ligament repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively reviewed 27 patients with CLAI and 10 controls without CLAI who underwent arthroscopic surgery. Three-dimensional volume-rendering models were reconstructed from preoperative magnetic resonance imaging scans of the ankle joints. For the primary outcome, the distance between the tip of the fibula and the proximal end of the CFL (dCFL), 3 vectors of the dCFL, and the horizontal angle of the ATFL (ATFL angle) were measured. For the secondary outcome, the clinical scores of patients with CLAI were evaluated pre- and postoperatively. Differences in parameters were compared among patients with no residual ankle instability, those with residual ankle instability immediately after arthroscopic ATFL repair, and the control patients. In addition, these parameters were compared between patients with non-recurrent and recurrent ankle instability at 1 year postoperatively.
Results:
As the primary outcome, the dCFL was greater, and its mediolateral vector, defined as the lateral direction as positive, was lower, indicating a medially shifted dCFL, in patients with residual ankle instability compared with patients without residual ankle instability and control patients. As a secondary outcome, there were no significant differences in clinical scores between the non-recurrence and recurrence groups. However, the ATFL angles in patients in the recurrent group were significantly smaller, indicating the talar side drooping of the ATFL, than in the nonrecurrence group.
Conclusion:
The CFL was injured and shifted medially in patients with residual ankle instability. Moreover, the ATFL in patients with recurrent instability showed talar side drooping. These findings suggest that additional CFL repair or ATFL augmentation may be beneficial in preventing recurrent instability after arthroscopic repair.
Ankle sprains are often encountered in daily clinical settings, and 10% to 30% of injuries can develop into chronic lateral ankle instability (CLAI) after an ankle sprain. 14 CLAI causes dysfunction and pain in the ankle joint, eventually leading to ankle osteoarthritis caused by abnormal stress distribution on the ankle joint due to instability.23,40 Therefore, eliminating ankle instability in CLAI is crucial to prevent the development of ankle osteoarthritis.
Recently, arthroscopic anterior talofibular ligament (ATFL) repair has become a widely performed procedure, and its outcomes are reported to be comparable to those of traditional open Broström procedures.1,13,21 However, some patients experience recurrent instability of the ankle joint after arthroscopic surgery, which is a clinical problem.21,48
Vega et al 43 reported that the lateral ankle ligament is composed of the superior fascicle of the ATFL (ATFLsf) and the lateral fibulotalocalcaneal ligament (LFCFL) complex, consisting of the inferior fascicle of the ATFL (ATFLif) and the calcaneofibular ligament (CFL), with independent functions. Although an arthroscopic procedure may repair only ATFLsf because ATFLsf is an intra-articular ligament, whereas the LFCFL complex is an extra-articular ligament, previous cadaveric studies have shown that the connecting fibers between the ATFLif and the CFL can transmit tension from each structure to the other, and certain suture passers allow for grasping of the ATFLif, which suggests that arthroscopic ATFL repair can provide tension to the CFL.2,4 However, this principle derived from cadaveric studies using healthy ankles may not necessarily apply to lateral ankle ligament injury in clinical practice. Reportedly, 30% of patients exhibit new radiographic signs of degenerative changes after the Broström procedure without CFL repair for CLAI, 22 which suggests that there are cases in which isolated ATFL repair cannot provide sufficient tension to the CFL through the connecting fiber. Therefore, understanding the morphology of injured lateral ankle ligaments, especially the relationship between the ATFLif and the CFL, is important to prevent recurrent instability postoperatively for CLAI in the recent trend of arthroscopically repairing ATFL without confirming CFL injury.
The primary aim of this study was to characterize the morphology of lateral ankle ligament injuries in patients with CLAI using 3-dimensional (3D) volume rendering of magnetic resonance imaging (MRI), and the secondary aim was to investigate the effect of morphological injury pattern on recurrent instability after arthroscopic ATFL repair. We hypothesized that there would be characteristic patterns of ATFL and CFL injuries in cases of residual instability after isolated ATFL repair or recurrence of ankle instability after surgery in cases of CLAI.
Methods
Ethics Statements
This study was approved by the local ethics committee of our university (approval number: E-879), and informed consent was obtained from all participants included in the study.
Study Design and Patients
A total of 27 ankles of 27 patients who underwent arthroscopic lateral ankle ligament repair for CLAI between December 2019 and December 2020 were retrospectively reviewed. The inclusion criteria were a diagnosis of CLAI by history, physical examination, and stress radiographs, and having undergone arthroscopic lateral ankle ligament repair. Patients with systemic diseases, such as rheumatoid arthritis, revision surgery, and medial ankle instability due to deltoid ligament tears or syndesmotic injuries, were excluded. A total of 33 patients met these criteria; however, 6 patients with inadequate imaging, as indicated by preoperative 0.8-mm sliced 3D MRI and varus stress radiographs at 1 year postoperatively, were excluded (Figure 1).
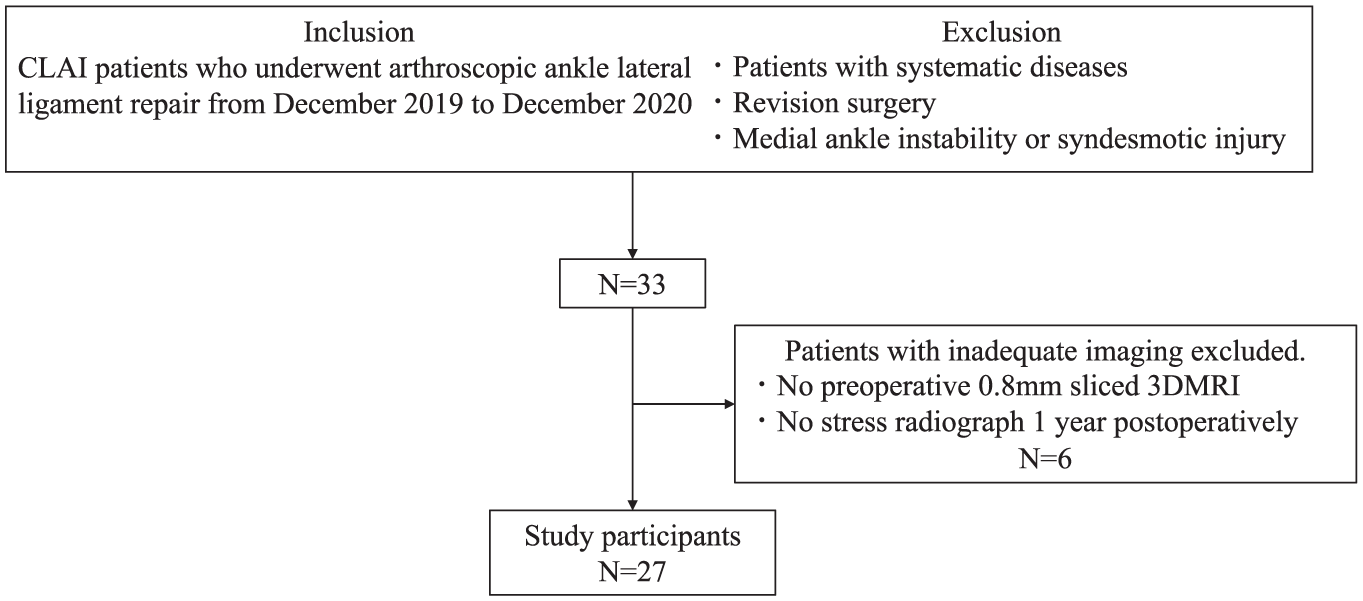
Participant flow chart. CLAI, chronic lateral ankle instability; 3D MRI, 3-dimensional magnetic resonance imaging.
For the control group with normal ankle lateral ligament, 10 ankles of 9 patients with osteochondral lesions of the talus (OLTs) without CLAI who underwent arthroscopic surgery were also included. The absence of CLAI was confirmed using stress radiography. The patients were also confirmed to have no ATFL injury by arthroscopy examination, and the CFL was intact as diagnosed by MRI. 25 They comprised 5 male and 4 female patients, with a mean age of 25.3 ± 13.1 years (range, 15-51 years).
Surgical Technique for CLAI
Arthroscopic ATFL repair was performed in accordance with previous reports. 26 Standard anteromedial (AM) and anterolateral (AL) portals were made, and a 30° oblique arthroscope was introduced. After a thorough evaluation of the ankle joint, an accessory AL portal (AAL) was created along the anterior border of the fibula as the working portal. A 23-gauge needle with a 3-0 nylon thread loop was inserted into the proximal ATFL remnant. Then, the nylon loop was retrieved, and a No. 2 thread (Ultra-Braid; Smith & Nephew) was passed through the loop and sewn using a racking hitch knot. Two additional threads were placed on either side of the first knot of the ATFL remnant. At least 1 of the 3 knot locations aimed to penetrate the confluent fibers of the ATFL and the CFL. If the quality of the ATFL remnant was poor, suture tape (Ultra-tape; Smith & Nephew) was used instead of No. 2 thread. Then, a drill hole was created in the ATFL footprint of the fibula. Next, No. 2 thread or suture tape through the ATFL remnant into a knotless anchor (Bioruptor; Smith & Nephew), and the anchor was inserted into the hole on the fibula and tightened with the ankle joint in the neutral position. After ATFL repair, a varus stress test was performed manually in neutral position using fluoroscopy to confirm whether CFL dysfunction was present (Figure 2). If talar tilt was not observed, surgery was completed; however, CFL repair was performed if talar tilt remained. The AAL portal was extended approximately 15 mm toward the fibular tip, and the CFL was found just deep to the peroneal tendon. A soft anchor (Q-Fix Mini; Smith & Nephew) was inserted into the CFL footprint under direct visualization. One end of the anchor suture was passed through the fibula side of the CFL and tightened using the sliding knot technique. Finally, varus stress was applied again to confirm the absence of instability. After surgery, the ankle joint was immobilized with a cast to restrict ankle motion for 2 weeks, and then it was replaced with an ankle brace. Weightbearing was permitted the day after surgery. Jogging was permitted at 6 weeks postoperatively, and return to sports activity was allowed at 3 months.

Stress radiographs during surgery. (A) Varus instability was confirmed before ATFL repair. (B) Residual instability after ATFL repair; CFL repair was done for these cases. (C) Absence of instability after the ATFL repair. ATFL, anterior talofibular ligament; CFL, calcaneofibular ligament.
Arthroscopic Evaluation of ATFL Remnant Quality
For patients with CLAI, the quality of the remnant ATFL was evaluated during surgery using arthroscopy, as described in a previous report with some modifications. 26 The quality of the remnants was divided into 3 groups: (1) poor, if poorly defined margins with hypoplastic ligament were present; (2) moderate, if stretched hyperplastic or hypoplastic ligaments with fibrotic tissue or synovitis were present; and (3) excellent, if the well-defined margin of the ligament with normal synovial tissue was present.
Stress Radiography
Varus stress radiographs were obtained for all ankles with CLAI before surgery and 1 year postoperatively. Radiography was performed at a force of 50 N using a tension device (Imada) in neutral position. The talar tilt angle (TTA) was measured, and a TTA >6° in the postoperative radiograph was defined as recurrent ankle instability according to a previous report. 21
Reconstruction and Evaluation of a 3D Model on MRI
For the primary outcome, the morphology of lateral ligament injury, as visualized with the reconstructed 3D model on MRI, was evaluated. MRI was performed preoperatively for patients with CLAI and OLT using a 1.5-T MR unit (1.5-T Achieva Release 3.2.3.4; Philips) with dual-phase array coils. During the MRI scan, the ankle joint was held at 0° in dorsiflexion. The following sequences were obtained: 3D T2-weighted images, repetition time, 1500 msec; echo time, 75 msec, field of view, 150 mm; matrix, 240 × 240; slice thickness, 0.8 mm with a −0.4 mm gap. 24 The MRI images were stored in the Digital Imaging and Communications in Medicine 3.0 standard format. The 3D volume-rendering model reconstruction of the tibia, fibula, ATFL, and CFL was built using ITK-SNAP 4.0.1 software (Penn Image Computing and Science Laboratory, University of Pennsylvania,) by manually segmenting each object on the axial, sagittal, and coronal planes of the T2-weighted images (Figure 3).
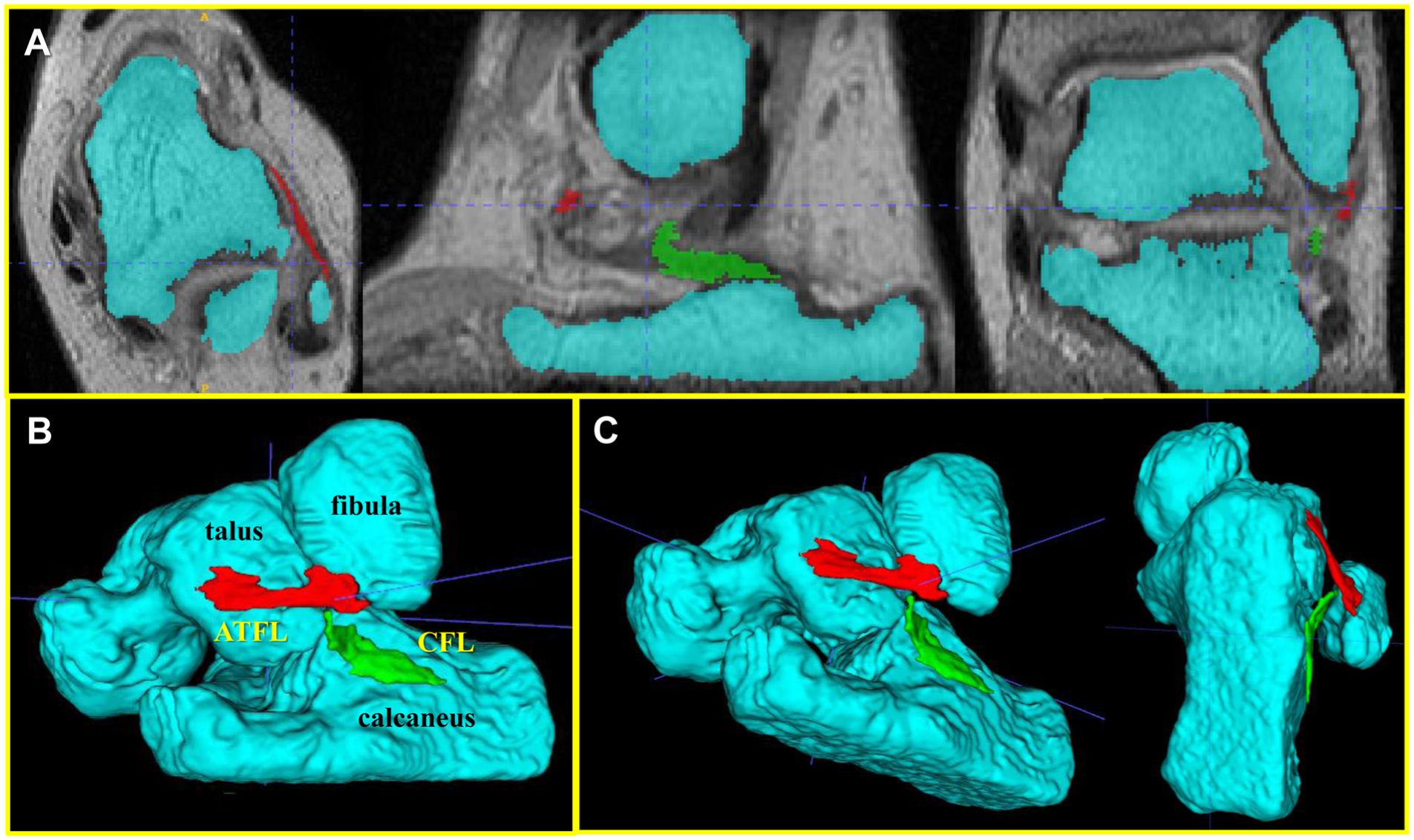
3D volume-rendering model on MRI reconstructed using ITK-SNAP. (A) The preoperative talus, fibula, calcaneus, ATFL, and CFL are segmented in the axial, sagittal, and coronal planes of MRI. (B) The reconstructed 3D volume-rendering model on MRI. (C) The 3D model is able to be observed from various views using ITK-SNAP. ATFL, anterior talofibular ligament; CFL, calcaneofibular ligament; MRI, magnetic resonance imaging; 3D, 3-dimensional.
The distance between the tip of the fibula and the proximal end of the CFL (dCFL) and the angle of the ATFL relative to the horizontal plane (ATFL angle) were measured using the following methods. The dCFL was calculated by measuring the vectors in 3 directions (Figure 4). First, the tip of the fibula and the dCFL were identified using the 3D volume-rendering model (Figure 4A). The parallel vector (dxCFL) and the perpendicular vector (dyCFL) of the dCFL (Figure 4B) relative to the reference line, which was drawn between the medial and lateral malleoli (Figure 4C), were measured in the axial plane. The dxCFL and dyCFL were defined as positive in the lateral and anterior direction with respect to the tip of the fibula, respectively. The vertical vector (dzCFL) was measured in the sagittal plane, defined as positive in the proximal direction with respect to the tip of the fibula (Figure 4D).
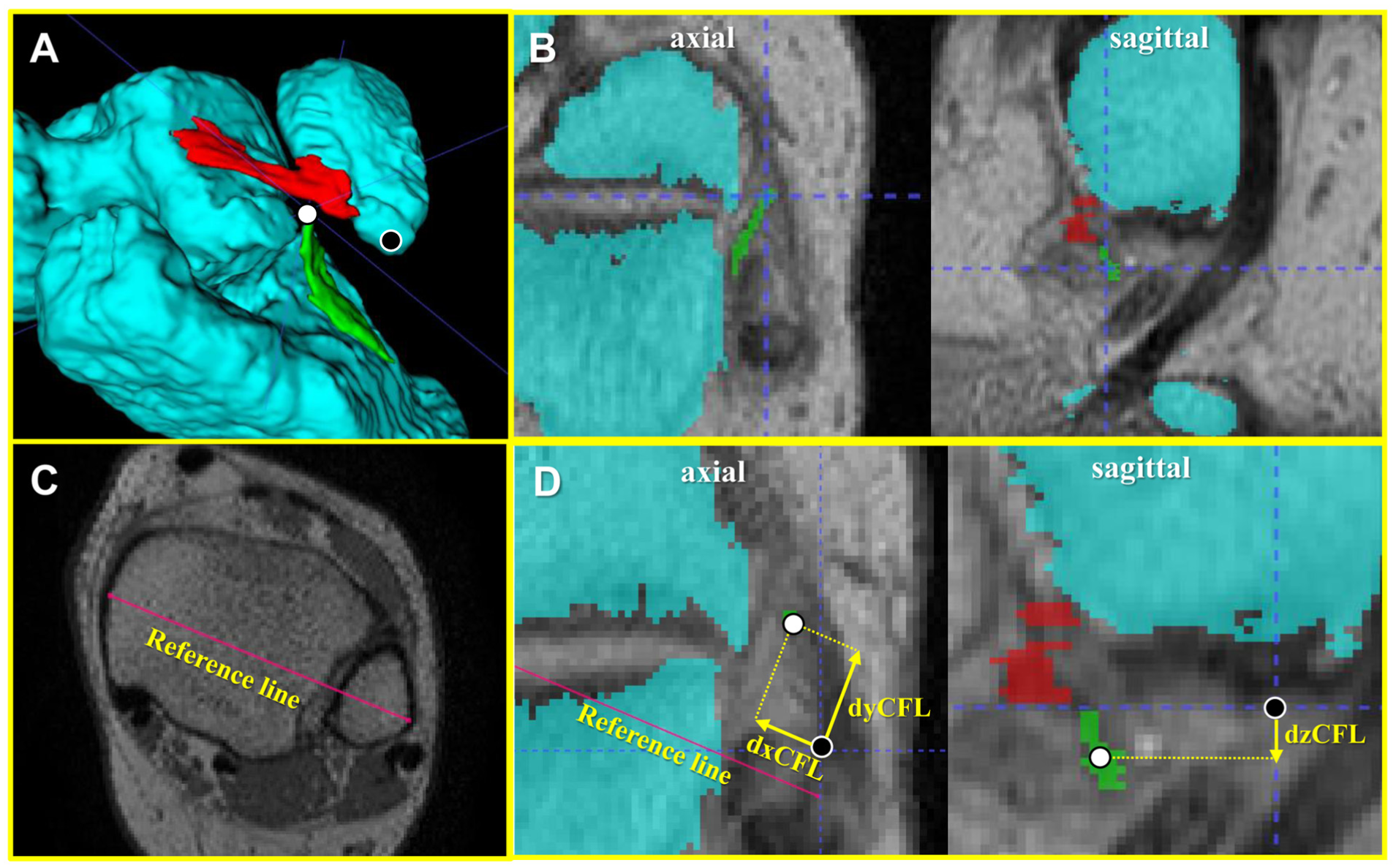
Measurement process of 3 vectors of the distance between the tip of the fibula and the dCFL. (A) The tip of the fibula and the dCFL are identified on the 3D model. Black dot: the tip of the fibula, white dot: the dCFL. (B) The points identified in the 3D model are also identified in the 2D image. The dCFL was localized in the axial and sagittal planes by the intersection of the blue dotted lines. (C) The reference line is drawn between the medial and lateral malleoli. (D) The measurement of the parallel, perpendicular, and vertical vectors of the dCFL: dx, dy, and dzCFL. The lateral, anterior, and proximal directions with respect to the tip of the fibula were defined as positive for dxCFL, dyCFL, and dzCFL, respectively. Therefore, the dxCFL, dyCFL, and dzCFL are negative, positive, and negative, respectively. Black dot: the tip of the fibula, white dot: the dCFL. CFL, calcaneofibular ligament; dCFL, proximal end of the CFL; dxCFL, parallel vector of dCFL; dyCFL, perpendicular vector of dCFL; dzCFL, vertical vector of dCFL; 3D, 3-dimensional.
Finally, the dCFL was calculated using the following formula: dCFL =
The ATFL angle was measured in the 3D volume-rendering model view (Figure 5). The angle between the long axis of the ATFL and the axial plane was measured using a protractor. An upward orientation of the talar side of the ATFL was defined as positive.
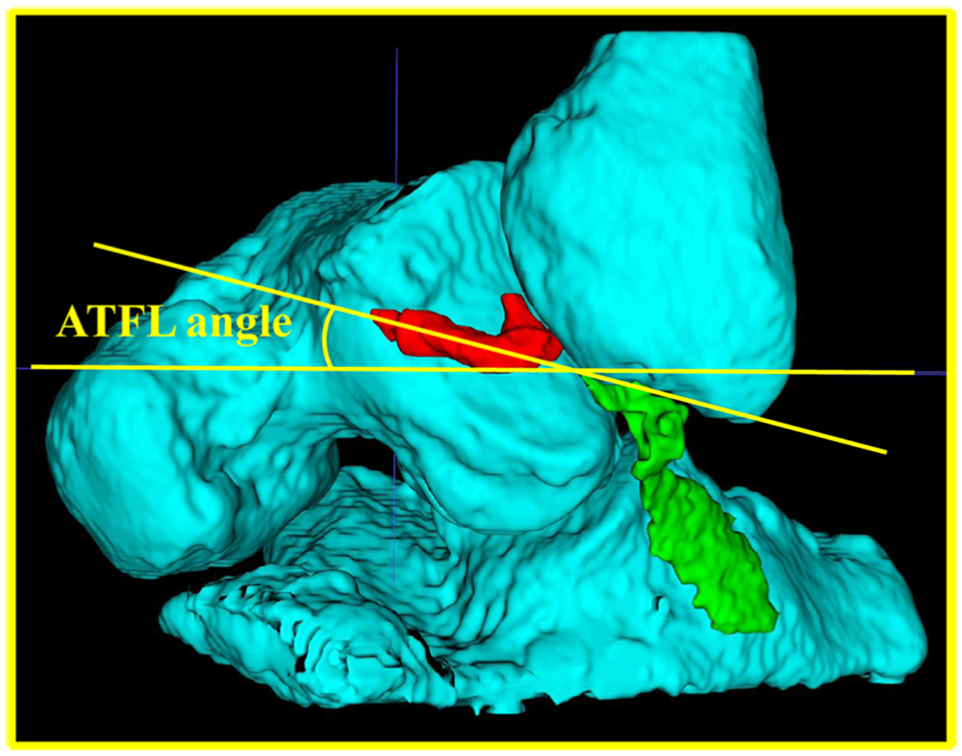
The ATFL angle, which is the angle between the long axis of the ATFL and the axial plane, was measured on a 3D volume-rendering model. ATFL, anterior talofibular ligament; 3D, 3-dimensional.
The reconstruction of 3D volume-rendering on MRI and measurement was performed by 2 foot and ankle surgeons (S.S. and D.M.), with no clinical information to assess the interrater reliability of the measurements.
Clinical Outcome Evaluation
For the secondary outcome, 3 scoring systems were used to evaluate the preoperative status and the final follow-up clinical outcome: the Japanese Society for Surgery of the Foot (JSSF),29,30 the Karlsson-Peterson (K-P) score, 15 and patient-reported outcomes using the Self-Administered Foot Evaluation Questionnaire (SAFE-Q), which comprises 5 subscales: (1) pain and pain-related visual analog scale score, pain in the morning, at the end of the day, during sleeping, and upon walking in several conditions in the past week; (2) physical functioning—difficulty going up and downstairs, squatting, putting on socks, going uphill- and downhill, and walking flat and on uneven ground; (3) social functioning—difficulty going out, performing routine activities, enjoying leisure activities, and doing work and school activities; (4) shoe-related—difficulty putting on high-fashion or formal shoes; and (5) general health and well-being—mental state, including anxiety, depression, and frustration.31,32
Statistical Analysis
Age, body mass index (BMI), dCFLs, 3 vectors of the dCFL, and the ATFL angle were compared among the no CFL repair, CFL repair, and control groups using the Kruskal-Wallis test. The same parameters and clinical outcome scores were compared between the recurrence and nonrecurrence groups using the Mann-Whitney U test and the post-hoc Holm test. The dCFL, 3 vectors of the dCFL, and the ATFL angle were compared between patients with 3 ATFL remnant qualities using the Kruskal-Wallis test. The correlations between preoperative TTA and the dCFL, as well as the 3 vectors of the CFL and the ATFL angle, in all patients with CLAI and in each group were examined using the Spearman correlation test. The intrarater and interrater reliability of all parameters were evaluated using the intraclass correlation coefficient (ICC). The ICC values were interpreted as follows: <0.40, indicating poor agreement; between 0.40 and 0.75, indicating fair to good agreement; and >0.75, indicating excellent agreement. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University), which is a graphical user interface for R (The R Foundation for Statistical Computing). Specifically, it is a modified version of R Commander designed to add statistical functions frequently used in biostatistics. Statistical significance was set at P < .05.
Results
The CLAI patients comprised 10 male and 17 female patients, with a mean age of 28.7 ± 15.4 years (range, 14-62 years), and control patients comprised 5 male and 4 female patients, with a mean age of 25.3 ± 13.1 years (range, 15-51years). To investigate the morphological characteristics of ankles with residual instability after ATFL repair as the primary outcome, patients with CLAI were divided into 2 groups: the no CFL repair group, who underwent ATFL repair only, and the CFL repair group, who underwent CFL repair in addition to ATFL repair. Among the control, no CFL repair, and CFL repair groups, there were no significant differences in age or BMI. In the 3D volume-rendering images, the ATFL ran straight from the talus to the fibula attachment and was clearly depicted as 2 bundles, ATFLsf and ATFLif, in the control group (Figure 6).
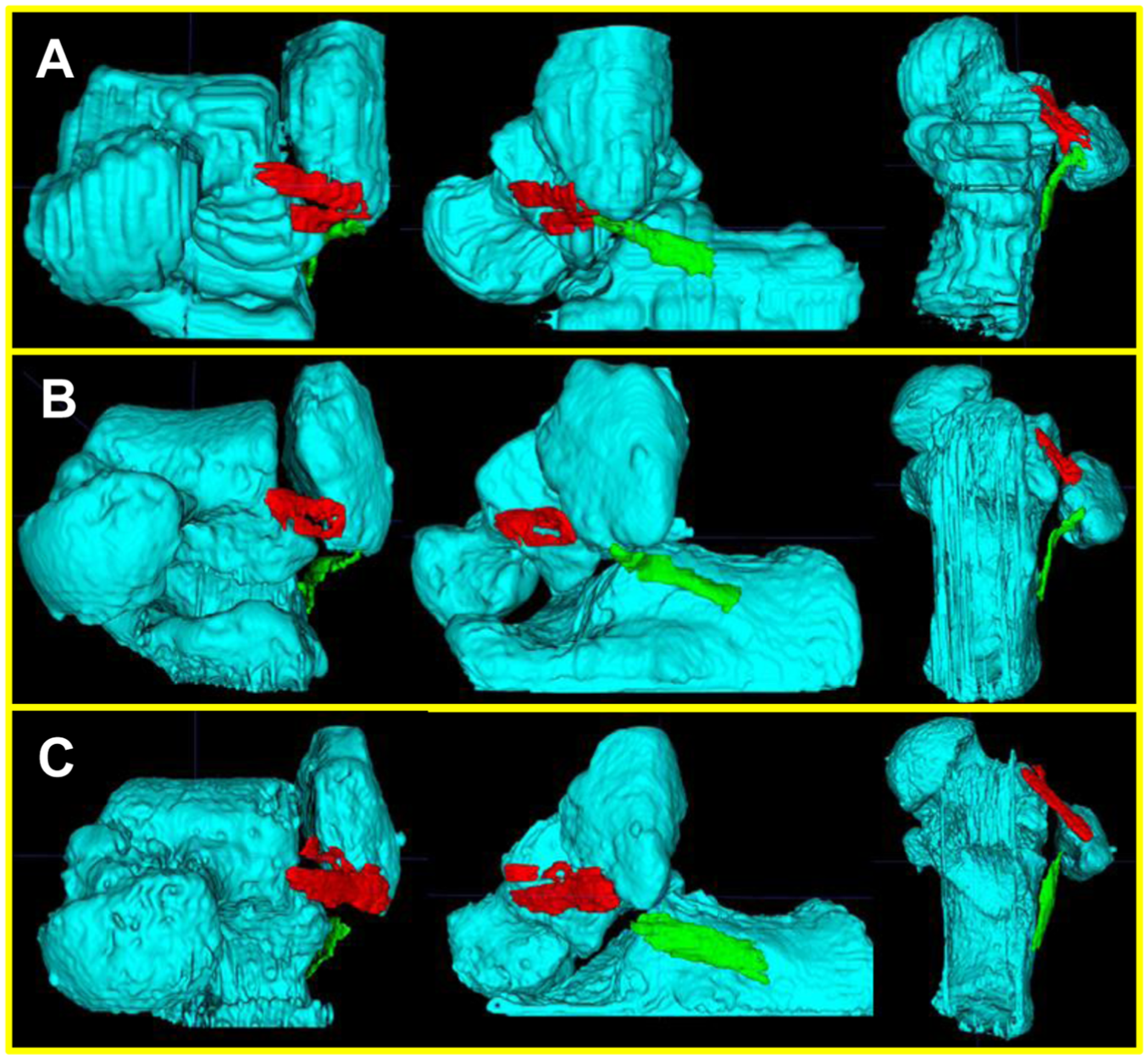
3D volume-rendering models: (A) control group; (B) no CFL repair group; (C) CFL repair group. CFL, calcaneofibular ligament; 3D, 3-dimensional.
In patients with CLAI, the 2 bundles of the ATFL were indistinct and ran irregularly or wavy. The CFL in the control and no CFL repair groups exhibited continuity from the calcaneus to the fibula attachment, and it became bent at the point of contact with the peroneal tendon. In contrast, the CFL was not continuous with fibular attachment in the CFL repair group. In addition, the CFL entirely deviated toward the calcaneus, and the curve at the peroneal tendon disappeared. The dCFL in the CFL repair group was significantly greater than that in the other 2 groups. Of the 3 dCFL vectors, dxCFL of the CFL repair group was significantly lower than that of the other 2 groups (Figure 7).
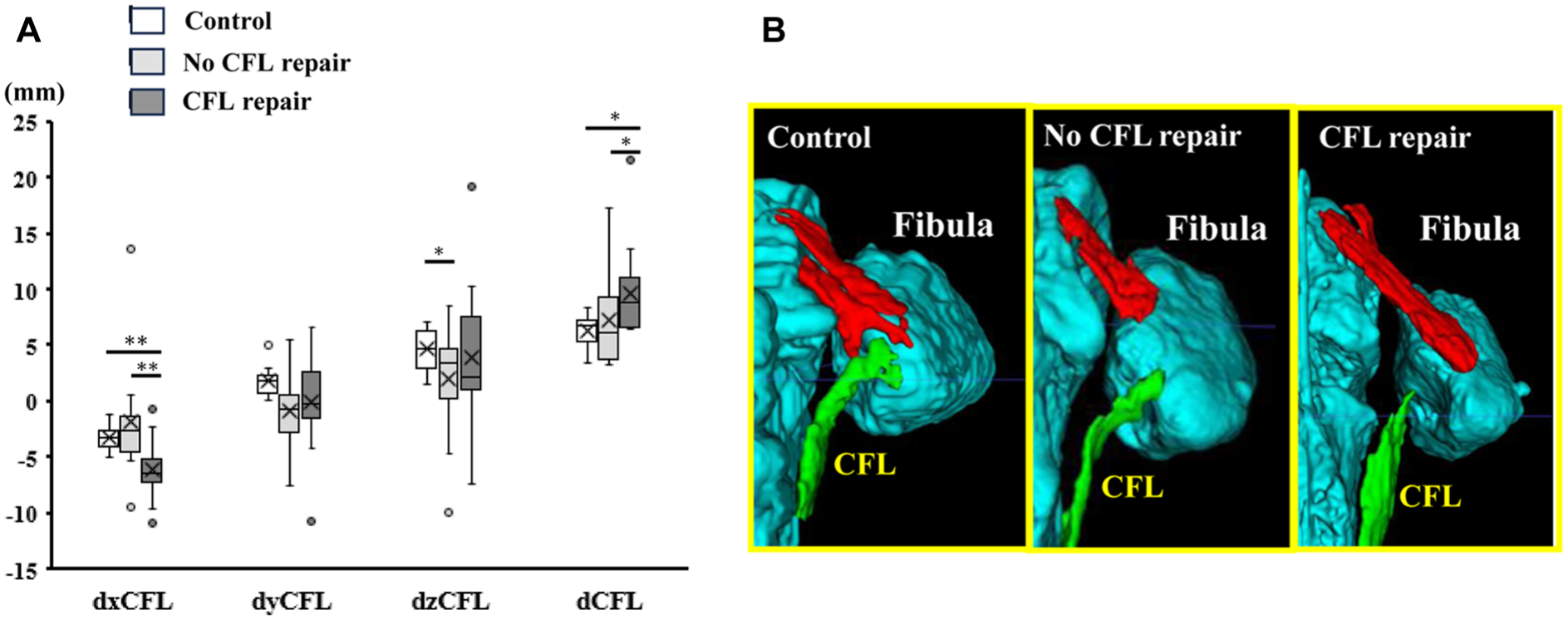
Distance between the tip of the fibula and the proximal end of the CFL (dCFL) and its 3 vectors in the control, no CFL repair, and CFL repair groups. (A) Box-and-whisker plots. (B) 3D volume-rendering models. *P < .05, **P < .01. CFL, calcaneofibular ligament; dCFL, proximal end of the CFL; dxCFL, parallel vector of dCFL; dyCFL, perpendicular vector of dCFL; dzCFL, vertical vector of dCFL; 3D, 3-dimensional.
The ATFL angle was not significantly different among the 3 groups (Table 1). Thus, instability may persist after ATFL repair in ankles where the tear ends of the CFL are far from the fibular attachment site. There was a significant correlation between preoperative TTA and dxCFL in the no CFL group (rs = −0.76; P < .01).
Patient Characteristics and 3D Volume-Rendering MRI Model Parameters in the 3 Groups a

Data are presented as mean ± SD (range). ATFL, anterior talofibular ligament; BMI, body mass index; CFL, calcaneofibular ligament; dCFL, proximal end of the CFL; dxCFL, parallel vector of dCFL; dyCFL, perpendicular vector of dCFL; dzCFL, vertical vector of dCFL; MRI, magnetic resonance imaging; Preop, preoperative; 3D, 3-dimensional; TTA, talar tilt angle; 3D, 3-dimensional.
P < .01 between the control and CFL repair groups.
P < .05 between the control and CFL repair groups.
P < .05 between the no CFL repair and CFL repair groups.
The recurrence (n = 11) and non-recurrence (n = 16) groups were compared to determine the association of the morphology of the lateral ankle ligament and the postoperative recurrence of ankle instability as the secondary outcome (Table 2).
Patient Characteristics, Clinical Outcome Scores, and 3D MRI Model Parameters of the Nonrecurrence and Recurrence Groups a

Values are presented as mean ± SD (range). ATFL, anterior talofibular ligament; BMI, body mass index; CFL, calcaneofibular ligament; dCFL, proximal end of the CFL; dxCFL, parallel vector of dCFL; dyCFL, perpendicular vector of dCFL; dzCFL, vertical vector of dCFL; JSSF, Japanese Society for Surgery of the Foot; K-P, Karlsson-Peterson; Preop, preoperative; SAFE-Q, Self-Administered Foot Evaluation Questionnaire; 3D MRI, 3-dimensional magnetic resonance imaging; TTA, talar tilt angle.
P < .05.
P < .01.
In the 3D volume-rendering image analyses, the ATFL angle was significantly lower in the recurrence group than in the non-recurrence group (P < .01) (Figure 8).

The ATFL angle in the nonrecurrence and recurrence groups. (A) Box-and-whisker plots. (B) Representative 3D volume-rendering models. **P < .01. ATFL, anterior talofibular ligament.
There were no significant differences in dCFL and the 3 vectors of the dCFL between the 2 groups. Regarding clinical scores, there were no significant differences in the pre- and postoperative JSSF and SAFEQ scores. Concerning the ATFL remnant quality, 6 ankles were excellent, 13 ankles were moderate, and 8 ankles were poor. Recurrent ankle instability occurred in zero ankles with excellent remnant quality, 5 ankles (38.5%) with moderate remnant quality, and 6 ankles (75%) with poor remnant quality. The dCFL and 3 vectors of the dCFL were not significantly different among these remnant qualities (Table 3).
The 3D Volume Rendering MRI Model Parameters of Each Remnant Quality a

Data are presented as mean ± SD (range). ATFL, anterior talofibular ligament; CFL, calcaneofibular ligament; dCFL, proximal end of the CFL; dxCFL, parallel vector of dCFL; dyCFL, perpendicular vector of dCFL; dzCFL, vertical vector of dCFL; MRI, magnetic resonance imaging; 3D, 3-dimensional.
Interobserver ICCs in the measurements of the dxCFL (0.77 [95% CI, 0.38 to 0.93), dyCFL (0.87 [95% CI, 0.63 to 0.96]), dzCFL (0.70 [95% CI, 0.25 to 0.90]), and ATFL angles (0.76 [95% CI, 0.36 to 0.93]) were good to excellent. Intraobserver ICCs in the measurement of the dxCFL (0.97 [95% CI, 0.90 to 0.99), dyCFL (0.91 [95% CI, 0.72 to 0.97), dzCFL (0.71 [95% CI, −0.02 to 0.92]), and ATFL angles (0.93 [95% CI, 0.74 to 0.98]) were good to excellent.
Discussion
To our knowledge, this is the first study to analyze the morphological characteristics of ankle lateral ligament injuries with residual or recurrent ankle instability after arthroscopic surgery using a 3D volume-rendering MRI model. In the primary outcome, although the preoperative dCFL was greater in the CFL repair group, the dxCFLs in the CFL repair group were significantly lower than those in the no CFL repair and control groups. Furthermore, in the secondary outcome, the ATFL angles in the recurrence group were significantly smaller than those in the nonrecurrence group. The greater dCFL and lower dxCFL indicate that the preoperative CFL is injured and shifted medially in the CFL-repaired group, and the smaller ATFL angle indicates that the preoperative ATFL has talar side drooping in the recurrence group. Our findings suggest that isolated arthroscopic ATFL repair may be insufficient to eliminate instability in CLAI, depending on the morphological characteristics of the ankle lateral ligament injury.
Although the morphology of the normal ankle lateral ligaments has been examined in several cadaveric studies,2,42 it is difficult to examine the preoperative morphology of injured ankle lateral ligaments in patients with CLAI using cadaveric specimens. Several studies demonstrated ATFL and CFL injury patterns on 2D images.25,39 Regarding the CFL, a previous report showed that the CFL injury decreased the flexed CFL angle, and it ran parallel to the axis of the calcaneus. 28 However, 2D images make it difficult to spatially understand the movement of injured ligaments. The 3D volume-rendering models created from MRI data can be equally effective for the comprehensive and accurate assessment of osseous and soft tissue structure, morphology, and pathology.3,11,20 Therefore, we reconstructed 3D volume-rendering models of preoperative ankle MRI scans to investigate the morphologic character of lateral ligament injuries in patients with residual or recurrent ankle instability after surgery for CLAI.
Recurrent or residual instability after lateral ankle ligament repair results in the suffering of repeated sprains and osteoarthritis changes, even though postoperative clinical scores do not differ from those of patients without recurrent instability.19,33 Several factors of recurrent instability have been reported, such as high BMI, general laxity, and poor ATFL remnant.5,21,46,48 However, there may be other surgical problems besides the predisposing factors for recurrent instability. Luthfi et al 21 analyzed factors for recurrent instability and showed that neglected CFL injury, in addition to previously reported factors, such as high activity and poor remnant quality, could result in recurrent instability. Maffulli et al 22 also reported that 30% of patients who underwent the Broström procedure without CFL repair showed new radiographic signs of degenerative changes despite good postoperative outcomes. These results suggest that arthroscopic ATFL repair without CFL repair may be insufficient to eliminate instability in patients with ATFL and CFL injuries. In our series, some patients showed residual ankle instability just after arthroscopic ATFL repair, and the residual instability was eliminated after CFL repair. Our results revealed that these patients have the characteristic morphology of CFL injury, characterized by a medially displaced dCFL.
Previous reports demonstrated that the CFL is a strong stabilizer of the ankle and subtalar joints and that its dysfunction affects the ankle and subtalar kinematics. 17 In a cadaveric experiment, Hunt et al 10 reported that more inversion of the talus and calcaneus and calcaneal medial displacement were seen in ankles with ATFL and CFL injuries than in ankles with ATFL-isolated injuries. Previous studies have reported that CFL injuries are common in severe ankle osteoarthritis, and the stress distribution of the subtalar joint is altered, which suggests that CFL injury can be a risk factor for ankle osteoarthritis caused by impairment of the compensatory function of the subtalar joint.12,24,34 Although some studies showed that CFL repair combined with ATFL repair achieved no better clinical outcomes than isolated ATFL repair,16,37 these previous evidence indicates that neglected CFL injury can result in the recurrence of instability.
Recently, re-tensioning of the CFL in arthroscopic ATFL repair has been studied. Vega et al 42 demonstrated that the ATFLif and CFL contain the connecting fibers that form the LFTCL complex. A biomechanical study showed that connecting fibers between the ATFLif and the CFL are robust enough to transmit tension from one structure to the other, which indicates that ATFLif repair can indirectly repair the CFL. 2 A cadaveric study using ankles with dissection of the ATFL and the CFL as the same unit showed that reattachment of only the ATFL could concurrently advance the CFL to the footprint of the fibula. 18 However, the repaired CFL did not show a normal strain pattern. 38 During arthroscopic ATFL repair, the surgical procedure of applying tension to the LFTCL complex by penetrating the microsuture lasso into the confluent fiber between the ATFLif and the CFL has been reported.6,13 It seems reasonable to suture the confluent fibers of the ATFL and the CFL to provide tension to both ligaments. However, our results indicated that this procedure does not provide sufficient tension to the CFL in some cases. In the present study, the ankle with residual instability after ATFL repair showed that the dCFL was displaced from its fibular attachment toward the calcaneus, suggesting that isolated ATFL repair no longer provides strain to the CFL through the confluent fibers. In these cases, additional CFL repair is needed, and it should be confirmed that no CFL dysfunction occurs immediately after isolated ATFL repair to avoid residual instability.
Despite additional CFL repair, some patients in our study showed recurrent ankle instability after surgery. The dCFLs were not significantly different between the recurrence and nonrecurrence groups, suggesting that CFL repair improved CFL dysfunction; however, other factors may have affected the recurrent instability. Focusing on the morphology of the ATFL injury, the ATFL angles of the recurrence group were significantly lower than those of the nonrecurrence group. However, there were no significant differences in the ATFL angles among the remnant qualities. These findings suggest that ankle joints with loosening of the entire ATFL length are at risk of postoperative recurrence, even if both the ATFL and the CFL are repaired. In fact, not all ankles with poor remnant quality exhibited recurrent instability.21,48 A previous report showed that loosening of the anterolateral capsule affects stability, including recurrent instability after arthroscopic repair, and this may be indicated by ATFL drooping in the 3D volume-rendering model. 27 The high incidence of recurrent instability in these ankles may be due in part to problems with the technique of arthroscopic repair. Most arthroscopic anatomic ATFL repair procedures, including ours, involve the repair of the fibular side.1,41 Therefore, slight residual laxity of the talar side of the ATFL may have led to the postoperative recurrence of ankle instability. Our findings that the morphology of lateral ankle ligament injuries influences clinical outcomes may contribute to reducing recurrent instability after arthroscopic ATFL repair. Because CLAI with a medial shifted dCFL and/or drooping talar side ATFL may result in recurrent instability after ATFL repair, augmentation or reconstruction may be necessary for CLAI patients with such ATFL and CFL injury patterns confirmed on MRI or with residual instability immediately after ATFL repair. Because ATFL augmentation shows biomechanical stability similar to that of an intact native ATFL 45 and obtains good clinical outcomes, 40 it should be considered to perform ATFL augmentation for drooping talar side ATFL.
Limitations
This study has several limitations. First, the reliability of reconstructing and assessing 3D volume-rendering models using MRI should be discussed. Although the software we used in this study, ITK-SNAP, is reported35,44 to be one of the best 3D segmentation software tools, 3D volume-rendering models had to be created with manual segmentation. There are a few reports on the reconstruction of 3D volume-rendering models of the lateral ankle ligaments on MRI. He et al 8 reported that reconstructing the 3D volume-rendering model on MRI provides a reference for the accurate anatomy of the area and location of the ATFL in healthy volunteers. However, they mentioned that reconstruction of the injured ATFL 3D volume-rendering model could be more complex. Regarding the injured ATFL, a 3D reconstruction model of the injured ATFL may also be an accurate method of detecting ATFL injury and measuring anatomic structures.7,47 However, CFL has never been reconstructed using 3D reconstruction. In our study, the intra- and interobserver reliability were good to excellent. However, it has not been confirmed whether the morphology of the lateral ankle ligament in the 3D volume-rendering model correctly reflects the actual anatomy. The reliability of the 3D volume-rendering model of the lateral ankle ligament requires further investigation. Second, MRI scans were performed only in the neutral and nonweightbearing positions. Therefore, the actual morphologies of the ATFL and CFL in the weightbearing and inversion positions with instability are unknown. An MRI scanning technology that allows imaging in various ankle positions or weightbearing positions needs to be developed. Finally, the number of patients included in this study is small, and they span a wide range of ages. Because the 3D MRI used in this study required a longer imaging time than a conventional MRI, some patients with CLAI refused to undergo the procedure, resulting in a small sample size and a wide age range. However, the primary aim of this study is to investigate the morphological patterns of lateral ankle ligament injury. Therefore, it is significant to analyze patients with a wide range of ages. Furthermore, it has been reported that age does not affect ankle lateral ligament morphology in studies using cadaveric specimens and MRI.9,36 Nevertheless, further studies with larger sample sizes are needed to address these limitations.
Conclusion
Our results of 3D volume-rendering model reconstruction of MRI revealed the preoperative morphology of lateral ankle ligament injury in residual or recurrent ankle instability after arthroscopic surgery for CLAI. Patients with residual ankle instability after arthroscopic ATFL repair had CFLs that were injured and shifted medially. Moreover, patients with recurrent ankle instability after ankle lateral ligament repair had ATFLs with talar side drooping. Based on these findings, we believe that additional CFL repair or ATFL augmentation may be effective in preventing recurrent ankle instability after arthroscopic surgery for patients with CLAI, depending on the morphological characteristics of the injured lateral ligament of the ankle.
Footnotes
Final revision submitted June 16, 2025; accepted July 15, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hiroshima University (approval number E-879).