
Abstract
Background:
Arthroscopic suprascapular nerve release treats suprascapular neuropathy, but surgical challenges require precise anatomic landmarks and optimal instrument positioning.
Purposes:
To examine the anatomic relationships of the suprascapular nerve to bony and arthroscopic landmarks, evaluate sex- and height-related variations, and provide insights to improve arthroscopic surgical accuracy and reduce complications.
Study Design:
Descriptive laboratory study.
Methods:
A total of 22 shoulders from 11 Thiel-embalmed cadavers (6 male, 5 female) were dissected to measure distances from the suprascapular nerve to bony landmarks (acromion, coracoid process, glenoid) and arthroscopic landmarks (coracoacromial ligament and conoid ligament). Notch dimensions and angles relevant to arthroscopic portal placement were also evaluated. Measurements were analyzed for correlations with sex and height.
Results:
The mean distance from the suprascapular nerve to the posterolateral acromion (D1) was 58.34 ± 6.58 mm, and to the anterolateral acromion (D2) was 59.50 ± 5.22 mm, both statistically significantly greater in male patients (D1, 63.38 ± 3.90 mm vs 52.29 ± 2.79 mm; D2, 63.09 ± 3.49 mm vs 55.20 ± 3.30 mm; P < .001). Arthroscopic landmarks showed no statistically significant correlation with height. The suprascapular notch was predominantly type 3 (90.9%) with a mean width of 9.93 ± 1.34 mm and nerve-to-lateral border distance of 4.67 ± 1.27 mm, consistent across sex. Moderate, statistically significant correlations with height were noted for distances D1 (r = 0.51).
Conclusion:
This study demonstrated that the suprascapular nerve's distance to bony landmarks varies by sex, while arthroscopic and notch dimensions remain consistent. Height moderately influences certain bony landmark distances.
Clinical Relevance:
These results provide essential anatomic references to enhance the precision of arthroscopic decompression
The suprascapular nerve, arising from the upper trunk of the brachial plexus, is essential for the innervation of the supraspinatus and infraspinatus muscles and contributes to the sensory innervation of the shoulder joint. Suprascapular nerve entrapment neuropathy can lead to persistent pain and weakness in these muscles, resulting in significant functional impairment of the shoulder and a marked decline in the patient's quality of life.4,9,18
Arthroscopic suprascapular nerve release has emerged as a preferred surgical treatment for patients with suprascapular neuropathy at the suprascapular notch, especially when nonoperative management fails. This minimally invasive technique offers superior visualization and access to the nerve, while minimizing soft tissue disruption compared with traditional open surgery.3,4,7 However, the intricate anatomic relationships between the suprascapular nerve at the suprascapular notch, surrounding bony landmarks, and adjacent structures present considerable challenges for surgeons during arthroscopic intervention.8,19
To the best of our knowledge, several cadaveric studies have delineated the safe zone of the suprascapular nerve, providing valuable guidance for shoulder surgeons in identifying the safe area between the glenoid rim and the suprascapular nerve at the suprascapular notch.6,14,15 However, many of these studies have not adequately focused on anatomic landmarks that could improve surgical accuracy and assist in determining optimal trajectories for cutting instruments during arthroscopic procedures. Arce et al 1 proposed a landmark-based approach for identifying the suprascapular nerve, beginning at the origin of the coracoacromial ligament at the acromion and tracing it to its posterior insertion at the coracoid. The method then follows the posterior coracoacromial ligament to the conoid ligament. Despite its utility, this approach does not comprehensively describe the distances between the coracoid process, conoid ligament, and suprascapular nerve, limiting its applicability in surgical contexts.
This study aimed to explore the anatomic relationship between the suprascapular nerve and surrounding structures, emphasizing its proximity to bony landmarks, arthroscopic (soft tissue) landmarks, and potential correlations with patient-specific factors such as sex and height. Particular attention is given to regions prone to nerve compression, such as the suprascapular notch, to provide insights that can enhance surgical techniques and reduce complications. We hypothesized that the distance from anatomic landmarks, such as the anterolateral corner of the acromion to the suprascapular notch, remains relatively constant regardless of the patient's sex and height.
Methods
This study utilized 22 shoulders from 11 full-body Thiel-embalmed cadavers,5,16,17 sourced from the Surgical Training Center at the Faculty of Medicine, Chulalongkorn University, Thailand. Cadavers exhibiting gross deformities, previous shoulder surgeries, or rotator cuff tears were excluded. The study received approval from the institutional review board of the Faculty of Medicine, Chulalongkorn University, in accordance with international guidelines for human research ethics and protection.
Dissection Procedures
After positioning each cadaver in a beach-chair position with the arm in 30° of abduction and 10° of external rotation, the dissection was performed by fellowship-trained sports medicine surgeons (T.I. and N.T.). The procedure began with a large, curved skin incision extending from the anterior aspect, approximately 4 to 5 cm inferior to the tip of the coracoid process, to the posterior aspect, approximately 4 to 5 cm inferior to the scapular spine. A subcutaneous skin flap was created to expose the deltoid muscle, which was then carefully detached from its attachments at the acromion process and clavicle. The supraspinatus muscle was carefully dissected from the suprascapular fossa and retracted posteriorly to expose the suprascapular notch, the suprascapular nerve, and the transverse scapular ligament, with meticulous attention to avoid damaging the suprascapular nerve as it emerged from the suprascapular notch (Figure 1).
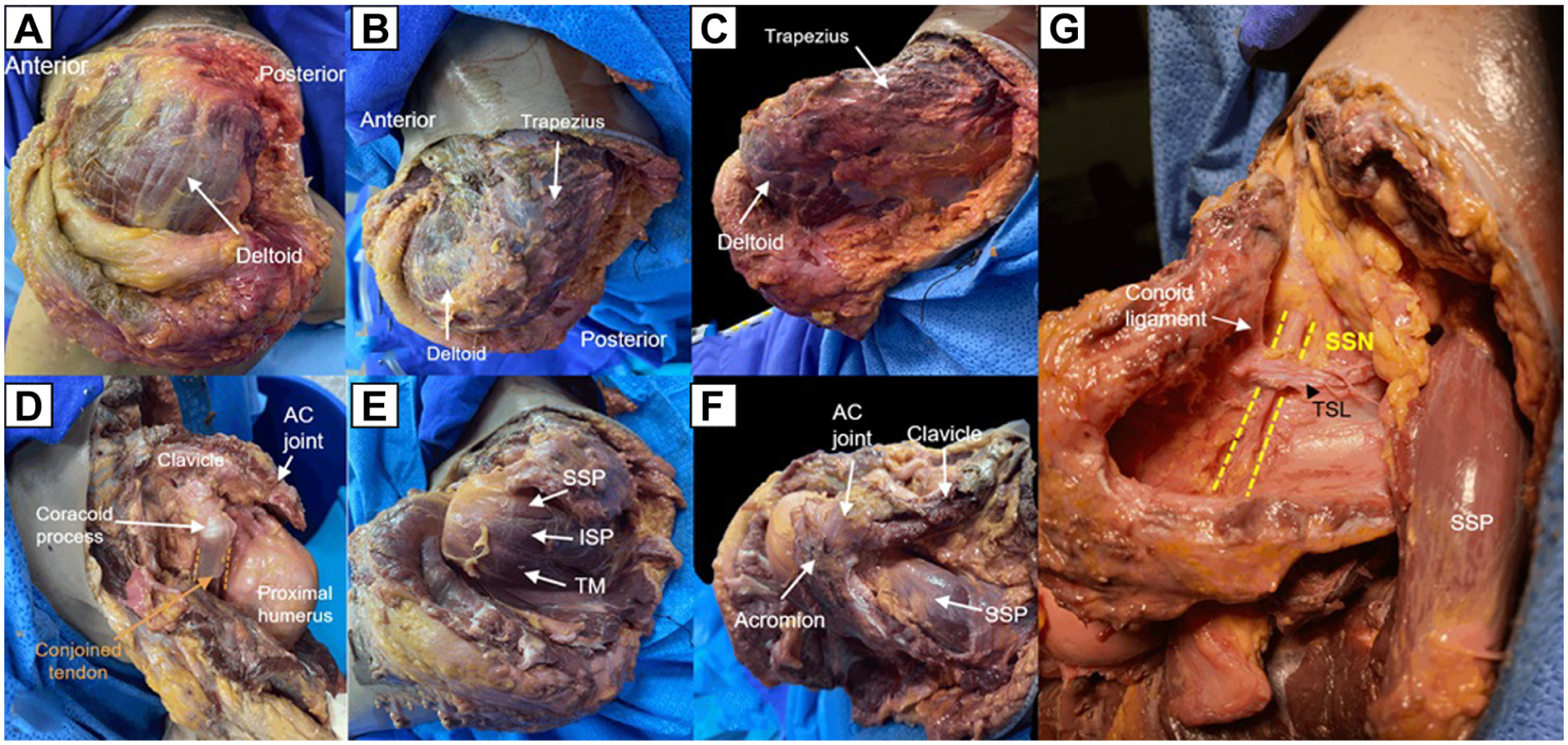
Cadaveric dissection steps: (A) Lateral view of the left shoulder, showing a large, curved incision extending from the anterior to posterior side to expose the deltoid muscle. (B) Superior view of the left shoulder, showing a large, curved incision from the anterior to posterior side to expose the deltoid and trapezial muscles. (C) Posterior view of the left shoulder, showing a large, curved incision from the anterior to posterior side to expose the deltoid and trapezial muscles. (D) Anterior view of the left shoulder, showing the deltoid muscle cut from its insertions at the acromion, clavicle, and scapular spine, exposing the tip of the coracoid process, the acromioclavicular (AC) joint, and the proximal humerus. (E) Posterior view of the left shoulder, showing the supraspinatus (SSP), infraspinatus (ISP), and teres minor (TM) muscles. (F) Superior view of the left shoulder after detaching the deltoid muscle from the acromion, clavicle, and scapular spine. (G) Superior view of the left shoulder, showing the SSP muscle cut and retracted posteriorly to expose the suprascapular notch, the suprascapular nerve (SSN), and the transverse scapular ligament (TSL).
Outcome Measures
Following exposure, the bony landmarks and arthroscopic (soft tissue) landmarks were marked by a researcher (P.P.) for measurement. Two fellowship-trained sports medicine surgeons (T.I. and N.T.) independently measured the distances and angles using a digital vernier caliper and digital goniometer (EC10; Becker), with an accuracy of 0.01 mm. To minimize measurement error, each surgeon performed 3 independent measurements for each point, and the mean was calculated. If the means differed by >10%, a third author (D.L.) was consulted for reevaluation.
This cadaveric study grouped measurements into 4 categories: bony landmarks, arthroscopic landmarks, angles, and the suprascapular nerve within the suprascapular notch. The bony and arthroscopic (soft tissue) landmarks specifically measured the distances to the suprascapular nerve, while the angles assessed anatomic landmarks to guide the placement of arthroscopic portals for scapular nerve navigation.
Bony Landmarks
The selected landmarks were chosen for their relevance to arthroscopic approaches to the shoulder, particularly in portal placement and nerve decompression. The study identified the following specific distances for measurement (Figures 2 and 3).
D1: from the posterolateral acromion to the suprascapular nerve at the suprascapular notch.
D2: from the anterolateral acromion to the suprascapular nerve at the suprascapular notch.
D3: from the tip of the coracoid process to the suprascapular nerve at the suprascapular notch.
D4: from the superolateral aspect of the glenoid to the suprascapular nerve at the suprascapular notch.
D5: the perpendicular distance from the acromion to the suprascapular nerve.
D6: from the posterolateral acromion to the closest point on the acromion to the suprascapular nerve.

(A) Illustration showing the superior view of the left shoulder with bony landmarks and measured distances. (B) Left cadaveric shoulder displaying bony landmarks and measured distances: from the posterolateral acromion to the suprascapular nerve at the suprascapular notch (D1); from the anterolateral acromion to the suprascapular nerve at the suprascapular notch (D2); and from the tip of the coracoid process to the suprascapular nerve at the suprascapular notch (D3). SSP, supraspinatus muscle; SSN, suprascapular nerve; TSL, transverse scapular ligament.

(A) Illustration showing the superior view of the left shoulder with bony landmarks and measured distances. (B) Left cadaveric shoulder displaying bony landmarks and measured distances: from the superolateral aspect of the glenoid to the suprascapular nerve at the suprascapular notch (D4). (C) Left cadaveric shoulder displaying bony landmarks and measured distances: the perpendicular distance from the acromion to the suprascapular nerve (D5). (D) Left cadaveric shoulder displaying bony landmarks and measured distances: from the posterolateral acromion to the closest point on the acromion to the suprascapular nerve (D6). SSP, supraspinatus muscle; SSN, suprascapular nerve; TSL, transverse scapular ligament.
Although the bony landmarks used in this study are subcutaneous, in vivo application may be affected by patient soft tissue thickness, particularly in individuals with higher body mass index. This limitation must be considered when translating cadaveric measurements into surgical practice.
Arthroscopic (Soft Tissue) Landmarks
The selected landmarks were chosen for their relevance to arthroscopic soft tissue navigation. The study identified the following specific distances for measurement (Figure 4, A and B).
S1: from the origin of the coracoacromial ligament at the acromion to its posterior insertion at the coracoid.
S2: rom the posterior coracoacromial ligament at the acromion to the conoid ligament.

(A) Illustration showing the anterior view of the left shoulder with arthroscopic (soft tissue) landmarks and measured distances. (B) Left cadaveric shoulder displaying arthroscopic (soft tissue) and measured distances: from the origin of the coracoacromial ligament at the acromion to its posterior insertion at the coracoid (S1) and from the posterior coracoacromial ligament at the acromion to the conoid ligament (S2). (C) Illustration showing the superior view of the left shoulder with suprascapular notch anatomy and measured distances. (D) Left cadaveric shoulder displaying arthroscopic (soft tissue) and measured distances: notch width (L1). (E) Illustration showing the superior view of the left shoulder with suprascapular notch anatomy and measured distances. (F) Left cadaveric shoulder displaying arthroscopic (soft tissue) and measured distances: from the suprascapular nerve to the lateral border of the notch (L2). CAL, coracoacromial ligament; SSN, suprascapular nerve; TSL, transverse scapular ligament.
Position of the Suprascapular Nerve in the Suprascapular Notch
The suprascapular notch was initially classified according to the Rengachary et al 12 system. The structure and location of the suprascapular nerve within the notch were evaluated by measuring (Figure 4, C-F).
L1: notch width.
L2: distance from the suprascapular nerve to the lateral border of the notch.
Angles to the Transverse Scapular Ligament
The angles were measured with a focus on their relevance to the Neviaser and anterior portals (Figure 5). 13
A1: angle from the posterior acromion to the suprascapular notch, representing the trajectory surgeons use when accessing the suprascapular nerve and transverse scapular ligament via the Neviaser portal. 13 This angle is crucial for optimizing the orientation of cutting instruments, facilitating a perpendicular approach to the transverse scapular ligament and thereby enhancing cutting efficiency and accuracy.
A2: angle from the tip of the coracoid process to the suprascapular notch and transverse scapular ligament, essential for accessing the nerve via the anterior portal. This angle helps define the boundaries for portal access from the anterior aspect of the shoulder, aiding in effective portal planning for the release of the transverse scapular ligament.

(A) Illustration showing the lateral view of the left shoulder with bony landmarks and measured angle: angle from the posterior acromion to the suprascapular notch (A1). (B) Left cadaveric shoulder displaying bony landmarks and measured A1 angle. (C) Illustration showing the superior view of the left shoulder with bony landmarks and measured angle: angle from the tip of the coracoid process to the suprascapular notch and transverse scapular ligament (A2). (D) Illustration showing the lateral view of the left shoulder with bony landmarks and measured A2 angle. (E) Left cadaveric shoulder displaying bony landmarks and measured A2 angle. TSL, transverse scapular ligament.
Statistical Analysis
All statistical analyses were conducted using STATA Version 18.0 (StataCorp). Demographic data, along with measurements of bony and arthroscopic landmarks, angles, and the position of the suprascapular nerve, were reported using means and standard deviations for continuous variables. The data were analyzed to determine whether anatomic measurements were influenced by sex or height. Pearson correlation coefficients (r) were calculated to examine the relationship between measurements and cadaveric height, while independent t tests were employed to compare measurements between male and female cadavers. Statistical significance was defined as a P value <.05.
To address potential bias from bilateral measurements, we conducted a sensitivity analysis restricted to 1 shoulder per cadaver (n = 11).
Sample size calculations were based on previously published data, 14 and to achieve a power of 80% with an alpha of .05, the minimum required sample size was determined to be 13. To account for potential dropouts or incomplete data, the sample size was increased by 20%, resulting in a minimal required sample size of 16.
Results
Demographic Data
A total of 11 cadavers (22 shoulders) were included in the analysis, consisting of 6 male and 5 female specimens. The mean age of the cadavers was 80 ± 16.6 years, with a mean height of 161 ± 5.0 cm.
According to the Rengachary classification, 12 20 out of 22 shoulders (90.9%) were classified as type 3 (U-shaped), while 2 shoulders (9.1%) were classified as type 1 (depression type).
Bony Landmarks and Correlation With Height
The distances from various bony landmarks to the suprascapular nerve at the suprascapular notch demonstrated variability. The mean distance from the posterolateral acromion (D1) was 58.34 ± 6.58 mm, ranging from 48.22 mm to 72.31 mm, with a moderate positive correlation with patient height (r = 0.51; P = .02). The anterolateral acromion (D2) measured 59.50 ± 5.22 mm, with a weaker correlation with height (r = 0.11; P = .64). The coracoid tip (D3) showed a mean distance of 46.49 ± 3.12 mm and a correlation coefficient of 0.30 (P = .17). The superolateral aspect of the glenoid (D4) had a mean distance of 39.26 ± 4.93 mm and a moderate correlation with height (r = 0.46; P = .03). The perpendicular distance from the acromion (D5) was 36.72 ± 6.37 mm, with a low correlation with height (r = 0.20; P = .38). Last, the shortest distance from the posterolateral acromion (D6) was 45.74 ± 6.48 mm, with a moderate positive correlation (r = 0.44; P = .04) (Table 1).
Distances and Position of the Suprascapular Nerve and Correlation With Height

Statistically significant at P < .05.
Indicates a moderate relationship with height. D1, distance from the posterolateral acromion to the suprascapular nerve at the suprascapular notch; D2, distance from the anterolateral acromion to the suprascapular nerve at the suprascapular notch; D3, distance from the tip of the coracoid process to the suprascapular nerve at the suprascapular notch; D4, distance from the superolateral aspect of the glenoid to the suprascapular nerve at the suprascapular notch; D5, perpendicular distance from the acromion to the suprascapular nerve; D6, distance from the posterolateral acromion to the closest point on the acromion to the suprascapular nerve; L1, width of the suprascapular notch; L2, distance from the suprascapular nerve to the lateral border of the notch; S1, distance from the origin of the coracoacromial ligament at the acromion to its posterior insertion at the coracoid; S2, distance from the posterior coracoacromial ligament to the conoid ligament.
Arthroscopic (Soft Tissue) Landmarks and Correlation With Height
The arthroscopic measurements showed that the mean distance from the coracoacromial ligament origin (S1) to the suprascapular nerve was 28.18 ± 4.51 mm, ranging from 21.16 mm to 36.31 mm, with a negligible correlation with height (r = 0.08; P = .72). The posterior coracoacromial ligament insertion (S2) distance averaged 29.94 ± 6.19 mm, ranging from 21.40 mm to 41.81 mm, with a weak correlation with height (r = 0.28; P = .21) (Table 1).
The arthroscopic landmarks S1 and S2 showed minimal correlation with height, without statistical significance (r = 0.08 and r = 0.28, respectively) (Table 1).
Position of the Suprascapular Nerve in the Suprascapular Notch and Correlation With Height
The width of the suprascapular notch (L1) was 9.93 ± 1.34 mm, ranging from 8.16 mm to 12.38 mm, with a low correlation with height (r = 0.09; P = .68). The distance from the nerve to the lateral border of the notch (L2) was 4.67 ± 1.27 mm, ranging from 2.36 mm to 6.72 mm, with no significant correlation with height (r = 0.07; P = .77) (Table 1).
The position of the suprascapular nerve in the suprascapular notch showed weak correlations with height for both L1 and L2 (r = 0.09 and r = 0.07, respectively), without statistical significance (Table 1).
Angles to the Transverse Scapular Ligament and Correlation With Height
The angles measured from bony landmarks to the suprascapular notch revealed varying degrees of correlation with patient height. The angle from the posterior acromion to the suprascapular notch (A1) had a mean of 83.74°± 16.71°, with a range of 43.09° to 110.00°. This parameter exhibited a very weak correlation with height (r = 0.06; P = .78) (Table 2).
Angles From Various Bony Landmarks to Suprascapular Nerve and Their Correlation With Patient Height

Statistically significant at P < .05.
Indicates a moderate relationship with height. A1, angle from the posterior acromion to the suprascapular notch; A2, angle from the tip of the coracoid process to the suprascapular notch and transverse scapular ligament.
In contrast, the angle from the coracoid tip to the suprascapular notch and transverse scapular ligament (A2) demonstrated a mean of 84.73°± 6.83°, ranging from 71.00° to 100.00°. This parameter showed a moderate positive correlation with patient height (r = 0.61; P = .002), indicating a statistically significant relationship (Table 2).
Sex Differences
The comparison of measured variables between male and female cadavers revealed significant differences in several parameters (Table 3).
Results of Comparison of Measured Variables Between Female and Male Cadavers

Statistically significant at P < .05. A1, angle from the posterior acromion to the suprascapular notch; A2, angle from the tip of the coracoid process to the suprascapular notch and transverse scapular ligament; D1, distance from the posterolateral acromion to the suprascapular nerve at the suprascapular notch; D2, distance from the anterolateral acromion to the suprascapular nerve at the suprascapular notch; D3, distance from the tip of the coracoid process to the suprascapular nerve at the suprascapular notch; D4, distance from the superolateral aspect of the glenoid to the suprascapular nerve at the suprascapular notch; D5, perpendicular distance from the acromion to the suprascapular nerve; D6, distance from the posterolateral acromion to the closest point on the acromion to the suprascapular nerve; L1, width of the suprascapular notch; L2, distance from the suprascapular nerve to the lateral border of the notch; S1, distance from the origin of the coracoacromial ligament at the acromion to its posterior insertion at the coracoid; S2, distance from the posterior coracoacromial ligament to the conoid ligament.
The distances from bony landmarks to the suprascapular nerve showed notable sex differences. Male cadavers had greater mean distances compared with females for D1 (63.38 ± 3.90 mm vs 52.29 ± 2.79 mm; P < .001), D2 (63.09 ± 3.49 mm vs 55.20 ± 3.30 mm; P < .001), D5 (39.18 ± 7.07 mm vs 33.76 ± 3.97; P = .044), and D6 (48.94 ± 5.11 mm vs 41.90 ± 6.01 mm; P = .007). The other bony landmarks, including D3 and D4, showed no statistically significant differences between male and female specimens.
Among the arthroscopic (soft tissue) landmarks, the distance from the origin of the coracoacromial ligament (S1) was significantly greater in male compared with female cadavers (30.44 ± 4.23 mm vs 25.47 ± 3.26 mm; P = .007). However, the posterior coracoacromial ligament distance (S2) showed no statistically significant difference between sex (P = .12).
The angles to the transverse scapular ligament exhibited no statistically significant sex differences. The mean angle A1 (posterior acromion to the suprascapular notch) was 86.43°± 11.59° in males and 80.51°± 21.59° in females (P = .42). Similarly, the mean angle A2 (coracoid process to the suprascapular notch and transverse scapular ligament) was comparable between males (84.75°± 8.76°) and females (84.70°± 3.88°) (P = .99).
No statistically significant sex differences were observed in the width of the suprascapular notch (L1) or the distance from the suprascapular nerve to the lateral border of the notch (L2). The mean width (L1) was 9.73 ± 1.38 mm in male and 10.16 ± 1.33 mm in female specimens (P = .47), while the distance (L2) was 4.34 ± 0.74 mm in male and 5.08 ± 1.67 mm in female specimens (P = .18).
Potential Bias From Bilateral Measurements
Sensitivity analyses revealed no statistically significant differences between the full data set and single-shoulder subset (all P values >.05) (Table 4). This approach yielded results congruent with our primary analysis, suggesting minimal influence of intra-cadaver dependency.
Sensitivity Analysis of Anatomic Measurements (Full Data Set vs Single-Shoulder Subset) a

Data are presented as mean ± SD unless otherwise indicated. P < .001 for intravariable correlations (eg, D1 in full data set vs subset). P values for group comparisons (full vs subset) calculated via paired t tests (for means) or Fisher z-transformation (for correlations).
Discussion
The most important finding of this study was the detailed anatomic relationships between the suprascapular nerve and its adjacent structures, which were critical for optimizing arthroscopic decompression procedures. By highlighting the complexity of the suprascapular nerve's position within the suprascapular notch, these findings underscored the importance of precise anatomic knowledge to improve surgical accuracy and minimize the risk of iatrogenic nerve injury. This understanding played a vital role in enhancing the safety and success of procedures targeting the suprascapular nerve.
Although the measurements were taken after removal of the skin and subcutaneous tissue, which limits direct application to live surgical conditions, the data offer valuable insights into the spatial anatomy relevant to arthroscopic portal planning. The distances from bony landmarks can help guide surgeons in approximating portal incision sites using surface anatomy, while the soft tissue (arthroscopic) landmarks assist in safely identifying the suprascapular nerve during decompression procedures. Furthermore, the measured angles support the use of anterior and Neviaser portals as optimal working trajectories for resecting the transverse scapular ligament. In clinical practice, combining these anatomic references with preoperative imaging, such as magnetic resonance imaging to assess soft tissue thickness, may further enhance the accuracy and safety of portal placement.
The measured distances between the suprascapular nerve and key bony landmarks, including the acromion, coracoid process, and glenoid, demonstrated strong alignment with previously reported values, thereby validating the findings of this study. Qawasmi et al 11 reported in their cadaveric study that a suprascapular nerve injection positioned approximately 3 cm from the posterior acromioclavicular joint vertex may accurately target the nerve. Terra et al, 15 in an anatomic investigation involving 16 cadavers, reported a mean distance of 61.0 mm from the superior edge of the acromion to the suprascapular nerve at the suprascapular notch. This value closely corresponded to the mean D1 and D2 measurements observed in this study (58.34 ± 6.58 mm and 59.50 ± 5.22 mm, respectively). Such consistency underscores the reliability of these anatomic landmarks as critical guides for surgical approaches to the suprascapular nerve. Gumina et al, 6 in their study of dried scapulae, reported a distance of approximately 30.1 mm from the supraglenoid tubercle to the suprascapular notch. In contrast, the present study found a mean D4 value of 39.26 ± 4.93 mm, which is significantly greater. This difference is likely due to the inclusion of soft tissue in our cadaveric study, which increases the measured distances. The higher values observed here may enhance the reliability of this parameter as a landmark for suprascapular nerve release. Unlike many previous studies,6,14,15 this study uniquely focuses on the application of anatomic insights to arthroscopic transverse scapular ligament release. Despite its clinical significance, this topic remains underexplored, making these findings particularly valuable for advancing surgical techniques.
Regarding height-related correlations, a moderate relationship was observed between cadaveric height and distances such as D1 (r = 0.51), D4 (r = 0.46), and D6 (r = 0.44). These results suggest that taller individuals may require tailored adjustments in arthroscopic portal placement to account for the increased distances between the suprascapular nerve and key bony landmarks.
A2 angle demonstrated a statistically significant and strong correlation with height (r = 0.61), indicating that taller individuals tend to have a wider lateral angle. This finding suggests that taller individuals may have a larger area available for portal placement via the lateral approach, potentially improving surgical access. In contrast, the minimal correlation between height and most other measurements underscores the importance of individualized assessments to ensure precision.
Sex differences were observed in the suprascapular safe zone, with measurements of D1, D2, D5, D6, and S1 being statistically significantly greater in the male compared with female specimens. These findings highlight the importance of considering anatomic variability during preoperative planning, as it may affect portal placement and decompression techniques. Interestingly, female specimens showed longer distances for the S2 measurement than males, although this difference was not statistically significant (28.08 ± 4.16 mm in males vs 32.18 ± 7.61 mm in females; P = .12). This observation underscores the need for caution when using the S2 measurement as a guide for surgical decompression. Similarly, Gumina et al 6 analyzed 500 dry scapulae to define the safe zone of the suprascapular nerve. Although their study focused on a different anatomic location, their findings aligned with this study, showing sex-specific variations, with men having a larger posterosuperior limit and women displaying a larger posterior limit. On the other hand, the consistent dimensions of the suprascapular notch (L1 and L2) across both sexes suggest that nerve entrapment and the feasibility of release are not significantly influenced by patient demographics. This consistency offers confidence that the same surgical technique can be applied to both male and female patients without major adjustments.
The anatomic characteristics of the suprascapular notch are vital for the safe and effective execution of arthroscopic decompression. Serving as the primary passageway for the suprascapular nerve, the suprascapular notch is a key site for potential nerve entrapment, underscoring the need for a thorough anatomic understanding in surgical planning. This study found that the suprascapular notch was predominantly classified as type 3 (U-shaped) in 90.9% of cases, which contrasts with the findings of Rengachary et al, 12 who reported 48% type 2 (U-shaped) and 31% V-shaped classifications. Interestingly, no V-shaped types were observed in this study. The measurements of the notch dimensions (L1 and L2) showed that the mean L2 (4.67 mm) was approximately half the value of the mean L1 (9.93 mm), suggesting that the suprascapular nerve is positioned in the middle of the suprascapular notch. This positioning allows for the release to be performed from either the medial or the lateral side.
Surgical Implications
On the basis of the findings of this study, the authors proposed the preferred technique for releasing the transverse scapular ligament using the landmarks 1 (Table 5, Figure 6). The patient should be positioned in a beach-chair position with the arm in 30° of abduction and 10° of external rotation, as done with the cadavers in this study. The authors recommend avoiding internal rotation of the arm, as this position may bring the suprascapular nerve close to the glenoid, increasing the risk of iatrogenic injury. This is supported by the study of Promsang et al, 10 which showed that the suprascapular nerve is closest to the posterior glenoid rim when the shoulder is internally rotated. The process begins by identifying bony landmarks, such as the acromion and coracoid, to approximate the suprascapular nerve's location at the suprascapular notch. These measurements aid in ensuring accurate surface anatomy–based incisions and portal placement. A standard posterior portal is initially established, followed by the evaluation of the subacromial space and the definition of anterior portal orientation using the A2 angle. Arthroscopic landmarks are then exposed through a bursectomy, with critical structures such as the coracoacromial ligament and conoid ligament serving as reliable references for locating the nerve. The transverse scapular ligament is addressed through triangulation techniques, utilizing the Neviaser portal and the A1 angle to ensure a trajectory perpendicular to the ligament. Accurate identification of the ligament allows for safe resection with minimal risk of iatrogenic injury.
Surgical Technique for Arthroscopic Suprascapular Nerve Decompression

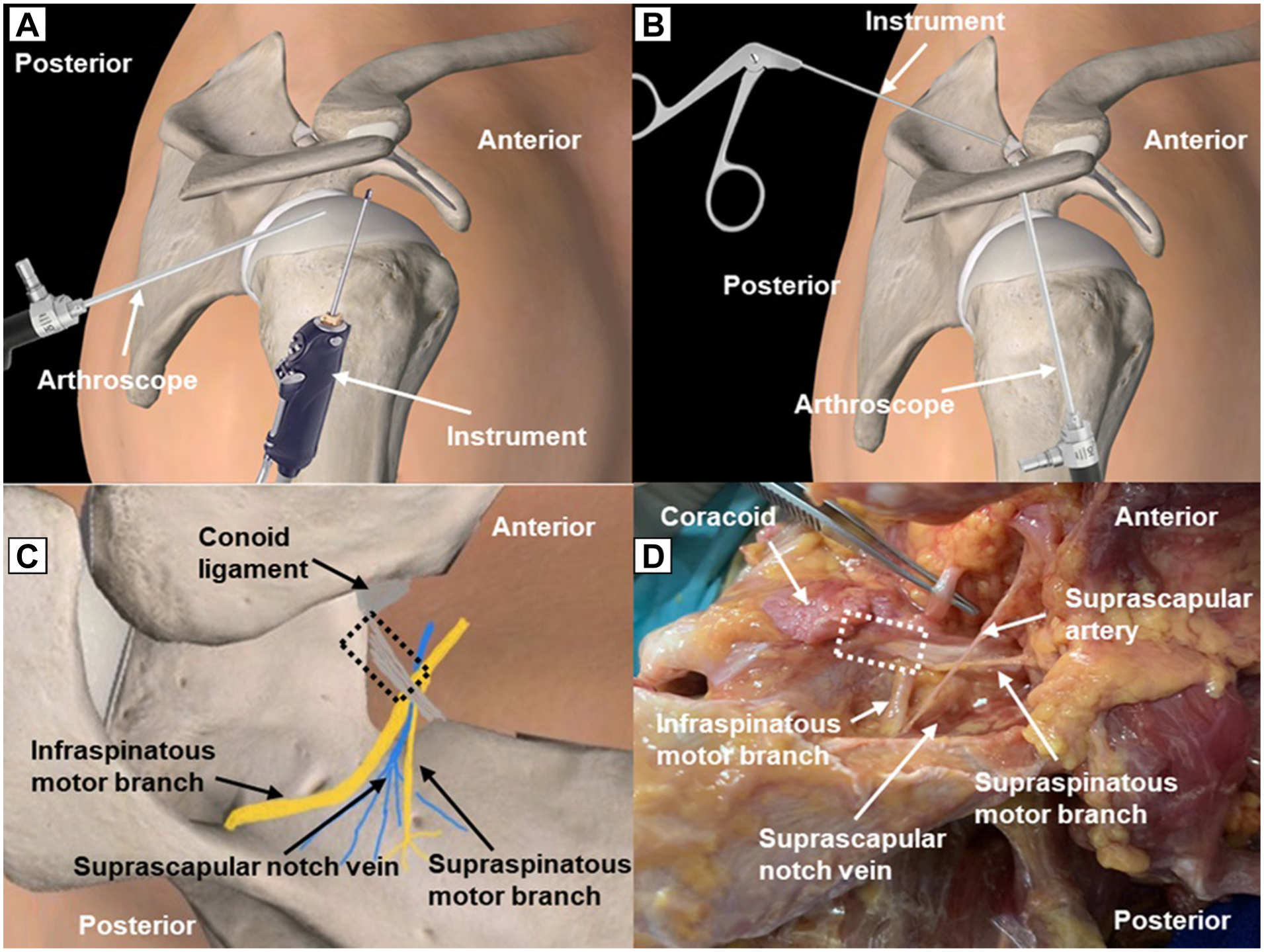
(A) Illustration of the lateral view of the right shoulder demonstrating the surgical technique for arthroscopic suprascapular nerve decompression. The arthroscope is inserted through the posterior portal, and the arthroscopic instrument is inserted through the lateral portal to perform bursectomy, exposing the soft tissue landmarks. (B) Illustration of the lateral view of the right shoulder demonstrating the surgical technique for arthroscopic suprascapular nerve decompression. The arthroscope is inserted through the lateral portal, and the arthroscopic instrument is inserted through the Neviaser portal to cut the transverse scapular ligament. (C) Illustration of the superior view of the left shoulder depicting the anatomy of the suprascapular nerve in the suprascapular notch and associated structures at risk. (D) Superior view of the left cadaveric shoulder showing the anatomy of the suprascapular nerve in the suprascapular notch and the associated structures at risk.
This study also highlights the position of the suprascapular nerve within the notch, with precise measurements of the notch's width and the relative position of the accompanying vein. A lateral or superior portal approach is recommended to reduce vascular or nerve injury risks. Finally, alternative approaches are suggested for cases involving concurrent superior labral lesions, 2 with anatomic landmarks such as D4 guiding surgical decision-making in these scenarios. This structured approach underscores the importance of anatomic precision in achieving safe and effective arthroscopic decompression of the suprascapular nerve.
Limitations
This study has several limitations. First, the cadaveric sample, sourced from elderly individuals, may not fully represent the anatomy of younger patients who typically undergo arthroscopic decompression for sports injuries or other causes of suprascapular nerve entrapment. As such, the anatomic variations observed may not be directly applicable to younger populations. Second, although Thiel-embalmed cadavers maintain excellent soft tissue preservation, they do not fully replicate the biomechanical and dynamic properties of living tissue, which may affect the validity of surgical simulation. Furthermore, postmortem body weight is not considered physiologically representative; as such, both body weight and body mass index were excluded from correlation analyses, in contrast to height, which remains a stable anthropometric parameter. Another limitation is the relatively small sample size, which may reduce the generalizability of the findings. The absence of functional testing in this cadaveric study also limits the ability to assess the actual clinical relevance of the anatomic findings. Furthermore, this study was conducted on fixed cadavers and did not account for dynamic variations present in living patients, such as soft tissue mobility or changes in nerve positioning due to muscle activity or joint motion. Coracoid morphology (eg, length and angulation), which may affect nerve relationships, was also not measured. To enhance clinical relevance, future studies should include these parameters, involve larger and more diverse populations, and consider the use of advanced imaging modalities such as computed tomography or magnetic resonance imaging for noninvasive, patient-specific anatomic assessment and preoperative planning. Longitudinal studies examining functional outcomes and the clinical effectiveness of the anatomic guidelines presented here could further enhance the applicability of these findings in real-world surgical settings. While we statistically controlled for bilateral dependency, the sample size remains modest. Future studies with larger, unilateral cohorts are needed to validate these findings.
Conclusion
This study demonstrated that the suprascapular nerve's distance to bony landmarks varies by sex, while arthroscopic and notch dimensions remain consistent. Height moderately influences certain bony landmark distances. These results provide essential anatomic references to enhance the precision of arthroscopic decompression.
Footnotes
Acknowledgements
The authors thank the Thai Orthopedic Society for Sports Medicine for their academic support.
Final revision submitted June 29, 2025; accepted August 15, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by grants for development of new faculty staff, Ratchadaphiseksomphot Fund, Chulalongkorn University (DNS_68_119_3000_012). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (No. 0668/67).
Data Accessibility Statement
Raw data can be made available upon reasonable request to the corresponding author.