
Abstract
Background:
Chronic Achilles tendon ruptures with large defects present a considerable challenge in treatment.
Purpose:
This study evaluated the midterm outcomes of fresh-frozen large-caliber allograft reconstruction for chronic Achilles tendon ruptures.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 32 patients (18 women and 14 men), with a mean age of 57.6 years (range, 21-81 years), were enrolled between 2007 and 2021. Of 32 ankles, 21 and 11 defects involved Achilles tendon ruptures at the middle and distal sections, respectively. The mean ruptured gap was 5.8 cm (range, 5-10 cm), and the mean follow-up period was 8.4 years (range, 3-16.9 years). The American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score, visual analog scale (VAS) score, and Achilles Tendon Total Rupture Score (ATRS) were used to evaluate the outcomes.
Results:
The patients’ AOFAS ankle-hindfoot score increased from 64.8 ± 10.8 to 95.4 ± 4.2 (P < .001), their mean VAS score decreased from 6.3 ± 0.9 to 1.7 ± 0.5 (P < .001), and their mean ATRS increased from 49.9 ± 12.6 to 97.9 ± 5.7 (P < .001). Three complications, comprising 2 superficial infections and 1 partial retear, were reported. No complete rerupture, revision reconstruction, or non-tendon healing was reported. At the final follow-up, no patient required an assistive device for ambulation, and good tissue incorporation was observed.
Conclusion:
Our midterm results revealed that fresh-frozen large-caliber tendon allografts represent a reasonable option for treating chronic Achilles tendon ruptures with large defects, achieving acceptable outcomes.
Keywords
The Achilles tendon is the strongest and largest fibrous cord in the human body, connecting the calf muscles to the calcaneus bone. 54 An acute Achilles tendon rupture is the most common type of tendon rupture in the lower extremity, 48 and it often occurs due to activities and incidents such as participating in recreational sports, jumping, falling from a height, and stepping into a hole. 31 The Achilles tendon typically ruptures after a sudden increase in the stress on the tendon due to an eccentric contraction, 55 and Achilles tendon rupture occurs in a relatively hypovascular area located 4 to 7 cm above its insertion into the calcaneus. 9
This type of rupture (75%) is frequently observed in men aged between 30 and 40 years, and it is prevalent in approximately 25% of sedentary patients. 31 However, because of its high incidence, >20% of acute ruptures are misdiagnosed. 42 Chronic ruptures of the Achilles tendon are those that are delayed diagnosed for ≥6 weeks after the original injury. 17 Managing chronic Achilles tendon rupture is challenging because primary repair with end-to-end approximation is often impossible because of tendon retraction, particularly when the gap is excessively large. The gap size is defined by the Myerson classification, 38 with type 1 being <2 cm, type 2 between 2 and 5 cm, and type 3 being larger than 5 cm. Currently, surgical intervention remains the gold standard for treating neglected Achilles tendon ruptures.10,25,30 Although various surgical methods have been proposed,2,14,47 no standardized treatment exists for large gap Achilles tendon ruptures.
In our study, we aimed to evaluate the clinical outcomes of fresh-frozen large-caliber tendon allograft (predominantly Achilles allograft) reconstruction and assess the durability of graft incorporation at midterm follow-up.
Methods
From October 2007 to August 2021, our hospital treated a total of 62 patients with chronic Achilles tendon ruptures (Figure 1). We enrolled patients who met the following criteria: (1) were at least 18 years old; (2) had a documented history of Achilles tendon trauma with an injury duration >6 weeks; (3) were unable to perform a single-limb heel rise; (4) had magnetic resonance imaging (MRI) findings and clinical presentation consistent with chronic Achilles tendon rupture; and (5) had an intraoperative debridement gap >5 cm. Patients with open Achilles tendon ruptures, local infection near the rupture site, or combined neurovascular injury were excluded from the present study.

Flowchart of patient selection process.
All included patients had a minimum follow-up period of 3 years. A total of 32 patients met the criteria (Figure 1 and Table 1), and a single surgeon (C.-C.W.) performed all Achilles allograft reconstruction procedures. Of the 32 procedures, 4 patients received a patellar tendon allograft, 4 patients received a quadriceps tendon allograft, and 24 patients received an Achilles tendon allograft (Figure 2). Graft selection was based on preoperative MRI evaluation of the expected defect size after debridement. When Achilles tendon allograft availability was limited, patellar tendon or quadriceps tendon allografts were selected for defects measuring approximately 4 to 6 cm after debridement. For patients with larger defects beyond this range, we preferentially waited for Achilles tendon allograft availability to ensure adequate graft size. Patellar tendon allografts were harvested from donors <30 years old to optimize graft quality, while quadriceps tendon allografts were trimmed intraoperatively for size matching. In cases where debridement resulted in a distal stump of <2 cm from the calcaneal insertion, consistent with a sleeve avulsion-type rupture, we utilized grafts with 1 bone block to allow for bone-to-bone fixation at the insertion site. All 32 patients underwent pre- and postoperative (at 6 months after surgery) sonographic and MRI evaluations.
Demographic Characteristics of Patients With Chronic Achilles Tendon Ruptures a
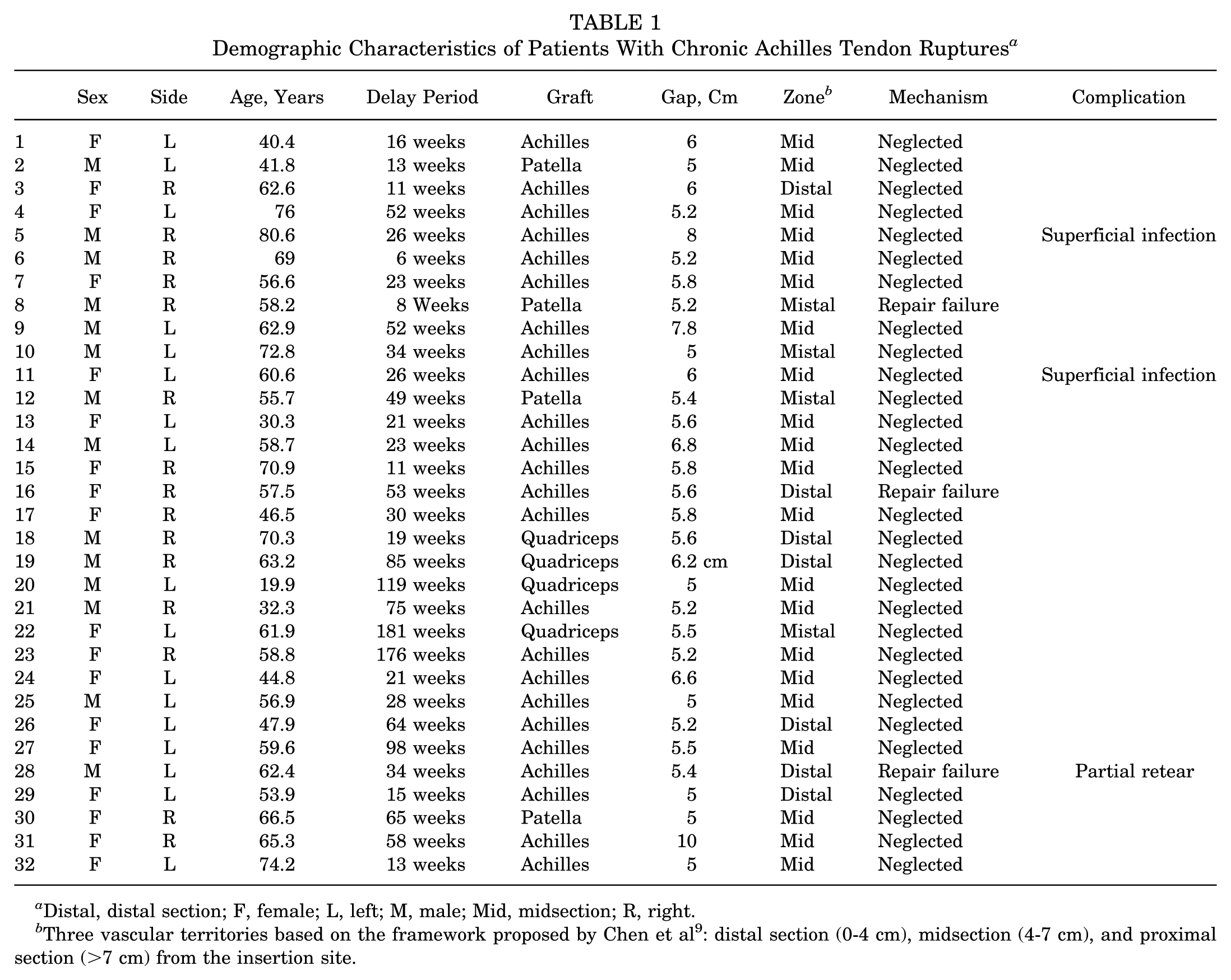
Distal, distal section; F, female; L, left; M, male; Mid, midsection; R, right.
Three vascular territories based on the framework proposed by Chen et al 9 : distal section (0-4 cm), midsection (4-7 cm), and proximal section (>7 cm) from the insertion site.

(A and B) A sterile, sealed envelope containing the fresh-frozen Achilles allograft is opened and inspected in the surgical suite. The Achilles allograft is subsequently placed in a warm 0.9% saline solution containing gentamicin for thawing and antibiotic soaking on the back table. After thawing, the allograft specimen is examined to identify the fiber track. (C) A quadriceps tendon allograft was prepared with a bone block at one end for bone-to-bone fixation. (D) A patellar tendon allograft harvested from a young male donor can typically be used to reconstruct defects of approximately 6 cm in length.
Surgical Technique
All operations were performed by 1 senior orthopaedic surgeon (C.-C.W.) in a single hospital. After suitable anesthesia, the patient was placed in a prone position on the operative table, and a thigh tourniquet was applied. A lazy S skin incision was made, deepened to the paratenon. The sheath was then incised, carefully preserving the surrounding layers, and the injured Achilles tendon was exposed. The interposed fibrotic tissue was debrided to the level of the deep fascia, and the ruptured stump was refreshed until healthy tendon texture was visible. The ruptured gap was measured with the ankle in a neutral position. After debridement, an end-to-end repair was attempted, and if this was impossible, reconstruction would be considered. The prepared fresh-frozen Achilles tendon allograft was applied to the defect area. Distal fixation was achieved using Bunnell sutures with 2-0 Ethibond, which provides a locking stitch configuration that distributes tension evenly across the graft, minimizes focal stress concentration, and promotes optimal tendon healing. If the distal stump was insufficient for approximation, a tendon allograft with a calcaneus bone block was used and fixed with screws (Figures 3 -5). The tension of the Achilles tendon was adjusted using the Thompson test, the 53 palpation test, and the Matles test. 34 For the Matles test, the patient was placed in a prone position with both knees passively flexed to 90°. The resting angle of the ankle on the operated side was compared with that of the contralateral, uninjured side. A decreased plantarflexion angle relative to the uninjured side indicated insufficient tension of the reconstructed tendon. Proximal stump approximation was adjusted accordingly to achieve symmetry between both sides. Subsequently, the wound was closed in layers after copious lavage with normal saline. The paratenon was closed using 3-0 Vicryl sutures, followed by subcutaneous closure with 2-0 Vicryl sutures. Skin closure was performed with 3-0 Nylon sutures.
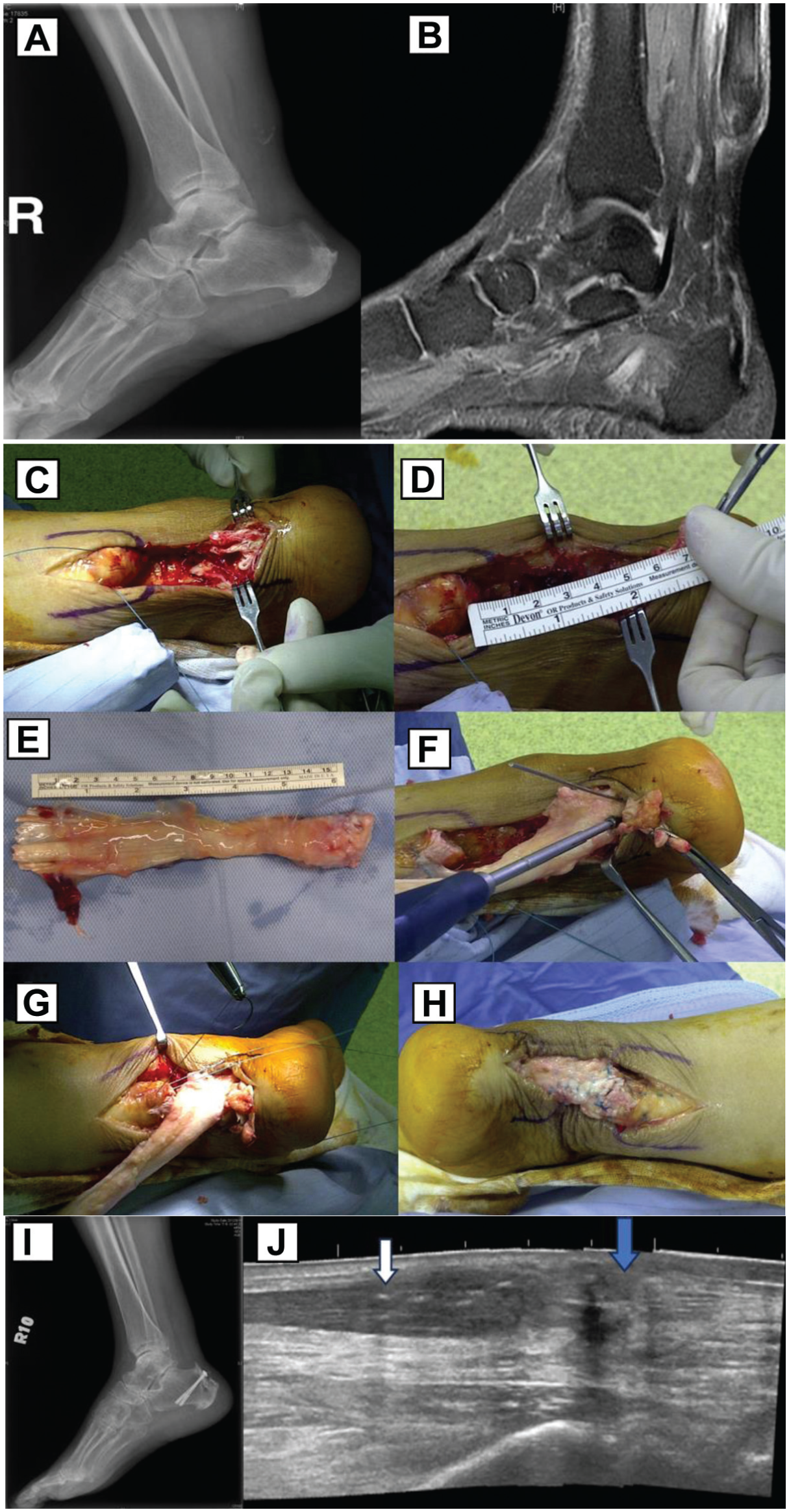
(A and B) A 63-year-old female patient with right Achilles tendon tendinitis after a steroid injection presented with a rupture that had persisted for 3 months. (C) The interposed fibrotic tissue is debrided to the level of the deep fascia. (D) The rupture gap is measured. (E) The fresh-frozen Achilles tendon allograft is prepared. (F) The graft is secured with two 4.0-mm cannulated screws. (G and H) The allograft is tensioned and repaired to the native Achilles tendon using the Bunnell method. (I) Postoperative radiograph image. (J) An ultrasound scan performed 6 months after surgery revealed good fiber continuity at the repaired site. The blue arrow indicates the repaired tendon allograft, and the white arrow indicates the recipient tendon.

(A) A 63-year-old male patient with right chronic Achilles tendon tear with a 6.2-cm gap, reconstructed using a quadriceps tendon allograft. (B) Postoperatively, an anterior below-knee splint was used. (C) MRI at 2 years postoperatively revealed intact tendon continuity, with no evidence of swelling, inflammation, or fat infiltration. (D) Radiograph at 2 years revealed union. MRI, magnetic resonance imaging.

(A) A 56-year-old male patient with a right chronic Achilles tendon tear with a 5.4-cm gap, reconstructed using a patellar tendon allograft. (B) Postoperatively, an anterior below-knee splint was used (C). The 6-month postoperative MRI revealed mild fluid accumulation within the midsubstance of the tendon; however, overall continuity was well-maintained, with no evidence of swelling or inflammation. (D) Radiograph at 1 year revealed union. (E) Balance assessment: ability to maintain single-leg balance for at least 15 seconds without instability. (F) Assisted single-leg heel raises were achieved at 6-month follow-up. (G) A lazy-S incision was made to optimize wound healing by minimizing skin tension, enhancing vascular supply, and providing better exposure while reducing the risk of skin necrosis.
Postoperatively, an anterior below-knee splint was used to maintain the ankle in 20° of plantar flexion. During the first 2 weeks, patients were allowed to perform open-kinetic-chain exercises within a 0° to 20° of plantar flexion. From the second to the fourth week, the splint was replaced with a below-knee walking boot, and the range of motion for open-kinetic-chain exercises was increased from 20° of plantar flexion to 10° of dorsiflexion. From the fourth to the sixth week, the range of motion was increased by 10° each week, and closed-chain exercises were initiated. At this point, partial weightbearing with crutched-assisted ambulation was allowed. Between 8 and 12 weeks postoperatively, patients were permitted to engage in light activities such as stationary cycling or swimming. Stationary cycling was performed without a walking boot or brace. Between 12 and 24 weeks postoperatively, progression to higher-level activities was permitted based on functional assessments, including (1) balance assessment: ability to maintain single-leg balance for at least 15 seconds without instability; (2) calf strength testing: bilateral heel raise strength reaching at least 1.5 times body weight (simulated with additional handheld weights), with supplemental assisted single-leg heel raises targeting approximately 0.75 times body weight to minimize contralateral compensation; (3) range of motion: achievement of at least 95% of full ankle dorsiflexion and plantarflexion range to prevent limited excursion during impact activities; and (4) tendon healing confirmation: ultrasonography and MRI were routinely performed at approximately 6 months postoperatively to confirm satisfactory tendon healing before allowing high-impact activities such as running or jumping (Figure 6).

A 59-year-old male patient with a neglected Achilles tendon rupture sustained 5 months earlier. Intraoperatively, the gap measured 7 cm after debridement. We performed Achilles allograft reconstruction. (A) The MRI image taken 5 months after injury; (B), (C), and (D) display the MRI images taken at 6 months after surgery, including sagittal, coronal, and axial cuts. No fatty infiltration of the calf muscles and no muscle atrophy were noted. MRI, magnetic resonance imaging.
In the postoperative period, we evaluated patients at 6 months, 12 months, and annually thereafter, with a minimum follow-up duration of 3 years. We used the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score to measure pain, function, alignment, and patient-related outcomes, the visual analog scale (VAS) score to measure pain intensity, and the Achilles Tendon Total Rupture Score (ATRS) (see Appendix Table A1) to evaluate outcomes after treatment for complete Achilles tendon rupture. 40 MRI was performed at the 6-month follow-up and subsequently every 2 years to assess tendon status. Failure of allograft reconstruction was defined as traumatic or nontraumatic rerupture, tendon laxity, or the inability to perform daily activities, necessitating revision allograft reconstruction. We used paired t tests to compare the scores on the pre- and postoperative questionnaires. The significance level was set at P < .05.
Results
The 32 enrolled patients comprised 18 women and 14 men, with a mean age of 57.6 years (range, 21-81 years). Among the 32 Achilles tendons treated, 17 and 15 were on the left and right sides, respectively. The mean ruptured gap was 5.8 cm (range, 5-10 cm). Distal stump treatment involved sutures for tendon end-to-end repair in 21 patients and bone block fixation with screws in 11 patients. The mean follow-up period was 8.4 years (range, 3-16.9 years). No rerupture was noted. No nonunion was observed in the 11 patients who underwent screw fixation.
A total of 3 complications were reported. Two cases involved surgical wounds with poor healing and accompanying superficial infections; 1 case required 7 debridements, and the other required 2 debridements before the infections were eventually controlled and wound healing was achieved. The third reported complication was a partial retear, which was discovered 6 months postoperatively during vigorous exercise (Figure 7). This case was successfully treated with nonoperative management by restarting our standard postoperative rehabilitation protocol, as previously described, for an additional 6-month period. Healing was confirmed 1 year after surgery.

A 62-year-old male patient experienced a rerupture at 1 month after undergoing tendon repair for an acute Achilles tendon rupture. The patient was referred to our hospital 12 weeks after the acute rupture. Intraoperatively, the gap measured 5 cm, and we performed reconstruction with an Achilles allograft without a bone block. (A) Five months postoperatively, a partial retear (red arrow) was observed in the dorsal part of the Achilles tendon midportion. (B) The patient subsequently underwent nonoperative treatment. Subsequently, healing was achieved (indicated by the green arrow) 1 year after surgery.
All patients were followed up for a minimum of 3 years. The mean preoperative AOFAS score was 64.8 ± 10.9 (range, 36-79), and significantly increased to 91.5 ± 9.3 (range, 60-99) at 6 months postoperatively (P < .001). The mean AOFAS score further improved to 95.6 ± 3.7 (range, 88-100) at 12 months postoperatively (P < .001) (Figure 8A). It stabilized at 95.4 ± 4.2 (range, 83-100) at 24 months postoperatively, with no significant difference observed between the 12- and 24-month scores (P = .49) (Table 2). The mean preoperative VAS score was 6.3 ± 0.9 (range, 5-8), and significantly decreased to 2 ± 0.8 (range, 1-3) at 6 months postoperatively (P < .001). The mean VAS score further improved to 1.8 ± 0.9 (range, 0-3) at 12 months postoperatively (P = .03) (Figure 8B). It stabilized at 1.8 ± 0.6 (range, 1-3) at 24 months postoperatively, with no significant difference observed between the 12- and 24-month scores (P = .77) (Table 2). The mean preoperative ATRS score was 49.9 ± 12.6 (range, 33-70), and significantly increased to 94.4 ± 10.6 (range, 60-100) at 6 months postoperatively (P < .001). The mean ATRS score further improved to 97.8 ± 5.5 (range, 78-100) at 12 months postoperatively (P < .001) (Figure 8C). It stabilized at 97.8 ± 5.7 (range, 78-100) at 24 months postoperatively, with no significant difference observed between the 12- and 24-month scores (P = .83) (Table 2). The AOFAS, VAS, and ATRS scores plateaued after 12 months postoperatively, showing consistent functional recovery over time.

Trends of clinical outcome scores over time with mean ± SD.
Comparison of P Values for AOFAS, VAS, and ATRS Scores Across Different Time Points a
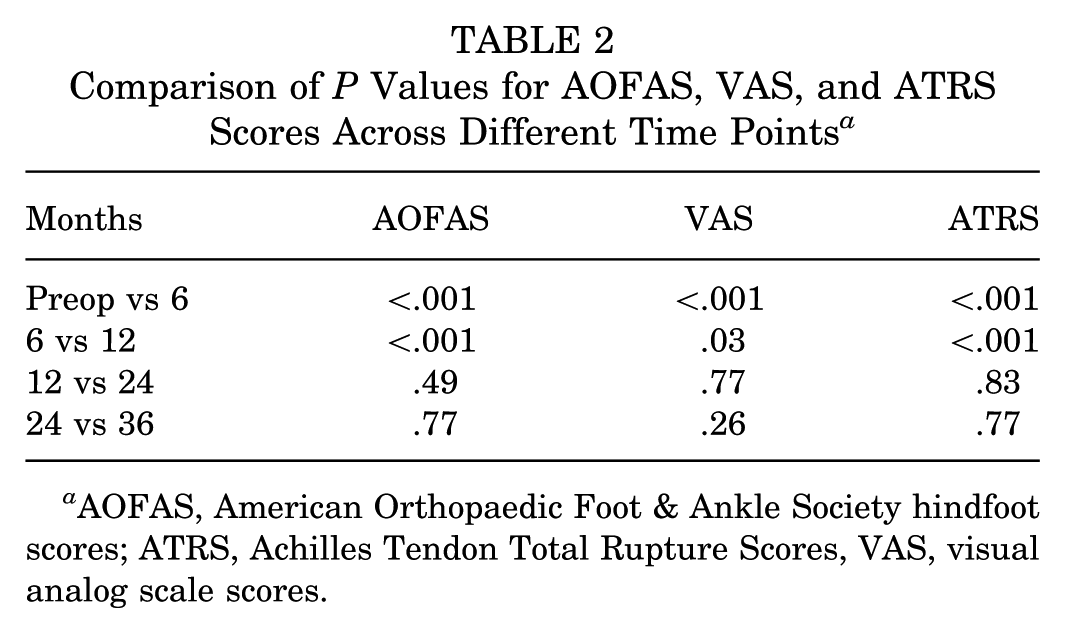
AOFAS, American Orthopaedic Foot & Ankle Society hindfoot scores; ATRS, Achilles Tendon Total Rupture Scores, VAS, visual analog scale scores.
Discussion
Achilles tendon ruptures are not uncommon and can be accurately diagnosed through a medical history review and physical examination. However, >20% of acute injuries are misdiagnosed or present late, leading to a chronic rupture. 42 A chronic Achilles tendon rupture poses various challenges in terms of treatment and limits the ability to perform active ankle plantar flexion. It can significantly disrupt normal gait patterns due to persistent weakness in plantarflexion, affecting the ability to push off and propel the body forward. This leads to slower gait speed, wider step width, shorter stride length, and a longer relative stance phase. 52 The tendon sheath frequently undergoes thickening and adheres to the retracted segments of the tendon, with little to no reparative tissue present in the intervening gap. 27
In cases of neglected Achilles tendon ruptures, a gap typically exists between the tendon ends because of the retraction of the proximal and distal stumps. This retraction causes a contraction of the triceps surae muscle bellies, resulting primarily in reduced ankle dorsiflexion and decreased muscle flexibility. Although contracture itself does not directly cause muscle weakness, the chronic shortening alters the muscle's length-tension relationship, thereby compromising the capacity to generate effective plantarflexion strength, particularly during dynamic activities. 44 This explains why most of the ruptures investigated in our study presented a gap exceeding 5 cm.
The timing and indication for treating chronic Achilles tendon rupture, according to Feng et al 15 , is to opt for surgical treatment only after 6 months of failed nonoperative treatment. However, in our case series, we proceed with surgical intervention when there is significant functional impairment (ie, pain, inability to perform a single heel rise, and disability in walking or climbing stairs), even if it has been <6 months. Among the patients with delays ranging from 6 weeks to 6 months, we attempted end-to-end repair but found it to be nearly impossible. Additionally, in our case series, the 3 complications observed all occurred in patients with delays >6 months.
The Achilles tendon is segmented into 3 vascular territories based on the framework proposed by Chen et al. 9 The pattern of blood supply leaves the Achilles tendon vulnerable to injury in a watershed area approximately 2 to 6 cm from its insertion on the posterior calcaneus. 45 The peroneal artery supplies the midsection (4-7 cm from insertion), while the posterior tibial artery supplies both the proximal (>7 cm) and distal (<4 cm) sections. In this study, we defined distal defects as those with a remaining distal stump of <4 cm after debridement, midsection defects as those between 4 and 7 cm, and proximal defects as those >7 cm. Midsection defects were typically managed with tendon-to-tendon sutures. However, in cases involving the distal section, if the refreshed stump end is <2 cm after debridement, which is characteristic of an Achilles sleeve avulsion type rupture, using tendon-to-tendon sutures often leads to suture cut-through or dislodgement. 29 Therefore, we opt for a bone block to achieve bone-to-bone fixation.
Chronic Achilles tendon ruptures are challenging to treat.19,28 Numerous surgical methods have been proposed for treating chronic Achilles ruptures, which are tailored to the gap size, tendon vascularity, and surgeon preference.4,7,8,14,27,43 Surgical methods are generally classified as direct end-to-end repair, Achilles tendon advancement or flap reconstruction, local tendon transfer, and implantation (autograft, allograft, and synthetic). 44
Several surgical techniques have been described for managing chronic Achilles tendon ruptures, with the choice often depending on the size of the defect, tissue quality, and the patient's functional demands. For moderate defects, the V–Y tendon advancement technique, first introduced by Abraham and Pankovich, 1 remains a commonly used method, especially for gaps between 2 and 5 cm; however, potential calf weakness due to muscle-tendon lengthening has been reported. Turndown fascial flaps, described by Christensen 10 and modified by Silfverskiöld 49 and Guclu et al, 19 have also demonstrated favorable outcomes; however, concerns remain regarding the risk of fascial flaps being too thin or fragile, which may compromise stability and strength, particularly in high-demand patients.
For larger defects, various tendon transfers have been utilized. Flexor hallucis longus transfer, as described by Wapner et al, 56 provides sufficient graft length while preserving ankle plantarflexor balance; however, patients may experience difficulty with sprinting due to reduced hallux push-off strength, which could significantly affect athletic performance. 35 Flexor digitorum longus (FDL) and peroneus brevis (PB) transfers have also been reported.32,35 While PB transfer can be a viable option, concerns exist regarding weakened ankle eversion after harvest. 38 Additionally, these tendon transfer procedures carry risks of donor site morbidity and may be limited by insufficient graft thickness, particularly in cases involving large defects. Moreover, evidence for FDL and PB transfers in managing large defects remains limited. While these techniques offer alternatives, each carries specific limitations, particularly when addressing extensive gaps exceeding 5 cm.
To restore a better biomechanical structure of the Achilles tendon, autograft and allograft grafts present as reasonable surgical options. The most commonly used autografts are the semitendinosus and quadriceps tendons. Semitendinosus grafts provide sufficient length and have shown favorable outcomes in some reports; however, higher complication rates, including infections, have also been documented, which limits their routine use. 51 Quadriceps tendon grafts offer the advantage of bone plug harvesting for bone-to-bone fixation, although clinical evidence supporting their use remains limited.6,37 In general, autograft procedures require multiple surgical sites and positioning, resulting in longer operative time and potential donor site morbidity.
Allografting is an alternative method for reconstructing chronic Achilles ruptures. Several recent studies have used allografts for this purpose.12,13,20,22,24,26,39,41,43 Through this method, Ofili et al 41 treated 14 patients with a mean defect size of 7 cm, and Jiménez-Carrasco et al 24 treated 8 patients with a mean defect size of 7.75 cm, with both of them reporting favorable outcomes. To the best of our knowledge, our study has the largest patient cohort in the literature to date. In the midterm follow-up, we also observed excellent clinical outcomes.
The caliber of an allograft is also a crucial concern. McCormick et al 36 performed dual semitendinosus allograft reconstruction, reporting no cases of rerupture and a high rate of good clinical outcomes (7/9) at short to midterm follow-up. Song et al 50 used single semitendinosus allografts to treat 34 patients, achieving good results. Over a mean follow-up period of 53 months (24-80 months), no infections or reruptures occurred. However, they did not specify the size groups of the gaps in which these small-caliber tendon allografts were used. Although no reruptures were noted, biomechanical research has indicated that 2 semitendinosus allografts provide superior tensile strength. 5 Our study included patients with gaps >5 cm, and we selected large-caliber tendon allografts, such as the patellar tendon, quadriceps tendon, or Achilles tendon. Although no clear evidence has been reported regarding the effectiveness of large-caliber versus small-caliber allografts in addressing large gaps, the use of large-caliber allografts for large gaps yielded good clinical outcomes in the present study.
Although the literature on the use of allografts for Achilles reconstruction indicates that reruptures are extremely rare, one of our patients exhibited signs of a retear at 6 months postoperation while participating in a high mountain expedition. In cases of acute Achilles tendon partial rupture, several studies have suggested that a rupture involving >50% of the cross-sectional area is an indication for surgery.21,46 However, our patient experienced a tear involving <50% of the cross-sectional area. We opted for nonoperative treatment based on the modified 3-month rehabilitation program by Masci and Alfredson, 33 which resulted in tendon healing. In addition to physiotherapeutic approaches, extracorporeal shockwave therapy and platelet-rich plasma injections are additional treatment options.16,23 However, no evidence-based treatment protocol is currently available for partial tears. 18
Allografts are not without drawbacks. Compared with autografts, they may have inferior tissue compatibility and require a longer period for incorporation and remodeling. Problems such as delayed union or nonunion after calcaneal bone block fixation have been reported, potentially necessitating extended partial weightbearing. 41 However, we typically perform bone block fixation in the distal section. According to Chen et al, 9 this area is not regarded as a relatively hypovascular zone, which may reduce concerns about nonunion. Additionally, no nonunion cases were observed among the 11 patients who underwent this procedure. Disease transmission is a concern in allografting. 11 Infections or wound issues have also been reported,3,4,20 but they are minor. Jiménez-Carrasco 24 successfully performed allograft reconstruction on a previously infected wound without leading to new infections or wound issues, and the allograft remained in good condition. Furthermore, no rerupture was reported in that study. In our case series, 2 patients experienced poor wound healing combined with local infection; however, their infections were brought under control after several debridement procedures and antibiotic treatment.
Allografting provides several advantages, including the ability to reconstruct larger defects, shorter surgical times, avoidance of donor site morbidity, and the provision of adequate tendon strength and length. When indicated, an allograft may be an effective and safe method for treating large chronic Achilles ruptures.
Limitations
This study has several limitations. First, it is a retrospective case series from a single surgeon's experience, which may limit generalizability and introduce selection bias. Second, while this represents one of the largest cohorts on large-gap Achilles reconstructions, the sample size remains relatively small, particularly for patients undergoing reconstruction with patellar tendon and quadriceps tendon allografts, which comprised 25% of the cohort. Third, outcome assessments primarily relied on subjective scoring systems (AOFAS, ATRS, or VAS), and additional objective biomechanical evaluations would strengthen the findings. Further prospective studies with larger cohorts and randomized designs are needed to validate these results.
Conclusion
Allograft reconstruction was successful in managing chronic Achilles tendon ruptures, particularly in cases with larger gaps. The midterm graft survival rate was favorable, with a high incorporation rate and a low graft collapse rate, even in hypovascular zones. Our study demonstrated that fresh-frozen allografts are a viable option for treating chronic Achilles tendon ruptures, yielding acceptable results.
Footnotes
Appendix
Achilles Tendon Total Rupture Score

| All questions refer to your limitations/difficulties related to your injured Achilles tendon. | ||||||||||
| Answer every question by grading your limitations/symptoms from 0-10. (0 = major limitations and 10 = no limitations) |
||||||||||
| 1. Are you limited due to decreased strength in the calf/Achilles tendon/foot? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 2. Are you limited due to fatigue in the calf/Achilles tendon/foot? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 3. Are you limited due to stiffness in the calf/Achilles tendon/foot? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 4. Are you limited due to pain in the calf/Achilles tendon/foot? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 5. Are you limited during activities of daily living? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 6. Are you limited when walking on uneven surfaces? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 7. Are you limited when walking quickly up the stairs or up a hill? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 8. Are you limited during activities that include running? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 9. Are you limited during activities that include jumping? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 10. Are you limited in performing hard physical labor? | ||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Total score: | ||||||||||
Final revision submitted June 15, 2025; accepted August 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Buddhist Tzu Chi Medical Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Buddhist Tzu Chi Medical Foundation, Taipei Tzu Chi Hospital