
Abstract
Background:
Treatment of isolated osteochondral lesions of the femoral head in young patients presents a clinical challenge for orthopaedic surgeons. Nonoperative management is associated with poor patient satisfaction and the development of osteoarthritis, while arthroplasty in young patients raises concerns regarding implant longevity.
Purpose:
To evaluate patient-reported outcome measures (PROMs) and the rate of conversion to THA after osteochondral allograft (OCA) transplantation via surgical hip dislocation (SHD) for isolated cartilage lesions of the femoral head.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent femoral head OCA via SHD at our institution between August 2010 and June 2023, with a minimum 2-year follow-up, were retrospectively reviewed. Demographic, perioperative, and complication data were collected prospectively from a registry. The Modified Harris Hip Score (mHHS) and the International Hip Outcome Tool-12 (iHOT-12) were administered pre- and postoperatively. The minimal clinically important difference (MCID) and patient acceptable symptom state (PASS) thresholds established for hip arthroscopy in patients with femoroacetabular impingement were used to assess patient outcomes.
Results:
A total of 24 patients (54% women; mean age, 22.4 years) were included. The mean lesion size was 488 mm2, and the mean OCA graft depth was 8.8 mm. At a mean follow-up of 47.9 months, mHHS scores improved from 62.1 preoperatively to 83.9 postoperatively (P < .001), and iHOT-12 scores improved from 35.5 preoperatively to 77.5 postoperatively (P < .001). The MCID was achieved by 67% and 76% of patients for the mHHS and the iHOT-12, respectively. The PASS was completed by 62% and 67% of patients for the mHHS and the iHOT-12, respectively. Two patients (8.3%) required subsequent hip arthroscopy, and 6 patients (25%) required conversion to hip arthroplasty at a mean of 3.8 years postoperatively (range, 0.75-10.3 years). Patients requiring conversion to THA demonstrated an increased OCA graft depth (P = .03) compared with those who did not require conversion to THA.
Conclusion:
Treatment of femoral head osteochondral lesions with OCA via SHD was associated with significant postoperative improvements in PROMs, with a 25% rate of conversion to hip arthroplasty, at a mean follow-up of 4 years. Increased OCA graft depth was associated with conversion to THA. OCA transplantation provides a versatile treatment option for isolated femoral head osteochondral lesions in young patients.
Keywords
Isolated, symptomatic chondral lesions of the femoral head in young, active patients are difficult pathologies to treat. These lesions may cause chronic pain, stiffness, and mechanical symptoms, with an increased risk of progression to early osteoarthritis (OA), which may be correlated with increasing lesion size. 19 Current treatment options for diffuse, advanced cartilage loss include total hip arthroplasty (THA) and hip resurfacing. However, concerns regarding implant longevity, activity restrictions, and eventual need for revision arthroplasty limit their use in young, active patients, especially those presenting with unipolar, symptomatic femoral head chondral lesions.14,38 Proximal femoral or periacetabular osteotomies have been described as possible strategies for unloading the symptomatic area. However, these procedures do not directly address the cartilage lesion and are associated with complications—including infection, non-union, femoral head ischemia, muscle or nerve injury, and the need for reoperation.2,6,15,45
Numerous surgical techniques have been developed and successfully implemented for treating osteochondral lesions in other joints—including microfracture, osteochondral allograft (OCA) or autograft transfer, and autologous chondrocyte implantation. 18 The use of OCA has been associated with good clinical and patient-reported outcomes in the knee,23,24,40,47 elbow,25,46 ankle,8,16 and glenohumeral joints.22,41 Similar procedures—including autologous osteochondral transfer (or mosaicplasty) and microfracture—have been described in the hip for treatment of avascular necrosis (AVN), 10 developmental hip dysplasia, 20 and traumatic osteochondral femoral head lesions.4,5 When performed arthroscopically, these procedures may be associated with good outcomes.17,28,37 An open approach may provide an advantage over arthroscopic procedures by allowing access to areas of the femoral head not easily accessed via arthroscopy and allowing for concomitant open surgical procedures (periacetabular osteotomy [PAO], femoral osteotomy, etc). Compared with the knee, shoulder, or ankle, open surgical approaches to the hip joint in young patients are more technically challenging, requiring meticulous dissection and preservation of the critical vascular supply to the femoral head. The surgical hip dislocation (SHD), in its current technique utilizing a trochanteric flip osteotomy, was first described by Ganz in 2001. 11 This procedure offers full access to the hip and allows the surgeon to both address cartilage lesions and other concomitant intra-articular pathology—including cam-type femoroacetabular impingement (FAI) or pincer lesions, labral tears, loose bodies, et cetera. However, this procedure requires disruption of the ligamentum teres. It may result in microtrauma to the labrum or compromise of the vascular supply, with the potential for AVN or microinstability, although further research is required. At the authors’ institution, SHD coupled with a femoral head OCA transplantation has been used as a strategy to address focal defects of the femoral head. There is a paucity of literature on outcomes after femoral head OCA via SHD for the treatment of isolated chondral lesions of the femoral head.
Therefore, this study aimed to evaluate clinical outcomes and patient-reported outcome measures (PROMs) after femoral head OCA via SHD. The authors hypothesized that femoral head OCA via SHD would be associated with a low rate of conversion to THA and would result in significantly improved postoperative PROMs.
Methods
This study was a retrospective review conducted at a tertiary care center, with approval from the institutional steering committee. Institutional review board approval was obtained before the initiation of the study (No. 2014-044). Patient data were drawn from a prospective, longitudinally maintained, single-center hip preservation registry.
All patients who underwent femoral head OCA via SHD at our institution between August 2010 and June 2023 were reviewed. All patients underwent SHD as initially described by Ganz et al,11,31,44 and femoral head OCA was performed in the standard fashion, with grafts sourced from JRF Ortho (Figures 1 and 2). Concomitant procedures performed at the time of femoral head OCA via SHD are listed in Table 2. The OCA graft diameter and depth were recorded from intraoperative measurements under direct visualization at the time of surgery. Graft dimensions were determined by surgeon preference based on preoperative magnetic resonance imaging (MRI) measurements and the intraoperative appearance of the lesion. Surgical indications for femoral head OCA via SHD included MRI demonstrating unipolar, focal, full-thickness chondral lesions of the femoral head with preserved cartilage of the remaining hip joint, clinical examination consistent with intra-articular pathology, and at least 6 months of nonoperative management (ie, intra-articular injection, anti-inflammatory medications, physical therapy, activity modification, etc). Patients who met these indications were eligible for study inclusion if they had a minimum 2-year follow-up or if they underwent conversion to THA before 2 years. Patients who demonstrated bipolar chondral lesions, multifocal chondral lesions, AVN, or isolated acetabular chondral lesions, or those who had <2-year clinical follow-up (without conversion to THA before 2 years) were excluded. Previous surgery (including hip arthroscopy) of the ipsilateral hip or concomitant procedures (including labral repair, osteoplasty, or PAO for concurrent pathology) at the time of surgery were not reasons for exclusion.

(A-C) Case example of a 20-year-old man with a history of Perthes disease with a femoral head osteochondral lesion measuring 25 × 27 mm on preoperative radiographs and MRI. (D) Intraoperative photograph demonstrating the area of full-thickness cartilage loss over the superolateral aspect of the femoral head (yellow arrow). (E-F) Intraoperative photographs demonstrating harvest and implantation of the femoral head OCA allograft, measuring 27.5 mm in diameter. An open femoral head osteoplasty and labral debridement were also performed in this case. OCA, osteochondral allograft; MRI, magnetic resonance imaging.

(A-B) Postoperative pelvis radiographs demonstrating healed periacetabular osteotomy and concomitant femoral head OCA transplantation (A) at a 6-month interval and (B) at a 2-year interval after hardware removal. (C-D) Coronal and sagittal postoperative MRI demonstrating healed OCA with preservation of overlying cartilage and articular contour. OCA, osteochondral allograft; MRI, magnetic resonance imaging.
Demographic, radiographic, and perioperative surgical data were prospectively collected via the institutional registry. Elements included age, sex, body mass index (BMI), primary diagnosis, history of previous surgery, and concomitant procedures. Complication data and the need for subsequent surgery were collected via prospective registry follow-up and review of the institutional electronic medical record. The standard of care included postoperative radiographs obtained at 6 months and 1 year postoperatively.
Patient Reported Outcome Measures
PROMs specific to the evaluation of hip pathology included the modified Harris Hip Score (mHHS) and the International Hip Outcome Tool-12 (iHOT-12). For both PROMs, higher scores on a scale of 0 to 100 indicated improved pain and functional scores. These hip-specific PROMs are administered electronically preoperatively and at regular postoperative intervals, as per registry protocol, including at 6 months, 1 year, and annually thereafter. For patients who required conversion to THA, the most recent PROM values obtained before their THA procedure were used for analysis.
Defining Minimal Clinically Important Difference and Patient Acceptable Symptom State Cutoffs
To our knowledge, minimal clinically important difference (MCID) and patient acceptable symptom state (PASS) have not been defined explicitly for patients undergoing femoral head OCA via SHD. However, MCID and PASS values previously established for hip arthroscopy for FAI have been previously applied to patients undergoing SHD. 44 In the setting of hip arthroscopy for FAI at a 2-year follow-up, the MCID for the mHHS and the iHOT-12 are reported as 9.2 and 13.9, respectively.26,32-34,39 PASS scores after hip arthroscopy for FAI at a 2-year follow-up for the mHHS and the iHOT-12 are reported as 83.3 and 72.2, respectively.23-26,29 These previously reported values were used as the MCID and PASS cutoffs for the mHHS and the iHOT-12 in this study.
Statistical Analysis
Descriptive statistics using means and standard deviations were reported for continuous variables. Frequencies and percentages were reported for categorical variables, and the proportion of patients achieving the MCID and the PASS. Age, preoperative iHOT scores, and graft diameter were normally distributed, as indicated by the results of the Shapiro-Wilk test. Independent samples t tests were used to compare age and graft diameter. Pre- and postoperative mHHS scores, postoperative iHOT scores, BMI, and graft depth were not normally distributed, as indicated by the results of the Shapiro-Wilk test. Wilcoxon Signed-Rank tests were used to compare means for pre- and postoperative mHHS and iHOT scores, and Mann-Whitney U tests were used to compare means for BMI and graft depth. The chi-square test was used to evaluate the effect of a history of previous hip surgery on the likelihood of conversion to THA. Statistical significance was defined as P < .05 for all variables, and statistical analyses were conducted using SPSS Statistics for Windows, Version 29.0.0 (IBM Corp).
Results
A total of 24 patients underwent femoral head OCA via SHD for isolated, unipolar osteochondral defects (Table 1). The mean age was 21.4 ± 6 years (range, 13-36.8 years), and the mean BMI was 23.3 ± 4.2 kg/m2. Thirteen patients (54.1%) were women in this study.
Patient Characteristics of Femoral Head OCA via SHD a

Data are presented as mean ± SD (continuous data), n (%) (categorical data), and mean (range). BMI, body mass index; OCA, osteochondral allograft; ORIF, open reduction internal fixation; THA, total hip arthroplasty; SHD, surgical hip dislocation.
One patient underwent THA at 9 months postoperatively.
Nine patients (37.5%) had previously undergone surgical intervention on the ipsilateral hip, at a mean of 6.4 ± 5.4 years (range, 1.2-16.7 years) before undergoing femoral head OCA via SHD. Previous surgical procedures included hip arthroscopy with or without labral repair (n = 4; 16.7%), open reduction and internal fixation of femoral neck or acetabular fractures (n = 2, 8.3%), hip arthroscopy with labral reconstruction (n = 1; 4.2%), intertrochanteric osteotomy (n = 1; 4.2%), hip shelf arthroplasty, and open reduction with Pemberton osteotomy (n = 1; 4.2%).
Preoperative diagnoses included FAI (n = 8; 33.3%), developmental dysplasia (n = 7; 29.2%), posttraumatic (n = 4; 16.7%), Legg-Calvé-Perthes disease (n = 2; 8.3%), focal AVN (n = 2; 8.3%), and chondroblastoma (n = 1; 4.2%). The mean lesion size was 488 mm2 (range, 201-962 mm2), and the mean OCA graft depth was 8.8 mm (range, 6-16 mm). A total of 23 (95.8%) of 24 patients underwent at least 1 concomitant procedure performed at the time of femoral head OCA via SHD (Table 2).
Concomitant Procedures Performed at the Time of Femoral Head OCA via SHD a

Concomitant procedures are not mutually exclusive. OCA, osteochondral allograft; SHD, surgical hip dislocation.
At a mean follow-up of 47.9 months (range, 24-126 months), 19 of 24 patients (79.2%) had pre- and postoperative PROMs. Mean mHHS scores significantly increased from 62.1 preoperatively to 83.9 postoperatively (P < .001) (Table 3). Similarly, mean iHOT-12 scores significantly increased from 35.5 preoperatively to 77.5 postoperatively (P < .001). The MCID was achieved by 67% of patients for the mHHS and by 76% of patients for the iHOT-12, and the PASS was achieved by 62% for the mHHS and by 67% of patients for the iHOT-12 (Table 4).
Pre- and Postop mHHS and iHOT-12 Scores a
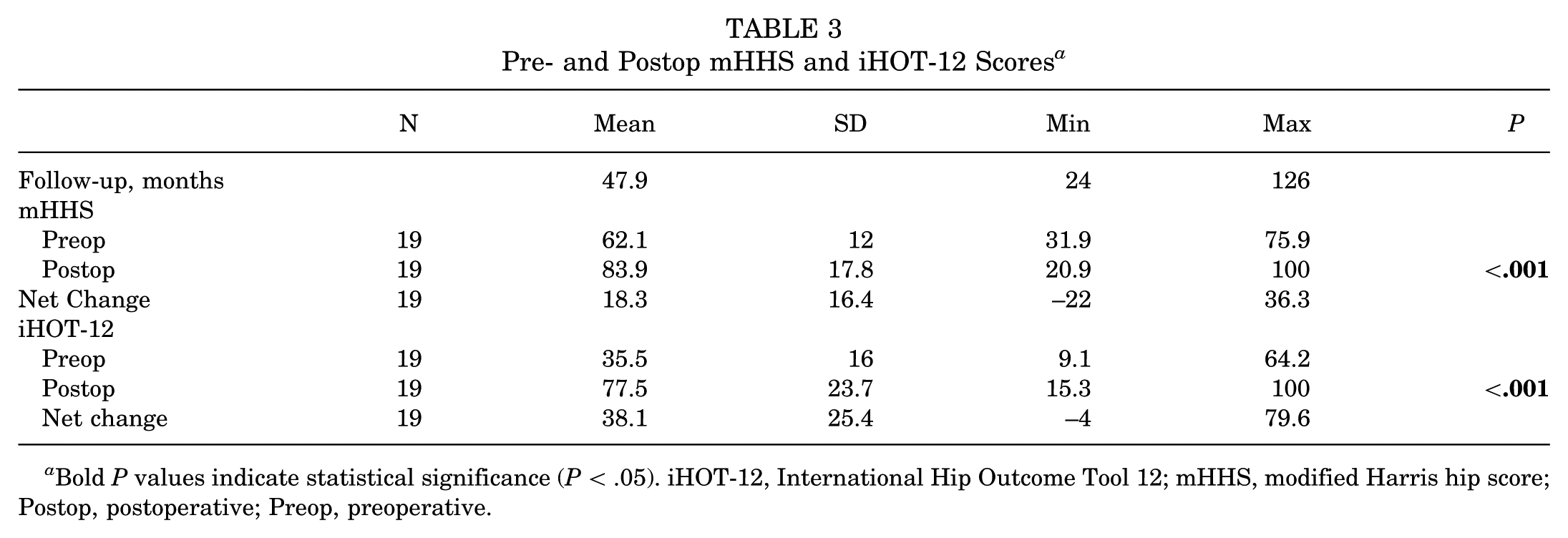
Bold P values indicate statistical significance (P < .05). iHOT-12, International Hip Outcome Tool 12; mHHS, modified Harris hip score; Postop, postoperative; Preop, preoperative.
Percentage of Patients Who Achieved MCID and PASS for Hip Outcome Scores at the Most Recent Follow-up a

iHOT-12, International Hip Outcome Tool 12; MCID, minimal clinically important difference; mHHS, modified Harris hip score; PASS, patient acceptable symptom state.
Seven patients required subsequent ipsilateral hip operations (29.2%). Two patients required hip arthroscopy, with 1 patient ultimately undergoing conversion to THA (Table 5). In total, 6 patients (25%) required conversion to hip arthroplasty (5 THAs and 1 hip resurfacing) at a mean of 3.8 years after femoral head OCA via SHD (Table 6). Patients who required conversion to THA demonstrated significantly larger OCA graft depth (10.7 mm vs 8.1 mm; P = .03) compared with patients who did not require conversion to THA (Table 7). There was no significant association between graft diameter (P = .16), sex (P = .48), age at index surgery (P = .89), BMI (P = .58), previous ipsilateral hip surgery (P = .81), or number of femoral head OCA plugs utilized (P = .78) and risk of requiring conversion to THA.
Subsequent Procedures Performed After Femoral Head OCA via SHD a
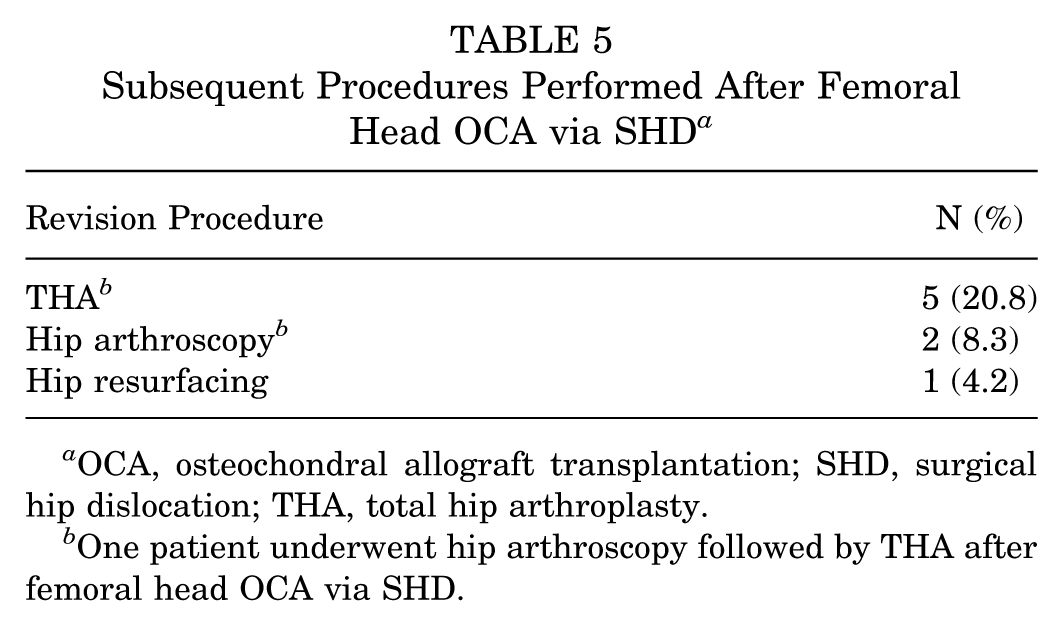
OCA, osteochondral allograft transplantation; SHD, surgical hip dislocation; THA, total hip arthroplasty.
One patient underwent hip arthroscopy followed by THA after femoral head OCA via SHD.
Patient Characteristics of those Who Required Conversion to THA a

AVN, avascular necrosis; BMI, body mass index; FAI, femoroacetabular impingement; OA, osteoarthritis; THA, total hip arthroplasty.
Comparison of Demographic and Perioperative Data Between Patients Who Required Conversion to THA vs Patients Who Did Not Require Conversion to THA After Femoral Head OCA via SHD a

indicates statistical significance (P < .05). BMI, body mass index; OCA, osteochondral allograft; SHD, surgical hip dislocation; THA, total hip arthroplasty.
Patients Requiring Conversion to Hip Arthroplasty
Five of the 6 patients (83.3%) who ultimately required THA demonstrated at least 1 year of symptom-free daily living. One patient (preoperative diagnosis: AVN status after prior femoral head stress fracture) initially did well for 2.5 years, returning to full activity as a gymnast. Ultimately, their pain recurred, requiring THA for worsening OA at 2.9 years after femoral head OCA. The second patient (preoperative diagnosis: FAI with osteochondral lesions) also recovered well after femoral head OCA and returned to all activities except running before suffering a second injury, resulting in a recurrent labral tear. This patient subsequently underwent hip arthroscopy for chondroplasty and debridement of the recurrent labral tear, and ultimately required THA for the development of OA at 3.7 years after femoral head OCA. The third patient (preoperative diagnosis: FAI with osteochondral lesions) did well for nearly 2 years after femoral head OCA, ultimately requiring conversion to THA for the development of OA at 2.9 years after femoral head OCA. The fourth patient (preoperative diagnosis: FAI with osteochondral lesion) did well for over 7 years after femoral head OCA, ultimately requiring conversion to THA for development of OA at 10.3 years after femoral head OCA. The fifth patient did well for nearly 2 years after femoral head OCA, but required conversion to THA for the development of OA at 2.3 years after femoral head OCA. Unfortunately, the last patient (preoperative diagnosis: AVN status after prior femoral neck open reduction internal fixation [ORIF] for fracture) did not significantly improve after femoral head OCA. Of note, this patient had significant focal collapse of his femoral head status after prior femoral neck ORIF, requiring the use of 3 OCA plugs at the time of attempted femoral head OCA versus SHD. At 6 months postoperatively, repeat hip MRI demonstrated minimal healing and a lack of graft integration, and the patient underwent conversion to hip resurfacing 9 months after femoral head OCA.
Discussion
The present study demonstrates that femoral head OCA performed via SHD is associated with significant improvements in PROMs postoperatively, with mean mHHS scores significantly increased from 62.1 preoperatively to 84.9 postoperatively and mean iHOT-12 scores significantly increased from 35.5 preoperatively to 78.3 postoperatively. The MCID was achieved by 67% of patients for the mHHS and 76% of patients for the iHOT-12, and the PASS was achieved by 62% for the mHHS and 67% for the iHOT-12. There was a rate of conversion to THA (25%), consistent with previous studies. Additionally, this study identified increased graft depth as a risk factor for conversion to THA after femoral head OCA via SHD.
In our cohort, the conversion rate to THA after OCA transplantation via SHD was 25% at a mean follow-up of 48 months, with a mean time to conversion to THA of 3.8 years. The rate of conversion to THA after femoral/acetabular OCA transplantation is variable in the literature, with reported rates ranging from 13.6% to 55% in previous studies. 9 Mei et al 29 examined 22 patients undergoing OCA via SHD for femoral head osteochondral lesions. They demonstrated that conversion to THA was 13.6% at 2 years and 21.5% at 5 years, with an overall conversion rate of 22.7% during the study period. Oladeji et al 35 reported a 30% conversion rate to THA in 10 patients undergoing OCA of the femoral head and/or acetabulum, with a mean follow-up of 1.4 years. Finally, Passaplan et al 36 found a conversion rate of 54.5% in 11 patients with OCA of the femoral head. Thus, the rate of conversion to THA found in the present study appears to be consistent with rates reported in the existing literature. Additionally, 29.2% of patients (8 surgeries in 7 patients) required reoperation in this cohort, with 1 patient requiring a subsequent hip arthroscopy followed by conversion to THA. This rate of subsequent surgery is similar to previously reported reoperation rates after femoral head OCA, with previous studies citing a reoperation rate of ~30% at a short-term follow-up, 35 and up to 63% at a long-term follow-up. 36 While there is variability in the survivorship of the native hip after femoral head OCA, 9 our results suggest that outcomes after femoral head OCA via SHD remain encouraging.
With respect to PROMs after femoral head OCA via SHD, our study demonstrated statistically significant improvements in pre-to postoperative mHHS and iHOT-12 scores. This finding is consistent with previous literature, which has shown significant improvements in mHHS and pain scores postoperatively after femoral head OCA via SHD in multiple studies.7,21 As mentioned previously, there are no established MCID or PASS thresholds for PROMs after femoral head OCA via SHD. 44 To rigorously evaluate the outcomes of the patients included in the present study, the authors utilized the thresholds used for hip arthroscopy to assess the percentage of patients achieving the MCID and the PASS for the iHOT-12 and the mHHS postoperatively. In our cohort, 67% of patients achieved the MCID thresholds for the mHHS, 76% for the iHOT-12, and 62% of patients achieved the PASS thresholds for the mHSS and 67% for the iHOT-12. These results are consistent with a recent study by Trotzky et al, 44 who reported clinical and radiographic outcomes in 117 patients (70 primary and 44 revision cases) who underwent SHD. 44 The authors reported that 87% and 66% of patients undergoing primary SHD achieved these same MCID and PASS cutoffs for mHHS, respectively. Similarly, 87% and 68% of patients undergoing primary SHD achieved MCID and PASS cutoffs for the iHOT-12, respectively. Thus, procedures performed via SHD for treatment of intra-articular hip pathology are associated with good postoperative patient-reported outcomes, which are significantly improved from preoperative values.
A key finding in this study was that increased OCA graft depth was associated with a higher rate of conversion to THA. Specifically, our results demonstrate that patients who required conversion to THA demonstrated a significantly larger graft depth (10.7 mm vs 8.1 mm) compared with patients who did not require conversion to THA. Although there is no clear consensus on optimal graft dimensions, the results of our study are consistent with the current literature. Ackermann et al 1 evaluated the associations between OCA graft morphology and OCA MRI scoring system measures in 74 femoral condyle OCA cases. The authors demonstrated that an OCA graft depth of >9 mm was associated with worse graft integration scores on MRI. Thus, the higher rates of conversion to THA in patients who required larger graft depths may be related to poor bony graft integration. Specifically, in 3 of 6 (50%) patients who required conversion to THA, a femoral head OCA graft with a depth >9 mm was utilized. Alternatively, none of the remaining 18 patients who avoided conversion to THA had an OCA graft with a depth of >9 mm.
OCA graft allogenicity may also play a role in clinical outcomes after transplantation,3,19,42,43 Previous studies have demonstrated that increased graft depth may limit access to the deep zones of the graft during graft preparation, a critical step in decreasing graft immunogenicity, with some authors suggesting an optimal graft depth of 5 to 8 mm.3,19,30 considering these data, the results of the present study support the recommendations that femoral head OCA graft depths of >9 mm may be associated with worse clinical outcomes. However, larger prospective studies are warranted to further corroborate these findings.
One major complication that can result from SHD includes femoral head AVN. The weightbearing portion of the femoral head is supplied by the medial femoral circumflex artery (MFCA), 12 which may be compromised during dissection during the SHD. Limited data exist on AVN rates after elective SHD for intra-articular hip pathology. Rates of MFCA injury and AVN in patients undergoing SHD for femoral head fractures have been reported as 7.7% to 11.7% in the literature. However, these rates may be higher than elective SHD due to the significant trauma associated with femoral head fractures.13,27 Interestingly, the 2 patients with preoperative diagnosis of focal AVN did ultimately require conversion to THA for worsening AVN and OA after femoral head OCA via SHD. Because of the limited number of patients with a preoperative diagnosis of AVN in this cohort, generalized conclusions regarding outcomes after femoral head OCA in these patients are limited. However, combining the outcomes of this patient with the association between increasing graft depth and the need for conversion to THA, the authors recommend caution when attempting OCA transplantation for focal, deep, collapsed femoral head lesions associated with AVN. Ultimately, larger prospective, long-term studies are warranted to evaluate rates of AVN after elective SHD procedures and outcomes after femoral head OCA performed for AVN.
Limitations
This study has several limitations. First, there are limitations inherent to retrospective cohort studies, and causal relationships cannot be established. Additionally, the absence of a comparison group or matched cohort limits the conclusions that can be drawn from this study in a comparative sense. However, the included PROMs were collected prospectively, and objective perioperative measurements (graft diameter, depth, etc) were performed at the time of the study, which may help mitigate the effect of the retrospective design. Second, selection bias is likely to exist for patients undergoing femoral head OCA via SHD compared with other surgical procedures (ie, hip resurfacing, THA, or hip arthroscopy). Third, given the rarity with which femoral head OCA via SHD is performed, our sample size was inherently limited. Despite the small sample size, statistically significant postoperative improvements in PROMs were demonstrated. There was a limited number of patients who ultimately required conversion to THA after femoral head OCA via SHD, which does limit the conclusions that can be made regarding these patients. However, this study did identify graft depth as a possible risk factor for subsequent conversion to THA after femoral head OCA via SHD. Finally, there was significant heterogeneity in preoperative diagnoses for the included patients, although the authors believe this demonstrates the versatility of the procedure and is representative of clinical practice. Future prospective studies are warranted to further evaluate long-term clinical, radiographic, and functional outcomes of femoral head OCA via SHD.
Conclusion
Treatment of femoral head osteochondral lesions with OCA via SHD was associated with significant postoperative improvements in PROMs, with a 25% rate of conversion to hip arthroplasty, at a mean follow-up of 4 years. Increased OCA graft depth was associated with conversion to THA. OCA transplantation provides a versatile treatment option for isolated femoral head osteochondral lesions in young patients.
Footnotes
Final revision submitted July 21, 2025; accepted August 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.M.S. is a paid consultant for Stryker and is an associate editor for The American Journal of Sports Medicine. R.J.W. is a paid consultant for Bauerfind and holds stock options in BICMD, Cymedica, Overture Orthopedics, Gramercy Extremity Orthopedics, Agelity, Pristine Surgical, and Brain Box Inc. A.S.R. is a paid consultant for Anika, BodyCad, NewClip, Ranfac/Marrow Cellution, Overture, Cervos, CONMED Linvatec, Moximed, and Smith & Nephew; and holds stock options in Enhatch and Overture. B.T.K. receives royalties from Arthex; holds stock options in MMI and ZEO ScientifiX; has ownership interest in Parvizi Surgical and Vincera Institute; and is on the advisory board for ZEO ScientifiX. A.H.G. is a paid consultant for Bioventus, JRF, Vericel, Smith & Nephew, Organogenesis, and Moximed.
AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital for Special Surgery (#2014-044).