
Abstract
Background:
Hip arthroscopy is one of the fastest-growing orthopaedic procedures. Minimizing operative time and room idle time may improve patient outcomes and reduce procedural costs.
Purpose:
To identify patient, surgeon, and procedural variables that are associated with operative and idle time that may result in improved patient outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients undergoing hip arthroscopy for femoroacetabular impingement from 2014 to 2022 were retrospectively reviewed from a multi-institutional health system. Multivariate linear regression was employed using patient age, sex, body mass index, American Society of Anesthesiologists (ASA) classification, annual surgeon hip arthroscopy procedural volume (APV), capsular closure, use of a post, femoroplasty, acetabuloplasty, and labral debridement versus repair. Multivariable logistic regression determined whether operative time or idle time was associated with emergency department visits, readmissions, or returns to the operating room (RTORs) within 1 year.
Results:
A total of 740 hip arthroscopies (704 patients) performed by 25 surgeons were included. Male sex (B = 12.1 minutes; 95% CI, 6.1 to 18.0; P < .001), capsular closure (B = 20.1 minutes; 95% CI, 14.1 to 26.0; P < .001), and femoroplasty (B = 11.5 minutes; 95% CI, 4.7 to 18.3; P < .001) were associated with increased operative time. Age (B = −0.5 minutes; 95% CI, −0.7 to −0.3; P < .001), ASA classification (B = −5.4 minutes; 95% CI, −10.7 to −0.2; P = .04), and APV >25 (B = −33.3 minutes; 95% CI, −39.4 to −27.1; P < .001) were associated with decreased operative time. Use of a post (B = 5.0 minutes; 95% CI, 1.4 to 8.7; P = .007) was associated with increased idle time. APV >25 (B = −15.8 minutes; 95% CI, −18.7 to −12.8; P < .001) and labral repair over debridement (B = −5.9 minutes; 95% CI, −9.7 to −2.2; P = .002) were associated with decreased idle time. Every additional minute of idle time was associated with increased odds of unplanned RTOR for ipsilateral hip pathology within 1 year by 2.3% (95% CI, 1.0%-3.6%; P = .001).
Conclusion:
Our study demonstrated that shorter operative times were associated with several patient-specific factors, including older age and higher ASA classification. Surgeons who performed ≤25 hip arthroscopies per year were associated with longer idle times, and longer idle times were associated with a greater risk of reoperation for ipsilateral hip pathology within 1 year.
Hip arthroscopy has been recognized as one of the fastest growing orthopaedic procedures in the United States.5,25,39,43 Its substantial increase in utilization has been guided by improved diagnostic capabilities and technical advancements over recent decades.8,9,11,13,18,30 However, as hip arthroscopy becomes popularized by an increasing number of surgeons in broader patient populations and patient care settings, factors associated with its safe and cost-effective performance must be continually studied.2,35,47,48
Several time-dependent adverse outcomes including increased surgical-site infection risk, prolonged hospital stays, thromboembolic complications, and returns to the operating room (RTORs) have been demonstrated with longer procedural durations among various surgical procedures.3,10,15,28,42,46 Despite their relative safety, a direct relationship between surgical time and complications also exists for arthroscopic procedures including higher rates of deep vein thrombosis, pulmonary embolism, and infection.3,15,28,46 Rates of perioperative complication after arthroscopic procedures of the hip have largely been described in terms of annual surgeon procedural volume (APV) and procedural duration, with higher surgeon volume being among many factors that lower rates of reoperation. 17
Regarding cost utilization, longer duration of care has been identified as a major driver of both total procedural charges for hip arthroscopy and broadly associated with increasing health care expenditures for many orthopaedic procedures.4,6,21,34,36,44,45 Bokshan et al 4 performed a multivariate linear regression and univariate analysis of cost predictors in 14,713 anterior cruciate ligament reconstruction procedures, finding operative time to be a significant cost generator amounting to $108 for each minute of time in the operating room (OR). In the setting of hip arthroscopy, a recent cost prediction analysis identified operative times >98 minutes as one of the strongest measures for increased total charges. 36 With the emergence of value-based care models, identifying the predictors of prolonged operative and room time are important to help mitigate patient complications and procedure-related costs.
Literature is limited regarding factors implicated in prolonging surgical time or total OR time during hip arthroscopy. With previous literature linking prolonged operative times to increased rates of postoperative complication, and increased OR time to increased procedure-related costs, additional research is warranted to establish risk factors for both. Therefore, the purpose of this study was to identify surgeon-related, patient-specific, and procedure-related factors that predict operative time and OR idle time. We hypothesized that operative time would decrease with greater surgeon volume and would be prolonged by performing a capsular repair. Additionally, we predicted that idle room time would be influenced by traction setup and patient body mass index (BMI).
Methods
After institutional review board approval was obtained, electronic medical records were obtained for all arthroscopic hip procedures performed within a large, multihospital academic health system between January 1, 2014, and June 15, 2022. Procedures were identified using the Current Procedural Terminology (CPT) identifiers for arthroscopic hip procedures, including 29860, 29861, 29862, 29863, 29916, 29915, and 29914. Inclusion criteria comprised any patient who underwent hip arthroscopy at one of the 11 facilities evaluated within our health system during the aforementioned time frame. A total of 950 hip arthroscopies were initially identified; however, 210 procedures (22.1%) were excluded. Procedures were excluded if they were converted to an open procedure (n = 27), revision procedures (n = 45), had incorrect or insufficient medical coding and/or operative reports (n = 20), or were performed for pathology unrelated to femoroacetabular impingement (FAI) (n = 118). Incorrect medical coding was determined when operations outside of hip arthroscopy were identified via CPT coding. Operative reports were deemed insufficient if they lacked critical information pertaining to the study—namely, operative time and total room time.
The remaining 740 arthroscopic hip procedures in 704 patients (36 staged bilaterals) were included in the analysis. Independent variables comprised various patient-, surgery-, and surgeon-specific factors that were independently documented by 2 reviewers (L.E.B. and B.J.K.). Patient information including age, sex, BMI, American Society of Anesthesiologists (ASA) class, race, and various medical comorbidities were also obtained. Procedure-related factors were recorded from operative reports and perioperative medical documentation including surgical indication, traction setup (post versus postless), labral treatment (repair or debridement), capsular management (capsular repair or not), femoroplasty (performed or not), and acetabuloplasty (performed or not). In addition, the APV was recorded for each surgeon and was defined as the total number of cases performed divided by the total number of years active during the study period. The year 2022 was excluded for this calculation as it was a partially recorded year. Surgeons were stratified into 2 volume-based groups. High-volume surgeons were defined as performing >25 hip arthroscopies per year while low-volume surgeons performed ≤25 than these procedures annually.
Dependent variables consisted of operative time and idle time, as well as unplanned return to the emergency department (ED), readmission, and RTORs all within 1 year. Operative time was defined as the length of time (in minutes) between skin incision and skin closure. Idle time was calculated as the difference between the total room time and operative time.
Statistical analysis was performed with SPSS 28 (IBM Corp). Continuous data are presented as mean ± SD. Multivariate linear regression was utilized to identify predictors of operative time and idle time. Multivariate logistic regression was employed to assess whether operative time or idle time predicted return to the ED, readmission, or RTOR within 1 year. Analyses were performed with the data pooled and partitioned by APV. A P value <.05 with a 95% CI that did not include 0 were used to determine statistical significance.
Results
Of the 740 arthroscopic hip procedures performed in 704 patients, 440 (59.5%) of the procedures were in female patients and the mean age was 36.9 ± 13.8 years (Table 1); 58 hips (7.8%) were <18 years old. A postless traction setup was implemented in 84.2% of cases. Femoroplasty and acetabuloplasty were performed in 61.9% and 62.2% of cases, respectively. Approximately 46.3% of patients underwent both acetabuloplasty and femoroplasty. A total of 96.1% underwent labral treatment procedures—either repair (82.0%) or debridement (18.0%). There were no labral reconstructions in this cohort of primary hip arthroscopy patients. The mean APV was 6.5 ± 11.0 hip arthroscopies for all included surgeons (n = 25). Two surgeons were considered high volume (mean APV, 31.8) and collectively performed 51.6% of the cases. The mean operative time was 95.0 ± 46.5 minutes while the mean idle room time was 58.7 ± 19.3 minutes. Within 1 year of surgery, 10.9% of patients had an ED visit while 6.5% and 4.6% were readmitted and returned to the OR, respectively.
Independent and Dependent Variables (n = 740 hips) a
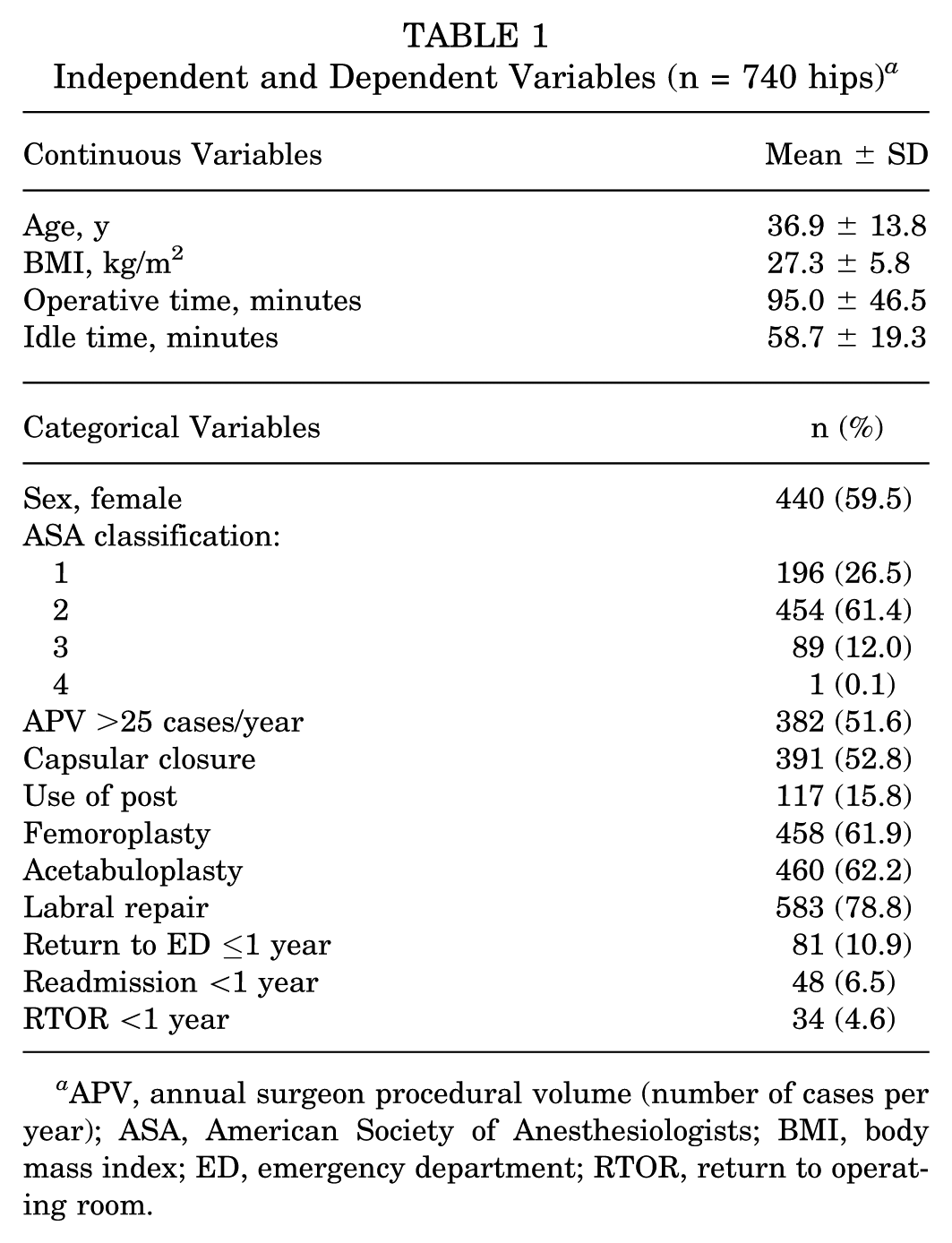
APV, annual surgeon procedural volume (number of cases per year); ASA, American Society of Anesthesiologists; BMI, body mass index; ED, emergency department; RTOR, return to operating room.
Multivariate linear regression revealed that male sex (B = 12.1 minutes; 95% CI, 6.1 to 18.0; P < .001), capsular closure (B = 20.1 minutes; 95% CI, 14.1 to 26.0; P < .001), and femoroplasty (B = 11.5 minutes; 95% CI, 4.7 to 18.3; P < .001) increased operative time. In contrast, age (B = −0.5 minutes; 95% CI, −0.7 to −0.3; P < .001), ASA classification (B = −5.4 minutes; 95% CI, −10.7 to −0.2; P = .04), and APV >25 (B = −33.3 minutes; 95% CI, −39.4 to −27.1; P < .001) decreased operative time. BMI, use of a post, acetabuloplasty, and choice of labral management did not affect operative time. Use of a post (B = 5.0 minutes; 95% CI, 1.4 to 8.7; P = .007) increased idle time while APV >25 (B = −15.8 minutes; 95% CI, −18.7 to −12.8; P < .001) and labral repair rather than debridement (B = −5.9 minutes; 95% CI, −9.7 to −2.2; P = .002) decreased idle time. The remaining independent variables did not influence idle time. When the corresponding linear regressions were performed separately based on APV, the low-volume surgeon cohort demonstrated that capsular closure (B = 28.1 minutes; 95% CI, 17.2 to 39.0; P < .001) increased operative time, age (B = −0.8 minutes; 95% CI, −1.2 to −0.3; P = .001) decreased operative time, and use of a post (B = 8.1 minutes; 95% CI, 2.2 to 14.0; P = .008) increased idle time. The high-volume surgeon cohort yielded the same findings for age (B = −0.3 minutes; 95% CI, −0.5 to −0.04; P = .02) and capsular closure (B = 8.8 minutes; 95% CI, 3.2 to 14.4; P = .002), but also showed that male sex (B = 13.5 minutes; 95% CI, 7.7 to 19.3; P < .001), femoroplasty (B = 19.6 minutes; 95% CI, 13.9 to 25.4; P < .001), and acetabuloplasty (B = 6.8 minutes; 95% CI, 1.8 to 11.9; P = .008) increased operative time.
Multivariable logistic regression demonstrated that idle time did not influence return to the ED or readmission rate, but did increase the risk for RTOR in the first postoperative year (B = 1.7%; 95% CI, 0.6-2.8; P = .003). Half of the 34 cases with RTOR <1 year were directly attributed to ipsilateral hip pathology. A breakdown of specific etiologies is listed in Table 2. When only these ipsilateral hip cases were utilized in the regression model, idle time persisted to increase the risk (B = 2.3%; 95% CI, 1.0-3.6; P = .001) of RTOR <1 year. When these data were further subdivided by APV, this relationship between idle time and RTOR <1 only persisted in the low-volume surgeon cohort (B = 2.5%; 95% CI, 0.9-4.0; P = .001). Operative time did not influence return to the ED, readmission, or RTOR within 1 year.
Ipsilateral Hip Etiologies for RTOR <1 Year (n = 17 cases) a

RTOR, return to operating room; THA, total hip arthroplasty.
Revision hip arthroscopy consisted of ≥1 of the following procedures: lysis of adhesions, revision labral repair, revision femoroplasty, or revision acetabuloplasty.
Discussion
The principal findings of this study are that male sex, capsular closure, and femoroplasty were associated with increased operative time. In contrast, age, ASA classification, and APV >25 were associated with decreased operative time. Use of a post was associated with increased idle time. APV >25 and labral repair over debridement were associated with decreased idle time. Every additional minute of idle time was associated with increased odds of unplanned RTOR for ipsilateral hip pathology within 1 year; however, this relationship only persisted in the low-volume surgeon group.
Surgeon Volume
Hip arthroscopy has been well studied in the context of surgeon proficiency.6,19,22,24,29,40 In the present investigation, the mean operative time—95.0 minutes—is comparable with values reported in previous literature. 19 Significant reductions in operative time have been observed after a surgeon's first 20 to 30 cases in several series.22,24,33 However, most volume-based thresholds are arbitrarily chosen and range widely. 24 For example, one volume-based outcome study 40 identified that significantly reduced rates of revision arthroscopy or conversion to total hip arthroplasty (THA) occur after a surgeon's first 519 cases. Out of the surgeons in the present study, those performing >25 hip arthroscopies annually were the only volume-based cohort significantly associated with a decrease in operative time. This is consistent with previous studies that note the inverse relationship between surgeon volume and procedural duration.6,17,19,29,40 However, the range of competency marks and methodologies used to define surgeon experience offers little consensus in defining the relationship between surgeon proficiency, measures of operative time, and patient safety.
Measures of idle time are less frequently reported in the literature and can be obscurely described. Of studies with defined measures, Dumont et al 19 reported a mean “setup” and “wake-up” time of 39.8 minutes across a series of 225 consecutive patients. Furthermore, the authors observed that these times remained relatively consistent regardless of surgeon experience. This finding contrasts the present study—surgeons who performed >25 hip arthroscopies annually were associated with approximately 16 fewer minutes of idle time than surgeons with a smaller surgical volume. This may reflect surgeon and OR staff familiarity, as a greater number of cases allows both parties to be more efficient with the required materials and setup.
Procedure-Related Factors
Postless traction systems have gained significant popularity among hip arthroscopists largely because of their potential superior safety profile compared with conventional techniques.16,32,41 In the present study, postless traction was more popular and was associated with decreased idle time by 5 minutes. Five minutes may not appear to be a substantial amount of time; however, time-related factors heavily influence ambulatory and hospital OR budgets, and the higher initial costs associated with proprietary postless traction systems may be justified by long-term savings.4,34,36 Additionally, some authors have described cost-effective means of achieving postless traction using standard hip distraction tables.16,31
Capsular closure was performed in just over half of cases and was associated with approximately 20 minutes of operative time. Although a growing amount of literature has advocated for capsular repair in the management of FAI, it was performed more sparingly than labral repair, acetabuloplasty, or femoroplasty in the present cohort.1,11,18,20,23 Considering that labral repair and acetabuloplasty were not associated with operative time in the pooled data, the prolonging effect of capsular repair may be related to surgeon inexperience and perhaps a steeper learning curve for this component of the procedure. The subanalyses by APV support this possibility, as capsular repair was associated with increased operative time by an additional 20 minutes in the low-volume cohort compared with their high-volume counterparts. In contrast, for femoroplasty, the high-volume cohort had an increase in procedural duration of 19.6 minutes, compared with only 11.5 minutes for the cohort as a whole. An adequate femoroplasty requires time and meticulous surgical technique. Inexperienced surgeons may not resect sufficient femoral neck to fully remove a cam lesion and thus may perform this portion of the procedure in a shorter amount of time. Alternatively, ease of femoroplasty is directly affected by proper exposure, which may be related to a larger capsulotomy, especially by less experienced surgeons. 23 As a result, this larger capsulotomy may then prompt some surgeons to perform a more extensive and time-consuming capsular closure.
Despite the increased technical demands of labral repair compared with debridement, performing the former was not associated with increased operative time. Instead, labral repair was associated with a decreased idle time by almost 6 minutes. This may be explained by surgeon and OR staff experience. More experienced hip arthroscopists may take on patients with larger labral tears or may be more willing to attempt a repair on a more degenerated labrum. Given that these more seasoned surgeons likely perform a greater number of cases, the OR staff is more familiar and efficient with the specific setup.
Patient Factors
Male sex was associated with increased operative time by approximately 12 minutes while age and ASA classification were both inversely correlated. Every 1-year increase in age or 1-stage increase in ASA classification was associated with an operative time decrease of 0.5 minutes and roughly 5 minutes, respectively. Earlier studies have concluded that older patients are more likely to receive temporizing procedures such as chondroplasty or labral debridement rather than repair. 43 By similar logic, patients with higher ASA classifications are more likely to be older, and surgeons may be more motivated to minimize operative time to limit the risks of prolonged anesthesia. Conversely, BMI was not associated with operative time, which is atypical in the context of other arthroscopic procedures. Previous investigations reported elevated BMI as prolonging operative times for both arthroscopic rotator cuff repair and anterior cruciate ligament reconstruction.3,15 It is possible that the use of longer cameras and instrumentation in hip arthroscopy may mitigate some of the challenges of increased BMI. Additionally, the health system where the present study was performed utilizes radiographic guidance when establishing hip arthroscopy portals. The widespread utilization of fluoroscopy may reduce the unique challenges and additional operative time that come with identifying anatomic landmarks in higher BMI patients.
RTOR
Within 1 year of the index surgery, the RTOR rate was 4.6% for any reason and 2.3% for etiologies involving the ipsilateral hip. Some earlier studies report a 10-fold lower RTOR rate at 0.4% and 0.3%; however, both investigations utilized the National Surgical Quality Improvement Program database, which only provides data up to 30 days postoperatively and does not always list a clear etiology.14,27 This temporal relationship is further illustrated in a systematic review of 92 studies (6134 patients) that yielded an RTOR rate of 6.3% after a mean of 16.4 ( +/−15.1) months. 26 The most common reported reason was conversion to THA, most notably in older patients and those with preexisting hip osteoarthritis. While older age, higher ASA classification, and BMI have also been associated with higher rates of postoperative complications, reoperation, or overnight hospital stay following hip arthroscopy, a paucity of research has examined the relationship between operative or idle times and RTOR.12,17,44 In the present investigation, every additional minute of idle time was associated with increased risk of RTOR by 1.7%. When the etiologies for RTOR were isolated to only those involving the ipsilateral hip, the risk rose to 2.3% per minute. When isolated to low-volume surgeons, the risk grew slightly higher to 2.5% per minute.
Limitations
This study is not without limitations. First, this is a retrospectively performed study that can demonstrate association, but not cause and effect, while also being prone to potential error in data entry including the interpretation of diagnoses and procedural information. Additionally, our patient-surgeon cohort was sampled from a regional health system, which may be less generalizable to different populations (such as those from nonacademic institutions) when compared with national registry studies or those from specialized, high-volume hip arthroscopy centers. In our multivariate model, it should be noted that the surgeon APV threshold of 25 was determined subjectively based on our own data and does not represent statistically validated cutoffs for performance. Future research is warranted to better establish the relationship between a wide variety of surgeon APV cutoffs and operative time. Moreover, the utilization of osteoplasties was reported without radiographic evaluation, which may have more accurately predicted their effect on procedural duration. Additional studies correlating radiographic parameters with operative times could be beneficial. Last, surgeon fellowship training was not reported in this study. While the effect of fellowship training on operative or room time is not documented in hip arthroscopy, it has been shown to affect patient outcomes and technique utilization in other orthopaedic disciplines.7,37,38
Conclusion
Our study demonstrated that shorter operative times were associated with several patient-specific factors, including older age and higher ASA classification. Surgeons who performed ≤25 hip arthroscopies per year were associated with longer idle times, and longer idle times were associated with a greater risk of reoperation for ipsilateral hip pathology within 1 year.
Footnotes
Final revision submitted May 15, 2025; accepted July 1, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Northwell Health (No. LIJVS 22-0698).