
Abstract
Background:
After concussion, metabolic disruption causes a mismatch between the brain’s energy demand and the body’s ability to deliver energy to the brain. Physical activity (ie, energy expenditure) is recommended after concussion to facilitate recovery. Low-energy availability (LEA) is defined as inadequate energy available to support physiologic function after accounting for exercise energy expenditure and may influence concussion symptoms or disrupt/prolong recovery.
Purpose/Hypothesis:
The purpose was (1) to investigate LEA indicators (LEA-I) among female adolescents with and without recent concussion and (2) to examine the relationship between LEA-I and concussion symptom severity. It was hypothesized that (1) participants with concussion would have higher LEA-I than controls and (2) LEA-I and concussion symptom severity would be moderately correlated.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Two groups of female adolescents ages 13 to 18 years completed the Low Energy Availability in Females Questionnaire (LEAF-Q): uninjured controls and adolescents within 21 days of concussion. The LEAF-Q evaluates gastrointestinal symptoms, menstrual function, and injury frequency (range, 0-25). LEA-I was defined as scores ≥8, indicative of high LEA risk. Participants with concussion rated symptoms using the Post-concussion Symptom Inventory (PCSI; range, 0-120), with higher scores indicating more severe symptoms. We used independent samples t tests and calculated effect sizes to examine LEAF-Q between-group differences and linear regression for a multivariable comparison. For the concussion group, the correlation between LEAF-Q and PCSI scores was examined via Pearson r coefficients.
Results:
We enrolled 117 female adolescents: 88 controls (mean ± SD age, 15.9 ± 1.5 years) and 29 with concussion (age, 15.5 ± 1.4 years). Upon univariable analysis, the concussion group reported significantly higher LEAF-Q scores than controls (9.1 ± 4.0 vs 6.0 ± 3.7; P < .001; Cohen d = 0.81). After adjusting for age and body mass index, LEAF-Q scores were 3.23 points higher on average for the concussion group as compared with controls (β = 3.23; 95% CI, 1.49-4.96; P < .001). For the concussion group, there was a small and insignificant correlation between LEAF-Q and PCSI scores (r = −0.06, P = .74).
Conclusion:
Female adolescents after concussion had LEAF-Q scores indicative of high LEA risk, while controls did not. The lack of correlation between LEAF-Q and PCSI scores suggests that LEA-I is not associated with concussion symptoms.
After concussion, defined as a traumatic brain injury caused by forces directly to the head or the body, 40 a set of complex pathophysiologic processes occurs within the brain.7,8 Animal models suggest that the processes that occur at the cellular level, such as neuronal depolarization, disrupted ionic flow, and decreased axonal function, create an increased energy demand to maintain homeostasis, and this process is ultimately responsible for recovery.7,8 Simultaneously, there is an impaired ability to deliver the energy needed to restore homeostasis within the brain owing to impaired cerebral blood flow, creating a mismatch between energy supply and demand.8,11 The cerebral metabolism impairments may contribute to common concussion symptoms, at least in part. 52 However, symptoms are often nonspecific to concussion, which can make it difficult to identify the many possible contributing factors to symptom etiology after concussion. 11 Physiologic dysfunction, including impaired cerebral blood flow, may exist after concussion symptoms resolve. 18 It is therefore possible that energy imbalance may influence concussion recovery as well as postconcussion outcomes beyond the time of symptom resolution, but energy availability is not typically assessed as part of current concussion protocols.9,26,40
Energy availability refers to the amount of energy remaining after exercise to maintain metabolic processes, calculated as the difference between energy intake and exercise energy expenditure relative to fat-free mass.24,25 Energy availability has been widely studied among athletes without concussion given the implications for health and performance.3,16,28,36 A mismatch between energy intake and exercise energy expenditure results in low-energy availability (LEA), a state characterized by inadequate energy to support basic physiologic functions and maintain homeostasis and optimal health.3,4,36 Problematic LEA, or prolonged duration or greater magnitude of LEA exposure, 35 is believed to be the underlying cause of the female athlete triad—the relationship among energy availability, menstrual function, and bone health—and the broader relative energy deficiency in sport (REDs).4,36,37 Chronic LEA may lead to metabolic, physiologic, and hormonal effects, which can negatively affect bone health, gastrointestinal function, reproductive function, injury risk, and athletic performance.3,16,28,34,36 Associations have been reported between LEA and menstrual dysfunction among female athletes (including amenorrhea and oligomenorrhea), a higher prevalence of bone and muscular injuries, and more symptoms of gastrointestinal dysfunction.1,10,29,42,44 Collectively, this evidence indicates that energy availability is a crucial component for optimal athletic performance and overall physical health.
Although the negative effects of LEA for athletes are well documented, particularly for female athletes,1,15,23,39,42,51,55 less is known about whether energy availability influences postconcussion outcomes among adolescents. Despite the “energy mismatch” that occurs in the brain after concussion,8,11 the primary rehabilitation strategy for concussion is physical activity, or exercise energy expenditure. 40 Concussion guidelines set forth by multiple medical groups and consensus statements recommend initiating physical activity at a level that does not exacerbate concussion symptoms within 2 days of concussion and gradually increasing as tolerated.9,26,40 Several studies have reported that physical activity initiated early after concussion is associated with faster recovery time.12,19-21,57 The ideal amount and intensity of physical activity to promote recovery are not fully understood, but emerging evidence suggests that more moderate to vigorous physical activity is associated with faster concussion symptom recovery and reduced anxiety.22,43,47 The evidence supporting physical activity to improve postconcussion outcomes overall is robust12,19-22,43,57; however, return-to-sport guidelines do not consider the full spectrum of energy availability, including basal metabolic demands and energy intake, of the recovering athlete who may be experiencing a mismatch between energy supply and demand.8,11,40 Self-reported LEA indicators (LEA-I) as assessed using the Low Energy Availability in Females Questionnaire (LEAF-Q) 34 are a useful way to obtain information about LEA risk through questions about injuries, gastrointestinal function, and menstrual function. A better understanding of LEA risk during concussion recovery may help individualize physical activity recommendations and nutritional practices/energy intake after concussion to facilitate recovery.
Therefore, to better understand the association between LEA-I and concussion, our primary purpose was to investigate LEAF-Q scores among female adolescents with a recent concussion as compared with uninjured female adolescents. We hypothesized that participants with concussion would have higher, or worse, self-reported LEAF-Q scores, indicative of a higher risk of LEA, as compared with control participants. Our secondary purpose was to examine the relationship between self-reported LEA risk and concussion symptom severity among participants with concussion. We hypothesized that LEAF-Q scores and concussion symptom severity would be moderately correlated.
Methods
This study is a secondary analysis of data collected for a larger prospective study between February 2021 and August 2024 of adolescent athletes with and without a recent concussion who were participating in a variety of organized sports. Athletes from both groups were eligible for inclusion in the parent study if they participated in an organized sport, defined as having a coach and structured practices and competitions. Athletes with concussion were recruited from 2 regional sports medicine programs in Massachusetts and Colorado and through community athletic trainers. Participants in the concussion group were eligible for study inclusion if (1) a physician diagnosed them with a concussion consistent with the definition in the international consensus statement on concussion in sport,30,40 (2) they were seen for initial study assessment within 21 days of concussion, (3) were 13 to 18 years of age, and (4) were symptomatic at the time of study enrollment as defined by a score ≥9 on the Post-concussion Symptom Inventory (PCSI).13,48 Participants were excluded if their concussion was sustained via a high-velocity mechanism, such as a motor vehicle crash, or they experienced a concussion in the previous 6 months before the current concussion. Control participants were included if they were 13 to 18 years of age and had not sustained a concussion in the previous 6 months. This secondary analysis represents a cross-sectional study of the female athletes with and without a recent concussion who were included in the parent study. Female participants from both groups were excluded from the secondary analysis if they were using hormonal medications other than oral contraceptives (ie, patch, ring, implant), owing to LEAF-Q scoring accounting for oral contraceptive use, but not use of other types of hormonal medications. The study was approved by the institutional review board before study commencement. Each participant and one’s parent or guardian if aged <18 years provided written informed assent/consent before study participation.
Study Assessments
During the study assessment, trained research professionals administered a health history questionnaire and symptom surveys. Each participant completed an intake form to provide demographic and health history information, including age, race, ethnicity, and prior concussion. Research professionals also measured participants’ height and weight. Participants completed the LEAF-Q, which involves questions about physiologic symptoms manifesting from low-energy intake, including gastrointestinal symptoms, menstrual dysfunction, and injury frequency. 34 The LEAF-Q score range is 0 to 25, with scores ≥8 indicating high risk for LEA (sensitivity = 0.83, specificity = 0.90). 34 The LEAF-Q has been used to screen for female athlete triad and REDs among adolescent athletes. 27
Participants with concussion rated their symptom severity using the PCSI. 46 The PCSI consists of 22 common concussion symptoms, each rated on a scale of 0 (not a problem) to 6 (severe problem) with higher scores indicating more severe symptoms. We used the PCSI version that was validated for participants between 13 and 18 years of age. 46
Statistical Analysis
Continuous variables are presented as mean (standard deviation) and categorical variables as frequency (percentage). We compared participant characteristics using independent samples t tests for continuous variables and Fisher exact tests for categorical variables. For our primary purpose, we compared LEAF-Q scores between the concussion and control groups using independent samples t tests, and we calculated Cohen d effect size to determine the clinical significance of a between-group difference. We interpreted effect size as small (d = 0.2-0.49), moderate (d = 0.50-0.79), and large (d > 0.8). We then used linear regression to compare LEAF-Q scores between groups while adjusting for age, body mass index (BMI), and participant characteristics that significantly differed between groups. To address our secondary purpose, we calculated correlation coefficients between LEAF-Q and PCSI scores for participants in the concussion group using Pearson r correlation coefficients. We defined correlation strength as follows: 0 to 0.29 (poor), 0.3 to 0.5 (fair), 0.6 to 0.8 (moderately strong), and ≥0.8 (strong). 5 Missing data were treated as such, and no imputations were performed. All tests were 2-sided, and significance was determined a priori as P < .05. Statistical analyses were performed in R Studio (Version 4.2.2; R Core Team).
Results
We initially enrolled 128 female adolescents. Six participants were excluded for incomplete LEAF-Q data, and 5 were excluded because they were taking hormonal medications other than oral contraceptives. Therefore, we included 117 participants in our analysis: 29 who were within 21 days of concussion and 88 uninjured controls (Table 1). A higher proportion of participants in the concussion group reported experiencing a prior concussion as compared with the control group; thus, concussion history was included as a covariate in our multivariable analysis.
Participant Characteristics by Control and Concussion Groups a

Data are reported as No. (%) for categorical variables and mean ± SD for continuous variables.
Those in the concussion group had higher LEAF-Q scores than control participants (Figure 1). A greater proportion of the concussion group scored ≥8, the previously established LEAF-Q score indicating LEA risk (69% of the concussion group vs 32% of the control group). A lower proportion of those with concussion reported experiencing no injury-related absences from training in the past year as compared with controls (Table 2). A higher proportion of the concussion group reported experiencing ≥5 injury-related absences from sport and missing ≥22 days from sports owing to injuries in the past year as compared with the control group. Responses to LEAF-Q questions about gastrointestinal and menstrual function were similar between groups. The 3 participants who reported that they have never menstruated were all <15 years of age (ie, younger than the age that would be considered primary amenorrhea 41 ).
LEAF-Q Responses Stratified by Group a
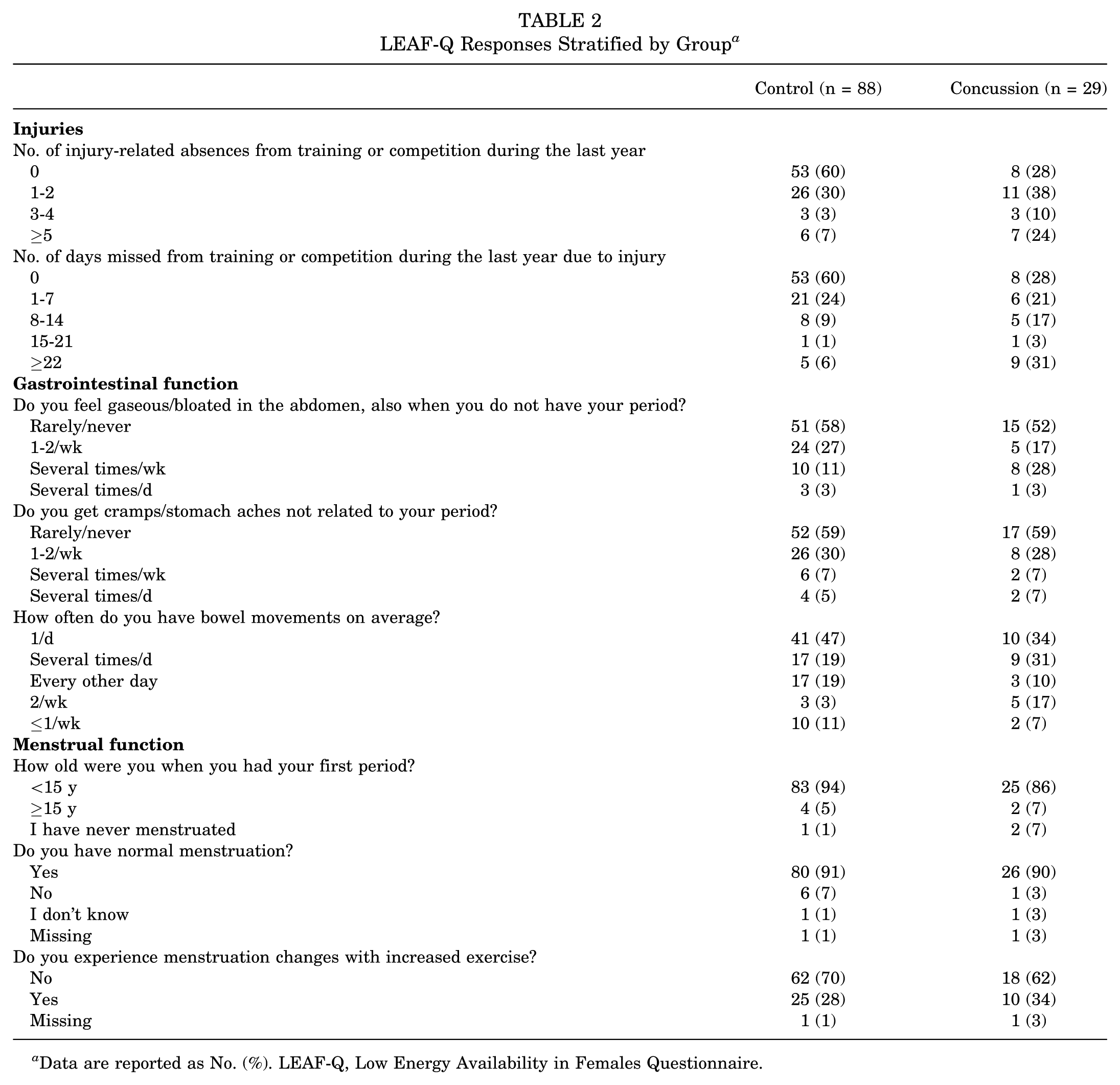
Data are reported as No. (%). LEAF-Q, Low Energy Availability in Females Questionnaire.

Box plot with individual data points (jittered) demonstrating the distribution of LEAF-Q scores between the control and concussion groups. Data are presented as median (line) and interquartile range (box). LEAF-Q, Low Energy Availability in Females Questionnaire.
After adjusting for age and BMI, individuals with a recent concussion scored, on average, 3.23 points higher on the LEAF-Q when compared with controls (Table 3). For the concussion group, we observed a small and insignificant correlation between LEAF-Q and PCSI scores (Figure 2).
Multivariable Regression Model Results for the Association Between Concussion/Control Group and LEAF-Q Scores, Adjusted for Covariates a

LEAF-Q, Low Energy Availability in Females Questionnaire.
Reference group: control.
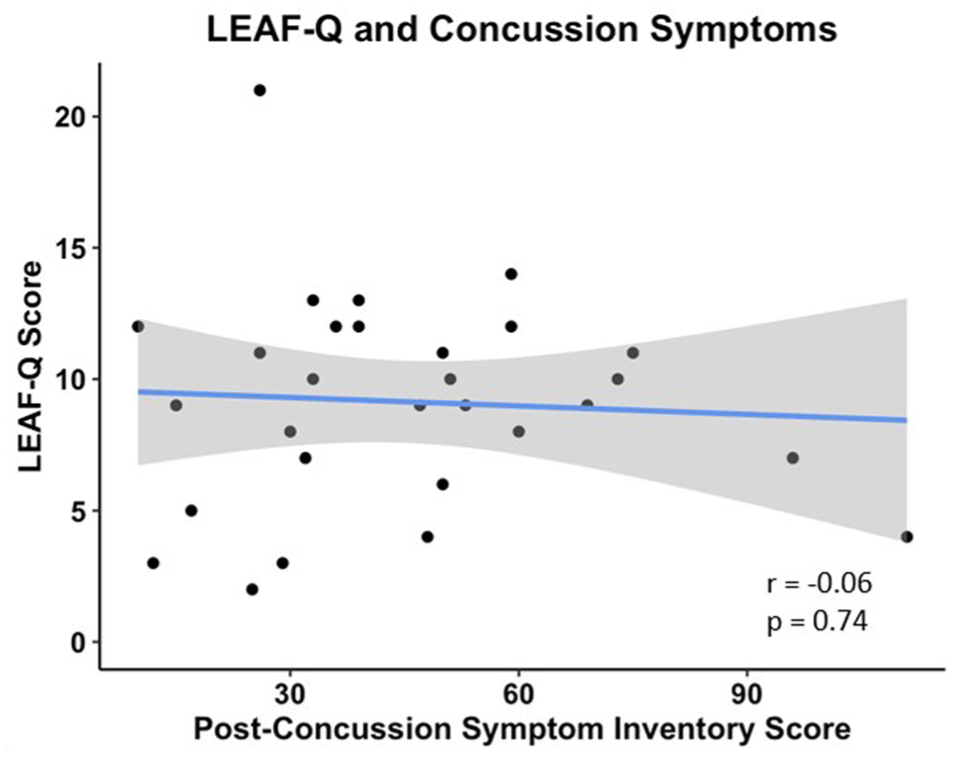
Scatter plot and line of best fit demonstrating the relationship between LEAF-Q and Post-concussion Symptom Inventory scores for the concussion group. Shaded area indicates 95% CI. LEAF-Q, Low Energy Availability in Females Questionnaire.
Discussion
We observed that female adolescents with a recent concussion had higher, or worse, LEAF-Q scores when compared with uninjured controls, indicating that those who sustained a concussion were more at risk for LEA based on higher LEAF-Q scores. The female adolescents with concussion had a mean LEAF-Q score ≥8, which is the previously reported score that indicates LEA risk, 34 while the mean score for the control group was <8. Previous research has observed many negative consequences of LEA on multiple aspects of health and athletic performance among athletes,3,16,28,36 but the relationship between LEA and concussion is understudied. Energy availability may be a critical component to consider after concussion, particularly considering the mismatch between energy supply and demand that is believed to occur after concussion.7,8 LEA may uniquely affect concussion recovery from a nutritional intake and energy expenditure (ie, physical activity) perspective.
Of the 3 components of energy availability assessed on the LEAF-Q—gastrointestinal symptoms, menstrual function, and injury frequency—we observed the biggest proportional between-group differences in questions about injuries. Sixty percent of the control group reported having no injury-related absences from sport in the past year, as opposed to only 28% of the concussion group. It is notable that 28% of the concussion group (8 participants) had no injury-related absences from sport, which suggests that their concussions may have occurred at the end of the season or in their off-season to not result in time loss from training. Furthermore, when compared with the control group, a larger proportion of the concussion group reported sustaining ≥5 injury-related absences from sport in the past year (7% vs 24%) and missing ≥22 days from sports owing to injuries in the past year (6% vs 31%). Given that the concussion group inclusion criteria required assessment within 21 days of concussion (mean, 11.8 ± 4.2 days), it follows that those who missed ≥22 days had sustained at least 1 injury in addition to their current concussion in the past year.
Prior cross-sectional studies have reported associations between LEA and both bone stress and muscular injuries.10,42 Our results build on this previous work, extending the association between LEA-I and injuries to female adolescents with a recent concussion, as the concussion group self-reported higher LEAF-Q scores as compared with controls. The higher proportion of those with concussion reporting multiple injuries over the past year as compared with uninjured controls is notable because sustaining an injury is a risk factor for future injuries. 31 After concussion, there is also a well-documented risk of subsequent injuries, both musculoskeletal injuries and concussions, once athletes return to sport. 32 LEA/LEA-I are associated with musculoskeletal injuries10,42,56 and may similarly be associated with concussions. It is also possible that recovery from a previous injury (musculoskeletal injury or concussion) could contribute to LEA, thus predisposing individuals to subsequent injuries (musculoskeletal injuries and/or concussions). The cumulative influence of multiple injuries throughout the year could have led to a higher-energy demand to heal from these injuries, potentially predisposing the concussion group to a higher risk of having LEA-I. The LEAF-Q may not be responsive to energy availability changes in the days to weeks after concussion; therefore, the higher scores among the concussion group may represent a longitudinal injury risk assessment rather than a postconcussion energy change. Our cross-sectional design limits our ability to address the directionality or temporality of the association between LEA-I and concussion, and future prospective studies are warranted to better understand the relationship between LEA and concussion risk and recovery.
Contrary to the proportional differences that we observed between groups for the injury LEAF-Q questions, we did not observe similar between-group differences for the gastrointestinal or menstrual function questions. To our knowledge, no studies have investigated gastrointestinal function after concussion. However, changes in the gut microbiome have been observed after traumatic brain injury in animal models, with decreased levels of beneficial bacteria reported as early as 2 hours after injury.2,14,38 One study of collegiate football players noted changes in the gut microbiome within 24 to 48 hours of concussion as compared with preseason measures; specifically, decreased levels of anti-inflammatory bacteria were observed. 50 Although changes in the gut microbiome were observed acutely after concussion, this study did not assess changes in gastrointestinal function, 50 and the gut microbiome may not reflect gastrointestinal symptoms as asked about on the LEAF-Q. Our assessment of gastrointestinal function involved self-reported questions about bowel movement frequency, abdominal cramping, and bloating. It is possible that the previously reported changes in gut microbiome after concussion would be associated with higher (ie, worse) gastrointestinal function scores on the LEAF-Q; yet, our initial assessment within 3 weeks of concussion could have occurred before microbiome changes resulted in noticeable alteration in gastrointestinal function that would be captured by the LEAF-Q. It is also possible that concussion is not associated with gastrointestinal function. Prospective studies are needed to better delineate this relationship.
Similarly, we observed minimal differences in self-reported menstrual function questions between our concussion and control groups. A similar proportion of the concussion and control groups reported having normal menstruation (90% vs 91%) and not experiencing menstruation changes with increased exercise (62% vs 70%). Independent of concussion, it may take a month or longer to see the effect of LEA on menstrual function. 37 Because our initial assessment occurred within 3 weeks of concussion (mean, 11.8 ± 4.2 days), changes in menstrual function were likely not reflected in the LEAF-Q scores. Researchers have observed changes in menstrual function among adolescent females and young women 3 to 4 months after concussion.45,49 Therefore, understanding whether a relationship exists between menstrual function and LEA-I after concussion may require more time to pass following injury to be identified via self-report measures. Longitudinal monitoring of LEA-I throughout concussion recovery is needed to better understand if and how energy availability changes after concussion and whether there is an association with menstrual function. We do not have information on medical diagnoses that may contribute to menstrual irregularity, such as polycystic ovary syndrome, which will be an important factor to consider in future research to better understand whether LEA influences menstrual function after concussion.
Our secondary purpose exploring the relationship between LEA-I and concussion symptoms among those in the concussion group indicated a small and insignificant correlation between LEAF-Q and PCSI scores. This suggests that the 2 tools that we used to assess overall concussion symptom severity and LEA-I are measuring different, nonoverlapping constructs. LEA-I may be present independent of concussion symptom severity, and each tool may uniquely inform management strategies for female athletes after concussion. It has been well established that initial concussion symptom severity is the most consistent predictor of recovery time17,33; however, it is unknown whether energy availability influences concussion recovery. The higher LEAF-Q scores for the concussion group versus controls warrants further research to understand if energy availability is associated with recovery time or longer-term outcomes after concussion. Given that physiologic dysfunction can outlast symptoms (ie, clinical recovery) 18 and LEA can lead to metabolic, physiologic, and hormonal effects, 3 it is possible that LEA contributes to ongoing dysfunction beyond clinical concussion recovery. Another possibility is that preexisting LEA may predispose individuals to sustaining a concussion, particularly given associations observed between LEA/LEA-I and musculoskeletal injuries,10,42,56 and further research is needed to better understand the directionality of the association.
Recommendations for concussion recovery are centered on initiating physical activity (ie, exercise energy expenditure) early after injury.9,26,40 However, these recommendations do not consider the more broad concept of energy availability, which may uniquely inform physical activity recommendations by considering energy intake and individual metabolic demands to facilitate healing. The timing, volume, and intensity of physical activity during concussion recovery may need to be individualized to maximize recovery outcomes and may require more nuance than a one-size-fits-all approach. Consideration of LEA risk could help inform the appropriate timing to initiate physical activity, the volume and intensity of the physical activity, and how to nutritionally support the prescribed physical activity recommendations. For example, if an individual is experiencing LEA after concussion, increasing physical activity could potentially exacerbate the LEA, which may complicate or prolong the concussion recovery. There is also the opportunity to provide nutritional recommendations and/or interventions to patients with LEA-I to ensure that they are consuming adequate caloric intake to support their prescribed physical activity and concussion recovery. Additionally, there is a bidirectional relationship between LEA and mental health outcomes, including increased anxiety and depression. 35 This is particularly concerning during concussion recovery, as these symptoms are often elevated after concussion, 6 which could be exacerbated by LEA. 35 Addressing LEA may help support postconcussion mental health outcomes. More moderate to vigorous physical activity after concussion is associated with improved mental health outcomes 47 ; thus, optimizing nutritional intake may indirectly benefit mental health by supporting the recommended physical activity intensity to reduce mental health symptoms during concussion recovery. Further research is needed to understand whether and how energy availability influences physical activity tolerance, overall concussion recovery, and specifically mental health outcomes after concussion.
Limitations
Our study has limitations that should be considered when interpreting our results. Our assessment of LEA-I was by self-report, and as with any self-report measure, our results could be influenced by the accuracy of participant responses. The retrospective nature of many of the LEAF-Q questions may limit the accuracy of the results owing to recall innacuracy (ie, how many injury-related absences from sports in the past year, how many days missed from sports in the past year owing to injury, age at first period). The LEAF-Q assesses LEA risk only and is not diagnostic of LEA. The LEAF-Q scores may be more representative of injury risk than true energy availability, so research using more objective measures of energy is needed. Disordered eating/eating disorders may also be important factors to consider for future research examining the association between LEA and concussion, particularly given prior work that reported a connection between disordered eating and sport-related injuries among adolescent female athletes. 53 We used BMI in our analysis, although BMI values may be normal for some female athletes with low body fat percentage 54 ; thus, body fat percentage may be a better measure of body composition, particularly in the setting of LEA. Our study population was recruited from 2 locations in large metro areas and includes a mostly White, non-Hispanic population, which may limit generalizability to other populations. Study participants were also a general sample of adolescents who were physically active, but they were not exclusively athletes who were actively participating in organized sports at the time of evaluation.
Conclusion
Female adolescents within 3 weeks of concussion had higher LEAF-Q scores than uninjured controls, suggesting that there may be an association between concussion and LEA-I. The difference that we observed in LEAF-Q scores between the concussion and control groups appears to be driven by differences in injury history as recorded on the LEAF-Q, with the concussion group reporting more injury-related absences in the past year than the control group. Among participants with a concussion, there was no significant association between LEAF-Q scores and concussion symptom severity, suggesting that LEA-I may not be associated with common concussion symptoms. Prospective studies are needed to better understand energy availability longitudinally throughout concussion recovery and its implications on individual treatment approaches, including nutritional guidance and physical activity recommendations.
Footnotes
Final revision submitted May 19, 2025; accepted July 15, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01HD108133) and the Denver Broncos Foundation. W.P.M. receives royalties from ABC-Clio Publishing, Springer International, and Wolters Kluwer and has received a grant from the National Football League. J.C.W. is a network team physician for US Soccer. D.R.H. has received research support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R03HD094560), the National Institute of Neurological Disorders and Stroke (R01NS100952, R43NS108823), the National Institute of Arthritis and Musculoskeletal and Skin Diseases (1R13AR080451), 59th Medical Wing Department of the Air Force, MINDSOURCE Brain Injury Network, the Tai Foundation, and the Colorado Clinical and Translational Sciences Institute (UL1 TR002535-05). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Colorado.