
Abstract
Background:
Labral eversion has recently been described as an anatomic variation in a nondysplastic patient with impingement-type hip pain and an otherwise intact labrum that is associated with microinstability.
Purpose:
To compare clinical outcomes after hip arthroscopy between patients with hip microinstability caused by everted labrums and those with femoroacetabular impingement (FAI).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included patients who underwent surgery at a tertiary hospital center between 2015 and 2022 after failure of nonoperative treatment for at least 6 months. Data—including demographic characteristics, body mass index, visual analog scale (VAS) scores, and preoperative and long-term follow-up Hip Outcome Score (HOS), lateral center-edge angle (LCEA), and upsloping lateral sourcil—were collected from the clinical records. The same surgical team treated all patients, followed the same rehabilitation protocol, and observed them for a minimum of 24 months. Clinical improvement was evaluated using HOS, VAS, and return to sports outcomes. Patients were organized into 2 groups. Group 1 included patients with an intraoperative diagnosis of everted labrum, whereas group 2 served as the control group, consisting of patients with classic FAI associated with labral tears. Statistical analysis was performed using the t test and 95% CI.
Results:
A total of 76 patients (n = 88 hips) who underwent hip arthroscopy during the study period were divided into 2 groups. We found a greater presence of upsloping lateral acetabular rim in group 1 (65% vs 11%; P = 4.77 × 10-7). Group 1 demonstrated a significantly greater LCEA compared with group 2 (37.1° vs 34.6°, respectively; P = .010). The HOS scores were 91.6 and 92.2 (P = .226) and 97.8 and 98.1 (P = .575) in groups 1 and 2, respectively, at 6 and 12 months postoperatively. Furthermore, postoperative VAS scores were not significantly different between the 2 groups (P = .574).
Conclusion:
Our study demonstrated that clinical and functional outcomes are not significantly different between patients operated on for an everted labrum with intra-articular anchor placement technique and those operated on for normal labral tears in FAI.
These findings suggest that, when appropriately identified and treated with a technique focused on restoring the labral seal, the everted labrum does not negatively affect long-term postoperative results. Recognition and proper management of this anatomic variant are therefore essential in achieving successful surgical outcomes.
The acetabular labrum is a fibrocartilaginous extension of the acetabular rim. 1 An intact labrum forms a suction seal, aids in proprioception and nociception, increases acetabular volume and articular surface area, dissipates loads, lubricates the joint, preserves cartilage, and stabilizes the femoral head during distraction.6,12 Hip suction seal, as described by Philippon et al, 14 refers to the biomechanical phenomenon where the acetabular labrum contributes to the stability of the hip joint by creating a negative pressure seal. This seal is crucial for maintaining hip stability against distractive forces. 14 Femoroacetabular impingement (FAI) frequently causes labral tears, which, in turn, can compromise the suction seal.
Based on its size and shape, several anatomic variants of the acetabular labrum (eg, triangular, flat, round, or irregular) have been defined.11,18 There is a relationship between a hypertrophic labrum and a decreased lateral center-edge angle (LCEA). 15 A hypertrophic labrum is commonly associated with hip dysplasia, whereas a hypoplastic labrum is observed in pincer-type FAI. 2 Labral eversion, when observed during revision arthroscopy, is characterized by an increased space between the labrum and the femoral head. This condition is often the result of a suboptimal arthroscopic labral repair, making it an iatrogenic injury. Its management typically involves labral reconstruction to restore the suction seal.
The “everted labrum” refers to a variant of the acetabular labrum where the labrum is flipped to the capsular side of the acetabular rim, resulting in a lack of apposition to the femoral head. 17 Imaging signs, such as the absence of contact between the labrum and the cartilage on coronal fat-saturated T2-weighted magnetic resonance imaging (MRI), are indicative of an everted labrum. In addition, a bone footprint is observed at the acetabular level, where the load zone is lost in relation to the contact zone of the labrum with the femoral head. 11
Recently, labral eversion has been described as an anatomic variation in nondysplastic patients with Pincer-type hip pain and an intact labrum, with no other injuries. The arthroscopic evaluation of the everted labrum involves identifying a native labral variant during hip arthroscopy, which is characterized by a segment of the acetabular labrum that lacks apposition to the femoral head when the hip is off traction. The everted labrum can be identified by assessing the labral seal during arthroscopy. 17
Herein, we present our approach for the operative treatment of patients with native labral eversion, with a focus on restoring labral function through appropriate repair techniques. Furthermore, we compare clinical outcomes in patients with hip microinstability caused by labral eversion to those with classic FAI. This study aimed to compare clinical outcomes after hip arthroscopy between patients with microinstability due to everted labrums and those with FAI-related labral tears. We hypothesized that patients with native everted labrums would show similar clinical improvements after arthroscopic labral repair compared with patients with FAI, when treated with a targeted surgical approach to restore the labral seal.
Methods
A descriptive retrospective cross-sectional study was performed with the approval of the scientific ethics committee of our institution (Scientific Ethics Committee of Orient Metropolitan Health Service; November 7, 2023). The study included patients who underwent surgery at a tertiary hospital center between 2015 and 2022 after failure of nonoperative treatment—including nonsteroidal anti-inflammatory drugs and physical therapy for at least 6 months. Written informed consent was obtained from all patients. All patients were operated on by a team of 2 senior surgeons (C.R. and J.E.M.) with >15 years of experience using the same approach. Nondysplastic patients with clinical manifestation of hip pain, apprehension test, traction test, joint laxity, and radiological signs of instability (upsloping acetabular source) underwent MRI with hipplastic or everted labrum, and underwent hip arthroscopy, in which an everted, hypoplastic, or insufficient labrum was confirmed during surgery. Dysplasia of the hip was defined 13 by the LCEA of <18°. FAI was compared between this group and a control group of patients with labral tears. Data—including demographic characteristics, age, body mass index (BMI), visual analog scale (VAS) scores, and preoperative and follow-up Hip Outcome Scores (HOS)—were collected from the clinical records at 1, 6, and 12 months. Complications such as adhesive capsulitis or adhesion, and iliotibial band friction were documented. Patients were organized into 2 groups: group 1 included patients with an intraoperative diagnosis of everted labrum, whereas group 2 served as the control group, consisting of patients with classic FAI associated with labral tears.
The exclusion criteria were age >50 years, dysplastic hips with indications for periacetabular osteotomy (<18° LCEA), previous revision hip arthroscopy, calcified labrum on radiographs or MRI, or the presence of significant chondral pathology that required other treatments (microfractures, or other) during hip arthroscopy.
Imaging Studies
After a complete clinical evaluation by 2 hip arthroscopists, standardized imaging studies—including anteroposterior pelvic radiography, anteroposterior hip radiography, and the Dunn view at 45°—were requested. Based on the LCEA, the acetabular coverage was classified as normal (25°-39.9°), overcoverage (≥40°), borderline dysplasia (18°-24.9°), or dysplasia (<18°). Based on the acetabular index, the acetabular coverage was classified as normal (0°-10°), overcoverage (<0°), or dysplasia (>10°). Hips with a femoroepiphyseal acetabular roof index of >5° with normal lateral convergence were classified as dysplastic. 20 Furthermore, hips with an anterior-wall coverage of <30% were classified as dysplastic. We also looked for the upsloping lateral acetabular rim described by Wong et al. 19 Moreover, MRI of the affected hip was performed, and if necessary, MR arthrography was performed under local anesthesia using lidocaine. MRIs were evaluated in consultation with a musculoskeletal radiologist trained in musculoskeletal radiology with ≥20 years of experience in the field (G.D.) to rule out labral tears. Labral dimensions were measured on MRI, and the labrum was characterized into 3 groups: hypoplastic, normal, and hypertrophic, based on the height-to-width ratio. The labral cross-sectional area describes hypotrophic labrum 12.1 mm2, normal 25.2 mm, 2 and hypertrophic 41.1 mm2 (Figure 1). Hypoplastic/everted labrum was defined as a height-to-width ratio of 2 to 1 on MRI, as described by Toft et al. 16
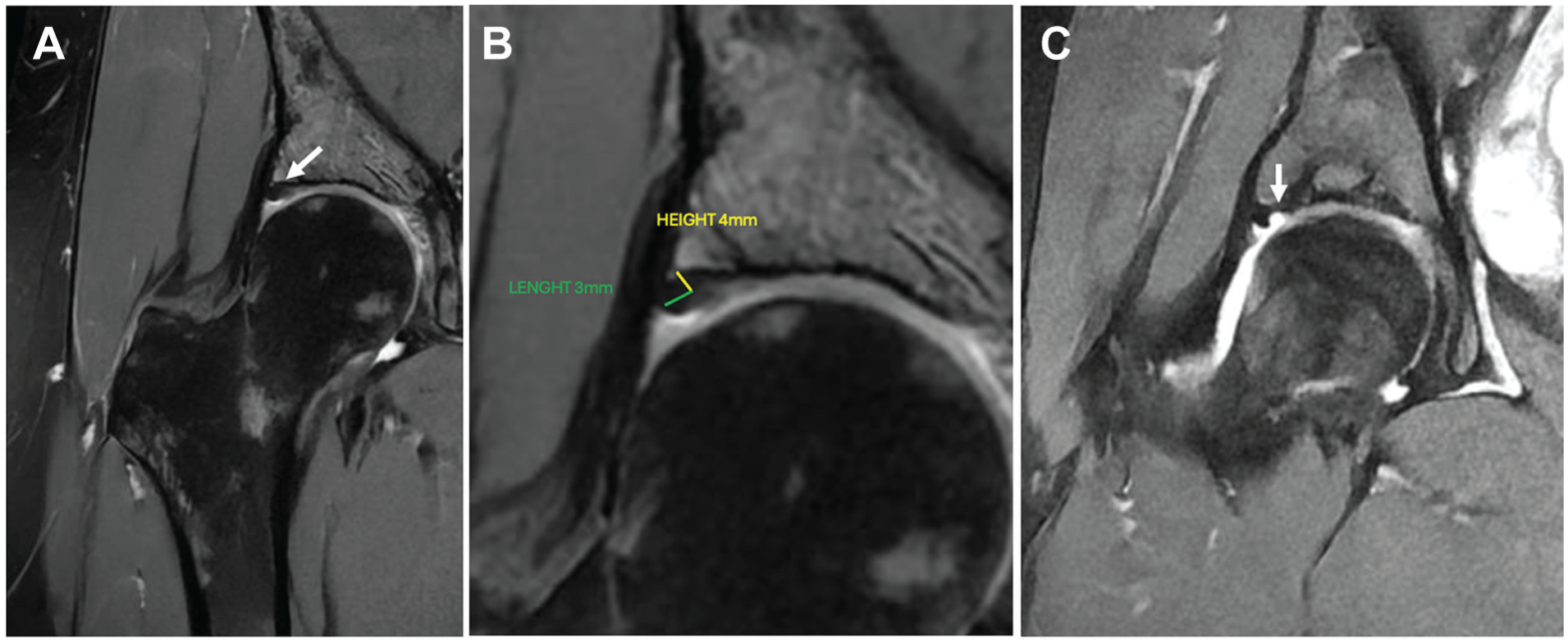
Coronal proton-density fat-suppressed MRI of the right hip. (A) An everted, hypotrophic acetabular labrum without a suction seal (white arrow). (B) The same image showing labral measurement; hypoplastic labrum measuring 3 × 4 mm (yellow and green lines). (C) Defect filled with intra-articular contrast indicating loss of the intra-articular vacuum effect (white arrow). MRI, magnetic resonance imaging.
Surgical Technique
Patients were anesthetized on a traction table. Anterior, anterolateral, and distal anterolateral portals were created, and a longitudinal capsulotomy was performed using an out-in approach. Visualization of the labrum without traction was achieved in all cases where a labrum everted to the capsular side (group 1) or a labrum positioned to the femoral head (group 2) was observed (Figures 2 and 3). Traction was applied to the hip, and the absence of a vacuum seal was confirmed. To further assess joint stability, flexion, axial traction, and rapid extension maneuvers were subsequently performed (Figure 4). The bone bed in the capsular side of the acetabulum was debrided, traction was released, and the entire labrum was repositioned toward the femoral head. The labrum was reattached using 2 to 4 intra-articular anchors on the acetabular side with a curved guide and sutured without traction, avoiding overcorrection. To achieve this, we positioned the femoral head toward the labrum (Figure 5). Finally, articular vacuum tests were performed. Femoral osteoplasty was performed if necessary, and the joint capsule was closed with normal rotation and without tension.

(A) Arthroscopic visualization of the everted labrum without traction from the anterolateral portal. (B) Explanatory schematic representation. A, acetabulum; AC, acetabular cartilage; C, capsule; EL, everted labrum; FH, femoral head.

(A) Arthroscopic visualization of a normal labrum without traction from the anterolateral portal. (B) Explanatory schematic representation. A, acetabulum; AC, acetabular cartilage; C, capsule; FH, femoral head; L, labrum.

Evaluation of hip instability. (A) Anteroposterior radiograph of the hip demonstrating an upsloping acetabular rim (red arrow). (B) Fluoroscopic view of the Hip subluxation under manual traction (red arrow). (C) hip subluxation using manual traction.

(A) Anterolateral portal view, intra-articular side-anchor placement from the distal anterolateral portal (DALA). (B) Schematic illustration of intra-articular side-anchor positioning. (C) Final repair of the everted labrum with restoration of the labral suction seal viewed from the anterolateral portal. A, acetabulum; AC, acetabular cartilage; EL, everted labrum; FH, femoral head; RL, repaired labrum.
Rehabilitation Protocol
Patients commenced ambulation with 2 Canadian crutches on the day of surgery, once the effects of anesthesia wore off, and were discharged 24 hours after surgery, after completing 2 physical therapy sessions. They were followed up once, 1 week postoperatively, to evaluate any early complications. They started physical therapy 1 week after surgery and completed 20 to 30 sessions. Thereafter, sequential evaluations were performed, in which 1 crutch was removed at 2 weeks, full weightbearing was permitted at 3 weeks, and complete rehabilitation was achieved between 8 and 12 weeks. Return to sports is typically achieved between 4 and 6 months, depending on the level of functional recovery. Patients were followed every 6 months for up to 1 year after surgery.
Statistical Analysis
Continuous variables—including HOS and VAS scores—were expressed as means and standard deviations. A paired-samples Student's t test was used to compare pre- and postoperative values within each group. In addition, independent-samples t tests were employed to compare outcomes between the 2 groups (everted labrum vs FAI control). A chi-square test was used to analyze categorical variables—including sex distribution and complication rates. Statistical analysis was performed using Stata/SE 18.0 (StataCorp). Statistical significance was set at P < .05.
A post hoc power analysis was performed using the observed means and standard deviations. The study had sufficient power (>99%) to detect major within-group differences (pre- vs postoperative HOS), but limited power (~37%) to detect minor between-group differences.
Results
This study included 76 patients (n = 88 hips) who underwent hip arthroscopy between 2015 and 2022. Participants were divided into 2 groups: group 1 (n = 44 hips) included patients with an intraoperative diagnosis of everted labrum, whereas group 2 (n = 44 hips) served as the control group, consisting of patients with classic FAI associated with labral tears.
Patient Characteristics
All patients were Caucasians. Groups 1 and 2 included 8 men and 29 women, and 21 men and 18 women, with a mean age of 33.8 years and 33.9 years, respectively. The mean BMI in groups 1 and 2 was 23.7 and 24.6 kg/m2, respectively (Table 1). A total of 7 patients exhibited bilateral everted labrum in group 1, whereas 5 patients had bilateral impingement in group 2.
Comparison of Demographic and Imaging Characteristics Between the 2 Groups a

Data are presented as mean SD, unless otherwise indicated. The bold P values indicate statistical significance (P < .05). AI, acetabular index; BMI, body mass index; F, female; LCEA, lateral center-edge angle; M, male.
Imaging
Group 1 had a mean LCEA of 37.1° (range, 29°-47°). Normal values were observed in 64% of patients, and 36% showed no overcoverage; no dysplasia was observed in this group. In group 2, the mean LCEA was 34.6° (range, 20°-50°), and normal values were reported in 72% of patients. Overcoverage and borderline dysplasia were observed in 20% and 8% of patients, respectively, and the difference was statistically significant (P = .033). The acetabular index in groups 1 and 2 was 3.5° and 3°, respectively; however, the difference was not statistically significant (P > .05). The percentage of anterior-wall coverage was 48% and 47% in groups 1 and 2, respectively; nonetheless, the difference was not statistically significant (P > .05). An upsloping acetabular rim was present in 65% of patients in group 1 compared with 11% of patients in group 2, which was statistically significant. (P = 4.77 × 10-7).
The preoperative HOS and VAS scores in groups 1 and 2 were 66.9 and 6.3, and 63 and 7.1, respectively (Table 2). At 1 month postoperatively, the HOS scores were 79.3 and 77.5 in groups 1 and 2, respectively, representing a statistically significant difference with respect to the preoperative HOS scores of the same groups (P value 5.39 × 10-22 and 1.38 × 10-16, respectively). At 6 months postoperatively, the HOS scores in groups 1 and 2 were 91.6 and 92.2 (P values 4.06 × 10-23 and 1.33 × 10–25, respectively), representing a statistically significant difference with respect to the preoperative HOS scores of the same groups. The mean duration to achieve HOS scores of >97 was 4 months, and the VAS score was 0 at discharge. At 12 months postoperatively, the HOS scores in groups 1 and 2 were 97.8 and 98.1 (P = 2.08 × 10-34 and 1.03 × 10–36, respectively), representing a statistically significant difference with respect to the preoperative HOS scores of the same groups. Complications were observed in only 9% of the patients in group 1 (4/44 patients), including 3 cases of iliotibial band friction syndrome and 1 adhesive capsulitis. Group 2 had a complication rate of 6.8% (3/44 patients), including 2 cases of adhesive capsulitis and 1 case of deep vein thrombosis. No patient required revision surgery. The VAS pre- and postoperative values between the same group were not statistically significant (P values of 1.02 × 10-32 and 9.58 × 10-22, respectively). Comparison of the pre- and postoperative VAS scores and HOS scores within the same group revealed statistically significant differences (P < .05). Comparison of the postoperative outcomes between the 2 groups showed no significant differences (VAS, P = .57; HOS, P = .58) (Table 2). Follow-up was completed in 70 patients (n = 82 hips), with no patients requiring surgical revision and no minor complications reported. A total of 6 patients were lost to follow-up at the 1-year mark (n = 6 hips): 3 from group 1 and 3 from group 2. This evenly distributed attrition did not affect the statistical analysis and was insufficient to compromise the study's statistical power.
Comparison of Pre- and Postoperative Characteristics Between the 2 Groups a
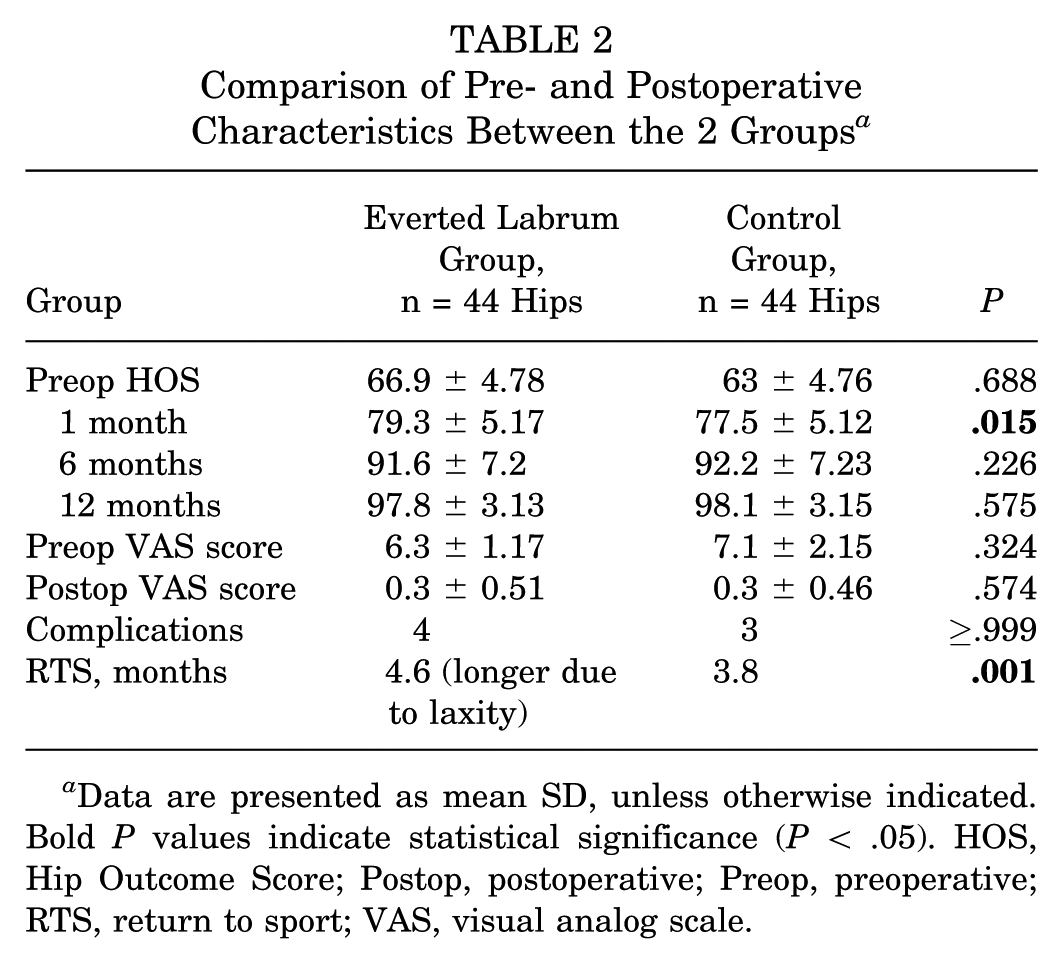
Data are presented as mean SD, unless otherwise indicated. Bold P values indicate statistical significance (P < .05). HOS, Hip Outcome Score; Postop, postoperative; Preop, preoperative; RTS, return to sport; VAS, visual analog scale.
Power analysis confirmed adequate sensitivity to detect the large clinical improvements observed within each group. However, the study also revealed limited power for identifying minor intergroup differences, such as those found in early postoperative HOS comparisons.
Discussion
The most important finding of this study is that an everted labrum is a recognized cause of hip microinstability, and its arthroscopic repair using intra-articular anchor placement successfully restores joint stability, with similar outcomes in HOS (P = .575) and VAS (P = .574) to those of classic FAI, with similar complications (P≥ .999). Notably, patients with this anatomic variant achieved clinical and functional outcomes comparable with those of patients with anatomically normal labrums presenting with reparable labral tears due to FAI.
These results may support the effectiveness of targeted labral management in addressing instability caused by structural labral insufficiency and reinforce the importance of recognizing this variant during surgical planning. Although an everted labrum without complications has recently been described with results similar to a classic FAI, 5 we have been identifying and addressing this pathology as a cause of hip microinstability for 7 years. In a study on dogs, Kim 9 demonstrated that an everted labrum causes instability and subsequent hip dysplasia. However, this association remained unclear until it was described by Vogel et al. 17 In addition to an everted labrum, we observed hypertrophy of the articular cartilage as a compensatory mechanism for load and tangential tension. 8 Despite the cartilage suggesting dysplasia, we did not find a hypertrophic labrum; on the contrary, it was hypoplastic and insufficient. One hypothesis is that the labrum assumes a hypoplastic and everted position owing to the growth of the acetabulum, which often exhibits an upsloping lateral rim in dysplastic hips. 19 Thus, this condition can be suspected based on an increase in the joint space toward the most lateral part of the acetabulum with an upsloping acetabular rim on anteroposterior pelvic radiographs (see Figure 5). However, previous studies have associated these findings with a hypertrophic labrum and hip instability. 18 Notably, the increased acetabular coverage in the target group compared with that in the control group in this study may be related to the presence of a hypoplastic labrum with a pincer type of FAI. A smaller labrum may not be able to create a vacuum, which, in our opinion, could explain the hip instability.
The suspicion of pain due to the instability was reinforced in the operating room using a fluoroscope during manual traction and achieved subluxation (Figure 4), and was confirmed arthroscopically when the labrum was visualized without traction and with the absence of vacuum (Figure 2).
In patients with pincer-type FAI presenting with an everted labrum, the use of intra-articular anchor placement is a recommended technique for restoring the labral seal and reestablishing hip joint stability. This approach allows precise repositioning of the labrum against the femoral head, recreating the suction effect that is essential for joint function and pain relief. Given that labral eversion often results in a loss of apposition and vacuum seal, especially in the context of overcoverage, intra-articular suture anchor fixation provides biomechanical advantages by securing the labrum closer to its native footprint. Previous studies have supported the superiority of anchor-based repair in restoring labral function and improving postoperative outcomes in cases of labral insufficiency because of mechanical alterations, such as those seen in pincer-type morphology.4,7
Vogel et al 17 proposed 2 factors that may contribute to an everted labrum in patients with hip dysplasia: (1) the shearing forces characteristic of hip instability due to a lack of apposition to the femoral head and (2) mismatch in growth between the acetabular rim and the labral tissue, leading to stretching of the labral tissue resulting in a smaller cross-sectional diameter. In contrast, in dysplastic hips, a noneverted labrum often hypertrophies due to mechanical stimulation by the developing hip, which is directly related to the degree of bone coverage. 10 In such cases, proper management of the labrum—including using intra-articular anchors to suture the labrum in a "C" shape completely—is crucial to restore the labral seal. 7 This is grounded in the understanding of labral morphology and its role in hip stability and dysplasia management described by Jackson et al. 7 Fry and Domb 4 provide additional insights into the technique of labral base refixation. The technique described involves refixation of the labrum at its base to reestablish the labral seal and improve joint stability. In a biomechanical study, 3 there is discussion about the advantage of a triangular versus tubularized reconstruction because it is more similar to the anatomic shape. Performing suturing without traction brings us closer to this shape. Overall, the rationale for a "C"-shaped configuration in labral repair is to ensure that the labrum can effectively contribute to hip stability by maintaining its anatomic shape and function.
Limitations
This study had several limitations. First, this study was retrospective, with a small sample size. Because native labral eversion is not a common anatomy shape of the labrum and has not been widely reported, the limited information available precluded a high-quality study. In the future, the patient cohort could be supplemented by those from other centers, following the same approach, to increase the number of cases. Second, as this condition is still not fully understood, the implications are inferred from the clinical improvement of patients upon restoration of labral function. Third, the functionality of the labrum of asymptomatic patients with an upsloping acetabular rim or an everted labrum on MRI is unknown. Further studies are needed to understand the biomechanics that cause this condition and how it can be prevented.
Conclusion
Our study demonstrated that clinical and functional outcomes are not significantly different between patients operated on for an everted labrum with intra-articular anchor placement technique and those operated on for normal labral tears in FAI.
These findings suggest that, when appropriately identified and treated with a technique focused on restoring the labral seal, the everted labrum does not negatively affect long-term postoperative results. Recognition and proper management of this anatomic variant are therefore essential in achieving successful surgical outcomes.
Footnotes
Final revision submitted May 18, 2025; accepted July 8, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Scientific Ethics Committee of the Orient Metropolitan Health Service.
Data Availability Statement
The data sets generated and/or analyzed during the current study are not publicly available due to confidential information, but are available from the corresponding author on reasonable request.