
Abstract

Pseudoaneurysms, also known as false aneurysms, occur when there is a breach in the arterial wall and pulsating blood escapes into the surrounding tissue but is contained by the surrounding adventitia or fibrous tissue, rather than all 3 layers of the vessel wall as in a true aneurysm.1,3 It can result in a hematoma, which is the pooling of blood that lacks communication with the arterial lumen. Clinically, they may present as localized swelling and tenderness. While the swelling accompanying a pseudoaneurysm can appear similar to a subcutaneous abscess, it can be differentiated and diagnosed using duplex ultrasonography, color Doppler, and computed tomography angiography.3,5,10 Treatment includes surgical interventions such as ligation, resection, and revascularization, 7 while nonsurgical options include ultrasound-guided compression repair, percutaneous thrombin injection, and collagen injection. 4 Previous case reports have described a pseudoaneurysm resulting from ligation and bypass of a popliteal artery aneurysm leading to a pathologic femoral fracture 6 in addition to pseudoaneurysms resulting from osteochondromas of the distal femur. 5 There are limited case reports investigating femoral pseudoaneurysms that could be due to bony outgrowths. This case report details a surgical correction of a femoral pseudoaneurysm, which could have formed due to a bony prominence perforation of the artery.
Case Presentation
Patient is a 17-year-old male with a medical history of type 1 diabetes mellitus who initially presented for an injury involving his right leg. The patient was running during a sporting event when he felt acute pain in the posterior thigh. Initial examination was unremarkable, with only tenderness to palpation over the medial hamstring muscle belly noted. Radiographs obtained demonstrated a small bony exostosis of the posterior distal femur (Figure 1).

(A) Lateral radiograph of the right knee demonstrating an exostosis-like lesion off the posterior distal femur. (B) Anteroposterior radiograph of bilateral knees.
Over the next 2 weeks, he developed numbness over the distal posterior thigh with extension to the anterior medial aspect of his shin, accompanied by swelling to the posterior thigh. He denied any tingling, paresthesia, or weakness. Magnetic resonance images of the right thigh demonstrated a near full-thickness tear of the distal semimembranosus muscle and a 5.2 × 8 × 11.2–cm intramuscular hematoma. The patient was initially treated with physical therapy and nonoperative measures, which significantly improved his pain and function. However, the swelling remained. Subsequent images obtained over the course of the next 4 months demonstrated a significant increase in size of the hematoma (12.8 × 12.4 × 24.4 cm) along with mass effect on the adjacent neurovascular structures (Figures 2-4). The patient was evaluated by a musculoskeletal oncology team (including A.T.B.) to rule out neoplastic etiology of the posterior thigh mass. A biopsy was performed and consistent with a hematoma showing blood clot and fibrin with focal organization, and no evidence of malignancy.
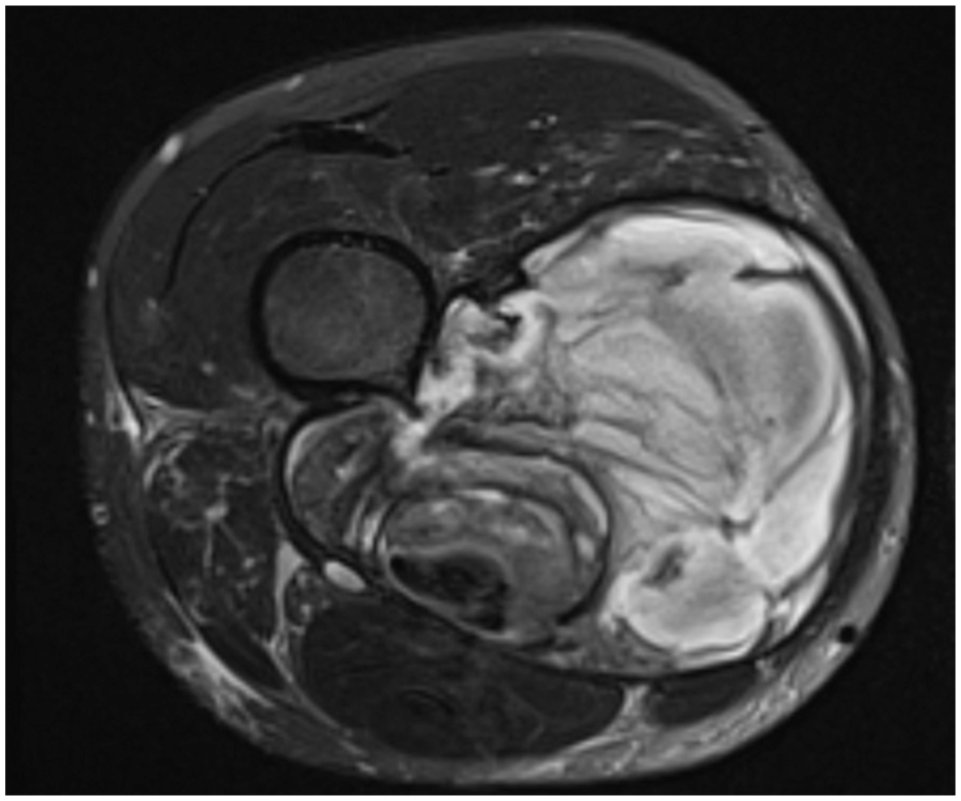
Axial T2 fat-suppressed magnetic resonance imaging of the right lower extremity demonstrating a heterogeneous circumscribed collection within the medial aspect with mass effect on the surrounding neurovascular structures.
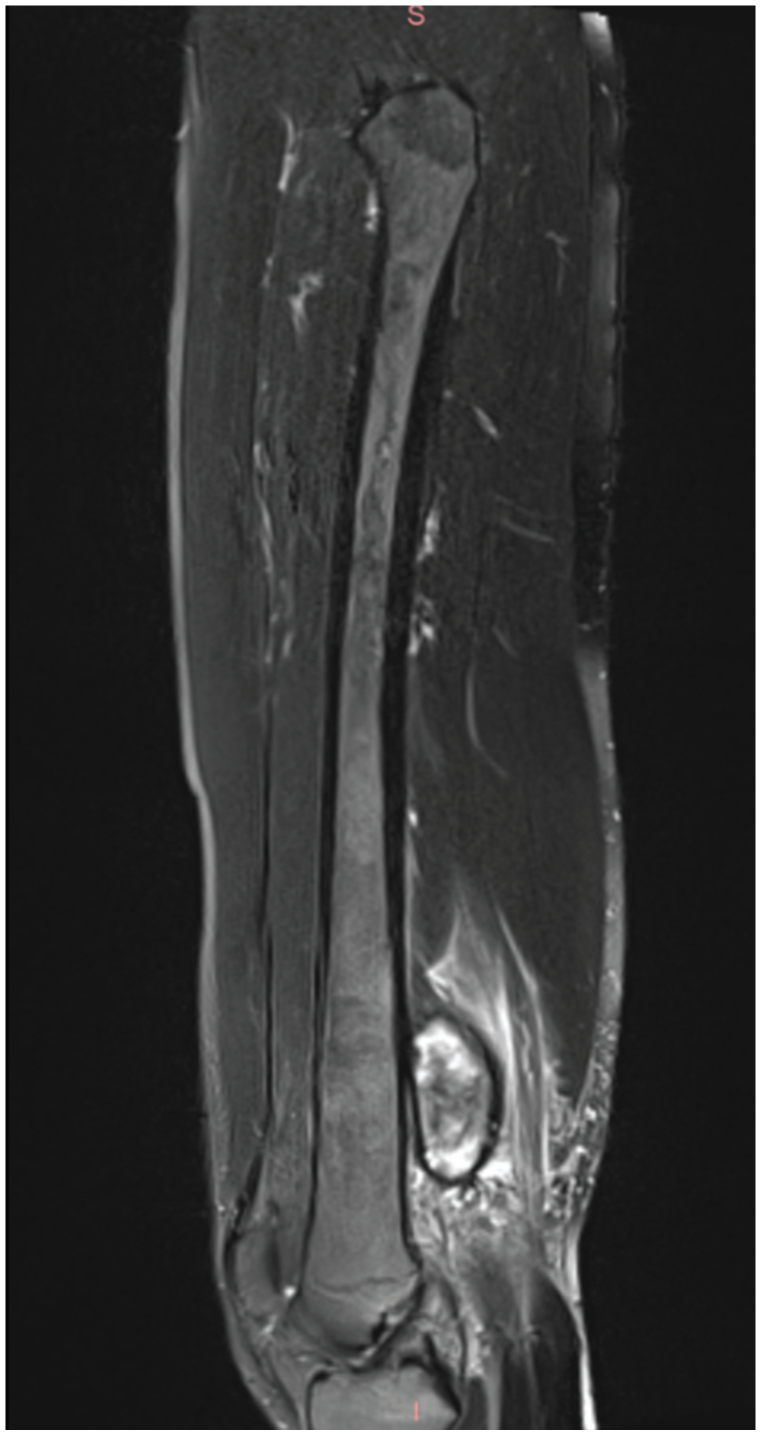
Sagittal T2 fat-suppressed magnetic resonance imaging demonstrating a heterogeneous collection in the medial thigh with hyperechoicity within the semimembranosus muscle.
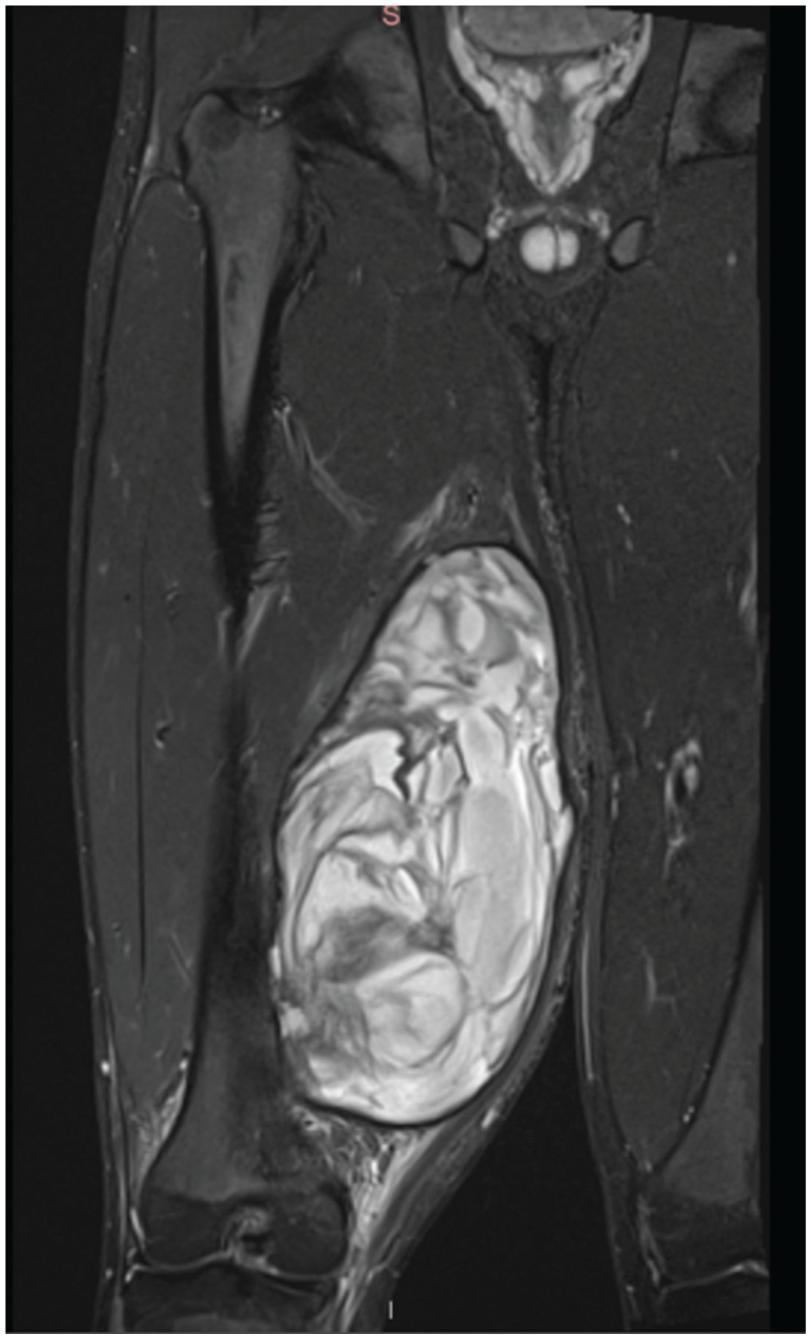
Coronal T2 fat-suppressed magnetic resonance imaging demonstrating a large heterogeneous circumscribed mass in the medial thigh with hyperechoicity within the distal semimembranosus.
Because of the symptomatic nature of the mass, surgical intervention was planned. A multidisciplinary surgical team decided to proceed with a first-stage interventional radiology evaluation and possible embolization of any active bleeding vessels into the hematoma. The second stage involved a minimally invasive evacuation of the hematoma. However, during the embolization procedure, the patient was found to have a large expanding pseudoaneurysm arising from the distal superficial femoral artery (SFA) (Figure 5). This prompted a vascular surgery consultation, which recommended open repair.

Right lower extremity arteriogram demonstrating pseudoaneurysm arising from the distal superficial femoral artery.
The patient was brought to the main operating room with vascular surgery the next day. An exploration of the SFA was performed at the level of the pseudoaneurysm. Once proximal control was established, a longitudinal incision was made medially over the hematoma and carried through the subcutaneous tissue and crural fascia. A 1.25-kg hematoma was then evacuated, exposing the SFA and pseudoaneurysm. Additionally, a 1-cm bony outgrowth was identified arising from the posterior femur at the level of the pseudoaneurysm, in proximity to the superficial femoral and proximal popliteal arteries (Figure 6). Pathology described the growth as necrotic bone and marrow. The devitalized bone had likely perforated the artery and contributed to the semimembranosus tear during the traumatic event due to the adjacent location.

Exostosis-like lesion from the posterior aspect of the distal femur.
Because of significant damage to the SFA, the decision was made to proceed with a bypass using a 10-cm segment of the greater saphenous vein (Figure 7). An angiogram confirmed adequate flow and significant vasospasm. There were no other complications, and the patient was safely discharged 4 days later. One year after the surgery, the patient noted no discomfort in his leg and was able to ambulate independently with full strength. Peripheral arterial duplex assessment demonstrated patent, triphasic right lower extremity arteries including the distal SFA to proximal popliteal artery interposition bypass graft.

(A) Arteriotomy (arrow) and removal of GORE VIABAHN Endoprothesis. (B) End-to-end popliteopopliteal bypass (arrow) using a reversed ipsilateral greater saphenous vein.
Discussion
Our case demonstrates the development of a pseudoaneurysm in the SFA secondary to an exostosis-like lesion trauma after a hamstring tear. Pseudoaneurysms occur when there is a breach in the arterial wall and pulsating blood escapes into the surrounding tissue but is contained by the surrounding adventitia or fibrous tissue.1,3 Common causes of pseudoaneurysms include trauma, such as blunt or penetrating injuries, and iatrogenic factors such as surgical procedures or invasive diagnostic interventions.1,4 In the context of trauma, pseudoaneurysms can arise from direct vessel injury or as a result of adjacent bone or soft tissue structures causing mechanical damage to the arterial wall. 1 Previous case reports reported bone causes such as osteochondroma 5 and interestingly described a femoral fracture as a result of a popliteal artery pseudoaneurysm. 6
Involvement of an exostosis-like lesion in the development of the pseudoaneurysm adds a layer of uniqueness to the presented case. In this case, our differential diagnosis for the exostosis-like lesion included osteophyte, avulsion fracture, enostosis, or osteochondroma. Image findings and final pathology reported necrotic bone and marrow. One possible cause of the bony fragment is the devitalization of the segment of cortical bone after a posttraumatic periosteal injury. Bony outgrowths are more commonly associated with joint degeneration and nerve pain8,9 rather than vascular conditions. However, previous studies examined bony outgrowths affecting blood flow in the vertebral arteries and aortic arteries. 2 This case examines the bony outgrowth in relation to the SFA. The bone growth likely acted as a mechanical irritant, perforating the adjacent SFA during the initial traumatic event, the semimembranosus tear, leading to the pseudoaneurysm formation. Previous case reports have looked more at repeated minor traumas causing the aortic pseudoaneurysm. 2
In the presented case, the exostosis-like lesion is suspected to have played a role in the development of the pseudoaneurysm, with the location adjacent to the SFA being noteworthy. Unlike the more common associations with bony outgrowths, such as joint degeneration and nerve pain,8,9 this instance involves a direct mechanical interaction between the devitalized bone and the arterial wall. Previous case reports examined bony outgrowths affecting blood flow in the aortic arteries along with perforation of the artery due to repeated minor trauma, 2 but this case examines the bony outgrowth in relation to the SFA. In our case, the single traumatic event, the semimembranosus tear, allowed the bony outgrowth to perforate the SFA, an area in which there is less research. Overall, this case highlights the importance of considering atypical mechanisms and locations in the pathogenesis of pseudoaneurysms, especially in the context of traumatic injuries involving adjacent bony structures.
Conclusion
This case is noteworthy for a number of reasons. This patient had an acute injury involving a hamstring tear of the semimembranosus at the same time as a traumatic arterial injury from a devitalized bone growth on the femur. The hamstring tear certainly clouded the clinical picture and ability to initially diagnose the pseudoaneurysm. Additionally, the unique nature of the devitalized bone growth inducing mechanical trauma leading to the vascular injury as opposed to the more commonly discussed iatrogenic 3 and femoral fracture 6 causes. Fortunately, our team decided to obtain a vascular study before potentially evacuating the hematoma, which was the diagnostic step that discovered the pseudoaneurysm. Ultimately, to restore proper blood flow, vascular surgery was required using a segment of the saphenous vein.
Footnotes
Final revision submitted May 14, 2025; accepted July 1, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.