
Abstract
Background:
Panner disease is a condition characterized by osteochondrosis of the humeral capitellum. Because of its rarity, clinical outcomes, including return to sports, have not been well described in previous studies.
Purpose:
To investigate the clinical and radiographic outcomes after nonoperative treatment of elbows affected by Panner disease.
Study Design:
Case series; Level of evidence, 4.
Methods:
The inclusion criteria for this study were as follows: (1) elbows diagnosed with Panner disease between January 2007 and March 2021, and (2) elbows in patients who were followed until clinical and radiographic healing was confirmed. Patient background (sports participation, familial smoking, steroid use, and bone age), symptoms, radiographic findings, and outcomes after nonoperative treatment were analyzed.
Results:
Seven elbows in 7 patients (5 boys and 2 girls; 4 gymnasts and 3 baseball players) were included. The mean age at the initial examination was 10 years (range, 7-11 years), and bone age was younger than the chronological age in 3 patients (43%). All patients were treated nonoperatively with a mean follow-up of 37 months (range, 14-109 months). At the initial examination, all patients experienced elbow pain, and a limited range of motion was observed in 4 patients (57%). Familial smoking was reported in 2 patients (29%), and steroid use in 1 patient (14%). After a mean of 7 months (range, 2-15 months) of overhead motion restriction and cessation of upper extremity loading, all patients returned to sports at a mean of 15 months (range, 10-24 months). Complete healing of the epiphyseal nucleus of the capitellum was observed at a mean of 12 months (range, 10-15 months).
Conclusion:
Nonoperative treatment for Panner disease resulted in favorable outcomes in 7 patients. All patients fully returned to sports with well-remodeled capitella.
Panner disease was first described in 1927 by Panner 8 as a necrotizing lesion of the ossification center of the capitellum. In 1960, Heller and Wiltse 5 redefined the lesion as an osteochondrosis of the humeral capitellum. Because of its rarity compared with osteochondritis dissecans of the capitellum, Panner disease has been predominantly reported as case reports. 3
The diagnosis of Panner disease is often challenging in its early stages. It is typically established through a comprehensive evaluation of patient history, clinical presentation, and imaging findings, including radiographs and magnetic resonance imaging (MRI).3,10 Most reported cases of Panner disease occur in boys, particularly those engaged in overhead sports, with onset typically in the unilateral elbow within the first 10 years of life.3,10 The primary symptoms include elbow pain and a limited range of motion (ROM).3,10 The radiographic findings of Panner disease closely resemble those of capitellar osteochondritis dissecans; however, in Panner disease, the entire capitellum is often affected. MRI findings typically demonstrate homogeneously decreased signal intensity in the entire capitellum.3,10
According to a literature review by Claessen et al, 3 nonoperative treatment is generally recommended. Panner disease is a self-limiting condition, and an excellent prognosis after nonoperative management has been reported. 3 However, a single case requiring arthroscopic debridement has been documented. 1 Rest and activity modification are usually necessary. Because most reported cases of Panner disease occur in baseball, gymnastics, or handball athletes, repetitive microtrauma to the capitellum during sports is considered a contributing factor.3,10 To reduce mechanical stress during overhead sports, we apply physical therapy interventions aimed at improving scapular dyskinesis and hip joint tightness based on physical evaluation. 10 However, treatment strategies, prognosis, and the relationship between Panner disease and sports activity remain unclear. Moreover, the timing of diagnosis and return to sports in patients with Panner disease has not been well described.
This study aimed to investigate the clinical and radiographic outcomes after nonoperative treatment of elbows affected by Panner disease. We hypothesized that nonoperative management would yield satisfactory clinical and radiographic outcomes.
Methods
Patients
The institutional review board of Funabashi Orthopaedic Hospital approved this retrospective study protocol (No. 2020056). The inclusion criteria for this study were as follows: (1) elbows diagnosed with Panner disease that underwent nonoperative treatment at our institution between January 2007 and March 2021, and (2) elbows that were followed until either return to sports activities or resolution of symptoms. The diagnosis of Panner disease was established based on radiographic findings and clinical features.
All patients were treated by 1 of 2 senior surgeons (H.S. and S.H.). Daily activities were permitted as long as they did not provoke pain in the elbow. Patients were restricted from overhead and weightbearing activities until pain subsided and ROM was restored. The importance of temporary cessation from sports activities was thoroughly explained to patients and their parents to ensure compliance. Physical therapy was initiated at the first clinical visit to improve elbow ROM, scapular function, and hip joint mobility. 10 Based on functional recovery and capitellar remodeling, patients were allowed to return to sports activities; the full return to sports activity was allowed when the ROM was fully restored and the capitellum was completely remodeled. 10 We did not immobilize elbows using a sling or brace during treatment. Full return to sports was permitted after complete recovery of the epiphyseal nucleus of the capitellum. 11
Clinical Evaluation
Medical records were reviewed to assess passive ROM in flexion and extension at the initial visit and final follow-up. Physical examinations were performed by 1 of 2 senior surgeons (S.H. and Y.U.). Patient background information, including exposure to passive smoking, history of steroid use, and participation in sports activities, was also collected.
Radiographic Evaluation
Patients underwent anteroposterior, tangential (45° elbow flexion), and lateral radiographic imaging of the elbow at the initial visit and every 2 months until complete remodeling of the capitellum was observed. These radiographs were also obtained at the final follow-up. MRI using a 1.5-T imager (Intera 1.5T; Philips) with a phased-array surface coil was performed at the second visit if the patient consented. Bone age was assessed using the classification by Cheng et al. 2
Statistical Analysis
The Mann-Whitney U test was used to compare preoperative and postoperative ranges of motion. Statistical analyses were conducted using R Version 3.1.0 (R Foundation for Statistical Computing; http://www.R-project.org/). The level of significance was set at a P value <.05.
Result
Patients
Between January 2007 and March 2021, 7 elbows with Panner disease in 7 patients were treated nonoperatively. No patients with Panner disease underwent surgical treatment during this period. The dominant elbows were affected in all patients (Table 1). The cohort consisted of 5 boys and 2 girls, with a mean age of 10 years (range, 7-11 years). All patients returned to sports. The patients were restricted from overhead and weightbearing activities for a mean of 7 months (range, 2-15 months), and capitellar remodeling was achieved with a mean follow-up of 37 months (range, 14-109 months). At the initial visit, all patients experienced motion pain in the elbow, and 4 patients (57%) exhibited a limited ROM. No patient had a history of traumatic injury. The diagnosis of Panner disease was established based on physical examination and radiographic findings, with a mean diagnostic delay of 2 months (range, 0-4 months) after the onset of elbow pain. Parental smoking was reported in 2 patients (29%), and steroid use was noted in 1 patient (14%). All patients participated in sports activities, including gymnastics (4 patients) and baseball (3 patients).
Patient Characteristics a

F, female; M, male.
Radiographic Evaluation
Focal radiolucency was observed in all patients at the initial visit. The mean bone age at the initial visit was 9 years (range, 7-11 years). Delayed ossification was identified in 3 patients (43%). After nonoperative therapy with restriction of sports activities, segmentation was most evident at a mean of 5 months (range, 3-7 months) after the initial visit. Sclerosis was observed at a mean of 12 months (range, 10-16 months) after the initial visit (Figure 1). The epiphyseal nucleus of the capitellum was restored at a mean of 12 months (range, 10-15 months). No elbows exhibited deformity or osteoarthritic changes at the final follow-up.

Images obtained in a 9-year-old baseball player with Panner disease (case 2). (A) Tangential view of the right elbow at the initial visit, showing focal radiolucency in the capitellum. (B) Six months after the initial visit, segmentation of the capitellum was observed. (C) One year after the initial visit, the capitellum was remodeled. (D) Nine years after the initial visit, no osteoarthritic changes were observed in the elbow.
MRI scans were obtained in 6 patients (86%). All elbows demonstrated low signal intensity in the entire epiphyseal region of the capitellum on both T1- and T2-weighted images (Figure 2). Subsequent MRI scans were obtained in case 2 at 43 months and case 5 at 8 months after the initial MRI scans. The capitellum of the 2 patients showed normal signal intensity on both T1- and T2-weighted images (Figure 3).
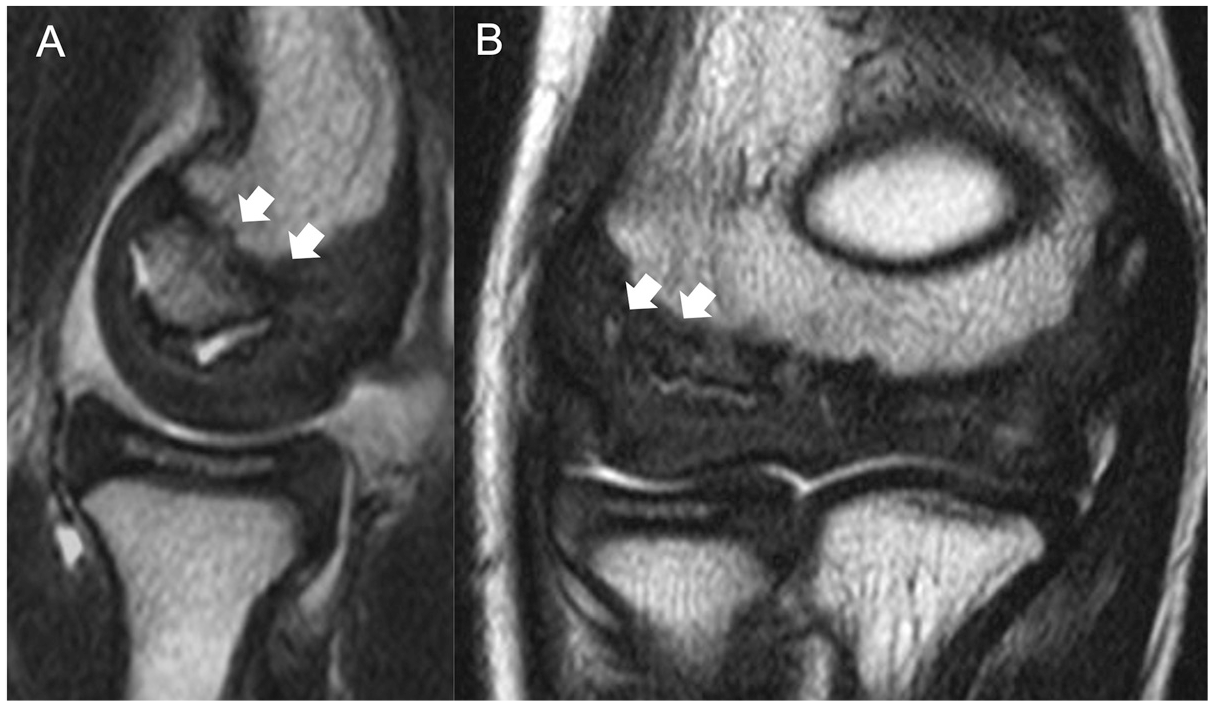
T2-weighted magnetic resonance imaging scans of the right elbow obtained in a 9-year-old baseball player with Panner disease (case 2). (A) Sagittal and (B) coronal images demonstrate homogeneous low signal intensity (arrows) throughout the entire capitellum with intact cartilage.

T2-weighted magnetic resonance imaging (MRI) scans of the right elbow obtained in case 2 (43 months after the initial MRI). Sagittal (A) and coronal (B) images demonstrate normal signal intensity (arrows) in the capitellum.
Clinical Outcomes
All 7 patients returned to sports at a mean of 15 months (range, 10-24 months) after the initial visit (Table 2). Both flexion and extension at the final follow-up were significantly improved relative to the initial visit (flexion, P = .04; extension, P = .02).
Clinical and Radiographic Outcomes

Discussion
This study demonstrated that complete clinical and radiographic recovery was achieved in all 7 elbows with Panner disease after nonoperative treatment. The epiphyseal nucleus of the capitellum was fully restored at a mean of 12 months after treatment. All patients returned to sports at a mean of 15 months. All patients participated in gymnastics or baseball and successfully resumed sports activities. The mean age at the initial visit was 10 years, and bone age was younger than chronological age in 43% of patients. The findings of this study support our hypothesis.
Consistent with previous literature,3,9 the cases in this study exhibited excellent healing with nonoperative management without the need for elbow immobilization. Surgical intervention will be indicated in cases refractory to nonoperative management, particularly when severe inflammation or intra-articular loose bodies are present in the elbow joint.1,3,9 Additionally, the recovery timeline was shorter than that reported in previous studies.3,9 The epiphyseal nucleus of the capitellum was fully restored within 12 months, and all patients returned to sports within 15 months. Previous studies have indicated that recovery typically requires 18 to 24 months.3,9 Early intervention and targeted rehabilitation, including the improvement of scapular and hip joint function, may have contributed to the improved outcomes. 10
A review of 30 patients with Panner disease reported that the dominant arm was involved in all cases and that the majority of patients participated in sports requiring throwing or weightbearing on the upper extremities, such as baseball, handball, and gymnastics. 3 Similarly, all patients in this study were involved in gymnastics or baseball. Microtrauma due to repetitive stress on the elbow joint from throwing or weightbearing activities may be associated with the development of Panner disease. 10 A previous study suggested that excessive loading on the immature capitellum can lead to vascular insufficiency and subsequent osteonecrosis. 3
Several possible factors related to the cause of Panner disease have been proposed. Passive smoking may contribute to thrombus formation in the blood vessels surrounding the epiphyseal nucleus, similar to its role in Legg-Calvé-Perthes disease. 4 Steroid use may also be a risk factor for Panner disease due to its potential to induce thrombus formation in blood vessels. 6 Kitoh et al 7 suggested an association between Legg-Calvé-Perthes disease and delayed maturation of the femoral epiphyseal nucleus. In this study, passive smoking and steroid use were reported in 29% and 14% of patients, respectively. Delayed maturation was observed in 43% of patients. These factors might be associated with the onset of Panner disease; however, establishing definitive risk factors remains challenging given the small sample size.
Limitations
This study has several limitations. First, it is a retrospective case series, and no comparisons were made between treatment options. Second, the small sample size may limit the statistical power of the findings. Because of the rarity of the disease, collecting a large patient cohort is challenging. Lastly, follow-up duration varied considerably among patients (range, 14-109 months), which may have influenced the study outcomes.
Conclusion
Nonoperative treatment for Panner disease resulted in favorable outcomes in 7 patients. All patients fully returned to sports with well-remodeled capitella.
Footnotes
Correction (October 2025):
This article has been updated to correct the range for complete healing of the epiphyseal nucleus of the capitellum to 10-15 months.
Final revision submitted May 16, 2025; accepted June 16, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Funabashi Orthopaedic Hospital (No. 2020056).