
Abstract
Background:
An all-inside lateral meniscus repair in relation to the popliteus tendon is still challenging in arthroscopic surgery, with a high rate of failure as the joint capsule is quite thin, often leading to insecure meniscal repairs. To reduce the rate of failure, vertical suturing has been suggested, but there is still a chance of iatrogenic peroneal nerve injury because the peroneal nerve is located close to the joint capsule and the popliteus tendon.
Purpose:
To evaluate the risk of iatrogenic peroneal nerve injury in all-inside meniscal repair with a vertical stitch, comparing between 90° and 120° of knee flexion, using full-body fresh-frozen cadavers.
Study Design:
Descriptive laboratory study.
Methods:
The study used 15 cadavers, 8 male and 7 female. A straight all-inside meniscal repair device with a 20-mm penetration depth was used for the meniscal repairs, randomized into repairs of the lateral meniscus penetrating the meniscus at the peripheral and inner one-third of the medial and lateral borders of the popliteus tendon in 2 knee positions. The shortest distance from the tip to the peroneal nerve was measured, and the measurements were compared between repairs in 2 knee positions.
Results:
In simulated cadaveric repair, there was a chance of iatrogenic peroneal nerve injury with vertical stitch deployment at the inner one-third of the medial border of the popliteus tendon, with injury incidences of 10% and 6.7% in 90° and 120° of knee flexion, respectively. The mean shortest distances related to the medial borders of the popliteus tendon in 90° of knee flexion were statistically significantly shorter than those with the knee in 120° of flexion.
Conclusion:
Vertical stitching at the lateral border of the popliteus tendon maintained a safe distance from the peroneal nerve. However, a small risk of iatrogenic injury remained at the inner one-third of the medial border.
Clinical Relevance:
The surgeon should avoid penetrating the lateral meniscus at the inner one-third of the medial border of the popliteus tendon, but if a repair must be done in this area, the surgeon should position the knee at 120° of knee flexion.
An all-inside lateral meniscus repair is still challenging in arthroscopic surgery, with a high rate of failure as the joint capsule is quite thin, leading to insecure meniscal repairs. The incidence of failure in earlier studies was found to be from 16% to 19.5%.11,14,15 There have been some recommendations to reduce the risk of repair failure with an all-inside technique. First, vertical suturing was recommended due to better results in biomechanical testing7,13 and a lower failure rate 1 with this method compared with the common horizontal suturing. Second, avoiding repairing through the popliteus tendon has been recommended because the suture is stressed when the knee is moved in the flexion-extension direction, leading to an increased risk of failure. 12 Third, inserting the all-inside meniscal repair device through an anteromedial portal may help reduce repair failure because the direction of the device from this portal will be perpendicular to the fibers of the lateral meniscus tissue, which will decrease joint capsule trauma.2,8
By following these recommendations and repairing the posterior horn of the lateral meniscus tissue with a vertical stitch, the all-inside meniscal repair device can be inserted through an anteromedial portal and deployed in 3 possible ways at either the medial or lateral border of the popliteus tendon (Figure 1). There will be a risk of iatrogenic peroneal nerve injury in repairing the lateral meniscus at either the peripheral and inner deployment holes, which will be different between repairs in relation to the medial border and the lateral border of the popliteus tendon, because the peroneal nerve is located close to the popliteus tendon and joint capsule, where the popliteus tendon passes the knee joint in an oblique direction. 6
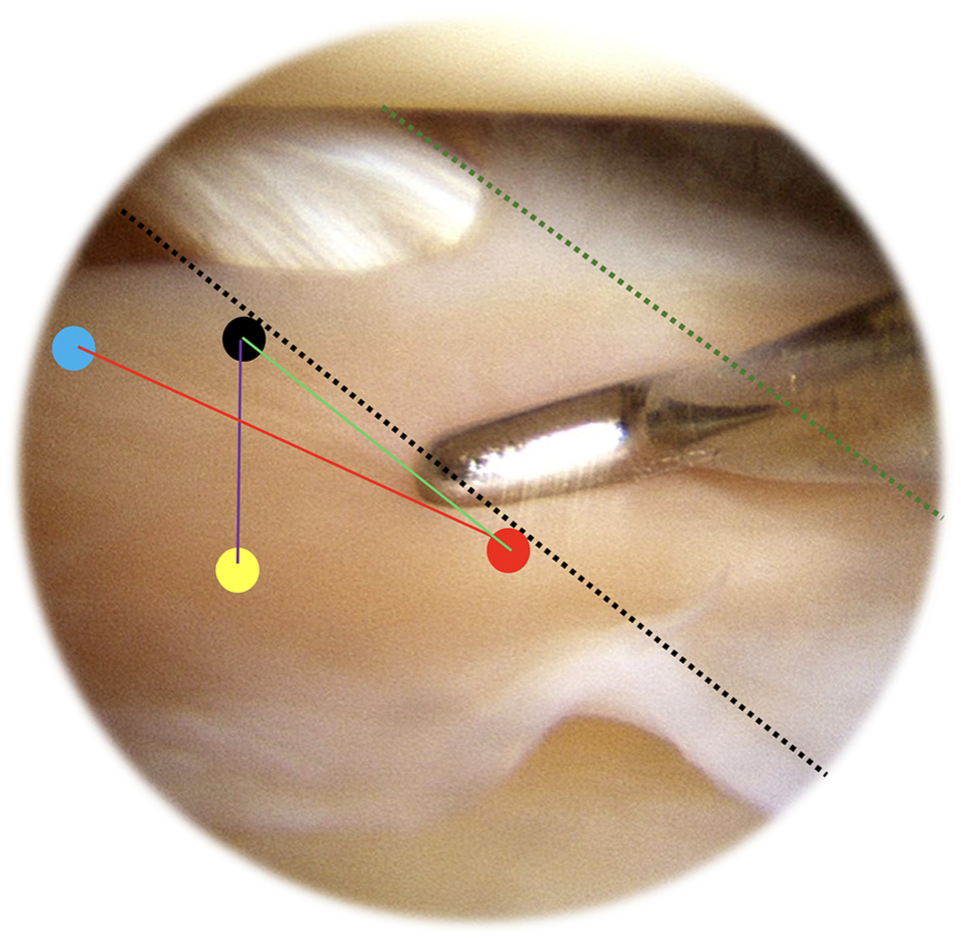
Arthroscopic view from an anterolateral portal of a right knee showing the 3 standard patterns (green, red, and purple lines) of vertical stitch, with penetrating sites located at the peripheral distal (caudad) one-third (black circle), inner distal (caudad) one-third (red circle), peripheral proximal (cephalad) one-third (light blue circle), and inner proximal (cephalad) one-third (yellow circle) along the lateral border of the popliteus tendon (black dotted line). Green dotted line indicates the medial border of the popliteus tendon.
To our knowledge, there have been no studies evaluating the chance of iatrogenic peroneal nerve injury in all-inside lateral meniscus repair with a vertical stitch using an all-inside meniscal repair device at the medial or lateral borders of the popliteus tendon using fresh-frozen full-body cadavers placed in 90° and 120° of knee flexion. In this study, we evaluated and compared the chance of iatrogenic peroneal nerve injury in all-inside lateral meniscus repair through the anteromedial portal by penetrating the lateral meniscus at the peripheral one-third and inner one-third of the medial and lateral borders of the popliteus tendon in both 90° and 120° of knee flexion using fresh-frozen full-body cadavers. On the basis of 2 existing studies,5,10 we hypothesized that suturing the lateral meniscus in 90° of knee flexion would have a higher risk of iatrogenic common peroneal nerve injury in lateral meniscus repair than in 120° of knee flexion, and vertical suturing in each penetrating site would have a different risk of iatrogenic peroneal nerve injury.
Methods
This study received approval from the institutional review board of the Faculty of Medicine of Prince of Songkla University and used 15 full-body fresh-frozen cadavers (8 male, 7 female) obtained from the Department of Anatomy, Faculty of Science of Prince of Songkla University. The mean age of death was 68.53 ± 8.53 years, and the mean height was 165.6 ± 7.07 cm.
Each cadaveric dissection began with the Henderson posterolateral approach 9 to identify the common peroneal nerve. A 6-cm curved incision was made along the interval between the iliotibial band and the biceps femoris tendon. The skin, subcutaneous tissue, and fascia were carefully dissected, centered over the fibular head. The iliotibial band was then gently retracted anteriorly to expose the common peroneal nerve. Then anteromedial and high anterolateral portals were created for a working portal at 5 mm from the medial edge of the patellar tendon and a viewing portal beside the lateral edge of the patellar tendon, respectively. The prepatellar fat pad and any obstructive soft tissue were removed using a shaver to improve visualization and access. A straight all-inside meniscal repair device (FAST-FIX 360; Smith & Nephew) with a 20-mm penetration depth was used to penetrate the lateral meniscus tissue from the anteromedial portal. There were 4 penetration sites, the peripheral one-third and inner one-third of the medial border of the popliteus tendon and the peripheral one-third and inner one-third of the lateral border of the popliteus tendon (Figure 2). Two knee positions were compared, 90° and 120° of knee flexion. The sequence of choosing location sites and knee positions was randomized by the block-of-4 technique.
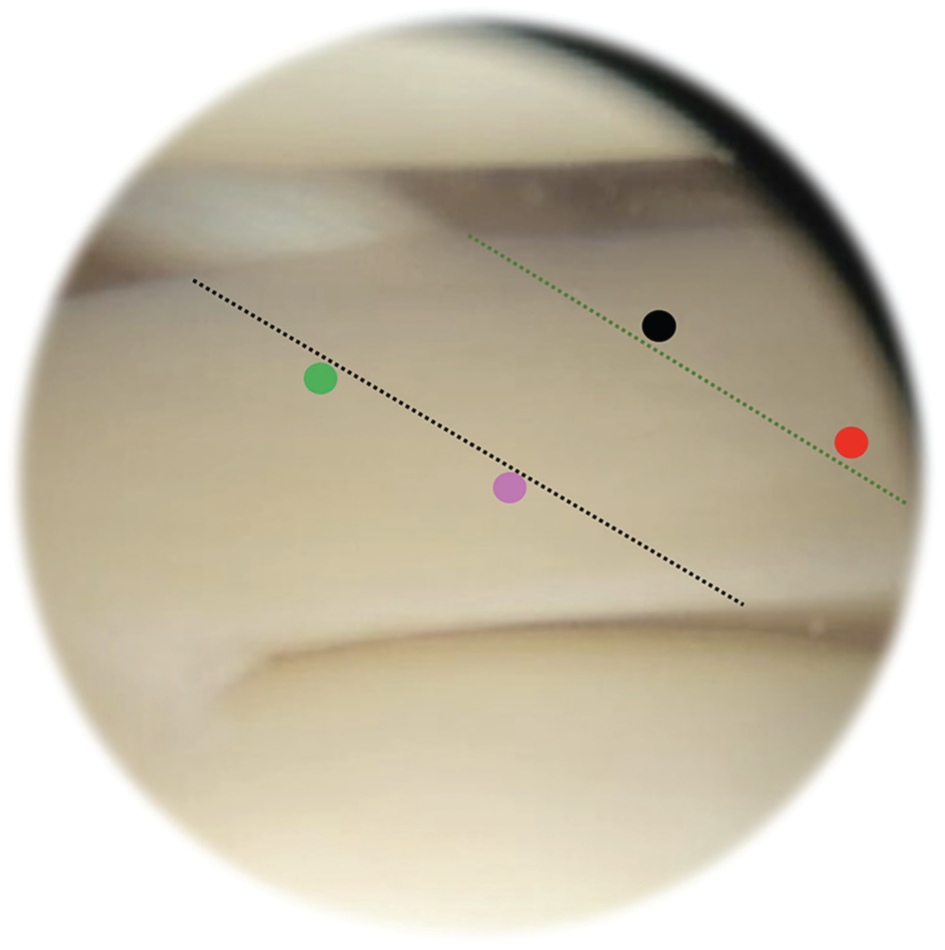
Arthroscopic view from the anterolateral portal of a right knee showing the lateral meniscus and popliteus tendon (outlined with black and green dotted lines) with the 4 penetration sites at the peripheral one-third (black circle) and inner one-third (red circle) of the medial border of the popliteus tendon and the peripheral one-third (green circle) and inner one-third (purple circle) of the lateral border of the popliteus tendon.
Measurements
After penetrating the lateral meniscus, if the tip of the straight all-inside meniscal repair device touched or penetrated the peroneal nerve, it was deemed as an incidence of iatrogenic peroneal nerve injury. If the tip did not touch or penetrate the peroneal nerve, the distance from the tip to the peroneal nerve was measured using a digital vernier caliper with a precision of 0.01 mm (Figure 3).

Shortest distance between the tip of the all-inside meniscal repair device and the peroneal nerve.
Statistical Analysis
All distances were measured 3 times by both an experienced sports medicine specialist (W.P.) and an orthopaedist-in-training (S.C.). To evaluate interobserver and intraobserver reliability, kappa values and intraclass correlation coefficients were calculated for categorical and continuous data, respectively. The results are reported using descriptive statistics (mean ± standard deviation) and incidence risk ratios. Statistical analyses were conducted using R software (Version 3.4.3; R Foundation for Statistical Computing) and the epicalc package. The statistical significances of the risks associated with iatrogenic peroneal nerve damage were determined using the chi-square test for independence and associations, considering a P value <.05 as statistically significant.
Results
Incidence of Iatrogenic Peroneal Nerve Injury
There were no instances of peroneal nerve penetration when inserting the straight all-inside meniscal repair device through the anteromedial portal and penetrating for deployment of the vertical stitch at either the peripheral one-third or inner one-third of the lateral border or the peripheral one-third of the medial border of the popliteus tendon in both 90° and 120° of knee flexion. However, there were instances of nerve penetration of iatrogenic peroneal nerve injury when inserting the device through the anteromedial portal and deploying the stitch at the inner one-third of the medial border of the popliteus tendon in both 90° and 120° of knee flexion, which were 3 of 30 (10.0%) and 2 of 30 (6.7%), respectively.
Shortest Distance From Tip of All-Inside Meniscal Repair Device to Common Peroneal Nerve
The shortest distances from the tip of the straight all-inside meniscal repair device to the common peroneal nerve during repair through the anteromedial portal at 90° of knee flexion were 30.2 ± 11.8 mm at the peripheral one-third and 21.0 ± 17.2 mm at the inner one-third of the medial border of the popliteus tendon. At 120° of knee flexion, these distances increased to 38.1 ± 23.6 mm and 27.4 ± 16.4 mm, respectively. The distances at 90° were significantly shorter than those at 120° for both measurement points (P = .022 and P = .038, respectively). However, no statistically significant differences were observed when comparing measurements taken at the peripheral and inner one-third of the lateral border of the popliteus tendon (Table 1).
Shortest Distances From Tip of Straight All-Inside Meniscal Repair Device to Common Peroneal Nerve in Repairing through Anteromedial Portal in 90° and 120° of Knee Flexion a

Data are presented as mean ± SD unless otherwise indicated. Bold P values indicate statistical significance (P < .05).
The intraobserver reliability and interobserver reliability for all measurements were 0.98 to 0.99 and 0.91, respectively.
Discussion
Our study found that repairing the lateral meniscus using a vertical stitch through the anteromedial portal at both the peripheral one-third and inner one-third of the lateral border, as well as deploying the upper stitch at the peripheral one-third of the medial border of the popliteus tendon, was associated with a lower likelihood of peroneal nerve penetration, based on the measured distances from the nerve in both 90° and 120° of knee flexion. However, there was a risk of peroneal nerve penetration when penetrating the meniscus at the inner one-third of the medial border of the popliteus tendon, with observed nerve penetration rates of 10% and 6.7% at 90° and 120° of knee flexion, respectively.
A lateral meniscus repair with a meniscal repair device involves a chance of iatrogenic peroneal nerve injury because this structure is located close to the lateral joint capsule and popliteus tendon. 6 There have been some recent studies based on cadavers and magnetic resonance imaging (MRI) to evaluate the risk of iatrogenic peroneal nerve injury during a lateral meniscus repair. Cuéllar et al 5 evaluated the risk of peroneal nerve injury when doing all-inside lateral meniscus repairs using midthigh to midleg cadavers. They inserted the all-inside meniscal repair device at the most medial and lateral corners of the popliteal hiatus. They found that there was no risk of iatrogenic peroneal nerve injury when performing repairs related to the medial and lateral borders of the popliteus tendon, and that the distances between the tip of an all-inside meniscal repair device and the peroneal nerve increased with higher degrees of knee flexion. Chuaychoosakoon et al3,4 conducted 2 complementary MRI investigations. In the first, 4 they overlaid straight, all-inside device trajectories from anteromedial and anterolateral portals across both borders of the popliteus tendon on standard knee MRI scans, revealing that each trajectory entered the peroneal nerve danger zone. A follow-up study 3 repeated these measurements with the knee in a figure-of-4 position under varus stress and joint distension, confirming persistent risk when the anteromedial portal crossed the medial border and the anterolateral portal crossed the lateral border of the popliteus tendon. All these studies used 1 insertion point at each of the medial and lateral borders of the popliteus tendon, that is, the horizontal stitching technique. As we know, use of this technique for repair at the posterior horn of the lateral meniscus has a high chance of failure because the joint capsule is thin and, in this area, separate from the meniscal tissue, with reported failure rates of between 16% and 19.5%.11,14,15 To decrease the chance of failure, a vertical stitch has been recommended for repairs around the lateral meniscus tissue,1,7,13 which our study found was mostly safe, but with a small risk of iatrogenic peroneal nerve injury in penetrations at the inner one-third of the medial border of the popliteus tendon. Furthermore, some surgeons prefer using the all-inside technique for lateral meniscus repair.
The site of penetration is not the only factor affecting the risk of peroneal nerve injury, as the knee position can also affect the risk of injury. Three studies found that the proximity of the neurovascular components to the posterior tibial cortex, edges of the popliteus tendon, and the nearest approach of the shaver to these structures varied with greater knee flexion. Our study evaluated the risk of peroneal nerve injury with repairs using a vertical stitch in relation to both the medial and lateral borders of the popliteus tendon using a straight all-inside meniscal repair device with 20 mm of penetration depth in both 90° and 120° of knee flexion.
Based on our findings, to avoid the chance of iatrogenic peroneal nerve injury when doing a lateral meniscus repair using a vertical stitch, we recommend performing the repair in the area lateral to the lateral border of the popliteus tendon in either 90° or 120° of knee flexion, both of which had no risk of injury in our study. In repairs in the area medial to the medial border of the popliteus tendon, there was a risk in penetrating the lateral meniscus at the inner one-third of the medial border of the popliteus tendon. We recommend avoiding repairs in this area, but if a repair must be done here, we suggest positioning the knee at 120° of flexion to ensure the peroneal nerve is at the farthest possible distance from the inner one-third hole of the vertical stitch deployment.
Limitations
This study had some limitations. First, we used a straight all-inside meniscal repair device for repairing the lateral meniscus to decrease the chance of measurement variations from the curvature of a curved all-inside meniscal repair device. When using a curved or reverse-curve all-inside meniscal repair device, the risk of injury might be different. Second, we created the anteromedial portal at 5 mm medial to the medial border of the patellar tendon. If the anteromedial portal is created at a different distance, the surgeon should use the results from this study with caution.
Conclusion
Vertical suture placement in all-inside lateral meniscus repair was associated with a greater mean distance from the peroneal nerve when the repair device was deployed at the peripheral one-third of the medial border and at both the peripheral and inner one-third of the lateral border of the popliteus tendon. Conversely, suture deployment at the inner one-third of the medial border of the popliteus tendon resulted in reduced distances from the peroneal nerve and a measurable incidence of iatrogenic nerve contact. Although this risk was present at both 90° and 120° of knee flexion, greater knee flexion (120°) was associated with increased distances from the nerve, thereby reducing the likelihood of nerve injury. Based on these findings, suture placement at the inner one-third of the medial border of the popliteus tendon should be avoided when feasible; however, if necessary, the knee should be positioned at 120° of flexion to increase the distance from the peroneal nerve and mitigate the risk of iatrogenic injury.
Footnotes
Acknowledgements
The authors sincerely thank Boonsin Tangtrakulwanich of the Department of Orthopedics, Faculty of Medicine of Prince of Songkla University, and Jirawan Jayuphan of the Epidemiology Unit, Faculty of Medicine of Prince of Songkla University, for providing statistical support; and Dave Patterson for his editing support. The study also received conceptual support by the Thai Orthopedic Society for Sports Medicine.
Final revision submitted May 10, 2025; accepted June 5, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Prince of Songkla University (REC 63-378-11-1). This study was supported by a research grant from the Faculty of Medicine, Prince of Songkla University.