
Abstract
Background:
Concomitant anterior cruciate ligament (ACL) and medial collateral ligament (MCL) injuries are among the most commonly reported injury patterns in high-energy knee injuries. Concomitant ACL and MCL reconstruction (ACLR + MCLR) is indicated in patients with full-thickness tears and persistent valgus laxity.
Purpose:
To systematically review the literature to identify studies reporting on patients undergoing concurrent primary ACLR + MCLR to better understand current indications, surgical techniques, complications, and outcomes.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Under the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, 702 studies published in PubMed, EMBASE, and the Cochrane Library reporting on patients undergoing ACLR + MCLR from inception to April 2025 were initially identified. The inclusion criteria included studies reporting on human subjects undergoing ACLR + MCLR with injury mechanism, tear characteristics, surgical technique, graft types used for reconstruction, complications, and postoperative outcomes. Incidence rates for variables of interest were pooled as proportions with inverse variance weighting and displayed in forest plots, with heterogeneity of included studies assessed using the I 2 statistic.
Results:
Seventeen studies, including 902 patients undergoing concurrent ACLR + MCLR, with a mean follow-up of 30.6 months (range, 15-61 months), were identified. The weighted mean patient age was 32.9 years (range, 14-74 years), and 68.4% (n = 471/689) of patients were men. Sports-related traumatic knee injuries accounted for 51.3% (n = 309/602) of injuries, while motor vehicular accidents comprised 12.1% (n = 73/602). Reported indications for MCLR in the setting of ACL injury were chronic (≥6 weeks) valgus knee laxity despite nonoperative management (81.5%, n = 667/818) and grade 3 MCL injury (22.2%, n = 182/818). Autografts were utilized in 69.7% (n = 265/380) of ACLR and 61.1% (n = 140/262) of MCLR procedures, while anterior tibialis allografts (28.4%; n = 108/380) and hamstring tendon autografts (53.4%; n = 140/262) were the most frequently reported graft types in ACLR and MCLR, respectively. Complications were reported in 14 cases, including persistent medial knee pain (n = 7) and reconstruction failure (MCLR, n = 1; ACLR, n = 2). Mean Lysholm scores improved from 55.9 to 87.6, while mean Tegner and subjective International Knee Documentation Committee (IKDC) scores improved from 3.1 to 4.8 and 46.5 to 88.5, respectively.
Conclusions:
Our review revealed that concomitant ACLR + MCLR is most commonly performed for injuries sustained during pivoting sports, which result in persistent valgus laxity. Autografts were used in 70% of ACLR and 61% of MCLR procedures. Improvements in Lysholm, Tegner, and IKDC scores were noted in the majority of patients with a low incidence of complications (7.9%) and reconstruction failures (1.7%). These findings may enhance the understanding of proper surgical indications and methodology, thereby optimizing treatments and postoperative outcomes.
Keywords
Concomitant injury to the anterior cruciate ligament (ACL) and medial collateral ligament (MCL) represents the most common form of multiligament knee injury, with a reported 20% to 38% of ACL injuries accompanied by a concurrent MCL injury. 56 While the ACL is the primary restraint to anterior tibial translation and internal rotation, rupture is associated with anterior laxity and increased risk for injury to the menisci and articular cartilage.5,9,12,36 The MCL serves as the primary restraint against valgus stress and is a secondary stabilizer to anterior tibial translation.5,35,45 According to the Hughston classification,35,44 grade 1 MCL injuries consist of localized tenderness with a firm endpoint to valgus stress and no joint laxity; grade 2 injury consists of generalized tenderness, a firm endpoint, and minimal laxity; while grade 3 injuries possess no endpoint to valgus stress with associated joint laxity.
ACL rupture is associated with 95% of grade 3 MCL injuries,11,32 often requiring surgical intervention to restore stability and function in active patients. 55 In the setting of ACL injuries, partial MCL tears (grade 1 or 2) are generally treated nonoperatively with bracing, physical therapy, and delayed ACL reconstruction (ACLR) for a duration based on the degree of MCL injury. 55 However, in the setting of concomitant ACL and MCL rupture, partial MCL deficiency has been shown to significantly decrease the success of ACLR due to increased strain on the ACL graft. 55 ACL injuries with grades 2 and 3 MCL tears that fail nonoperative modalities, along with distal MCL tears that are displaced superficial to the pes anserine tendons or folded into the joint under the medial meniscus, are treated operatively through either ligament repair, reconstruction, or a hybrid of both surgical options.4,55
While previous investigations have reported successful management of concurrent grade 3 MCL injuries using bracing,16,46,55,57 other studies have advocated for operative intervention.3,48,56 In such cases, MCL reconstruction (MCLR) in patients with ACL tears has been shown to provide a more stable construct with improved overall outcomes compared with ACLR alone or MCL repair. 36 MCLR is indicated in cases of chronic valgus laxity, failure of nonoperative treatment, and/or previous repair, and in competitive athletes25,53 to achieve a faster return to sport.
There is a lack of consensus regarding the optimal treatment for patients with combined ACL and high-grade MCL tears. Few studies report outcomes after combined ACLR and MCLR, as well as specific indications for MCLR.7,28 Therefore, this study aimed to systematically review the literature and identify studies reporting on patients undergoing concurrent primary ACLR + MCLR to better understand the current indications, graft types, surgical techniques, surgical timing (both acute and delayed reconstruction), postoperative complications, and outcomes after this combined procedure. We hypothesized that MCLR in patients with persistent or severe valgus knee laxity in the setting of an ACL tear would be associated with a low prevalence of complications and favorable postoperative outcomes.
Methods
Search Strategy and Eligibility Criteria
A systematic review was conducted according to the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 42 A literature search identifying studies reporting on clinical outcomes in patients with ACL and MCL injuries undergoing concurrent primary ACLR + MCLR was conducted on April 14, 2025. Two authors (D.C.T. and F.N.G.) independently conducted a systematic review of the current literature utilizing PubMed, Cochrane Database for Systematic Review, Cochrane Central Register for Controlled Trials, and Embase databases from inception to April 2025. The search was performed using the following search terms: “anterior cruciate ligament,” “medial collateral ligament,” “reconstruction,” “knee,” “multiligament injury,” “posterior medial corner,” “complications,” and “outcomes.”
The inclusion criteria consisted of studies written in English or with English-language translation reporting concurrent, primary ALCR + MCLR with reported injury causes (eg, sports, traffic accident, etc), symptom characteristics (eg, knee pain, instability), diagnostic modalities and findings, surgical indications (eg, distal MCL tears, chronic valgus knee laxity ≥6 weeks, acute reconstruction for a faster return to sports), surgical techniques, graft types used for ACLR + MCLR, incidence of any postoperative complications, and any patient-reported outcomes. The exclusion criteria included cadaveric, biomechanical, and animal studies; case reports; previous systematic reviews and meta-analyses; review articles; and editorial commentaries. Studies that comprised patients undergoing revision ACLR, staged ACLR followed by MCLR, ACL or MCL repair, or patients with concomitant posterior cruciate ligament (PCL) or posterolateral corner (PLC) injuries undergoing PCL or PLC repair or reconstruction were also excluded. Given the high rate of concomitant meniscal and chondral injuries in the setting of ACL + MCL injuries, patients with reported meniscal and/or chondral pathology were not excluded from analysis.
Two authors (D.C.T. and F.N.G.) independently performed title and abstract screening, followed by a full-text review to determine whether studies met the inclusion and exclusion criteria. (Figure 1) The senior author (D.M.K.) was assigned to consult if any disagreements were encountered between the 2 authors, but none were encountered. References from the included studies were reviewed to ensure no additional studies meeting the inclusion criteria had been overlooked, and no further studies were identified.

PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Review and Meta-analysis.
Data Extraction
For studies meeting the criteria for full-text review, the following study characteristics from each article were extracted and entered in a Microsoft Excel Version 16.84 (Microsoft Corp) spreadsheet: study title, year published, first author, level of evidence, patient characteristics (eg, age at the time of presentation, sex), final follow-up time, time from injury to surgery, mechanism/causes of injury, pertinent physical examination findings (when reported), knee arthrometer results (when reported) (KT-1000/2000 arthrometer; MEDmetric Corp, to assess ACL laxity); radiographic measure of valgus laxity (Telos SE stress device), indications for reconstruction, reconstruction techniques, grafts used, additional concomitant injuries and interventions (eg, meniscal repair), incidence of postoperative complications/adverse events (eg, graft failure, postoperative stiffness, revision, and reoperation), and postoperative outcomes including return to activity (RTA) and patient-reported outcome measures.
Study Quality Assessment
To minimize bias, a methodological quality assessment was performed by 2 independent authors (D.C.T., F.N.G.) using the Methodological Index for Non-Randomized Studies (MINORS) criteria. 52 If any disagreements were encountered, a third author (D.M.K.) was consulted, and no disagreements were reported. The MINORS criteria consist of 8 questions for nonrandomized noncomparative studies and 12 questions for nonrandomized comparative studies, with each question scored as follows: 0 (not reported); 1 (reported but inadequate); or 2 (reported and adequate). The highest achievable score for a nonrandomized noncomparative study is 16, while the highest achievable score for a nonrandomized comparative study is 24.
Data Analysis
Patient and study characteristics were compiled and analyzed using Microsoft Excel Version 16.84 (Microsoft Corp). Variables, including patient age, mean follow-up, postoperative complications, postoperative outcome measures, and RTA reported in at least 3 studies, were calculated and displayed as a weighted mean with minimum and maximum values. When assessed, the level of sporting activity was assigned according to the International Knee Documentation Committee (IKDC) scoring system. 18 The incidences of overall complications, long-term postoperative knee pain, and reconstruction failures were compiled and pooled as proportions with inverse variance weighting. Forest plots were generated for complications/adverse events, postoperative pain, and reconstruction failures. All results not meeting the criteria for pooling were displayed in table format. The heterogeneity of the included studies was assessed using the I 2 statistic. All analyses were performed using Microsoft Excel Version 16.84 (Microsoft Corp).
Results
The initial literature search identified 702 articles. (Figure 1). After the removal of duplicates (n = 26), 676 articles underwent title and abstract screening. A total of 96 articles were then selected to undergo full-text review. After full-text review, 17 studies were identified as meeting the inclusion and exclusion criteria and were included for further review. One study was level 1 evidence, 2 studies were level 2 evidence, 4 studies were level 3 evidence, and 10 studies were level 4 evidence. The mean MINORS score for the 15 studies that met the assessment criteria was 15.9 (range, 12-22). The mean score for the 10 noncomparative studies was 13.5 (range, 12-16), while the mean score for the 5 comparative studies was 20.6 (range, 18-22). (Appendix Figure A1) Two randomized comparative studies7,13 did not meet the criteria for assessment using the MINORS criteria.
Study and Patient Characteristics
A total of 902 patients undergoing concomitant ACLR and MCLR were identified from the 17 included studies (Table 1). The weighted mean patient age was 32.9 years (range, 14-74 years), while 68.4% (n = 471/689) of patients were men. The weighted mean time to the final follow-up was 30.6 months (range, 15-61 months), as reported for 140 patients in 4 studies.7,8,13,61
Overview of Included Studies and Patients a
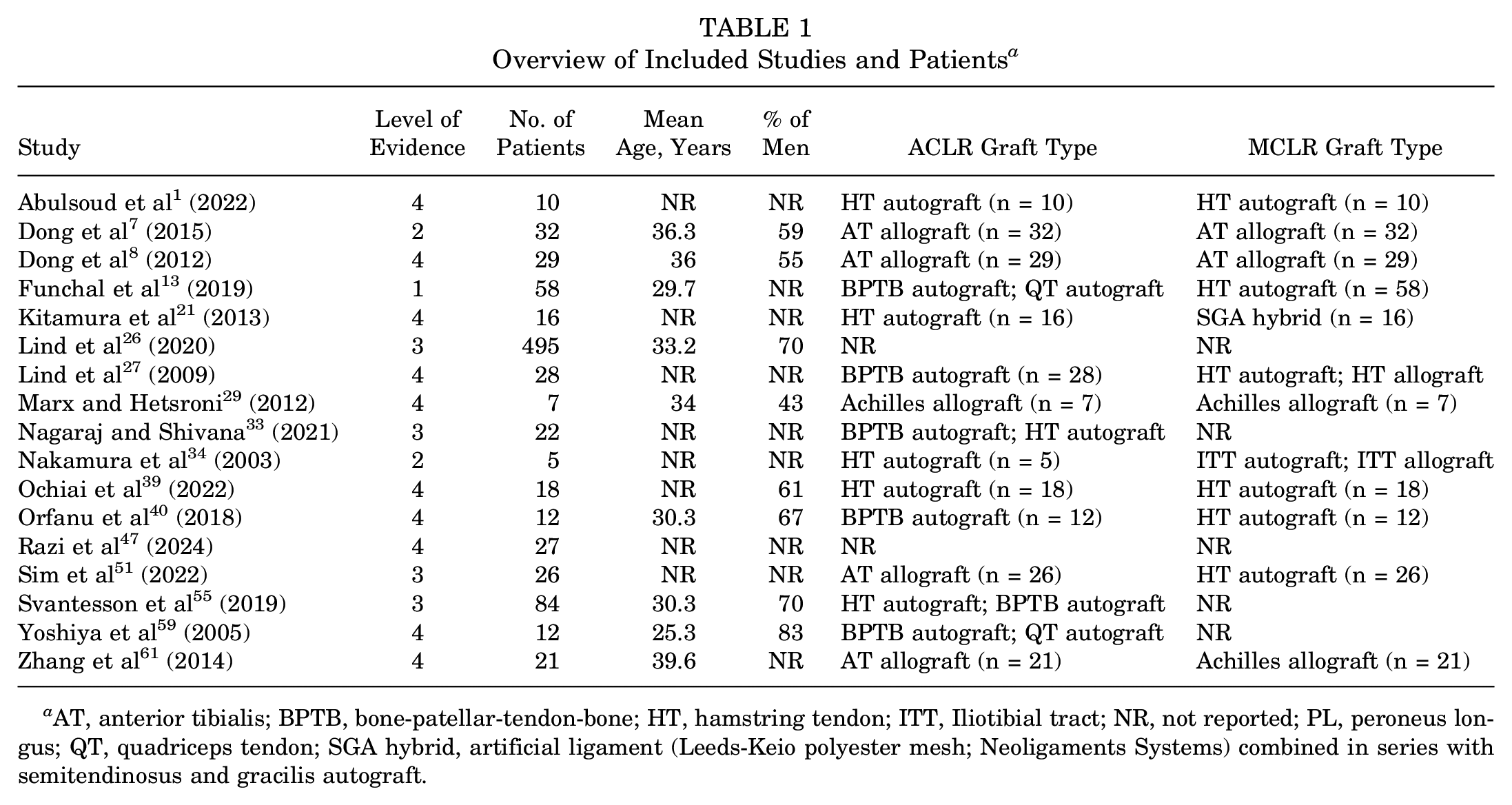
AT, anterior tibialis; BPTB, bone-patellar-tendon-bone; HT, hamstring tendon; ITT, Iliotibial tract; NR, not reported; PL, peroneus longus; QT, quadriceps tendon; SGA hybrid, artificial ligament (Leeds-Keio polyester mesh; Neoligaments Systems) combined in series with semitendinosus and gracilis autograft.
Injury mechanism was reported in 66.7% (n = 602/902) of cases. Sports-related26,34,39,55 injuries were the most commonly reported causes (51.3%; n = 309/602), with level (jumping, cutting, and pivoting sports)18,26,55 accounting for 60.8% (n = 188/309) of sports-related cases, followed by skiing and snowboarding 26 injuries (33%, n = 102/309). Additional causes of injury included motor vehicular collisions26,34,39 (12.1%, n = 73/602) and injuries occurring during activities of daily living 26 (13.3%, n = 80/602).
Concomitant injuries were reported in 75.8% (n = 684/902) of cases. Ipsilateral meniscal injuries1,7,26,29,34,39,55,59,61 accounted for 43.6% (n = 298/684) of concomitant injuries, while articular cartilage injury7,26,55,61 was reported in 16.8% (n = 115/684).
Diagnostics and Operative Indications
Preoperative diagnostic imaging was reported in 31.9% (n = 288/902) of cases. Magnetic resonance imaging1,7,8,13,27,33,34,39,47,51,61 was utilized in 95.8% (n = 276/288) of initial evaluations to assess ligamentous knee injuries, while the use of plain radiographs1,7,8,13,27,33,34,39,40,47,61 was reported in 81.3% (n = 234/288). MCL injury was confirmed through manual valgus stress ‡ testing in 94.1% (n = 289/307) of preoperative clinical examinations, while valgus stress radiography1,7,8,34,39,40,47,61 was used in 53.5% (n = 154/288) of preoperative assessments. The presence of ACL injury was confirmed preoperatively through the Lachman7,13,29,34,40,47 (45.9%, n = 141/307), pivot shift13,29,40,47 (33.9%, n = 104/307), and anterior drawer7,13 (29.3%, n = 90/307) tests. Patients reported subjective knee instability8,21,27,29,61 in 77.9% (n = 113/145) of cases in which preoperative symptoms were reported.
Surgical indications for concomitant ACLR + MCLR were reported in 90.7% (n = 818/902) of cases. Chronic medial laxity, despite ≥6 weeks of nonoperative management before operative intervention,1,8,21,26,27,29,34,39,47,59,61 was the most common indication for MCLR, reported in 81.5% (n = 667/818) of cases. A total of 59 patients received early ACLR + MCLR within 3 weeks from injury, according to the individual study protocol,7,51 or to achieve a faster return to competitive sports. 39 Grade 3 MCL injuries were reported in 22.2% (n = 182/818) of cases, serving as an indication for MCLR.1,7,8,21,33,34,39,51,59 A total of 58 patients who sustained a grade 2 MCL injury underwent surgical reconstruction based on arthroscopic findings per individual study protocol. 13 The weighted mean time from injury to surgery was 10.1 months (range, 4 days-204 months), reported in 101 patients over 5 studies,7,8,29,59,61 with all surgeries performed concurrently during a single surgical procedure.1,7,21,29,33,39,40,47,59,61
Operative Technique
During ACLR, autografts1,13,21,27,33,34,39,40,55,59 were utilized in 69.7% (n = 265/380) of procedures, while allografts7,8,29,51,61 were used in 30.3% (n = 115/380) (Table 1). Soft-tissue grafts1,7,8,21,34,39,51,61 (eg, semitendinosus, gracilis, and tibialis anterior) comprised 57.3% (n = 157/274) of ACLR grafts, while grafts with a bone block13,27,29,40 (eg, bone-patellar-tendon-bone, quadriceps tendon, Achilles tendon) were utilized in 42.7% (n = 117/274) of cases. The most common graft used for ACLR was the tibialis anterior allograft7,8,47,51,61 in 28.4% (n = 108/380) of patients.
During MCLR surgeries, autografts1,13,21,39,40,51 were utilized in 61.1% (n = 140/229) of procedures, while allografts7,8,29,61 were used in 38.9% (n = 89/229). Soft-tissue grafts1,7,8,13,21,27,34,39,40,51 comprised 89.3% (n = 234/262) of MCLR grafts, while bone block grafts29,61 were utilized in 10.7% (n = 28/262) of cases. The most frequent graft type for MCLR was the hamstring (semitendinosus and gracilis) autograft,1,13,21,39,40,51 reported in 53.4% (n = 140/262) of patients.
Concomitant surgical procedures were reported in 66% (n = 595/902) of patients and consisted of unspecified meniscal7,61 procedures (35%, n = 208/595), followed by meniscectomy29,39 (3.9%, n = 23/595), meniscal repair1,29,39 (n = 15), and microfracture 7 (n = 1).
Postoperative Outcomes
The weighted mean Tegner score improved from 3.1 preoperatively to 4.8 postoperatively13,26,29,51 (Table 2). The weighted mean preoperative13,39,40 Lysholm score was 55.9 (range, 26-76), while the mean postoperative13,21,29,33,39,40,51 score was 87.6 (range, 73-100). The weighted mean IKDC score improved from 46.5 preoperatively40,61 to 88.5 postoperatively.29,40,61 The RTA7,39,40,51,61 rate was reported in 11.8% (n = 106/902) of patients, with 84% returning to their previous level of activity/sport participation. The RTA was assessed at the end of individual study periods at a weighted mean of 23.4 months (range, 12-48 months).
Postoperative Outcomes and Adverse Events a
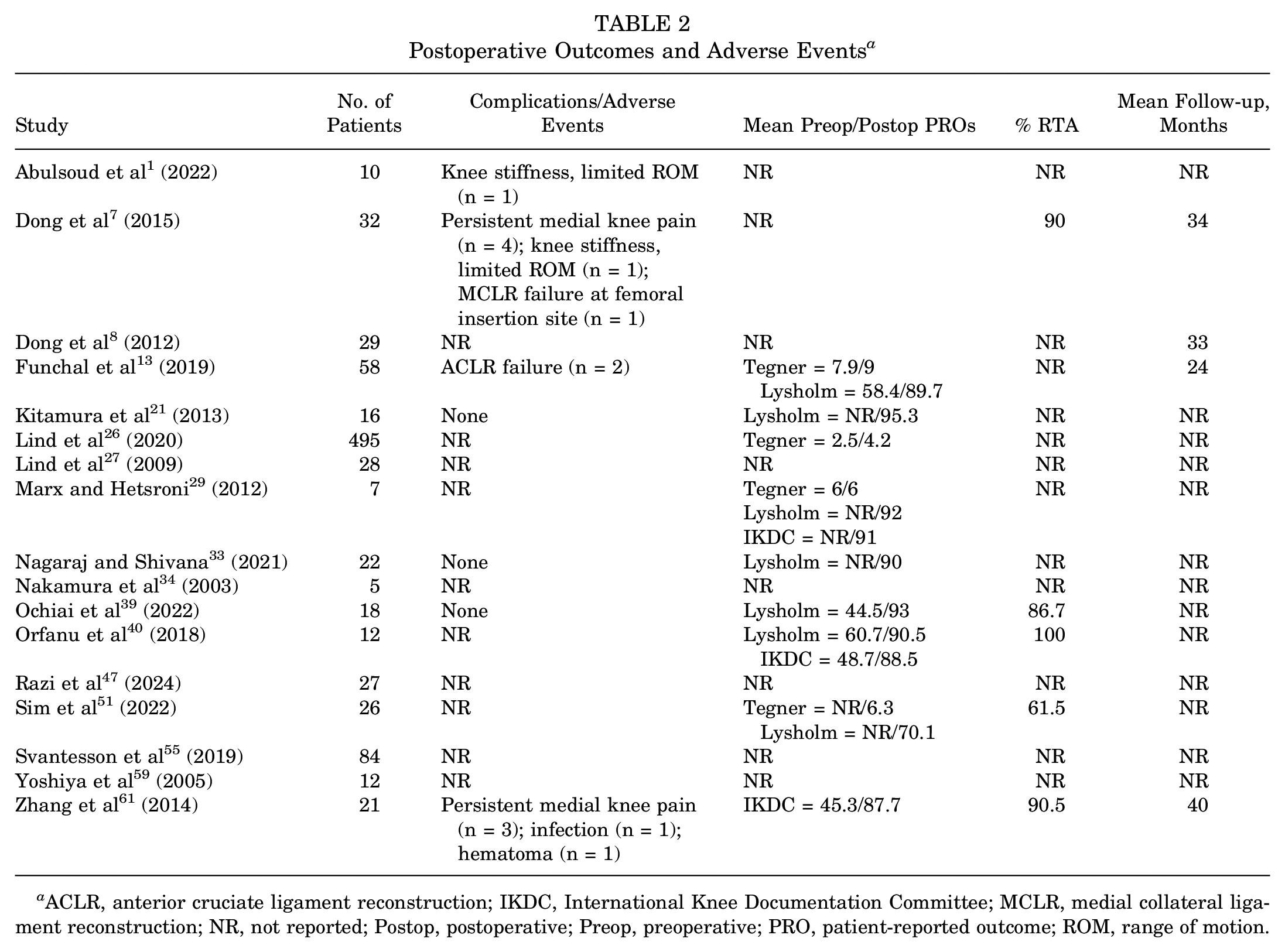
ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; MCLR, medial collateral ligament reconstruction; NR, not reported; Postop, postoperative; Preop, preoperative; PRO, patient-reported outcome; ROM, range of motion.
The KT-1000/2000 arthrometer side-to-side difference in ACL laxity was reported in 59.9% (n = 540/902) of cases preoperatively,26,40,59,61 while the postoperative26,34,40,59,61 side-to-side difference was reported in 62.2% (n = 561/902). The weighted mean side-to-side difference in ACL laxity improved from 6.4 mm (range, 5 to 13.2 mm) preoperatively to 1.7 mm (range, –1.2 to 5 mm) postoperatively. Radiographic medial compartment widening under valgus stress was reported in 11.8% (n = 106/902) of patients preoperatively7,8,40,59,61 and 13.5% (n = 122/902) postoperatively.7,8,21,40,59,61 The weighted mean preoperative medial compartment widening was 8.8 mm (range, 3 to 10.7 mm) and improved to 2 mm (range, –1.2 to 2.6 mm) postoperatively.
Postoperative Complications/Adverse Events
The presence or absence of postoperative complications/adverse outcomes was reported in 19.6% (n = 177/902) of cases across 7 studies1,7,13,21,33,39,61 (Table 2). Postoperative complications were reported in 7.9% (n = 14/177) of patients. The pooled incidence of all complications was 6.9% ± 1.9% (n = 14/177 [95% CI, 3.6%-11.1%]; I 2 = 65.18%; P = .01) (Figure 2). Persistent medial knee pain7,61 after surgery was the most commonly reported adverse outcome (4%, n = 7/177), with a pooled incidence of 3.1% ± 1.3% (n = 7/177 [95% CI, 0.9%-6.2%; I 2 = 56.33%; P = .03) (Figure 3). Four patients who underwent triangular vector reconstruction 7 had prolonged medial knee pain, diagnosed as chronic inflammation, which later resolved with physical therapy and nonsteroidal anti-inflammatory medication. 8 One patient with persistent medial-sided pain 61 underwent screw and washer removal at the MCLR tibial insertion site, with reported resolution of pain. Two additional patients with prolonged postoperative pain 61 were reported to possess advanced articular cartilage injury confirmed during surgery.

Forest plot of proportions for the prevalence of complications related to combined ACLR + MCLR. ACLR, anterior cruciate ligament reconstruction; Ev, events (total number of patients facing complications related to combined ACLR + MCLR); 1a , heterogeneity statistic; MCLR, medial collateral ligament reconstruction; Trt, treatment (total number of patients treated).

Forest plot of proportions for the prevalence of medial knee pain related to combined ACLR + MCLR. ACLR, anterior cruciate ligament reconstruction; Ev, events (total number of patients facing complications related to combined ACLR + MCLR); 1a , heterogeneity statistic; MCLR, medial collateral ligament reconstruction; Trt, treatment (total number of patients treated).
Three cases of reconstruction failure (1.7%, n = 3/177) were reported with a pooled incidence of 2.4% ± 1.2% (n = 3/177 [95% CI, 0.6%-5.2%]; I 2 = 0%; P = .95) (Figure 4). Two failures involved the ACL graft, 13 while 1 MCL graft failure was reported due to fixation screw-pullout at the femoral insertion site. 7 Two cases of postoperative knee stiffness1,7 were reported, with 1 case requiring manipulation under anesthesia. 7 Additional complications included infection 61 (n = 1) and hematoma 61 (n = 1).

Forest plot of proportions for the prevalence of reconstruction failures related to combined ACLR + MCLR. ACLR, anterior cruciate ligament reconstruction; Ev, events (total number of patients facing complications related to combined ACLR + MCLR); 1a , heterogeneity statistic; MCLR, medial collateral ligament reconstruction; Trt, treatment (total number of patients treated).
Discussion
The significant findings of our review demonstrated that sports-related injuries accounted for 51% (n = 309/602) of patients undergoing concurrent primary ACLR + MCLR, with pivot-based sports comprising the majority of cases (61%, n = 188/309). Chronic medial knee laxity after ≥6 weeks of nonoperative management was the most common surgical indication for MCLR, reported in 82% (n = 667/818) of patients, with grade 3 MCL injuries confirmed in 22% (n = 182/818) of cases. Autografts comprised 70% (n = 265/380) and 61% (n = 140/262) of ACLR and MCLR grafts, respectively. When reported, patients returned to their previous activity levels in 84% (n = 89/106) of cases, with improvements in Lysholm, Tegner, and IKDC scores. Persistent medial-sided postoperative pain was the most common adverse outcome, but it was reported in only 4% (n = 7/177) of patients.
Chronic valgus laxity, despite a period of nonoperative management before surgery, and the presence of a grade 3 MCL tear were the most common indications for MCLR. Clinical evidence has established the successful nonoperative management of grade 1 and stable grade 2 MCL injuries in the setting of concomitant ACL rupture.2,16,37,49,60 However, an ongoing debate persists regarding the management of grade 3 and unstable grade 2 tears and the superiority of MCLR versus repair with combined ACLR. Indications for the acute repair of grade 3 injuries include severe valgus malalignment, avulsion fracture, and displacement of the distal aspect of the MCL proximal to the fibers of the pes anserinus (Stener-type lesion) or intra-articularly under the medial meniscus.6,31,50,51 Primary surgical repair of medial knee structures for combined MCL and ACL injury has yielded favorable results.19,22,41,58 However, prominent drawbacks of primary repair include higher rates of postoperative stiffness, slower strength gains, and residual medial laxity resulting from creep and stress relaxation of the injured tissues.15,17,38,43,51 Alternatively, multiple reconstruction methods have evolved to provide immediate medial, sagittal, and rotatory stability with low overall rates of arthrofibrosis.7,50,51,53 Indications for MCLR include failed nonoperative treatment resulting in continued valgus laxity (grade 3 injury) and failed primary repair. Moreover, MCLR is indicated in complex multiligament injuries involving the posteromedial corner (PMC), which necessitate anatomic reconstruction of the superficial MCL (sMCL), deep MCL, and posterior oblique ligament (POL).24,25 When compared with primary repair, primary anatomic reconstruction of the PMC structures has been shown to provide superior stability and lower failure rates. 54
Early MCLR + ACLR was performed within 3 weeks of injury in 59 cases based on individual study protocol or to achieve a faster return to competitive sports. Controversy exists around the timing of MCLR for grade 3 injuries in the setting of ACLR, with no established consensus. Given the excellent healing capacity of the proximal fibers of the MCL, many surgeons prescribe early motion, functional rehabilitation, and bracing with delayed ACLR (>6 weeks) to allow for MCL healing and decrease the risk of motion loss postoperatively.8,21,27,29,61 The MCL is then assessed at the time of ACLR, and a combined reconstruction is performed in those patients who continue to experience excessive valgus laxity at 0° and 30° of knee flexion after nonoperative treatment. In contrast, MCLR + ACLR may be performed acutely (<3 weeks from injury). Proponents of acute reconstruction advocate for early surgery based on data supporting better functional outcomes and higher postoperative outcome scores in patients undergoing early multiligament reconstruction.7,39,51 An additional argument for acute MCLR is to protect the ACLR from further valgus stress, as the ACLR and MCLR work synergistically to provide valgus, anteroposterior, and anteromedial rotatory stability during healing.11,20,26,30,61 A third approach is to perform a combined reconstruction in the subacute timeframe,7,14 between 3 and 6 weeks after injury. This approach aims to achieve the combined benefits of early and delayed reconstruction. Patients are given time to regain some degree of knee motion preoperatively, decreasing the risk of postoperative motion loss or arthrofibrosis, while minimizing residual laxity associated with more delayed intervention.
Autografts comprised 70% and 61% of ACLR and MCLR grafts, respectively. Numerous MCLR techniques have been successfully reported, ranging from all-soft-tissue single- and double-bundle constructs to tibial inlay reconstructions using a graft with a bone block (eg, Achilles tendon). The hamstring tendon (semitendinosus or gracilis) autograft is a widespread graft for MCLR given its proximity to the MCL, favorable safety and biological incorporation profiles, and ability to provide concomitant anatomic sMCL and POL reconstructions.13,21,51,54 Given that the hamstring tendons provide a dynamic restraint to valgus stress, it can be argued that these tendons should not be sacrificed to reconstruct the MCL. Further research is necessary to compare hamstring autografts to allograft tissues for MCLR.
Dong et al7,8 reported simultaneous reconstruction of the middle portion of the sMCL and central arm of the POL using a single continuous tibialis anterior tendon via the “triangular vector” technique. Single-soft-tissue anatomic PMC reconstruction has proven to restore valgus and rotational stability,7,8,54 Alternatively, tibial inlay techniques with an Achilles tendon allograft may more effectively reproduce the native anatomy and orientation of the MCL because of the added stability of bone-to-bone healing.29,61 Proponents of the inlay method further assert the disadvantages of all-soft-tissue autografts—including donor site morbidity and a nonanatomic graft insertion on the tibia (typically too anterior) when preserving the semitendinosus insertion.10,51 As autografts are preferred for combined reconstructions, a common approach is to utilize bilateral hamstring tendons1,21,39 or a bone-block autograft (eg, bone-patellar tendon-bone, quadriceps tendon) for ACLR with contralateral hamstring autograft13,40 for MCLR. However, other reports prefer to minimize donor morbidity and utilize allografts for both ACLR and MCLR.7,8,29,61
Persistent knee pain after surgery was the most common complication in 4% of cases, with reconstruction failures reported in 3 additional patients (2 ACLR failures and 1 MCLR failure). Four patients experiencing prolonged medial pain underwent a “triangular vector” reconstruction, which calls for graft passage through a tibial tunnel with a single femoral fixation point.7,8 While this approach reestablishes valgus and rotational stability, a chronic inflammatory response may develop from graft excursion within the tunnel.6,7 For this reason, Dong et al 7 advised suturing the graft to the surrounding soft tissues to minimize shear stress at the graft-tunnel interface. Coincidentally, the single confirmed MCLR failure was also associated with a triangular vector reconstruction method due to interference screw pull-out at the femoral tunnel. 7 The 2 reported ACLR failures were associated with PMC reconstruction methods that retained the gracilis tibial insertion. 13 This MCLR method offers the advantages of autograft tissue while eliminating the need for routing through a tibial bone tunnel. Unfortunately, the nonanatomic configuration of the triangular vector may lead to increased failure risk due to the anterior placement of the reconstructed sMCL. 6 As reported by LaPrade et al, 23 the placement of a tibial reconstruction tunnel slightly anterior to the pes anserinus resulted in persistent graft failure during biomechanical testing. Further studies are needed to compare the outcomes and complications associated with combined ACRL and MCLR based on graft type and reconstruction method.
This study was not without limitations. The quality and quantity of the current literature represent an inherent limitation of any systematic review. Specifically, a limited number of studies were identified detailing the combined reconstruction of concomitant ACL and MCL injuries. Although there is no comparison to patients with MCL injuries treated nonoperatively or with acute repair, the current study expands on the existing literature by allowing data synthesis of reported techniques and outcomes after ACLR + MCLR. The mean follow-up time for this investigation was limited to four studies, all of which had mean follow-up times under three years. Medium- to long-term follow-up would provide a more thorough analysis of combined reconstruction methods through patient-reported outcomes and clinical evaluation. The included studies consisted predominantly of level 3 and 4 reports, emphasizing the need for additional high-level evidence evaluating outcomes after combined ACLR and MCLR. Furthermore, the weighted mean time from injury to surgery was 10.1 months, which is not indicative of current treatment standards, as early injury identification and management are essential to ensure optimal outcomes. This finding is likely secondary to the small number of studies reporting time from injury to surgery, as well as a wide range of reported times from the included studies, representing an inherent limitation present in the current literature. Due to the heterogeneity of data, small sample size, and the limited number of studies reporting time intervals from injury to surgery, complications, RTA, and patient-reported outcomes, any meaningful statistical analysis drawing comparisons based on graft type (ie, autograft vs allograft), reconstruction method, including surgical timing (ie, acute vs delayed reconstruction), and postoperative rehabilitation techniques, and protocols could not be performed, limiting the findings of this study. Furthermore, patients sustaining injuries to the menisci and chondral surfaces undergoing concomitant procedures were not excluded because of the high frequency of these injuries. This may have affected our ability to identify key variables that may be used to predict long-term success or failure unique to patients undergoing isolated ACLR + MCLR.
Conclusion
Our review revealed that concomitant ACLR + MCLR is most commonly performed for injuries sustained during pivoting sports, which result in persistent valgus laxity. Autografts were used in 70% of ACLR and 61% of MCLR procedures. Improvements in Lysholm, Tegner, and IKDC scores were noted in the majority of patients with a low incidence of complications (7.9%) and reconstruction failures (1.7%). These findings may enhance the understanding of proper surgical indications and methodology, thereby optimizing treatments and postoperative outcomes.
Footnotes
Appendix
Final revision submitted April 30, 2025; accepted May 20, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.H.B. is a paid consultant for Syneos and Anika and the chair of the National Football League (NFL) Musculoskeletal Committee. M.J.M. is a paid consultant for Arthrex, BREG, and Ostesys; is the chair of the NFL Research and Innovation Committee; and has received support for education from Elite Orthopaedics. M.V.S. has received speaking and consulting fees from Arthrex and support for education from Elite Orthopaedics. D.M.K. has received a grant from Arthrex and support for education from Elite Orthopedics and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.