
Abstract
Background:
Between 1.7 and 3 million sports-related concussions occur every year. While most concussion symptoms resolve within 3 weeks, the absence of biomarker-based tests makes evaluating return to sport difficult. Existing guidelines primarily focus on cognitive and executive functions and often overlook proprioceptive abilities. This omission may increase athletes’ risk of subsequent lower extremity injuries during competition.
Purpose/Hypothesis:
The purpose of this study was to assess the rate of lower extremity injuries in athletes in the year following their first concussion. It was hypothesized that athletes with a concussion would be at an increased risk for a subsequent lower extremity injury within 1 year compared with nonconcussed counterparts.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective cohort study utilized the PearlDiver database and was queried on March 29, 2024. International Classification of Diseases, Tenth Revision (ICD-10) codes for sports physicals, activity in sports, and concussions were used to create concussed and nonconcussed athlete cohorts. ICD-10 codes for acute lower extremity injuries were used to identify specific injuries within the concussed and nonconcussed populations at 3, 6, 9, and 12-month intervals. Relative risks (RRs) were then calculated for each observed injury.
Results:
Of the 899,269 athletes, 58,569 (6.5%) suffered a concussion, and of these concussed athletes, 6051 (10.3%) suffered a subsequent lower extremity injury within 1 year. Compared with nonconcussed athletes, there was a significantly increased risk of an unspecified ankle injury (RR, 1.40; P < .05), unspecified knee sprain (RR, 1.36; P < .05), unspecified foot injury (RR, 1.23; P < .001), medial collateral ligament sprain (RR, 1.23; P < .05), ankle sprain (RR, 1.18; P < .001), and foot sprain (RR, 1.10; P < .05). There was no significantly increased risk of sustaining lateral collateral ligament sprains, medial malleolar fractures, and lower extremity muscle strain ≤1 year after a concussion.
Conclusion:
This study found a significant increase in several lower extremity injuries ≤1 year after a concussion. Additional studies are warranted to better understand the different factors affecting concussion risk, which could include inadequate return-to-sport (RTS) protocols and prolonged vestibular dysfunction.
Between 1.7 and 3 million sports-related concussions occur every year in the United States. 7 This can pose a significant concern for the athlete and his or her overall health, as well as the treating physician, who is tasked with safely clearing the athlete for RTS. The difficulty in determining full recovery can often complicate the decision-making process behind clearance for RTS postconcussion. Concussion injuries commonly occur due to high-velocity direct effects or sudden unexpected movements that cause the brain to move within the skull. 7 These mechanisms of injury are commonly seen in football, soccer, hockey, and other contact sports. The incidence of concussions in young athletes is a growing concern, with concussions accounting for nearly 9% of all high school sports-related injuries. 10 Furthermore, emerging research has shown that the developing adolescent brain takes longer to heal after a concussion, and premature RTS may exacerbate the risks of subsequent concussions and other associated injuries. 6
The stages of a concussion can be broken down into 3 phases: the acute symptomatic phase, recovery phase, and recovered phase. 8 Common symptoms involve headache, dizziness, and brief visual deficits, but providers should be aware of red flag symptoms, including loss of consciousness for >1 minute, repeated vomiting, seizures, sustained extremity weakness or paresthesia, persistent vision changes, and personality changes.8,20 During the symptomatic phase, the American Medical Society for Sports Medicine recommends a 24-hour cessation of all athletic activities. 18 Symptoms usually begin to improve after 3 days of rest, and during the recovery phase, athletes are encouraged to resume light aerobic exercise and gradually return to the preinjured state; however, it is not uncommon for symptoms to initially worsen as activities increase in intensity.8,18 After ≥1 week after the initial concussion, provided they are symptom-free and cleared by medical staff, athletes enter the recovered stage and are allowed to return to full competition.8,18 Most athletes recover rapidly after their first concussion, with most returning to competition within 8 days.9,15,17,26 However, the decision to clear the athlete is difficult, as it is largely a clinical diagnosis dependent on the medical team’s judgment, with some athletes continuing to have symptoms for 12 months.4,5
One of the most feared consequences of clearing an athlete to RTS prematurely is the theoretical risk of a new athletic injury. Previous studies have demonstrated a link in athletes between recent concussions and lower extremity injuries. § However, most of these studies utilized a small sample size of professional athletes, thus limiting their generalizability. This current study aims to determine whether an athlete suffering his or her first concussion increases the risk of developing a lower extremity injury within 1 year in comparison with athletes who did not suffer a concussion. We hypothesize that concussed athletes will have a higher risk of subsequent lower extremity injuries within 1 year compared with healthy counterparts.
Methods
This retrospective cohort study utilized the PearlDiver M157 database, which provided publicly available Health Insurance Portability and Accountability Act–compliant deidentified information from 151 million patients spanning 2007 to 2020. Search queries of the database were achieved using International Classification of Diseases, Tenth Revision (ICD-10) codes related to sports activity and lower extremity musculoskeletal injuries. Institutional review board approval was not needed for this study. Final search queries were performed on March 29, 2024.
ICD-10 codes Z02.5 (examination for participation in sport), Y93.22 (activity, ice hockey), Y93.61 (activity, American tackle football), Y93.63 (activity, rugby), Y93.65 (activity, lacrosse and field hockey), Y93.66 (activity, soccer), and Y93.67 (activity, basketball) were used to define our initial athlete population. A group of concussed athletes was then created by filtering the athlete population for the first instance of diagnostic codes related to concussions (S06.0X0A, S06.0X1A, S06.0X2A, S06.0X3A, S06.0X4A, S06.0X5A, S06.0X9A, S06.0XAA). All patients also had to be active in the database for 12 months before and after their first concussion and be <30 years of age. A control population was created from the same athlete population to include patients who did not suffer from a concussion for ≥1 year before and after the indexed ICD-10 code for participation in their respective sport. The cohorts did not significantly differ in demographic characteristics or Charlson Comorbidity Index, a predictor of 10-year survival based on medical comorbidities (Table 1). All patients had no history of previous coded concussions.
Age, Sex, and Charlson Comorbidity Index of All Study Cohorts a

Data are presented as median ± SD or n (%) unless otherwise indicated. There were no statistically significant differences between demographic parameters for patients included. CCI, Charlson Comorbidity Index; LE, lower extremity.
ICD-10 codes for acute lower extremity injuries, such as joint sprain, joint dislocation, muscle strain, ankle fracture, and meniscal tear, were used to identify specific injuries within the concussed and nonconcussed athlete populations. A complete list of ICD-10 codes and types of injuries is found in Appendix Table A1.
Statistical analysis was initially performed using a chi-square analysis to compare the rates of specific injuries between the 2 populations at 3, 6, 9, and 12 months. This was followed by a relative risk (RR) analysis, which determined the magnitude of association between a concussion and specific lower extremity injuries at the same time intervals. The threshold for statistical significance was set as a P value of <.05. Subsequent risk factor analysis was performed with significance set at a P value of <.05.
Results
There were a total of 899,269 athletes who met the inclusion criteria with a median age of 15. Of these athletes, 58,569 (6.5%) suffered a concussion during the time frame of the study. A total of 6051 (10.3%) concussed athletes endured a total of 9384 acute lower extremity injuries ≤1 year following their first concussion. The most common injuries among concussed athletes were ankle sprain (n = 3168; 39.1%), knee sprain (n = 1319; 21.8%), unspecified ankle injury (n = 1247; 15.4%), meniscal injury (n = 923; 11.4%), and unspecified foot injury (n = 751; 9.3%) as shown in Figure 1. These were also the top 5 most common injuries among nonconcussed athletes. When compared with the nonconcussed athlete population, there was a significant increase in the risk of suffering an unspecified ankle injury (RR, 1.40; 95% CI, 1.32-1.48; P < .05), unspecified knee sprain (RR, 1.36; 95% CI, 1.27-1.46; P < .05), unspecified foot injury (RR, 1.23; 95% CI, 1.14-1.32; P < .001), medial collateral ligament (MCL) sprain (RR, 1.23; 95% CI, 1.11-1.38; P < .05), ankle sprain (RR, 1.18; 95% CI, 1.14-1.22; P < .001), and foot sprain (RR, 1.10; 95% CI, 1.01-1.21; P < .05) (Figure 2). There was no significant difference in the risk of lateral collateral ligament sprains (RR, 1.07; 95% CI, 0.87-1.33; P = .42), medial malleolar fractures (RR, 0.95; 95% CI,0.73-1.23; P = .14), and lower extremity muscle strain (RR, 1.07; 95% CI, 0.98-1.17; P = .15). The injury rate per 1000 concussed athletes was initially lower for ankle sprains, MCL sprains, unspecified foot injury, and foot sprain at 3 months compared with the nonconcussed athlete population but then became higher than that of nonconcussed athletes by the 12-month mark (Figure 3). Risk factors within the concussed cohort also consisted of female sex (odds ratio [OR], 1.14; 95% CI, 1.08-1.21; P < .05), tobacco use (OR, 1.33; 95% CI, 1.21-1.46; P < .05), and obesity (OR, 1.25; 95% CI, 1.16-1.35; P < .05) (Table 2).

Most common injuries at 1 year in both concussed and nonconcussed young athletes. Comparisons between groups were performed using Chi square analysis. *P < .05.

Relative risk of sustaining a lower extremity injury 12 months after a concussion and with error bars representing a 95% CI. Bolded injuries represent P < .05. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament.
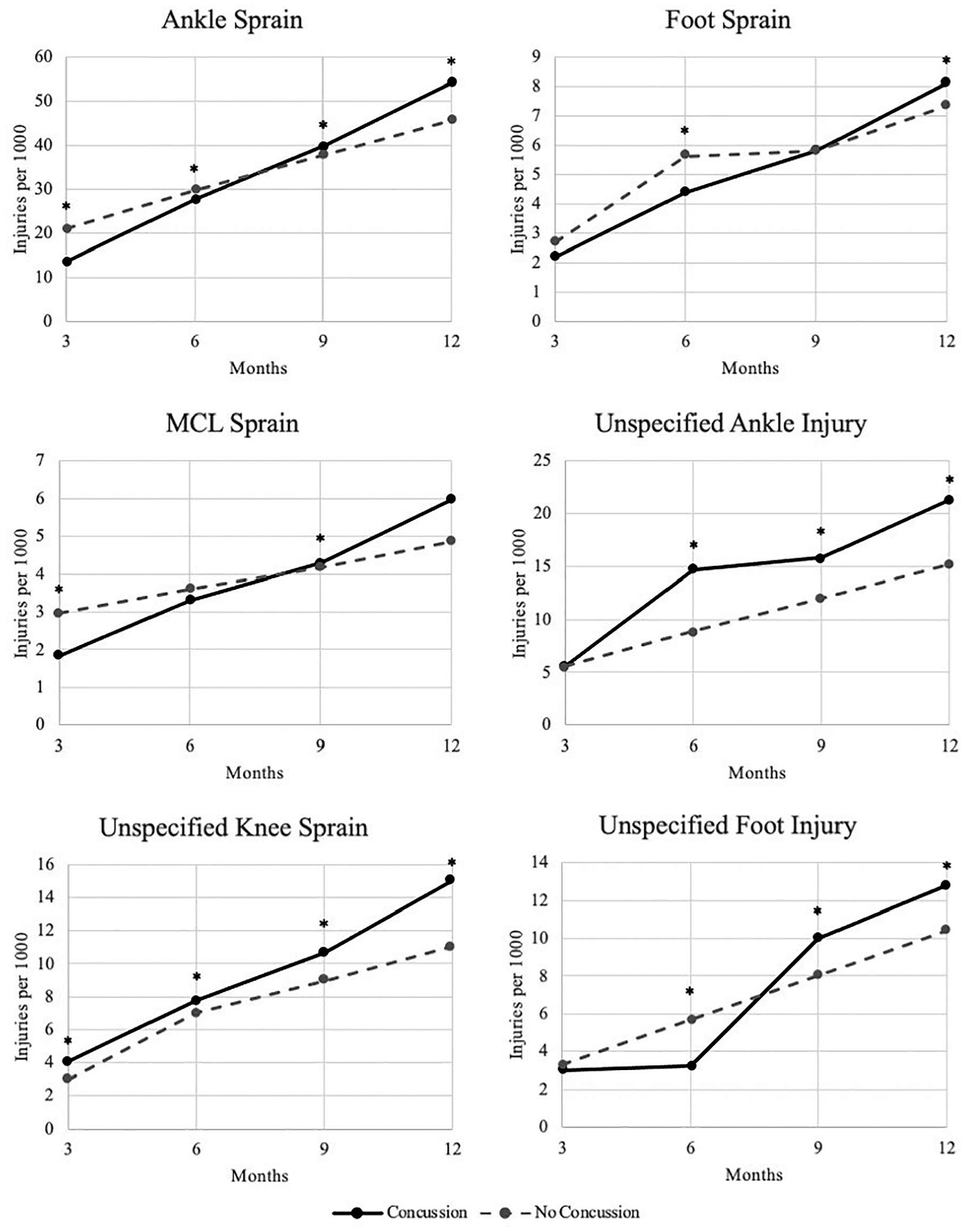
Rate of lower extremity injuries in concussed and healthy athletes over 12 months. Asterisk indicates a significant difference between the 2 cohorts (P < .05) from Chi square analysis. MCL, medial collateral ligament.
Demographic Risk Factor Analysis for Developing a Lower Extremity Injury After a Concussion

Discussion
The results of this study demonstrate that concussed athletes are at a 40% increased risk of an unspecified ankle injury, a 36% increased risk of an unspecified knee sprain, a 23% increased risk of an MCL sprain, a 23% increased risk of an unspecified foot injury, an 18% increased risk of an ankle sprain, and a 10% increased risk of a foot sprain in the year after their first concussion when compared with athletes who did not sustain a concussion. There was no significant increase in the risk of more serious injuries such as fractures and ligamentous tears. The most common injuries for all athletes were ankle sprain, followed by knee sprain, meniscal injury, and foot injury. In addition, during the first 3 months after a concussion, concussed athletes sustained injuries at a lesser rate compared with athletes who did not endure a concussion.
We hypothesized that concussed athletes would experience a statistically significant increase in lower extremity injuries over the year after their concussion when compared with athletes who did not have a concussion. This hypothesis was corroborated by the findings from our large-scale data set, which tracked thousands of athletes and their injuries. This trend has been observed in other studies. In a meta-analysis of 8 studies, McPherson etal 19 found that concussed athletes were 1.67 times more likely to experience a lower extremity musculoskeletal injury after returning to play compared with nonconcussed athletes. Similarly, Nordstöm etal 21 found a hazard ratio of 1.47 for lower extremity injuries in European soccer players in the year following a concussion, and Herman etal 11 found a 3.4-fold increase in lower extremity injuries after a concussion in National Collegiate Athletic Association Division I athletes.
Even with these increased lower extremity injuries, the overall prognosis for recovering from a concussion is quite favorable. In a meta-analysis of 120 studies, Carroll etal 5 found that the majority of adults recovered fully in 3 to 12 months with no persistent symptoms or cognitive impairment. Additionally, immediate reporting of concussion-like symptoms and prompt removal from physical activity or competition has been shown to decrease recovery times. 25 However, the added disability from the increased risk of lower extremity injuries can have lasting effects on athletes’ careers and daily lives. A study by Anandacoomarasamy and Bransley 1 found that 74% of individuals reported pain, swelling, weakness, or instability 1 to 4 years after an ankle sprain with a long-term study by Konradsen etal 14 showing 32% of patients complaining of similar symptoms 7 years after their initial ankle injury. These findings, taken together, highlight the importance of treating both the initial concussion and the prevention of subsequent injuries to maintain a high level of functioning during athletic events and activities of daily living.
A finding in our study that has not been previously reported in the literature is that concussed athletes did not tend to contract lower extremity injuries at a higher rate than their concussion-free counterparts during the acute phase of their recovery (Figure 3). For example, rates of ankle sprain per 1000 athletes were lower in the concussed population at 3 and 6 months compared with those of controls. Only after 9 months did rates of ankle sprain increase in the concussed population compared with the nonconcussed. This overall trend was also seen with MCL sprains, foot sprains, and unspecified foot injuries. This finding may be in part due to concussed athletes’ receiving reduced playing time and increased restrictions during training in the acute phase after a concussion. Furthermore, athletes with a concussion near the end of the season may opt to sit out for the remainder of their schedule and reduce the risk of injuries. However, in a study of professional basketball players in the National Basketball Association (NBA) who experienced non–season ending concussions, the concussed athletes were 4.69 times more likely to sustain an acute lower extremity musculoskeletal injury in the immediate 90-day period after the concussion compared with nonconcussed controls. 16 While it can be assumed that players in the NBA were receiving adequate treatment and rehabilitation after their concussion, the incentives and contractual obligations of returning to extremely high levels of physical activity may make this finding ungeneralizable to the broader young athlete population. The lower acute time frame injury rate and higher 12-month injury rate of concussed versus nonconcussed athletes further support the idea that clinical and subclinical effects of concussions exist for up to a year and possibly beyond, which should be considered in future updates of concussion management protocols and RTS guidelines.
Reasons for the increased risk of numerous lower extremity injuries in the year following a concussion are multifactorial, with the nature of the initial injury, rehabilitation process, and RTS criteria all having an effect. One area of interest in the current literature is vestibular dysfunction and its relationship with subsequent injuries. In a study by Howell etal, 12 the researchers found that peak mediolateral acceleration during the gait cycle was reduced for up to 2 months after a concussion, which is longer than the typical time frame that neurocognitive symptoms resolve and when most athletes are cleared to RTS. Parrington etal 23 also found that concussed athletes had significantly higher amounts of sway with the Balance Error Scoring System, one of the major tests used for evaluating RTS after a concussion. This deficit remained for the duration of the 8-week study period, which is longer than the normal RTS time frame. Further work is needed to fully assess the interconnected nature of concussions, vestibular dysfunction, and injury risk in athletes.
Limitations
Although this study includes a large sample size, it does have limitations. The first and most important thing is that although a database study allowed us to increase our sample size to the largest cohort of young concussed athletes to date, insights from the data are limited by ICD code classifications. Additionally, with a database study, the data are deidentified, and patient chart information is not available, which made it difficult to control for possible confounding variables, such as initial injury severity, concomitant cervical spine trauma, training schedule, playing surfaces, medical care, and individual return-to-play protocol. Furthermore, depending on the timing or severity of the injury, players may opt to extend their recovery, sit out for the remainder of the season, or stop playing the sport entirely, which would underestimate the perceived correlation between a primary concussion and subsequent lower extremity injury. Most importantly, as with any database study, the data collected are limited to what is coded in the chart and billed for by treating physicians. Many athletes do not seek professional medical care for routine muscle strains and minor injuries. This can result in a substantial underestimation of most muscular injuries, particularly in those treated by on-site physical therapists and team staff who would not record the injury in an insurance-based database.
Conclusion
Our study found a significant increase in several lower extremity injuries up to 1 year after a concussion. Additional studies are warranted to better understand the different factors affecting concussion risk, which could include inadequate return-to-play protocols and prolonged vestibular dysfunction.
Footnotes
Appendix
ICD-10 Codes Used to Define Lower Extremity Injuries a

| Outcome | ICD-10 Code |
|---|---|
| Dislocation, patella | ICD-10-D-M2200, ICD-10-D-M2201, ICD-10-D-M2202, ICD-10-D-S83094A, ICD-10-D-S83095A, ICD-10-D-S83096A |
| Subluxation, patella | ICD-10-D-M2210, ICD-10-D-M2211, ICD-10-D-M2212, ICD-10-D-S83001A, ICD-10-D-S83002A, ICD-10-D-S83003A, ICD-10-D-S83004A, ICD-10-D-S83005A, ICD-10-D-S83006A, ICD-10-D-S83011A, ICD-10-D-S83012A, ICD-10-D-S83013A, ICD-10-D-S83014A, ICD-10-D-S83015A, ICD-10-D-S83016A, ICD-10-D-S83091A, ICD-10-D-S83092A, ICD-10-D-S83093A |
| Disorder, patella, other | ICD-10-D-M223X1, ICD-10-D-M223X2, ICD-10-D-M223X9, ICD-10-D-M228X1, ICD-10-D-M228X2, ICD-10-D-M228X9 |
| Tear, ACL | ICD-10-D-M23611, ICD-10-D-M23612, ICD-10-D-M23619 |
| Tear, PCL | ICD-10-D-M23621, ICD-10-D-M23622, ICD-10-D-M23629 |
| Tear, MCL | ICD-10-D-M23631, ICD-10-D-M23632, ICD-10-D-M23639 |
| Tear, LCL | ICD-10-D-M23641, ICD-10-D-M23642, ICD-10-D-M23649 |
| Tear, knee ligament, unspecified | ICD-10-D-M23601, ICD-10-D-M23602, ICD-10-D-M23609, ICD-10-D-M23671, ICD-10-D-M23672, ICD-10-D-M23679 |
| Instability, knee | ICD-10-D-M2350 |
| Dislocation, knee | ICD-10-D-M24361, ICD-10-D-M24362, ICD-10-D-M24369, ICD-10-D-M24461, ICD-10-D-M24462, ICD-10-D-M24469, ICD-10-D-S83104A,ICD-10-D-S83105A, ICD-10-D-S83114A, ICD-10-D-S83115A, ICD-10-D-S83116A, ICD-10-D-S83124A, ICD-10-D-S83125A, ICD-10-D-S83126A, ICD-10-D-S83134A, ICD-10-D-S83135A, ICD-10-D-S83136A, ICD-10-D-S83144A, ICD-10-D-S83145A, ICD-10-D-S83146A, ICD-10-D-S83194A, ICD-10-D-S83195A, ICD-10-D-S83196A |
| Subluxation, knee | ICD-10-D-S83101A, ICD-10-D-S83102A, ICD-10-D-S83111A, ICD-10-D-S83112A, ICD-10-D-S83113A, ICD-10-D-S83121A, ICD-10-D-S83122A, ICD-10-D-S83123A, ICD-10-D-S83131A, ICD-10-D-S83132A, ICD-10-D-S83133A, ICD-10-D-S83141A, ICD-10-D-S83142A, ICD-10-D-S83143A, ICD-10-D-S83191A, ICD-10-D-S83192A, ICD-10-D-S83193A |
| Fracture, medial malleolus | ICD-10-D-S8251XA, ICD-10-D-S8251XB, ICD-10-D-S8251XC, ICD-10-D-S8252XA, ICD-10-D-S8252XB, ICD-10-D-S8252XC, ICD-10-D-S8253XA, ICD-10-D-S8253XB, ICD-10-D-S8253XC, ICD-10-D-S8254XA, ICD-10-D-S8254XB, ICD-10-D-S8254XC, ICD-10-D-S8255XA, ICD-10-D-S8255XB, ICD-10-D-S8255XC, ICD-10-D-S8256XA, ICD-10-D-S8256XB, ICD-10-D-S8256XC |
| Fracture, lateral malleolus | ICD-10-D-S8261XA, ICD-10-D-S8261XB, ICD-10-D-S8261XC, ICD-10-D-S8262XA, ICD-10-D-S8262XB, ICD-10-D-S8262XC, ICD-10-D-S8263XA, ICD-10-D-S8263XB, ICD-10-D-S8263XC, ICD-10-D-S8264XA, ICD-10-D-S8264XB, ICD-10-D-S8264XC, ICD-10-D-S8265XA, ICD-10-D-S8265XB, ICD-10-D-S8265XC, ICD-10-D-S8266XA, ICD-10-D-S8266XB, ICD-10-D-S8266XC |
| Fracture, bimalleolar | ICD-10-D-S82841A, ICD-10-D-S82841B, ICD-10-D-S82841C, ICD-10-D-S82842A, ICD-10-D-S82842B, ICD-10-D-S82842C, ICD-10-D-S82843A, ICD-10-D-S82843B, ICD-10-D-S82843C, ICD-10-D-S82844A, ICD-10-D-S82844B, ICD-10-D-S82844C, ICD-10-D-S82845A, ICD-10-D-S82845B, ICD-10-D-S82845C, ICD-10-D-S82846A, ICD-10-D-S82846B, ICD-10-D-S82846C |
| Fracture, trimalleolar | ICD-10-D-S82851A, ICD-10-D-S82851B, ICD-10-D-S82851C, ICD-10-D-S82852A, ICD-10-D-S82852B, ICD-10-D-S82852C, ICD-10-D-S82853A, ICD-10-D-S82853B, ICD-10-D-S82853C, ICD-10-D-S82854A, ICD-10-D-S82854B, ICD-10-D-S82854C, ICD-10-D-S82855A, ICD-10-D-S82855B, ICD-10-D-S82855C, ICD-10-D-S82856A, ICD-10-D-S82856B, ICD-10-D-S82856C |
| Fracture, Maisonneuve | ICD-10-D-S82861A, ICD-10-D-S82861B, ICD-10-D-S82861C, ICD-10-D-S82862A, ICD-10-D-S82862B, ICD-10-D-S82862C, ICD-10-D-S82863A, ICD-10-D-S82863B, ICD-10-D-S82863C, ICD-10-D-S82864A, ICD-10-D-S82864B, ICD-10-D-S82864C, ICD-10-D-S82865A, ICD-10-D-S82865B, ICD-10-D-S82865C, ICD-10-D-S82866A, ICD-10-D-S82866B, ICD-10-D-S82866C |
| Tear, meniscus | ICD-10-D-S83200A, ICD-10-D-S83201A, ICD-10-D-S83202A, ICD-10-D-S83203A, ICD-10-D-S83204A, ICD-10-D-S83205A, ICD-10-D-S83206A, ICD-10-D-S83207A, ICD-10-D-S83209A, ICD-10-D-S83211A, ICD-10-D-S83212A, ICD-10-D-S83219A, ICD-10-D-S83221A, ICD-10-D-S83222A, ICD-10-D-S83229A, ICD-10-D-S83231A, ICD-10-D-S83232A, ICD-10-D-S83239A, ICD-10-D-S83241A, ICD-10-D-S83242A, ICD-10-D-S83249A, ICD-10-D-S83251A, ICD-10-D-S83252A, ICD-10-D-S83259A, ICD-10-D-S83261A, ICD-10-D-S83262A, ICD-10-D-S83269A, ICD-10-D-S83271A, ICD-10-D-S83272A, ICD-10-D-S83279A, ICD-10-D-S83281A, ICD-10-D-S83282A, ICD-10-D-S83289A, ICD-10-D-M23300, ICD-10-D-M23301, ICD-10-D-M23302, ICD-10-D-M23303, ICD-10-D-M23304, ICD-10-D-M23305, ICD-10-D-M23306, ICD-10-D-M23307, ICD-10-D-M23309, ICD-10-D-M23311, ICD-10-D-M23312, ICD-10-D-M23319, ICD-10-D-M23321, ICD-10-D-M23322, ICD-10-D-M23329, ICD-10-D-M23331, ICD-10-D-M23332, ICD-10-D-M23339, ICD-10-D-M23341, ICD-10-D-M23342, ICD-10-D-M23349, ICD-10-D-M23351, ICD-10-D-M23352, ICD-10-D-M23359, ICD-10-D-M23361, ICD-10-D-M23362, ICD-10-D-M23369, ICD-10-D-M238X1, ICD-10-D-M238X2, ICD-10-D-M238X9, ICD-10-D-M2391, ICD-10-D-M2392 |
| Sprain, MCL | ICD-10-D-S83411A, ICD-10-D-S83412A, ICD-10-D-S83419A |
| Sprain, LCL | ICD-10-D-S83421A, ICD-10-D-S83422A, ICD-10-D-S83429A |
| Sprain, ACL | ICD-10-D-S83511A, ICD-10-D-S83512A, ICD-10-D-S83519A |
| Sprain, PCL | ICD-10-D-S83521A, ICD-10-D-S83522A, ICD-10-D-S83529A |
| Sprain, knee, unspecified | ICD-10-D-S83401A, ICD-10-D-S83402A, ICD-10-D-S83409A, ICD-10-D-S83501A, ICD-10-D-S83502A, ICD-10-D-S83509A, ICD-10-D-S8360XA, ICD-10-D-S8361XA, ICD-10-D-S8362XA, ICD-10-D-S838X1A, ICD-10-D-S838X2A, ICD-10-D-S838X9A, ICD-10-D-S8390XA, ICD-10-D-S8391XA, ICD-10-D-S8392XA |
| Strain, Achilles | ICD-10-D-S86001A, ICD-10-D-S86002A, ICD-10-D-S86009A, ICD-10-D-S86011A, ICD-10-D-S86012A, ICD-10-D-S86019A, ICD-10-D-S86091A, ICD-10-D-S86092A, ICD-10-D-S86099A |
| Strain, lower extremity muscle | ICD-10-D-S86101A, ICD-10-D-S86102A, ICD-10-D-S86109A, ICD-10-D-S86111A, ICD-10-D-S86112A, ICD-10-D-S86119A, ICD-10-D-S86191A, ICD-10-D-S86192A, ICD-10-D-S86199A, ICD-10-D-S86201A, ICD-10-D-S86202A, ICD-10-D-S86209A, ICD-10-D-S86211A, ICD-10-D-S86212A, ICD-10-D-S86219A, ICD-10-D-S86291A, ICD-10-D-S86292A, ICD-10-D-S86299A, ICD-10-D-S86301A, ICD-10-D-S86302A, ICD-10-D-S86309A, ICD-10-D-S86311A, ICD-10-D-S86312A, ICD-10-D-S86319A, ICD-10-D-S86391A, ICD-10-D-S86392A, ICD-10-D-S86399A, ICD-10-D-S86801A, ICD-10-D-S86802A, ICD-10-D-S86809A, ICD-10-D-S86811A, ICD-10-D-S86812A, ICD-10-D-S86819A, ICD-10-D-S86891A, ICD-10-D-S86892A, ICD-10-D-S86899A, ICD-10-D-S86901A, ICD-10-D-S86902A, ICD-10-D-S86909A, ICD-10-D-S86911A, ICD-10-D-S86912A, ICD-10-D-S86919A, ICD-10-D-S86991A, ICD-10-D-S86992A, ICD-10-D-S86999A, ICD-10-D-M62061, ICD-10-D-M62062, ICD-10-D-M62069, ICD-10-D-M62071, ICD-10-D-M62072, ICD-10-D-M62079, ICD-10-D-M62161, ICD-10-D-M62162, ICD-10-D-M62169, ICD-10-D-M62171, ICD-10-D-M62172, ICD-10-D-M62179, ICD-10-D-S96001A, ICD-10-D-S96002A, ICD-10-D-S96009A, ICD-10-D-S96011A, ICD-10-D-S96012A, ICD-10-D-S96019A, ICD-10-D-S96091A, ICD-10-D-S96092A, ICD-10-D-S96099A, ICD-10-D-S96101A, ICD-10-D-S96102A, ICD-10-D-S96109A, ICD-10-D-S96111A, ICD-10-D-S96112A, ICD-10-D-S96119A, ICD-10-D-S96191A, ICD-10-D-S96192A, ICD-10-D-S96199A, ICD-10-D-S96201A, ICD-10-D-S96202A, ICD-10-D-S96209A, ICD-10-D-S96211A, ICD-10-D-S96212A, ICD-10-D-S96219A, ICD-10-D-S96291A, ICD-10-D-S96292A, ICD-10-D-S96299A, ICD-10-D-S96801A, ICD-10-D-S96802A, ICD-10-D-S96809A, ICD-10-D-S96811A, ICD-10-D-S96812A, ICD-10-D-S96819A, ICD-10-D-S96891A, ICD-10-D-S96892A, ICD-10-D-S96899A, ICD-10-D-S96901A, ICD-10-D-S96902A, ICD-10-D-S96909A, ICD-10-D-S96911A, ICD-10-D-S96912A, ICD-10-D-S96919A, ICD-10-D-S96991A, ICD-10-D-S96992A, ICD-10-D-S96999A |
| Rupture, lower extremity tendon | ICD-10-D-M66261, ICD-10-D-M66262, ICD-10-D-M66269, ICD-10-D-M66271, ICD-10-D-M66272, ICD-10-D-M66279, ICD-10-D-M66361, ICD-10-D-M66362, ICD-10-D-M66369, ICD-10-D-M66371, ICD-10-D-M66372, ICD-10-D-M66379, ICD-10-D-M66861, ICD-10-D-M66862, ICD-10-D-M66869, ICD-10-D-M66871, ICD-10-D-M66872, ICD-10-D-M66879, ICD-10-D-M67863, ICD-10-D-M67864, ICD-10-D-M67869, ICD-10-D-M67873, ICD-10-D-M67874, ICD-10-D-M67879, ICD-10-D-M67961, ICD-10-D-M67962, ICD-10-D-M67969, ICD-10-D-M67971, ICD-10-D-M67972, ICD-10-D-M67979 |
| Sprain, ankle | ICD-10-D-S93401A, ICD-10-D-S93402A, ICD-10-D-S93409A, ICD-10-D-S93411A, ICD-10-D-S93412A, ICD-10-D-S93419A, ICD-10-D-S93421A, ICD-10-D-S93422A, ICD-10-D-S93429A, ICD-10-D-S93431A, ICD-10-D-S93432A, ICD-10-D-S93439A, ICD-10-D-S93491A, ICD-10-D-S93492A, ICD-10-D-S93499A, ICD-10-D-M24271, ICD-10-D-M24272, ICD-10-D-M24273 |
| Sprain, foot | ICD-10-D-S93501A, ICD-10-D-S93502A, ICD-10-D-S93503A, ICD-10-D-S93504A, ICD-10-D-S93505A, ICD-10-D-S93506A, ICD-10-D-S93509A, ICD-10-D-S93511A, ICD-10-D-S93512A, ICD-10-D-S93513A, ICD-10-D-S93514A, ICD-10-D-S93515A, ICD-10-D-S93516A, ICD-10-D-S93519A, ICD-10-D-S93521A, ICD-10-D-S93522A, ICD-10-D-S93523A, ICD-10-D-S93524A, ICD-10-D-S93525A, ICD-10-D-S93526A, ICD-10-D-S93529A, ICD-10-D-S93601A, ICD-10-D-S93602A, ICD-10-D-S93609A, ICD-10-D-S93611A, ICD-10-D-S93612A, ICD-10-D-S93619A, ICD-10-D-S93621A, ICD-10-D-S93622A, ICD-10-D-S93629A, ICD-10-D-S93691A, ICD-10-D-S93692A, ICD-10-D-S93699A, ICD-10-D-M24274, ICD-10-D-M24275, ICD-10-D-M24276 |
| Injury, ankle, unspecified | ICD-10-D-S99911A, ICD-10-D-S99912A, ICD-10-D-S99919A, |
| Injury, foot, unspecified | ICD-10-D-S99921A, ICD-10-D-S99922A |
| Injury, ankle, other | ICD-10-D-S99811A, ICD-10-D-S99812A, ICD-10-D-S99819A |
| Injury, foot, other | ICD-10-D-S99821A, ICD-10-D-S99822A, ICD-10-D-S99829A |
| Joint disorder, ankle/foot, other | ICD-10-D-M25871, ICD-10-D-M25872, ICD-10-D-M25879 |
| Dislocation, ankle | ICD-10-D-M24371, ICD-10-D-M24372, ICD-10-D-M24373, ICD-10-D-M24471, ICD-10-D-M24472, ICD-10-D-M24473 |
| Dislocation, foot | ICD-10-D-M24374, ICD-10-D-M24375, ICD-10-D-M24376, ICD-10-D-M24474, ICD-10-D-M24475, ICD-10-D-M24476, ICD-10-D-M24477, ICD-10-D-M24478, ICD-10-D-M24479, ICD-10-D-S93111A, ICD-10-D-S93112A, ICD-10-D-S93113A, ICD-10-D-S93114A, ICD-10-D-S93115A, ICD-10-D-S93116A, ICD-10-D-S93119A, ICD-10-D-S93121A, ICD-10-D-S93122A, ICD-10-D-S93123A, ICD-10-D-S93124A, ICD-10-D-S93125A, ICD-10-D-S93126A, ICD-10-D-S93129A, ICD-10-D-S93304A, ICD-10-D-S93305A, ICD-10-D-S93311A, ICD-10-D-S93312A, ICD-10-D-S93313A, ICD-10-D-S93314A, ICD-10-D-S93315A, ICD-10-D-S93316A, ICD-10-D-S93324A, ICD-10-D-S93325A, ICD-10-D-S93326A, ICD-10-D-S93334A, ICD-10-D-S93335A, ICD-10-D-S93336A |
| Subluxation, foot | ICD-10-D-S93131A, ICD-10-D-S93132A, ICD-10-D-S93133A, ICD-10-D-S93134A, ICD-10-D-S93135A, ICD-10-D-S93136A, ICD-10-D-S93139A, ICD-10-D-S93141A, ICD-10-D-S93142A, ICD-10-D-S93143A, ICD-10-D-S93144A, ICD-10-D-S93145A, ICD-10-D-S93146A, ICD-10-D-S93149A, ICD-10-D-S93301A, ICD-10-D-S93302A, ICD-10-D-S93321A, ICD-10-D-S93322A, ICD-10-D-S93323A, ICD-10-D-S93331A, ICD-10-D-S93332A, ICD-10-D-S93333A |
ACL, anterior cruciate ligament; ICD-10, International Classification of Diseases, Tenth Revision; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament.
Presented at the annual meeting of the AOSSM, Denver, Colorado, July 2024.
Final revision submitted April 8, 2025; accepted May 6, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.L. has received other professional activities/other intellectual property from Arthrex. A.S. has received consulting fees from Medacta USA and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.