
Abstract
Background:
Intra-articular injections of autologous platelet-rich plasma (PRP) have been shown to reduce joint pain in many patients with mild to moderate knee osteoarthritis (OA) (PRP responders). However, for unclear reasons, 20% to 30% of patients experience little to no improvement in symptoms (PRP nonresponders). Understanding the mechanisms underlying PRP's action is crucial to address this limitation. In vitro and animal studies suggest that the benefits of PRP in knee OA are partly attributable to exosomes secreted by platelets and other cells.
Purpose/Hypothesis:
This study aimed to (1) determine the effects of intra-articular PRP injections in patients with symptomatic knee OA on pain and physical function, and (2) evaluate whether PRP exosome concentration and size were associated with therapeutic efficacy. Responsiveness to PRP therapy in patients with knee OA may be related to exosome concentration and size.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 60 patients seeking nonsurgical treatment of symptomatic mild to moderate knee OA—Kellgren-Lawrence (KL) grades 1 to 3—were prospectively enrolled in the study. Baseline descriptive and health data were collected, including patient-reported pain and functional outcomes at baseline, 6 weeks, and 12 weeks after injection. PRP responders were defined as patients with ≥20% reduction in the Numerical Rating Scale (NRS) of joint pain at 12 weeks after treatment. Exosome size and concentration and platelet concentration were measured in each sample. Logistic regression was used to explore relationships between responder status and patient factors—age, body mass index (BMI), sex, and KL grade. The mean exosome size and concentration were also compared between responders and nonresponders using an independent t-test.
Results:
Of the 58 patients included in the analyses, 43 (73%) reported a 20% reduction in NRS scores. The mean exosome size among a subset of patients who reported unacceptable pain symptoms before treatment (n = 43) was 80.8 ± 2.7 nm for responders and 78.0 ± 1.5 nm for nonresponders, a statistically significant difference (P = .005). There was no significant difference between responders and nonresponders in terms of platelet or exosome concentration. Age, BMI, sex, and KL grade were not significantly associated with the odds of PRP treatment response (all P > .05).
Conclusion:
PRP-derived exosome size appears to be associated with improvements in pain at 12 weeks after injection.
Introduction
Osteoarthritis (OA) is one of the most frequently treated musculoskeletal disorders and is a leading cause of chronic pain and long-term disability in adults. 27 It can affect any joint in the body; however, OA most commonly affects the knee. 40 The prevalence of knee OA continues to rise due to an aging and increasingly obese adult population, with a projected 855% increase in demand for total knee arthroplasty by 2050. 15 Current estimates indicate knee OA contributes to ≥$27 billion in health care spending annually, resulting in increased financial burden for patients and the health care system as a whole. 23 Furthermore, reduced activity as a consequence of knee OA likely contributes to other morbidities.
Treatment options for knee OA vary depending on patient symptoms, degree or grade of OA, most frequently assessed by the Kellgren-Lawrence (KL) grading system, 18 and other patient-related factors. Nonoperative management is typically pursued before surgical considerations, with options including weight loss, exercise, physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), and intra-articular injection of steroids or hyaluronic acid.7,19 An increasingly popular treatment option for nonsurgical management of knee OA is intra-articular platelet-rich plasma (PRP) injection, which has demonstrated promising results despite the current exclusion from clinical practice guidelines.7,19,25,26,27 PRP is a heterogeneous autologous blood product, containing a high concentration of platelets. 9 This isolate is believed to promote tissue healing and joint homeostasis through a complex mechanism of immunomodulation, cell signaling, and anti-inflammatory effects induced by platelet activation, as well as exosomes that contain growth factors, proteins, nucleic acids, and other small molecules that augment the intra-articular environment.6,37,38
Exosomes are small, lipid-bound extracellular vesicles that exist within PRP and have been investigated as a possible therapeutic agent responsible for the effectiveness of PRP in treating OA.21,22,43,44 Several studies have suggested that PRP-derived exosomes decreased inflammation and chondrocyte apoptosis while promoting articular cartilage repair in both in vivo animal studies and in vitro studies of human chondrocytes.29,30
Although PRP and its associated exosomal contents are an emerging area of interest with respect to the possible mechanism of action of PRP, few studies have examined the potential role of exosomes within PRP on treatment effects in patients. Thus, this study aimed to (1) determine the effects of intra-articular PRP injections in patients with symptomatic knee OA on pain and physical function, and (2) evaluate whether PRP exosome concentration and size were associated with therapeutic efficacy.
Methods
Patient Enrollment
The patients enrolled in this study were treated in the Iowa Department of Orthopedics and Rehabilitation Sports Medicine Clinic from May 17, 2022 to July 25, 2023. Eligible patients were adults referred to our center for symptomatic knee OA, defined as self-reported knee pain ≥3 on the Numerical Rating Scale (NRS, 0-10), with a KL grade 1 to 3 in the symptomatic knee(s). To confirm the KL grade and assess that pain was likely intra-articular based on physical examination and imaging, patients were evaluated by fellowship-trained sports medicine physicians and orthopaedic sports medicine physicians (K.R.D., M.M.H., R.C.K.) prior to enrollment. Patients with bilateral knee symptoms were included if both knees were symptomatic and met these criteria. Patients with inflammatory arthritis, KL grade 4 OA, or hematologic malignancy were excluded. All patients meeting the criteria were prospectively enrolled, and all data were prospectively collected. Institutional review board (IRB) approval was obtained, and all participants provided informed consent using IRB-approved consent forms. After PRP treatment, participants attended scheduled clinic visits at 6 and 12 weeks after injection.
Treatment
PRP Preparation and Injection
Patients were asked to avoid NSAIDs for 1 week before the scheduled procedure. PRP was prepared using 54 mL of whole blood obtained using an 18 ga needle via the antecubital fossa. The whole blood was combined with 6 mL Anticoagulant Citrate Dextrose Solution, Solution A (Citra Labs). For bilateral treatment, twice the volume of blood was drawn and divided into 2 aliquots of 54 mL each. This was then processed via centrifugation using the GPS III system (Zimmer Biomet) at 3200 rpm for 15 minutes and prepared with the GPS III system (Zimmer Biomet), yielding a leukocyte-rich PRP (LR-PRP). No exogenous activation methods were used. Within 20 minutes of processing, 5 mL of PRP was injected under ultrasound guidance with either a 27g 1.25 in, 25g 2 in, or 22g 2.5 in needle, using a standard in-plane, superior lateral approach into the suprapatellar recess of the knee joint. Excess LR-PRP was immediately processed for exosome isolation and characterization of the size and concentration as described below.
Postinjection Protocol
Participants were instructed to rest the knee for 2 to 3 days after injection and avoid excess activity over the first 2 weeks. Normal day-to-day activities were allowed as tolerated. Impact and heavy use (eg, running or heavy lifting) were not recommended for at least 4 to 6 weeks, at which time participants were allowed to gradually progress back to desired activities based on pain. Participants were asked to avoid NSAIDs for at least 2 weeks after the injection and up to 6 weeks if tolerable.
Measurements
Anthropometrics/Descriptive Data
Heights and weights were collected, and body mass index (BMI) was calculated. Heights were collected using a Seca telescopic height measuring rod at the baseline visit and reported in centimeters. Weights were collected at each visit on an SR Instruments digital stand-on scale (reported in kg). Participants were asked to provide their race, ethnicity, highest level of education, and pain medication use for symptomatic knee OA of the index knee.
Radiographs
Standard anterior-posterior, posterior-anterior flexion, lateral, and Merchant view radiographs were obtained. Knee radiographs were taken at baseline assessment prior to enrollment and graded using the KL criteria 14 by the principal investigator (K.R.D.).
Patient-Reported Outcome Measures
NRS of Knee Pain. Pain severity (worst and average) was measured using the pain NRS. 2 This scale ranges from 0 to 10, with higher values indicating greater pain severity. Participants were asked to rate the amount of knee pain in the past 24 hours before each visit. Participants who experienced a ≥20% decrease in the worst NRS score from baseline to 12 weeks after treatment were defined as PRP responders. 11
Pain Catastrophizing Scale
The Pain Catastrophizing Scale (PCS) consists of 13 items that result in a total score ranging from 0 to 52, with higher values indicating more pain catastrophizing. 36
Knee injury and Osteoarthritis Outcome Score
Knee injury and Osteoarthritis Outcome Score (KOOS) scores were reported for the Activities of Daily Living (ADL) and Pain health domains. 32 .
Patient-Reported Outcomes Measurement Information System Instruments
Patient-Reported Outcomes Measurement Information System (PROMIS) instruments are nondisease-specific measures of health domains.8,42 Higher scores indicate more of the measured health domain.
Marx Activity Rating Scale
The Marx Activity Rating Scale (MARS) measures activity levels of patients with knee disorders. Scores range from 0 to 16, with higher values indicating a greater level of activity. 24
Patient-Acceptable Symptom State
The Patient-Acceptable Symptom State (PASS) is defined as the value beyond which patients consider themselves well. 39 Participants were asked to indicate whether or not their current state is satisfactory, considering all the activities they have in daily life, the level of pain, and functional impairment.
Global Rating of Change
The Global Rating of Change (GROC) is a single question where participants are asked to rate their response to treatment. It was used to evaluate perceived change in knee status from PRP treatment. 16
Physical Performance
Five times sit-to-stand times (5XSTS) is a timed chair-stand test that was utilized as a measure of physical performance.1,5 Tests were conducted at baseline and the 12-week follow-up visit.
Exosome Isolation and Characterization
A total of 54 mL of whole blood was collected from each patient. The volume remaining after PRP treatment (2 mL) was utilized for platelet counts, exosome isolation, and analysis. Platelets were counted using a hemocytometer. Samples were then centrifuged at 3000 g for 15 minutes to remove residual cells (platelets and leukocytes). The supernatant was next mixed with ExoQuick (System Biosciences) reagent and incubated for 30 minutes at 4°C to isolate exosomes according to the manufacturer's instructions. The exosome concentration and size after the exosome isolation were determined using microfluidic resistive pulse sensing (MRPS) on a nanoparticle analyzer (nCS1). In brief, PRP exosomes were mixed with reference beads and loaded into the C-400 cartridge, which is suitable for quantifying particles in the 65 to 400 nm range. Exosomes that are <65 nm are not detected by the system. The cartridge was inserted into the instrument, and physical characteristics were measured at a voltage of 4 V. Results were reported for platelet concentration as well as exosome concentration and size (small, large, or average).
Exosome surface markers were characterized by immunoblotting using the Exo-Check antibody array assay (System Biosciences). The array includes epithelial cell adhesion molecule, flotillin 1, tumor susceptibility gene 101, intracellular adhesion molecule, ALG-2 interacting protein X, cluster of differentiation proteins 63 and 81, annexin 5, and Cis-Golgi matrix protein (GM130). Serum-derived exosomes serve as a positive control. The absence of a cellular contamination marker, GM130 (negative control), indicates purity, and serum-derived exosomes serve as a positive control.
Exosome uptake by human chondrocytes was confirmed by labeling exosomes with PKH67, a fluorescent lipophilic dye (Millipore Sigma), then incubating cells for 24 hours in culture medium containing the labeled exosomes. Exosome uptake was imaged on an Olympus FV1000 confocal microscope (Olympus America). A Hitachi HT7800 transmission electron microscope (TEM) was used to image PRP-derived exosomes (Hitachi High Tech).
Statistical Analysis
Before participant enrollment, a sample size calculation was performed to determine the minimum number of participants needed to detect a significant odds ratio (OR) for the relationship between exosome size and concentration and the odds of a good response to PRP treatment. Using pilot data obtained from patients with knee OA at our center that showed a mean ± standard deviation exosome concentration of 3.02 ± 2.02 x 1011/mL, we determined that a sample size of 60 participants would provide >90% power (alpha = .05, 2-sided test) to detect an OR of at least 1.5. The primary outcome of interest was response to PRP based on an NRS pain score.
Descriptive statistics of participant baseline characteristics were performed for all participants and categorically by responder status. Continuous data were summarized as mean ± standard deviation or as medians (interquartile range [IQR]) if skewed or not normally distributed. Categorical data were summarized as frequencies (percentages). Baseline differences between groups were evaluated using chi-square tests for categorical variables and independent t-tests or Wilcoxon Rank Sum tests for continuous variables with and without normal distributions, respectively. Logistic regression was used to model the relationship between the odds of PRP response and exosome number. The same analytic methods were used to explore relationships between responder status and patient factors that could be associated with it, including patient age, BMI, sex, and KL grade. Based on the rule of thumb that, on average, the minimum ratio of events to variables is 10 to 1 for obtaining reliable models, a sample size of 60 participants and an expected response rate of 80% would allow for a 4 to 5 predictor model. In sensitivity analyses, we evaluated additional indicators of treatment response at 12 weeks after treatment, including the presence of a PASS and a GROC score that corresponded with a good to excellent treatment response. In accordance with guidance from the OMERACT-OARSI (Outcome Measures in Rheumatology-Osteoarthritis Research Society International) task force for assessing efficacy in OA clinical trials, 31 data were analyzed with and without patients who reported PASS at baseline. The cohort of patients reporting PASS at baseline ultimately consisted of 9 out of 42 responders (21.4%) and 7 out of 16 nonresponders (43.8%).
Our secondary outcome, change in knee physical function, was based on the 5XSTS. A multivariable generalized linear model was planned to be constructed with the change from baseline to week-12 5XSTS time as the dependent variable. We first explored associations between change in 5XSTS time and our main predictor variable, mean exosome number, as well as participant characteristics in univariate analyses. Variables having a univariate test result with a P value of at least 0.2 were considered for inclusion in the multivariable model. Model fit was evaluated using the Akaike Information Criterion. Analyses were performed using SAS statistical software Version 9.4 (SAS Institute Inc). Independent t tests were also used to compare the mean exosome size and concentration between responders and nonresponders. Linear regression was used to evaluate the relationships between platelet counts and exosome concentration using GraphPad Prism software (GraphPad Software).
Results
Clinical Study
Baseline Assessments
Anthropometrics/Demographics. A total of 60 participants were enrolled in this study. Two participants were later excluded: 1 patient experienced a nontreatment-related fall and knee injury that required surgery before the study conclusion, and 1 patient was determined to have a KL grade 4 knee OA during a post hoc radiographic review, resulting in a sample size of 58 (40% women).
The mean age and BMI were 55.5 ± 11.3 years and 31.4 ± 7.1 kg/m2, respectively (Table 1). Participants were predominantly Caucasian (98%), mostly inactive (median [IQR] MARS score, 2 [0-7]), and the majority had a higher education level, with 71% reporting a Bachelor's degree or higher. A total of 21 participants (36%) had bilateral treatment, and 16 (28%) reported PASS prior to treatment.
Descriptive and Baseline Data for PROMs and 5XSTS Times for All Participants (n = 58) a

Data are presented as n (percentage), mean ± SD or median (IQR). ADL, activities of daily living; BA, Bachelor's degree; BMI, body mass index; 5XSTS, 5 times sit to stand times; IQR, interquartile range; KL, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; MARS, Marx Activity Rating Scale; NRS, numerical rating scale; PASS, Patient Acceptable Symptom Scale; PCS, Pain Catastrophizing Scale; PROM, patient-reported outcome measure; PROMIS, Patient-Reported Outcomes Measurement Information System.
Patient-Reported Outcomes
PROMIS scores for self-efficacy and social health were in the normal-mild range (44.6 ± 6 and 45.4 ± 8.1, respectively), while physical function scores indicated mild-moderate impairment (43.4 ± 6.6) (Figure 1).
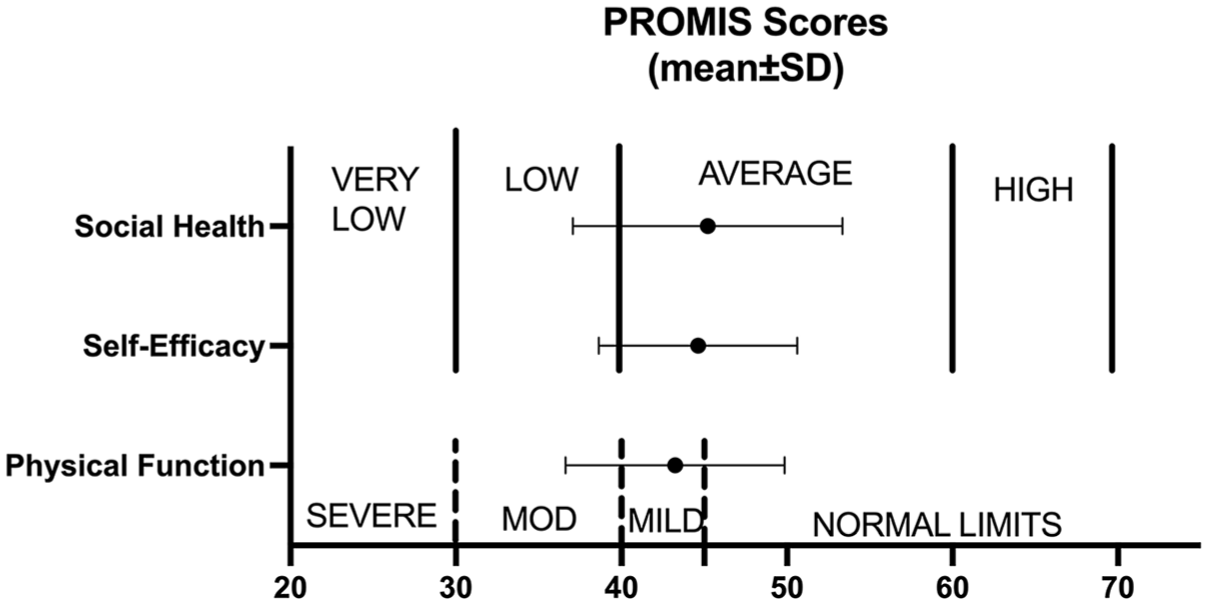
Distribution of PROMIS scores. Means and standard deviations for social health, self-efficacy, and physical function are presented, with 28.8% reporting low social health, 25.4% (n = 15) reporting low self-efficacy, and 37.3% (n = 22) reporting a low level of physical function. PROMIS, Patient Reported Outcomes Measurement Information System.
The median (IQR) PCS score was 8 with a range of 4 to 19. Only 3 participants (5%) met the clinical threshold for high levels of catastrophizing. The mean KOOS-ADL and Pain subscale scores were 70.4 ± 16.4 and 59.7 ± 13.6, respectively. Further evaluation of KOOS scores revealed that 5 participants (9%) reported moderate levels of impairment in performing knee-related ADLs, and 12 (21%) reported moderate levels of knee-related pain. A total of 22 patients (38%) were found to have a 5XSTS time of >11.4 seconds, slower than the average for 60 to 69-year-olds. 5 There were no significant differences between responders and nonresponders with respect to baseline characteristics (Table 1).
Relationships Between Baseline Measures and Odds of Nonresponse to PRP
Results of univariate logistic regression analyses showed no significant associations between the odds of nonresponse and demographic characteristics or baseline measurements, including exosome size and concentration (Figure 2A). However, excluding participants who reported PASS at baseline, we found that the mean exosome size was significantly associated with higher odds of response (OR, 0.62 [95% CI, 0.42-0.91]; P = .015) (Figure 2B). The same results were found after evaluating forward selection to construct a multivariable model.

Univariate relationships between baseline characteristics and odds of positive PRP response. ORs with 95% CIs are presented, with (A) including all patients (N = 58) and (B) excluding baseline PASS patients (n = 42). The mean exosome size correlated significantly with OR among PASS-at-baseline participants (P = .015). OR, odds ratio; PASS, Patient Acceptable Symptom State.
Baseline to Week 12 Changes in Outcomes
As expected, responders versus nonresponders experienced greater improvements in self-reported level of physical function (PF) (PROMIS-PF: 4.8 ± 5.4 vs 1.3 ± 5.5; P = .029), self-efficacy (SE) (PROMIS-SE: 7 ± 7.9 vs 0.6 ± 5.1; P < .001), satisfaction with social roles (Soc) (PROMIS-Soc: 8.2 ± 9.3 vs 1.1 ± 7.7; P = .008), and ability to perform knee-related ADL (KOOS-ADL: 14.4 ± 12.9 vs 3.9 ± 12.9; P = .007), respectively (Figure 3). Likewise, responders versus nonresponders showed a greater reduction in 5TSTS times (median [IQR]: 1.65 vs 0.6; P = .022). However, there were no significantly greater reductions in total PCS scores between responders and nonresponders (−5 vs −3.5; P = .207) (Figure 4).

Changes in PROMIS scores by responder status. Changes from baseline to 6 and 12 weeks after treatment for responders (circles) and nonresponders (boxes). (A) Physical function. (B) Self-efficacy. (C) Satisfaction with social roles. Means ± standard deviations are presented. P values indicate the significance of differences between the groups at 12 weeks. PROMIS, Patient Reported Outcomes Measurement Information System.

Changes in KOOS, 5XSTS, and PCS scores by responder status. Changes from baseline to 6 and 12 weeks after treatment for responders (circles) and nonresponders (squares). (A) KOOS-ADL scores. (B) 5XSTS times (seconds). (C) PCS scores. P values indicate the significance of differences between the groups for each assessment at 12 weeks. ADL, activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; 5XSTS, 5 Times Sit-to-Stand Test; PCS, Pain Catastrophizing Scale.
Unilateral Versus Bilateral Treatment
Of the 58 participants, 37 had unilateral treatment and 21 had bilateral treatment. KOOS-ADL scores were significantly lower in the bilateral group (73.9 ± 16.4 vs 64.3 ± 14.8; P = .030). No other PROMs differed significantly, and there was no significant difference in response rate between the 2 groups (73% vs 71%; P = .899).
PASS at Baseline
A minority of patients (n = 16) reported PASS at baseline. The cohort exhibited significantly lower BMI than other participants (26.6 ± 3.6 vs 33.3 ± 7.3 kg/m2; P≤ .001) and were predominantly male (62% vs 31%; P = .028). PCS scores were significantly lower in the PASS at baseline cohort (7.1 ± 5.7 vs 13.8 ± 11.6; P = .033), significantly higher MARS activity scores (6.2 ± 5.6 vs 3 ± 4.2; P = .030.031), and significantly higher KOOS-ADL scores (78 ± 15.1 vs 67.5 ± 16.1; P = .028). PROMIS scores were also significantly higher in the PASS at baseline cohort (PF: 47.9 ± 7 vs 41.6 ± 5.6; P < .001; SE: 49.4 ± 9.4 vs 42.8 ± 5.2; P < .001; SoC: 53 ± 8 vs 45.8 ± 6; P≤ .001). The mean NRS scores were significantly lower in the PASS at baseline cohort (2.3 ± 0.9 vs 3.6 ± 2.2; P = .030.030).
Exosome Characterization
Immunoblot analysis showed that exosomes isolated by the precipitation method were positive for exosome-specific protein markers and were not contaminated with cellular protein (Figure 5A). Densitometric analysis of exosome immunoblots from 3 different patient PRP samples gave consistent results (Figure 5B). Signals for all exosome markers were significantly above background (blank 0.05), whereas the signal for the intracellular protein (GM130) was not (P = .156). Cell culture experiments also demonstrated that PRP exosomes were internalized by human chondrocytes, a requirement for biologic activity (Figure 5, C and D).

Exosomes isolated from PRP display canonical protein markers and are taken up by human chondrocytes. (A) The representative Exo-Check antibody array confirms the presence of exosome markers (EPCAM, FLOT1, TSG101, ICAM, ALIX, CD63, CD81, and ANXA5) and the absence of a cellular contamination marker (GM130). Serum-derived exosomes serve as a PC. (B) Densitometric analysis of immunoblots of PRP exosomes from 3 different patients (means ± SD). (C) Confocal imaging of chondrocytes after exposure to unlabeled exosomes and (D) green fluorescent-labeled exosomes. Cells were counterstained with DAPI to identify nuclei (blue). Scale bars = 100 μm. ALIX, ALG-2 interacting protein X; ANXA5, annexin 5; CD63 and CD81, cluster of differentiation proteins 63 and 81; EPCAM, epithelial cell adhesion molecule; FLOT1, flotillin 1; GM130, Cis-golgi matrix protein; ICAM, intracellular adhesion molecule; PC, positive control; PRP, platelet-rich plasma; TSG101, tumor susceptibility gene 101.
MRPS analysis showed heterogeneity in exosome sizes, which ranged from 60 to 115 nm (Figure 6A). The distribution of measured exosomes was unimodal and non-Gaussian, with the largest population of exosomes in the 70 to 75 nm range (24.6% ± 3.8%). Replicate analyses of the same sample showed that the measurements were highly reproducible (Figure 6B). TEM imaging revealed that exosomes were intact and confirmed size variability (Figure 6C).

Size and morphology of PRP exosomes. (A) Size distribution determined by MRPS for all 60 PRP samples (mean ± SD). (B) Replicate MRPS measurements (n = 8) of exosome sizes in a single PRP sample (mean ± SD). (C) A TEM image showing typical exosome morphology (scale bar, 200 nm). The white arrow points to a large exosome (~100 nm in diameter) and the grey arrow to a small exosome (~70 nm in diameter). An exosome that appears <60 nm is circled. Such smaller objects were not detected by MRPS. MRPS, microfluidic resistive pulse sensing; PRP, platelet-rich plasma; TEM, transmission electron microscopy.
Total exosome concentrations varied over a 10-fold range, and the mean concentration of small exosomes (<90 nm) comprised 80% of the total.
Exosome Versus Platelet Concentration
There were no significant correlations between exosome and platelet concentrations, including when accounting for exosome size (r2 < 0.02) (Figure 7). These findings suggest that leukocytes present in LR-PRP contribute to exosome content.

Low correlation between platelet and exosome counts. Linear regression analysis of platelet versus exosome concentrations among all participants. (A) Platelets versus total exosomes (small + large). (B) Platelets versus small exosomes. (C) Platelets versus large exosomes. Correlation coefficients (R2 values) of <0.02 indicate no correlation between the variables.
Relationships Between PRP Responses and Exosome Characteristics
Neither exosome size nor concentration was associated with age, BMI, sex, or KL grade. There was no significant difference in exosome size between responders and nonresponders (P = .204) (Figure 8A). In addition, no significant differences were observed between responders and nonresponders with regard to exosome concentration (Figure 8B) or the ratio of small to large exosomes (Figure 8C). Among the 16 patients who reported PASS at baseline, only 56% were found to be responsive at the 12-week follow-up, which was in contrast to the overall response rate of 72% for all 58 patients. These findings underscore difficulties in detecting a ≥20% improvement when NRS scores at baseline were already comparatively low. In the sub-analysis excluding patients who reported PASS at baseline, significantly larger exosome size (80.8 ± 2.7 nm vs. 78.0 ± 1.5 nm; P = .005) was noted in responders in addition to further correlations between response and exosome size but not exosome concentration (Figures 8, D, E, and F).
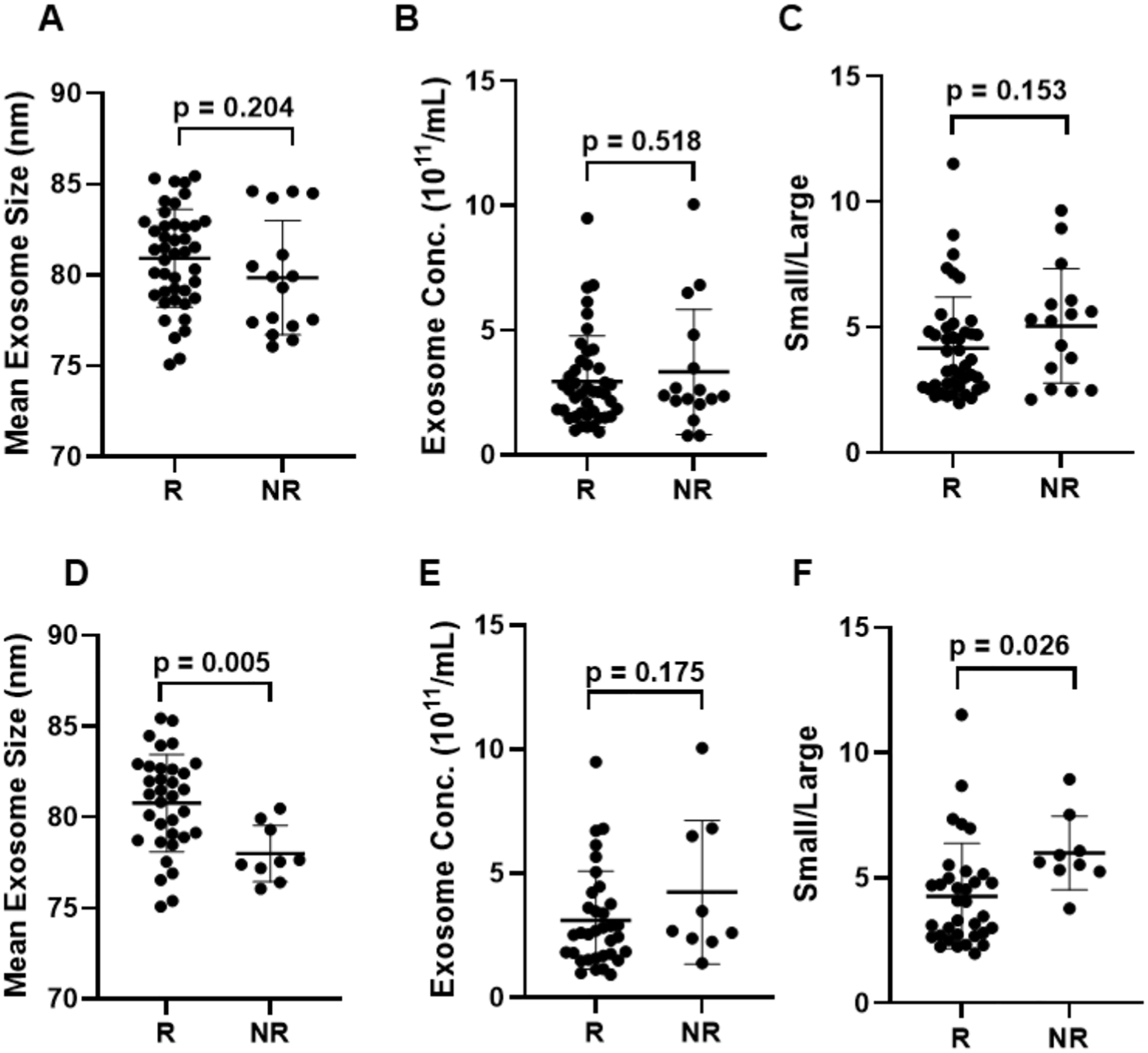
Relationships between PRP response and exosome size and concentration. (A and D) Differences between R and NR with respect to mean exosome size, (B and E) exosome concentration (all sizes), and (C and F) the ratio of small to large exosomes (small/large). (A, B, and C). Analysis with PASS at baseline, patients included. (D, E, and F). Differences with PASS at baseline, patients excluded. Horizontal lines and error bars represent means and standard deviations, and P values show the results of t tests. Additional analyses using alternative definitions of PRP responder, including PASS at 12 weeks, decreases in 5XSTS times of ≥33%, and GROC score ratings of “excellent” at 12 weeks, indicated significant relationships between exosome size and these parameters (Table 2). 5XSTS, 5 times sit to stand times; GROC, global rating of change; N, nonresponders; PASS, Patient Acceptable Symptom State; PRP, platelet-rich plasma; R, responders.
Sensitivity Analyses Reveal Correlations Between Exosome Size and Multiple Definitions of Response at 12 Weeks a
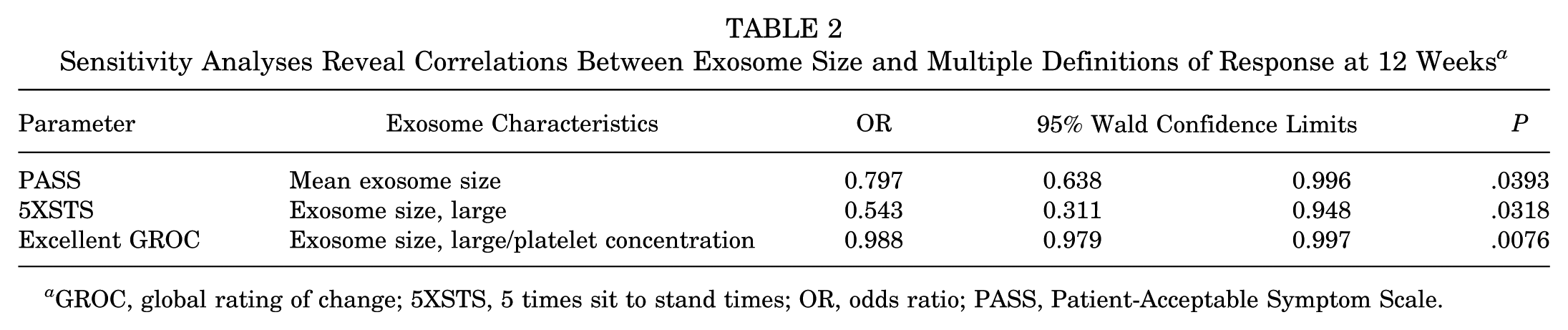
GROC, global rating of change; 5XSTS, 5 times sit to stand times; OR, odds ratio; PASS, Patient-Acceptable Symptom Scale.
Discussion
In the present study, 72% of patients with KL grades 1 to 3 knee OA achieved at least a 20% reduction in pain at 12 weeks after injection, comparable with response rates previously reported in the literature.3,7 The response rate in our study was not associated with exosome concentration, age, sex, BMI, or KL grade, and baseline PROMs—including NRS, KOOS, PROMIS, PCS, and MARS activity scores—were not predictive of responder status at 12 weeks. However, there was an interesting relationship between exosome size and outcomes at 12 weeks among a subgroup of patients who did not report PASS at baseline that is deserving of further discussion.
Clinical trials to assess the efficacy of PRP in healing tendon, ligament, muscle, and bone injuries have been conducted on the assumption that regenerative growth factors in PRP would promote tissue repair in all cases. 35 However, it has been suggested that because healing processes differ in different tissues, expectations of such broad-spectrum regenerative effects may be unrealistic. For example, PRP typically contains high levels of vascular endothelial growth factor (VEGF), an angiogenic protein that may promote bone, ligament, and muscle healing but impair cartilage regeneration. 10 This implies that PRP could be customized for treating OA by adding engineered exosomes carrying factors that suppress VEGF signaling. 13
In the present study, the mean exosome size trended larger in the responder group than in the nonresponder group. Among a subset of patients whose pain symptoms at baseline allowed for measurable improvement (n = 42), the difference in mean exosome size and the ratio of small to large exosomes between the groups was statistically significant (P = .005 and P = .026, respectively).
Exosome size was also an influential factor when alternative definitions of response were analyzed. PASS at 12 weeks, and improvements in 5XSTS times and GROC scores were significantly related to exosome size, particularly when patients reporting PASS at baseline were excluded. In general, these findings suggest that large exosome size is associated with positive responses to PRP treatment and is a deserving area for further study. Although our primary measure of PRP responsiveness was joint pain, we included functional assessments (eg, 5XSTS times) as well as assessments of global well-being (eg, PROMIS and GROC), conforming to guidance provided by the OMERACT-OARSI task force for evaluating responder status in clinical trials of OA therapies. 31
Given the complexity of PRP's cellular composition, which includes platelets as well as multiple immune cell types, the heterogeneity in exosome size we observed in LR-PRP is unsurprising. Exosomes secreted by any given cell type can vary in physical characteristics, molecular cargo, and effects on recipient cells. In 1 example, Willms et al 41 showed by sucrose gradient centrifugation that exosomes secreted by melanoma cells fall into high- and low-density fractions carrying distinct cargoes that have differing effects on endothelial cells. Moreover, exosome uptake by recipient cells is selective and depends on donor cell identity and environmental conditions. 14 It is unclear how such considerations apply to PRP therapy, as it remains to be seen if there are response-related variations in the composition of PRP-derived exosomes. 12
The efficacy of PRP injection in the treatment of knee OA remains controversial. Most studies indicate beneficial responses, while others cast doubt on its therapeutic value, with some suggesting a placebo effect.17,22-24 One confounding factor suggested by our findings could be that PRP is only an effective treatment for a subset of patients with specific health and pain profiles at baseline, and that the criteria for patient selection are inconsistent across studies. Conflicting results have also been attributed in part to differences in the methods and instrumentation used for PRP isolation. 10 For example, Rui et al 33 showed that PRP exosome sizes and protein content are affected by agents used for platelet activation, which vary among centers.
PRP generated by different methods may be leukocyte-poor or leukocyte-rich and may or may not be diluted with PPP, which may affect exosome concentration and content. In our study, the lack of correlation between exosome and platelet counts suggests a substantial contribution of leukocyte-derived exosomes, which may differ in size and composition from platelet-derived exosomes. 14 In addition, PRP responses may be affected by the concentration of platelets and injection volumes, which can vary with different processing and treatment protocols. To that point, in a recent review of 29 clinical trials of PRP for knee OA, Berrigan et al 4 concluded that blood centrifugation protocols had significant effects on platelet concentrations and outcomes.
Importantly, all PRP isolates in the present study were prepared using the same Zimmer Biomet system, which yields only leukocyte-rich PRP. Moreover, none of the isolates were treated with activators to stimulate platelet degranulation (eg, thrombin), and none were diluted with PPP; thus, the variability in response we observed is unlikely to have been due to inconsistencies in PRP processing. By the same token, the methods we used to isolate and quantify the sizes and concentrations of PRP exosomes proved to be reproducible and were applied consistently throughout this study.
There are several limitations to this study. Patients were considered to have an intra-articular source of knee pain on history and physical examination. However, extra-articular causes of knee pain that would not be expected to improve with an intra-articular intervention, such as tendinopathy and bursitis, may also be present and are difficult to delineate using the outcome measures employed in this study. Second, patients independently sought treatment or were referred by other providers for consideration of PRP. The baseline characteristics of this study suggest that those seeking treatment vary widely regarding symptomatology, as evidenced by the fact that several patients who reported “PASS” at baseline still sought treatment. To account for this, a subanalysis was performed excluding these baseline PASS patients, which is consistent with the OMERACT-OARSI task force recommendations that patients recruited for interventional trials should be demonstrably symptomatic before treatment because assessing response to an intervention is difficult when margins for detecting success are narrow or nonexistent. 31 Moreover, we did not collect information on concurrent treatments or comorbid conditions such as diabetes, hypertension, and smoking status 17 and could not rule them out as confounding factors in this study.
All available patient factors—including patient characteristics, baseline physical activity measures, and relevant comorbidities were initially evaluated in our univariate logistic regression analyses (Figure 2). After this comprehensive assessment, we employed forward selection to construct the multivariable model. Notably, only the mean exosome size retained a significant association with PRP response, indicating that, within our dataset, baseline physical activity and comorbid conditions did not contribute additional predictive value. We acknowledge that future studies with larger cohorts might further elucidate the role of these factors in treatment outcomes.
Although exosome size was determined to be important in the present study, mechanisms of action remain obscure and can only be elucidated through molecular characterization of large and small exosomal cargos, a limitation that will be addressed in future studies. The Zimmer-Biomet system used for PRP preparation in our clinic does not allow for the removal of leukocytes; however, given evidence that immune cells in LR-PRP contribute to its therapeutic effects, 20 comparing exosomes from leukocyte-rich vs leukocyte-poor PRP is of interest. Last, it will be important to determine whether the analgesic effects apparent in 12-week follow-up visits are accompanied by delays in the progression of joint degeneration as assessed over longer timeframes.
Conclusion
This study is the first to suggest that the mean exosome size is associated with improved PRP response for the treatment of mild to moderate knee OA. Although we did not characterize exosomal cargos in the present study, our finding that exosome size is associated with PRP responsiveness suggests that there may be differences in the surface characteristics and/or contents of large and small exosomes that underlie differences in their uptake and subsequent biologic effects in target cells. Future work will address these issues and determine whether differences in exosome composition influence patient responses to PRP. These efforts may lead to strategies to customize exosomes to improve outcomes in patients with OA who do not respond to conventional PRP therapy.
Footnotes
Acknowledgements
The authors thank Abbie Smith for administrative assistance.
Final revision submitted March 29, 2025; accepted April 25, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by a grant from the Orthopedic Research and Education Foundation and supported by the University of Iowa Central Microscopy Research Facility. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Iowa (institutional review board ID No.: 202205217).