
Abstract
Background:
Recent studies have emphasized the importance of lesion location and tear structure for understanding Bankart lesions; however, knowledge on anterior labroligamentous periosteal sleeve avulsion (ALPSA) lesion characteristics in anterior shoulder instability remains limited.
Purpose:
To evaluate the prevalence of various ALPSA lesion patterns and their effect on redislocation rates after labrum repair.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Patients with ALPSA lesions who underwent arthroscopic labrum repair between 2015 and 2022 were retrospectively evaluated. Labrum tears were categorized into specific positions: isolated ALPSA lesions (3- to 5-o’clock position), ALPSA lesions with tears extending to the 1 o’clock position (1- to 5-o’clock position), and ALPSA lesions with tears extending into other positions. In addition, transverse tears that disrupted the circular continuity of the labrum were defined as radial tears. Patients were categorized as having no dislocated lesions or having redislocated lesions based on postoperative redislocation history. Descriptive data, tear extensions, radial tears, and patient-reported outcome measures (PROMs) were compared between the 2 groups.
Results:
The study included 178 patients (mean age, 25.7 ± 7.1 years), with a mean follow-up of 69.4 ± 27.2 months. Of these patients, 35 experienced lesion redislocation, while 143 patients did not experience lesion dislocation. In patients with no lesion dislocation, 43% of lesions were located in the 1- to 5-o’clock position, 36% in the 3- to 5-o’clock position, and 21% in other locations; in patients with lesion redislocation, 60% of lesions were observed in the 3- to 5-o’clock position, 29% in the 1- to 5-o’clock position, and 11% in other locations (P1-5 = .04, P3-5 = .001, and Pothers = .08). Radial tears were more frequent in the group with lesion redislocation (49%) compared with the group with no lesion dislocation (23%) (P < .001). Regression analysis demonstrated that radial tears (odds ratio [OR], 4.67) and the 3- to 5-o’clock lesion position (OR, 3.65) were significantly associated with redislocation (P = .01, P = .03, respectively). Both groups demonstrated significant improvements in PROMs compared with the preoperative period (P < .001). However, final follow-up PROMs were significantly worse in the group with lesion redislocation (P < .001).
Conclusion:
The present study demonstrated that an isolated ALPSA lesion at the 3- to 5-o’clock position and the presence of radial tears were independent factors increasing the risk of redislocation after arthroscopic ALPSA repair.
Keywords
The anterior labroligamentous periosteal sleeve avulsion (ALPSA), initially described by McLaughlin and Maclellan 16 in 1960, was subsequently explained by Neviaser 20 as a significant factor in recurrent anterior shoulder instability in 1993. In contrast to the Bankart lesion, the ALPSA lesion is characterized by the medial and inferior displacement of the anteroinferior labrum along with the scapular periosteum. 22 In the literature, ALPSA lesions have been associated with chronic recurrent shoulder instability as well as greater humeral and glenoid bone loss.7,21,23 Also, ALPSA lesions have been repeatedly identified as a risk factor for recurrent shoulder instability after arthroscopic shoulder stabilization.10,21,25,28
Studies demonstrated that patients with ALPSA lesions have nearly double the recurrent instability rate compared with those undergoing standard arthroscopic Bankart repair.3,21 On the other hand, several studies have reported that the presence of an ALPSA lesion is not a predictive factor for failure when compared with arthroscopic Bankart repair.12,26 Also, the reported recurrence rates in the literature3,13,26 vary on a broad interval, ranging from 7.7% to 32%. The phrase "one size does not fit all" may provide a logical explanation for the variability in outcomes. ALPSA lesions may vary in tear extensions and characteristics, necessitating a detailed and individualized description. Recent studies have emphasized the importance of labrum lesion location in understanding and classifying Bankart lesions; however, research on the relationship between ALPSA lesion characteristics and clinical outcomes in anterior shoulder instability remains limited.1,17 Understanding the tear extension and characteristics of ALPSA lesions is important to determine the prognosis of shoulder stability and the selection of the most effective treatment modality.
Therefore, the main objective of the presented study was to evaluate the prevalence of various ALPSA lesion patterns and assess their effect on redislocation rates after labrum repair. We hypothesized that the tear characteristics of the ALPSA lesion would affect the clinical outcomes and the recurrent instability rates after arthroscopic labrum repair.
Methods
Institutional review board approval was received from the Gazi University Ethics Committee (Protocol: 2024-1385). The study adhered to the guidelines of the World Medical Association’s Declaration of Helsinki.
Patient Selection
Patients who were admitted to the institution with a diagnosis of labrum tears and underwent arthroscopic surgery by a single senior surgeon (U.K.) between February 2015 and August 2022 were retrospectively evaluated. The data of 1053 patients were collected prospectively. The inclusion criteria were as follows: (1) patients with ALPSA lesions that were managed arthroscopically; (2) patients with a minimum follow-up of 2 years; and (3) patients with adequate and accessible data—such as preoperative history, surgical video recordings, and patient-reported outcome measures (PROMs)—includingoxford shoulder instability score (OSIS), subjective shoulder value (SSV), and visual analog scale (VAS) scores—and verified redislocation records. The exclusion criteria were as follows: (1) labral pathologies other than ALPSA lesions (Bankart lesions, glenolabral articular disruption lesions, and Perthes lesions); (2) patients with concomitant pathologies (rotator cuff tears, long head of biceps pathologies, and glenohumeral arthritis); (3) patients with off-track or engaging Hill-Sachs lesions (determined by computed tomography using the method proposed by Di Giacomo et al 8 ); (4) patients with >13.5% glenoid defect (defect size defined as the ratio of the width of the resulting defect to the width of a best-fit circle, utilizing the inferior edge of the glenoid as a reference) 18 ; (5) revision surgeries; (6) ligamentous laxity—those with a Beighton score >3; (7) missing data; (8) patients who did not participate in the final follow-up; and (9) patients lost to follow-up. Adhering to the defined criteria, 178 patients met the requirements and were included in the study. The patient selection process is described in a flowchart in Figure 1.

Flowchart of the patient selection process. ALPSA, anterior labroligamentous periosteal sleeve avulsion; GLAD lesion, glenolabral articular disruption.
Arthroscopic Examination
To assess the labrum tears in ALPSA lesions, the surgical video recordings of patients who met the inclusion criteria were evaluated by 2 authors (T.K.E. and A.E.O.) who were blinded to patient outcomes. The evaluations were conducted on arthroscopic views obtained after the removal of synovial fibrous tissues on the retracted labrum. First, the presence of any additional tears extending from the ALPSA lesion in the labrum was evaluated. To determine labral tear locations, a clock-face reference system was established by generating a best-fit circle within the plane of the glenoid labrum. The most superior aspect of the superior labrum was established as the 12 o'clock position for further referencing. For consistent interpretation, the right glenoid was used as the template for a clockwise description of anatomic landmarks, while the clock face for the left glenoid was inverted accordingly. Labrum tears were categorized into specific positions based on their positional characteristics: isolated ALPSA lesions (3- to 5-o’clock position), ALPSA lesions with labral tears extending to the 1-o’clock position (1- to 5-o’clock position), and ALPSA lesions with labral tears extending into other positions (other locations) (Figure 2).2,6

Schematic illustration depicting the labral lesion locations and their frequencies.
Then, the anatomic continuity of the labrum, which had been displaced from its normal position and retracted medially, around the circular structure of the glenoid was assessed. Based on this evaluation, transverse tears that disrupt the circular continuity of the labrum were defined as radial tears (Figures 3 to 5). Intra- and interobserver reliability analyses were performed to obtain more consistent results in identifying radial tears and the location of labrum lesions. To assess intraobserver reliability, 1 author (T.K.E.) reevaluated all video recordings at intervals of >2 weeks from the initial evaluation. To evaluate interobserver reliability, another experienced surgeon (A.E.O.), who was unaware of the other surgeon's assessment and the patients’ clinical outcomes, independently reviewed all surgical videos in random order to identify the presence of radial tears and lesion locations.

Schematic illustration depicting the radial tear locations and their frequencies.
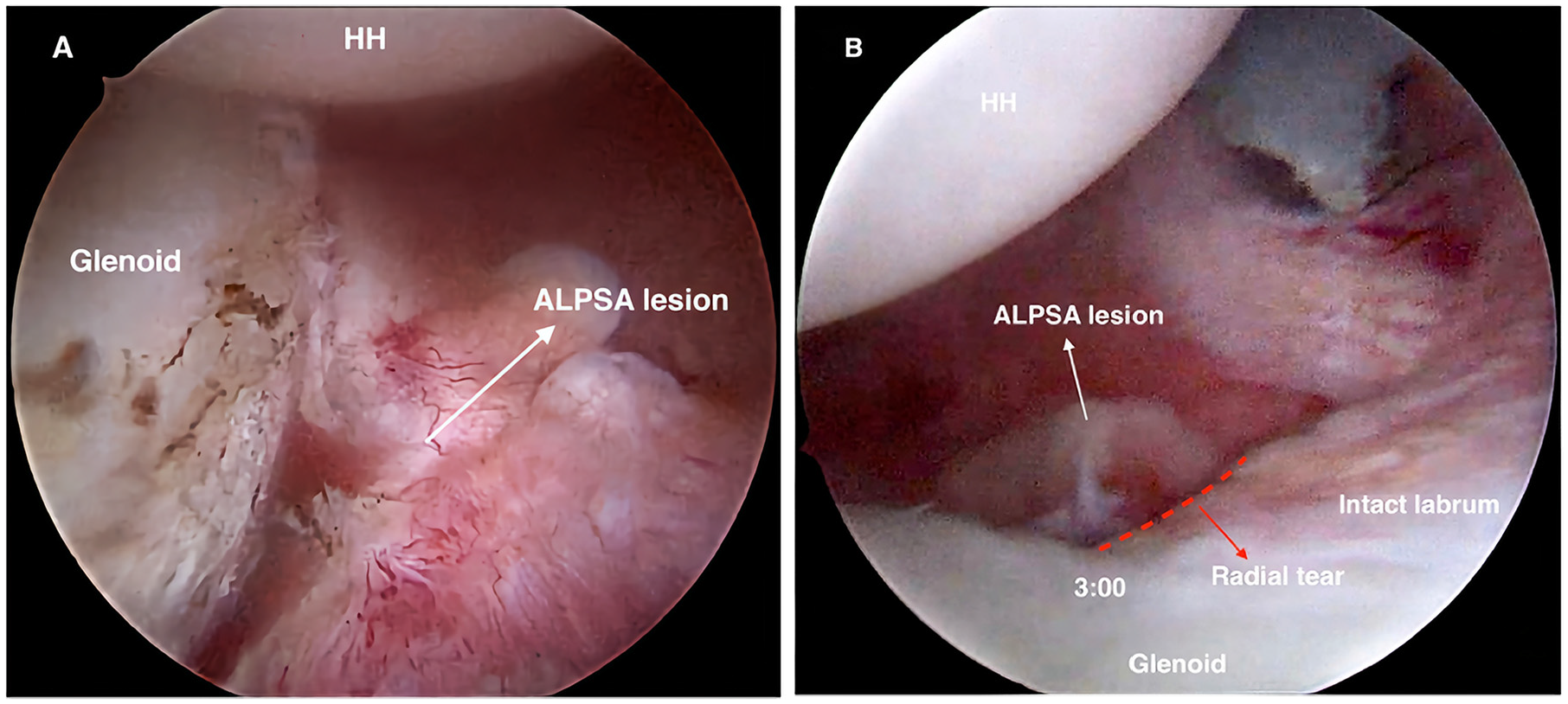
Arthroscopic view of the left shoulder, with the patient in the lateral decubitus position and the arthroscope in the (A) anterosuperior and (B) posterior viewing portals. (A) The image illustrates an ALPSA lesion viewed from the anterosuperior portal. (B) The image illustrates a radial tear at the 3 o'clock position and a retracted ALPSA lesion. ALPSA, anterior labroligamentous periosteal sleeve avulsion; HH, humeral head.
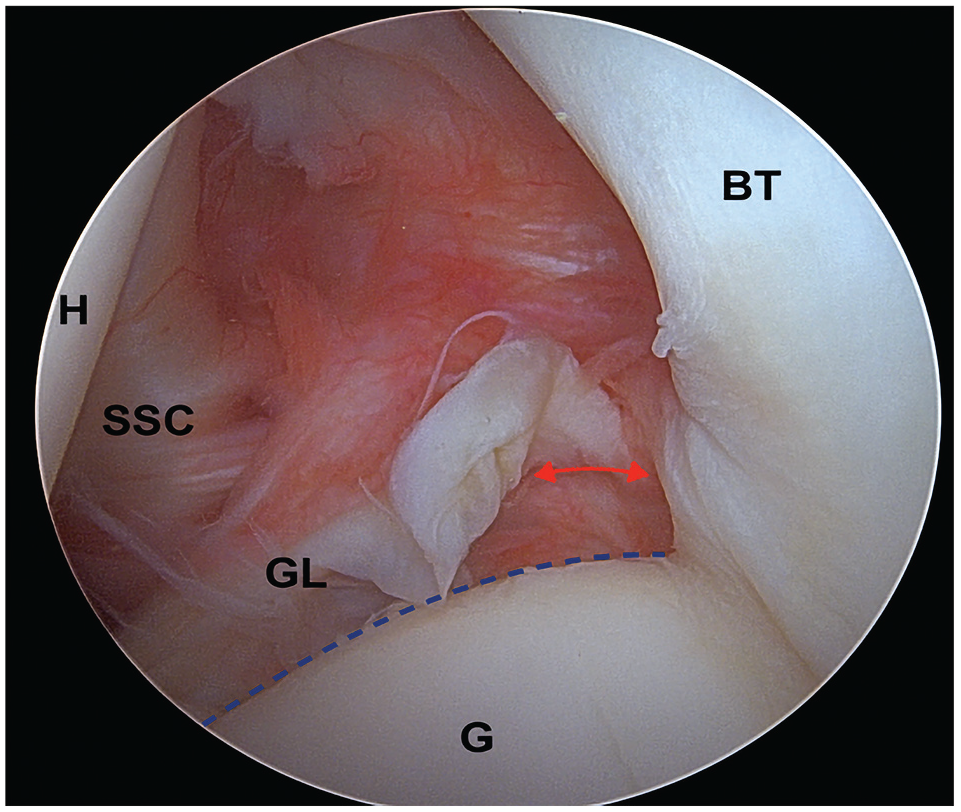
Arthroscopic view of the left shoulder, with the patient in the lateral decubitus position and the arthroscope in the posterior viewing portal. Illustration of the radial tear at the 1 o’clock position in a patient presenting with a labral tear extension. The red double-headed arrow shows a radial tear. ALPSA, anterior labroligamentous periosteal sleeve avulsion; BT, biceps tendon; G, glenoid; GL, glenoid labrum; H, humeral head; SSC, subscapularis.
Surgical Procedures
Patients were operated on in the semilateral decubitus position, which provided the orientation of the glenoid fossa parallel to the ground with the arm at 45° of abduction and 15° of flexion <10 lbs of longitudinal traction on a shoulder holder. All surgical procedures were performed with the patient under interscalene block with or without general anesthesia. Initially, the arthroscope was inserted through the posterior portal to inspect the anterior and superior labrum, which was then examined using a probe. Next, the arthroscope was placed in the anterosuperior portal to assess the inferior and posterior labrum. After the arthroscopic determination of the tear location, the labrum was released using an appropriate elevator and repositioned to the glenoid level suitable for repair. The labral tear repair was then performed using a double-loaded suture anchor (2.9 mm GRYPHON, No. 2 sutures; DePuy Mitek). In the repair of isolated ALPSA lesions, the first anchor was placed at the 5:30 position, followed by 2 additional anchors placed proximally at intervals of 8 to 10 mm. In groups with additional tear extensions, the ALPSA lesion was repaired using the same approach, with additional anchors placed at 8 to 10 mm intervals according to the extent of the tear. A simple vertical suture and a horizontal mattress suture were performed in each anchor for optimal stability. In patients with radial tears, both sutures were placed using the horizontal mattress suture technique to reunite the 2 ends of the radial tear. For tears extending superiorly with accompanying superior labrum anterior-posterior (SLAP) lesions, SLAP repair was performed. Labral repair was complete when the entire labrum was secured to the glenoid rim.
Postoperative Rehabilitation Protocol
Postoperatively, the affected arm was kept in a sling for 6 weeks. Passive shoulder, active elbow, wrist, and hand range of motion (ROM) exercises begin on days 3 to 5 after surgery. Active shoulder ROM exercises were applied starting from 4 weeks with relative immobilization. Patients were prescribed a supervised, patient-specific rehabilitation program for 8 weeks. Strengthening exercises and a gradual progress to daily activities were started after the third month.
Functional Outcome Evaluation
Patients who met the criteria were invited for a final follow-up evaluation. The patient data were collected by an author (F.A.) who was unaware of the details of the present study. The initial examination involved the assessment of patients for a history of recurrent dislocation after the primary procedure, as well as the determination of whether they had undergone a subsequent revision surgery. To assess the history of recurrent dislocations, patients were initially asked, “Have you experienced a dislocation after surgery?” For patients who responded “yes” to this question, their records in the national health database were reviewed to verify the history of redislocation. Patients whose redislocation data could not be confirmed were considered as having ’’missing data’’ and were excluded from the study. Based on the history of recurrent dislocation, the study population was classified into 2 groups: (1) Patients with no lesion dislocation and (2) patients with lesion redislocation. Shoulder function and pain levels in these groups were evaluated with the OSIS, SSV, and VAS scores.
Statistical Analysis
All statistical analyses were performed using SPSS for Mac Version 28.0 (IBM Corp). The Shapiro-Wilk test was used to assess the normality of continuous variables. Descriptive statistics were reported for the total patient cohort and stratified by the presence of redislocation. Categorical variables were analyzed using the chi-square test. For continuous variables that did not follow a normal distribution, the Wilcoxon signed-rank test was used to compare pre- and postoperative scores within the same group, while the Mann-Whitney U test was used for intergroup comparisons between patients with and without redislocation. For the logistic regression analysis, a univariate model was initially performed for each candidate variable. Variables that reached statistical significance at P < .10 in the univariate analysis were then entered into a fixed-effects multivariate logistic regression model using the Enter method. The Hosmer-Lemeshow goodness-of-fit test was employed to assess model fit, and variance inflation factors were examined to evaluate potential collinearity among predictors. An alpha of .05 was used to determine significance in the final multivariate model. Inter- and intraobserver reliability was analyzed using the kappa statistic (k) defined as k > 0.8 = excellent. 14
Results
In total, 178 patients who underwent arthroscopic ALPSA lesion repair were included in the study. The mean patient age was 25.7 ± 7.1 years (range, 14-52 years), with 159 male and 19 female patients. A total of 109 patients underwent surgery on the dominant arm, while 69 patients had surgery on the nondominant arm. The mean follow-up duration was 69.4 ± 27.2 months (range, 24-117 months).
In this study group, 36.5% of patients had isolated ALPSA lesions (3- to 5-o’clock position), 42.1% had labral tears extending to the 1 o’clock position alongside ALPSA lesions, and 21.4% had labral tears extending into other positions in addition to ALPSA lesions (Figure 2). A radial tear was identified accompanying the labrum tear in 41 patients, whereas no additional labral pathology was observed in the remaining patients. The radial tear was observed at the proximal edge of the labral lesion (eg, in lesions located between the 1- and 5-o’clock position, the radial tear, if present, was at the 1 o'clock position) (Figures 3 to 5). Overall, 15 patients exhibited a radial tear at the 1 o'clock position, while 26 patients had a radial tear at the 3 o'clock position (Figure 3). Recurrent dislocations were reported in 35 patients from the study group during the postoperative period.
No significant differences were found between the 2 groups in age, sex, dominant arm surgery, time from first dislocation to surgery, number of preoperative dislocations, follow-up duration, heaviness of work, or sports activity level (Table 1). On the other hand, the redislocation group consisted predominantly of isolated ALPSA lesions, whereas tears extending to the 1 o’clock position alongside ALPSA lesions were more commonly observed in the no dislocation group. Furthermore, radial tears were identified as significantly more common in patients with redislocation (Table 1). Logistic regression analysis revealed that radial tears and isolated ALPSA lesions were significantly associated with postoperative redislocation (Table 2). No significant relationship was observed between redislocation and age, sex, dominant arm surgery, time from first dislocation to surgery, number of preoperative dislocations, follow-up duration, heaviness of work, or sports activity level (Table 2). Intra- and interobserver agreement for labral tear localization (κ = 0.922 and κ = 0.887, respectively) and radial tear presence (κ = 0.894 and κ = 0.833, respectively) demonstrated excellent reliability, as measured by the Cohen kappa statistic.
Patient Characteristics a

Data are presented as mean ± SD or n (%). The bold P values indicate significance. Preop, preoperative.
Significant at P≤ .05.
Logistic Regression Model Predicting the Dislocation of ALPSA Lesions Based on Patient Characteristics a

The bold P values indicate significance. Exp (B), exponentiated regression; OR, odds ratio; Preop, preoperative.
Significant at P≤ .05.
Both groups demonstrated significant improvements in these PROMs compared with the preoperative period (Table 3). However, a comparison of the PROMs obtained at the final follow-up indicated that the VAS, OSIS, and SSV scores were significantly worse in the redislocation group than those in the no dislocation group.
PROMs at the Final Follow-up a

Data are presented as mean ± SD. The bold P values indicate significance. OSIS, Oxford Shoulder Instability Score; Postop, postoperative; Preop, preoperative; PROM, patient-reported outcome measures; SSV, subjective shoulder value; VAS, visual analog scale.
P for intragroup comparison of pre- and postoperative values (P≤ .05).
P for the comparison of pre- and postoperative values between the 2 groups (P≤ .05).
Discussion
The objectives of the present study were to (1) describe ALPSA lesions based on their labral tear extension and characteristics, and (2) report the clinical outcomes of patients. The analyses conducted in line with these objectives have revealed several important findings. First, unlike those previously described, ALPSA lesions are not confined to a specific location; instead, they demonstrate a wide range of labral tear extensions, which may include superior and posterior regions. Second, isolated ALPSA lesions at the 3- to 5-o’clock position and the presence of radial tears were identified as independent factors contributing to an increased risk of redislocation after arthroscopic labrum repair. Third, the assessment of functional outcomes demonstrated that patients who experienced redislocation had lower clinical scores at the final follow-up.
ALPSA lesions were classically defined as localized to the anteroinferior labrum, and previous studies on their outcomes did not provide detailed information about the tear extensions on the glenoid labrum. 23 Only 1 study, conducted by Lee et al, 15 reported that the ALPSA group had a significantly higher rate of lesion extending to the superior part at the 2 o'clock position compared with the Bankart group. However, they did not include information about the extension or frequency of injuries in other locations. The present study identified isolated ALPSA lesions at the 3- to 5 o’clock position in 65 patients. Also, ALPSA lesions with labral tear extension at the 1 o’clock position were identified in 75 patients, while superior and posterior extensions at other locations were observed in 38 patients. These findings demonstrate that ALPSA lesions are not isolated to the anteroinferior labrum and show significant variability in their possible locations. The variety of tear extensions and the high rate of involvement of multiple locations on the glenoid labrum observed in the present study highlight the importance of thoroughly investigating different lesion locations.
ALPSA lesions have been identified as a risk factor for recurrent shoulder instability after arthroscopic shoulder stabilization. Also, ALPSA lesions have been reported to be associated with a higher rate of preoperative dislocations, larger Hill-Sachs lesions, and greater glenoid bone loss compared with Bankart lesions.4,21 These factors have been suggested as potential contributors to recurrence.4,9,21 However, it has also been reported that ALPSA lesions can occur in first-time shoulder dislocations without significant bone loss.3,27 On the other hand, there are several well-known factors that contribute to recurrence after shoulder stabilization, including age, male sex, participation in collision sports, and involvement of the dominant arm.5,19,24,28 Given the variety of independent factors influencing shoulder stability, the importance of analyzing ALPSA lesion characteristics within a homogeneous cohort becomes evident. In this study, the patient population was narrowed to those with ALPSA lesions, without subcritical glenoid bone loss and off-track Hill-Sachs lesions. No differences were observed between the 2 groups regarding age, sex, hand dominance, heaviness of work, sports activity, preoperative number of dislocations, and time to surgery from the first dislocation at the final follow-up. However, 2 important parameters have been identified as risk factors for recurrent instability after arthroscopic repair of ALPSA lesions: (1) an isolated ALPSA lesion without labral tear extension, and (2) the presence of a radial tear.
Recent literature has emphasized the importance of comprehensively evaluating all portions of the glenoid labrum to eliminate recurrent instability and improve clinical outcomes. Similarly, the variety of tear patterns and the high rate of involvement of various locations on the glenoid labrum observed in the present study revealed the effect of different ALPSA lesion locations on clinical outcomes. Our findings indicated a significant association between isolated ALPSA lesions at the 3- to 5-o’clock position and a higher risk of redislocation after arthroscopic labrum repair. Biologically, the 3- to 5-o’clock region has been shown to have good vascularity and cell composition. 11 However, this seemingly counterintuitive result can be explained physically; (1) in an isolated ALPSA lesion at the 3- to 5-o’clock position, the entire loading force is concentrated on a small area through the inferior glenohumeral ligament, increasing the load per unit area, and (2) a smaller contact area may diminish the healing capacity because of relatively higher tensile forces. These factors could lead to a heightened risk of redislocation. In accordance with these hypotheses, the results revealed that a patient with an isolated ALPSA lesion at the 3- to 5-o’clock position had a 3.65-fold higher risk of redislocation compared with a patient with a lesion in other areas.
Another major finding was that the presence of the radial tear is also a significant independent risk factor for redislocation. The presence of a radial tear increases the likelihood of redislocation in patients with ALPSA lesions after repair compared with structurally intact ones. A possible explanation is that radial tears of the labrum disrupt the transmission of circumferential load sharing, making the ALPSA lesion more susceptible to reinjury. The likelihood of redislocation was found to be 4.67 times higher in patients with a radial tear lesion compared with those with structurally intact ALPSA lesions.
Reported recurrence rates after arthroscopic repair of ALPSA lesions have ranged between 7.7% and 32% in recent literature.3,26 While the recurrence rates for ALPSA lesions were reported to be double those for Bankart lesions in some studies, other studies found no increased failure rate after arthroscopic repair of ALPSA lesions.26,28 This controversy can be explained by variations in ALPSA lesion location and the presence of radial tears—factors that were not clarified in previous studies. The overall redislocation rate in this patient cohort was 19.6%. However, the redislocation rate was 41.4% in patients with isolated ALPSA lesions at the 3- to 5-o’clock position and 32.8% in patients with radial tears. Also, although VAS, OSIS, and SSV scores significantly improved postoperatively in all patients, those who experienced redislocation had significantly lower patient-reported outcomes. The variety of tear patterns and the high redislocation rates associated with specific locations on the glenoid labrum, as demonstrated in the present study, emphasize the importance of thoroughly evaluating ALPSA lesions during intraoperative assessment.
The conclusion of this study should be interpreted in the context of certain limitations. The retrospective nature of the analysis may introduce potential bias; however, all data were collected prospectively, which mitigates the influence of these limitations. The conducted study is based on existing data, relying on images and videos without “real-time” dynamic analysis, which may limit the ability to identify certain injury locations. While the sports activity levels of the patients have been evaluated, the clinical outcomes, specifically in contact/collision athletes, have not been analyzed. The correlation between various lesion types and the development of postoperative contractures, particularly in abduction and external rotation capabilities, has not been thoroughly examined during the postoperative follow-up.
Conclusion
The present study classified ALPSA lesions based on their tear locations and characteristics, highlighting significant variability in tear extensions among patients with ALPSA lesions. Notably, an isolated ALPSA lesion at the 3- to 5-o’clock position and the presence of radial tears were identified as independent factors increasing the risk of redislocation after arthroscopic ALPSA repair.
Footnotes
Final revision submitted March 29, 2025; accepted April 23, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Gazi University Ethics Committee (Protocol: 2024-1385).