
Abstract
Background:
While meniscal tears, particularly when treated by meniscectomy concurrent with anterior cruciate ligament reconstruction (ACLR), are known to increase the risk of osteoarthritis and lead to poorer outcomes, their effects on return to sport (RTS) have been little studied so far.
Purpose:
To assess the effect of meniscal tears on RTS in the context of ACLR depending on the affected meniscus.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors conducted a retrospective analysis based on data from a prospective cohort single-center study involving 504 patients who received the same postoperative follow-up for a minimum of 3 years between April 2015 and December 2019. The preinjury Tegner Activity Scale score was collected preoperatively, and the Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) score was collected 6 months after surgery. At the last follow-up, information such as RTS levels, return to the same sport and same athletic level, Self Knee Value, International Knee Documentation Committee score, ACL-RSI score, Tegner score, graft failure, contralateral rupture, and reintervention was collected. Isolated ACLR was compared with ACLR involving medial meniscus (MM), lateral meniscus (LM), and bi-menisci (BM) injuries, and then meniscal repair and meniscectomies were compared for MM and LM injuries.
Results:
A total of 504 patients were included with a mean follow-up of 4.9 ± 1.2 years; 6 patients were lost to follow-up. The mean postoperative Tegner score was significatively lower for ACLR with MM injuries than for isolated ACLR (5.4 ± 2.0 vs 6.0 ± 2.0; P = .01). Compared with isolated ACLR (93.9%), the RTS rate was significantly lower for MM injuries (85.1%) and BM injuries (84.1%) (P = .02). Outcomes were similar in ACLR with LM and in isolated ACLR. MM repairs significantly increased the mean Tegner score compared with MM meniscectomies (5.8 ± 1.9 vs 4.7 ± 2.1; P < .001). No other significant differences were found on RTS.
Conclusion:
MM tears encountered at the time of ACLR led to a lower Tegner score and a lower RTS rate. Patients undergoing MM repair had higher postoperative activity levels than those undergoing meniscectomy. These findings highlight the importance of repairing MM tears whenever possible at the time of ACLR.
Keywords
Injuries to the anterior cruciate ligament (ACL) mainly occur in physically active individuals27,35 and are associated with cartilage and meniscal injuries in 30% to 50% of cases.19,36 ACL reconstruction (ACLR) is therefore an increasingly common surgical procedure that should provide reproducible and reliable outcomes. 28
A meta-analysis showed that the rate of osteoarthritis after ACL injury was 0% to 13% at 10 years. 56 In another study, patients with intact or repaired menisci who underwent ACLRs had an osteoarthritis rate of 16.4% at 10 years, whereas this rate was dramatically increased to 50% in those who had undergone meniscectomy. 20 Management of meniscal tears is thus very important to reduce the risk of osteoarthritis, which is why the “save the meniscus” strategy is widely accepted. It consists of performing a meniscal repair or leaving the meniscal lesion in place when healing appears to be possible. 10 In addition, poorer long-term patient-reported outcome measures (PROMs) have been reported in patients who had meniscal injuries associated with ACLR than in those who received isolated ACLR. 5 Of note, meniscal repair improved these outcomes compared with meniscectomy. 50
Despite these functional consequences, the MOON Knee Group study, 51 with a 10-year follow-up, showed that patients who underwent ACLR were able to perform sports-related functions and maintain a high knee-related quality of life even with a meniscal lesion. It would appear that in the long term, 8.1 years after an ACLR, an associated meniscal injury did not affect the return-to-sport (RTS) rate, 47 although the time to recovery was longer. 33 However, few outcomes have been reported regarding the medium- and long-term influences of meniscal injury management on RTS. Most studies on this subject have focused on analyzing the results of test batteries11,34,68 assessing patients’ ability to return to sport activity after an ACLR 6 and have reported contradictory results.17,52,59
However, although the rate and level of RTS are known for ACLR, few studies to date have specifically investigated the relationship with an associated meniscal lesion, which needs to be clarified. 61 The aim of our study was to analyze the medium-term influence of meniscal tears and their management on RTS at the time of ACLR. We hypothesized that the presence of a meniscal tear at the time of ACLR would lead to a lower RTS compared with isolated ACLR. In addition, we hypothesized that meniscal repair would improve RTS compared with meniscectomy.
Methods
Study Design
This retrospective analysis based on data from a prospective cohort single-center study included patients who underwent knee ACLR performed by 2 surgeons (N.G. and N.B.) at the Clinique du sport de Bordeaux-Merignac, using the same standardized surgical technique, the same rehabilitation protocol, and the same prospective follow-up. This study conducted on the MERIscience cohort was approved by the Vivalto Santé institutional review board (CERC-VS-2024-10-2) and consists entirely of patients who have given consent to participate.
The inclusion criteria were as follows: ACLR using a hamstring reconstruction with a 4-strand semitendinosus graft with or without an additional anterolateral ligament (ALL) reconstruction with or without a meniscal procedure, a composite evaluation at 6 months postoperatively including an Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) score, and a minimum follow-up of 3 years. Patients were excluded in the case of multiple ligament injuries; degenerative knee with a Kellgren and Lawrence score ≥2; incomplete follow-up; absence of sociodemographic, clinical, or radiological data; unwillingness to participate; or no contact details.
Study Population
A total of 504 patients who underwent surgery between April 2015 and December 2019 and were followed up for at least 3 years with a composite test at 6 months were included (Figure 1). Six patients were excluded due to the absence of a 6-month ACL-RSI score.
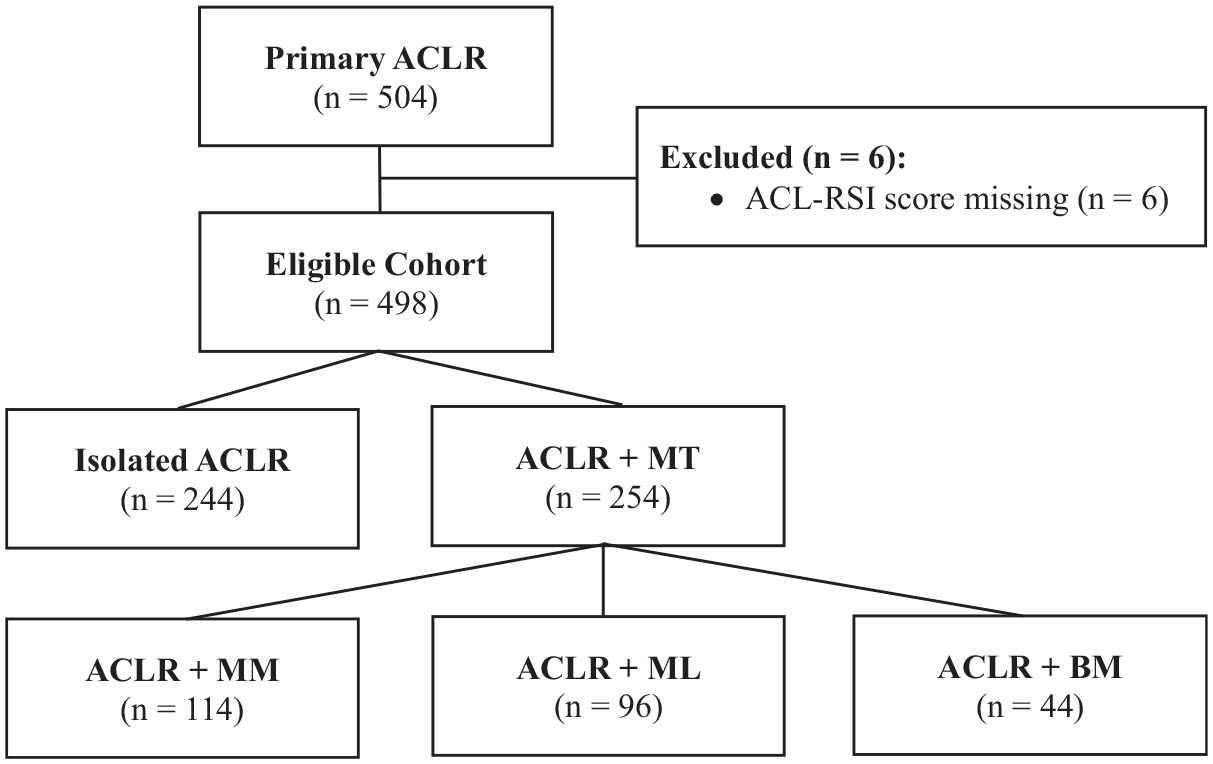
Flowchart of a 504-patient cohort describing exclusion criteria and formation of the analysis group. ACLR, anterior cruciate ligament reconstruction; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; BM, bi-menisci; LM, lateral meniscus; MM, medial meniscus; MT, meniscal tear.
Surgical indication was determined after a preoperative consultation including a full clinical examination of the knee, an assessment of the preinjury Tegner Activity Scale score, and a radiological analysis including AP and sagittal radiographs and magnetic resonance imaging. When necessary, an anterolateral procedure was preoperatively planned in accordance with the recommendations of the ALL study group 62 : pivot-shift grade ≥2, hyperlaxity with knee recurvatum >10°, elite athlete, and bony avulsion of the tibial ALL insertion on AP radiograph.
Meniscal tears were confirmed, described, and classified according to preoperative data and surgical findings. If a meniscal injury was treated, it was classified in the relevant meniscus affected (medial meniscus [MM] injury, lateral meniscus [LM] injury, or bi-menisci [BM] injury) and then was classified relative to the treatment performed on the medial or lateral meniscus, in either the meniscectomy or meniscal repair subgroup. 67 Patients with no meniscal injury and all meniscal injuries not requiring meniscal treatment were classified in the isolated ACLR group.
Surgical Technique
All procedures were standardized and were based on a quadruple hamstring graft. 21 ACLR was performed using a femoral tunnel drill from inside out, leaving a socket 25 mm deep. A complete tibial tunnel was obtained with an outside-in technique. Tibial and femoral tunnels were dimensioned to the size of the graft and fixed with 2 suspensory buttons: PullUp and PullUp XL (SBM). 22 Reconstruction of the ALL used a gracilis autograft, previously shaped and fixed to the tibia with an ACL TightRope II suspensory button (Arthrex) and to the femur with a FastThread BioComposite Interference Screw (Arthrex). The femoral entry point was 1 cm posterior and proximal to the lateral epicondyle. The tibial entry point was posterior to the tubercule of Gerdy, 7 mm below the joint line, and the graft was passed underneath only the iliotibial band and not the lateral collateral ligament.14,41
The choice of meniscal treatment was at the surgeon’s discretion and was based on international consensus recommendations, 9 depending on the patient’s characteristics, the type of meniscal tear, and its location. Incomplete meniscal tears (affecting a single joint surface), tears in the process of healing, or stable vertical lesions of the MM and the posterior horn of the LM were left in situ. 60 Meniscal tears in zone 1 (red-red) were repaired as far as possible using an all-inside meniscal repair system (Air+; Stryker)31,54 by classic or auxiliary arthroscopic approaches. For meniscal tears in zone 3 (white-white), meniscal flaps and degenerative lesions were resected using arthroscopic biters and smoothed with shaving.
An exploration of the posteromedial compartment was systematically performed to diagnose and characterize ramp lesions according to the classification of Thaunat et al. 66 Type 1 lesions were repaired with a minimum of 2 separated sutures performed using a 25° curved hook (QuickPass SutureLasso; Arthrex) loaded with a No. 0 absorbable monofilament suture (PDS II; Ethicon) via a posteromedial approach. 63 Other types were considered to be classic meniscal injuries and were managed using the technique previously described.
The same postoperative protocol was applied for all patients: immediate weightbearing as tolerated except for radial tears, which required 1 month without any weightbearing. For all patients, there was no period of immobilization, no restriction in the range of motion, and no brace wear.
Assessment of Outcomes
Follow-up was standardized with clinical evaluations at 1, 3, and 6 months and 1 year. At the 1-month postoperative clinical evaluation, we evaluated healing of the wounds, recovery of complete extension, and 90° of knee flexion. At the 3-month evaluation, we aimed to allow the beginning of the return to sports-specific activities time based on validation of recovery of range of motion and strength of quadriceps muscle and hamstrings. At 6 months, patients had the opportunity to benefit from an individual assessment of their performance for a fee of €60. All patients underwent a composite test including 1-foot jump tests and isokinetic and psychological evaluation using the ACL-RSI score. 69 At 1 year, all patients underwent full clinical examination. The last evaluation was performed at least 3 years after surgery, by telephone or email, by a surgeon who was not involved in the initial diagnosis and treatment. It included a subjective analysis of the knee using the International Knee Documentation Committee (IKDC) score 38 and Self Knee Value (SKV) score, 49 an activity analysis using the Tegner Activity Scale, 65 a psychological analysis using the ACL-RSI score, and other outcomes such as graft failure, contralateral rupture, surgical reintervention, and RTS for the same sport and at the same level.
First, patients were grouped according to the meniscus affected, which enabled the effect of meniscal lesions and their location to be assessed in comparison with isolated ACLR. Second, meniscal repair was compared with meniscectomy for both the MM and the LM injuries, allowing assessment of the effect of meniscal treatments.
Statistical Analysis
Data are reported in accordance with STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. Data are summarized using descriptive statistics, including count and percentage for categorical variables and mean and standard deviation for continuous variables. The chi-square and Fisher exact tests were used to test for differences between categorical variables, and the Kruskal-Wallis test was used for continuous variables.
Statistical tests to determine the sample size were performed using G*Power software. 29 Regarding the effect of meniscal injuries and with reference to the minimum detectable change of the Tegner score, 15 the number of patients required was estimated based on the assumption that the mean Tegner score would be 6.0 ± 1.0 in the isolated ACLR group and 5.0 ± 1.0 in the 3 other groups (ACLR + MM injury, ACLR + LM injury, ACLR + BM injury). With a first species risk (α) of 5.0%, second species risk (1 – β) of 20.0%, and size effect (d) of 0.2165, it was calculated that 240 patients would be required, that is, 60 in each group.
Regarding the effect of meniscal management, the number of patients required was estimated on the assumption that the mean Tegner score would be 6.0 ± 1.0 in the meniscal repair group and 5.0 ± 1.0 in the meniscectomy group. With a first species risk (α) of 5.0%, second species risk (1 – β) of 20.0%, and size effect (d) of 0.5, it was calculated that 52 patients in each group would be required.
All analyses were performed using IBM SPSS software for Windows (Version 27; IBM Corp).
Results
Study Population
The statistical analysis included 498 patients with a mean follow-up of 4.9 ± 1.2 years. Their baseline characteristics (Table 1) reflect a population mostly involved in competitive sports with a mean age of 27.6 ± 1.9 years (range, 14-58 years) and a mean Tegner score of 7.1 ± 0.9 (range, 2-9) preinjury and 6.0 ± 2.1 (range, 0-10) at the last follow-up, with an RTS rate of 91% (452/498).
Patients Characteristics at Baseline a

Results are reported as n (%) or mean ± SD (range). ACLR, anterior cruciate ligament reconstruction; BM, bi-menisci; LM, lateral meniscus; MM, medial meniscus; MT, meniscal tear.
There were 254 patients with meniscal tears treated at the time of ACLR (51.0%), including isolated MM tears (114 patients; 44.9%), isolated LM tears (96 patients; 37.8%), and BM tears (44 patients; 17.3%).
Among patients with injuries of the MM, 75 (65.8%) had a meniscal repair and 39 (34.2%) had a meniscectomy. Among patients with LM tears, 62 (64.6%) had a meniscal repair and 34 (35.4%) had a meniscectomy.
Effect of Meniscal Tears
Compared with isolated ACLR, the RTS rate was not different for patients with an LM injury (93.9% vs 92.7%), but was significantly lower for patients with an MM injury (93.9% vs 85.1%; P = .02) or a BM injury (93.9% vs 84.1%; P = .02) (Table 2).
RTS and Medical Outcomes Depending on Meniscal Tears and Their Location a

Results are reported as n (%). Bold P value indicates statistical significance. ACLR, anterior cruciate ligament reconstruction; BM, bi-menisci; LM, lateral meniscus; MM, medial meniscus; RTS, return to sport.
The Tegner Activity Scale revealed a significantly lower postoperative score for patients with MM injury (5.4 ± 2.0; P = .01) than for those with isolated ACLR (6.0 ± 2.0), but this was not the case for patients with LM injury (6.3 ± 2.0; P = .27) and BM injury (6.2 ± 2.0; P = .70) (Table 3). There were no statistical differences caused by the presence and different location of a meniscal lesions in terms of return to the same sport and return to the same level.
PROM Results Depending on Meniscal Location Compared With Isolated ACLR a

Results are reported as mean ± SD. Bold P values indicate statistical significance. ACLR, anterior cruciate ligament reconstruction; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; BM, bi-menisci; IKDC, International Knee documentation Committee; LM, lateral meniscus; MM, medial meniscus; PROM, patient-reported outcome measure; SKV, Self Knee Value.
In patients with isolated MM injuries, the SKV was significantly lower (85.0% ± 16.4% vs 88.2% ± 13.1%; P = .048) and the IKDC score was significantly lower (76.2% ± 14.4% vs 79.8% ± 10.7%; P = .01) than in patients without any meniscal injuries. Patients with BM injuries had the lowest SKV, with a 7.5% loss (80.7% ± 19.0% vs 88.2% ± 13.1%; P < .001) and a statistically significant decrease of ACL-RSI throughout follow-up (–2.5% ± 27.1% vs 6.01% ± 25.7%; P = .04).
Compared with isolated ACLR, LM injuries concomitant with ACLR did not show significant differences in any of the data studied. Moreover, meniscal lesions, depending on their location, had no influence on the rates of graft failure, contralateral rupture, or reintervention.
Effect of Meniscal Management
MM repairs showed a significantly higher postoperative Tegner score than meniscectomies at the time of ACLR (5.8 ± 1.9 vs 4.7 ± 2.1; P < .001), which was not found in the case of LM repairs (Table 4). Regarding RTS, return to the same sport, and return to the same athletic level, no significant differences were found between the different meniscal treatments performed for both the MM and LM. Nor was a difference found for the assessment of PROMs or in graft rupture, contralateral rupture, and reoperation rates between meniscal repair and meniscectomy for both the MM and LM.
Outcomes of Meniscal Repair Versus Meniscectomies Compared in MM and LM a

Results are reported as n (%) or mean ± SD. Bold P value indicates statistical significance. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; LM, lateral meniscus; MM, medial meniscus; RTS, return to sport; SKV, Self Knee Value.
Discussion
The main finding of this study is that patients with medial or bi-meniscal lesions at the time of ACLR have a lower rate of RTS, and MM injuries are associated with a lower postoperative Tegner score. Patients undergoing MM repair had higher Tegner scores than those undergoing medial meniscectomy. However, those with LM injuries have a similar RTS rate and Tegner score to patients with isolated ACLR.
The mean follow-up was 4.9 years, which is longer than the 2-year period usually used to describe an RTS and therefore provides a reliable analysis of the patient’s physical capacity. 2 All patients underwent surgery using a ACLR + semitendinosus graft technique, the outcomes of which showed no clinical or functional differences compared with other available techniques. 37 A high rate of meniscal repair was obtained in both MM and LM (65.8% and 64.6%, respectively), reflecting our conservative approach to the management of meniscal injuries. 10 The Tegner score, RTS rate, and levels of return to the same sport and same athletic level allowed us to study return to activity. SKV 49 and IKDC 38 studies have demonstrated the clinical relevance of these indicators in the functional assessment of patients who receive ACLR. Additionally, the ACL-RSI can be used to assess subjective psychological aspects associated with RTS. 53
To evaluate rehabilitation, the literature describes composite tests aiming to assess the ability to RTS. 11 Our composite test, based on these recommendations, was performed for all patients at 6 months postoperatively and consisted of isokinetic tests, 1-foot jump tests, single-leg squats, and a psychological evaluation.44,55 Although the RTS after ACLR has been extensively studied, few sufficiently powerful studies have focused on the effects of meniscal injuries and their management 61 in the medium term.
With a preoperative Tegner score of 7.1, our population consisted of many competitive athletes. 18 As shown in the literature, this score decreases for each group after ACLR.40,43 However, compared with isolated ACLR, patients with MM injuries had a significantly lower Tegner score, whereas this difference was not found for LM or BM injuries. The RTS in our study was 9% higher than that in the literature, which describes a return to any sport participation rate of 82%. 3 In our study, each patient benefited from a systematic individual assessment before RTS, which may explain our higher RTS rate.25,30 MM tears have detrimental consequences, with RTS rates significantly reduced by 8.8%, and BM tears have the lowest RTS rate, with a decrease of 9.8%, while injuries to the LM are associated with rates comparable to those observed in isolated ACLR. Lucidi et al 46 showed that injuries of the LM posterior root did not affect rotatory knee laxity and did not increase anterior tibial translation, which is in favor of low clinical repercussions. However, our results show that MM tears may have a major influence and repercussions on RTS, and although statistical significance was found, the clinical relevance may not be achieved for the Tegner score. Indeed, for this score Briggs et al 15 showed a measurement error of 0.64 and a minimum detectable change of 1.0. As reported in the literature, future studies are therefore needed to clarify the effect of these meniscal injuries.4,45
Furthermore, MM repair results in a significant increase of 1.1 points in the Tegner score compared with MM meniscectomy at the time of ACLR, but no differences were found regarding the RTS rate. This is therefore an interesting new finding for patients with an ACLR and an MM injury, as a meniscal repair would improve the level of sport activity. This outcome was supported by the beneficial influence of meniscal repair on walking biomechanics 16 in particular for MM injuries, resulting in improved knee function and proprioception. 8 Additionally, it has been shown that the frequency of injuries to the MM increases with the delay between trauma and surgery. 26 These outcomes should therefore be taken into consideration when adapting the management of isolated ACL injuries with a view to early intervention, particularly in sports patients.
Our study found no significant ACL-RSI difference at the last follow-up when meniscal tears were documented at the time of ACLR, regardless of their location and the treatment performed, suggesting that the difference in RTS rates was not influenced by psychological factors. Only patients with associated ACLR and BM tears experienced a significant decrease (2.5%) in ACL-RSI score between the 6-month postoperative assessment and the last follow-up, showing a progressive loss of confidence in their knee, which may be associated with poorer PROMs in this group. This difference was not found in the other groups, and consistent with the literature, an increase was observed at the last follow-up. 48 However, interpretation of this score remains difficult because there was no Patient Acceptable Symptom State. There was only an association with an RTS at the same level when the ACL-RSI score was >58% to 65%. 12 Accordingly, the analysis of this score is left to the discretion of each team to authorize a return to activity. 10
Patients with meniscal injuries at the time of ACLR have significantly worse medium-term PROMs than patients who have isolated ACLR, which is consistent with the literature.23,57 It would appear that the greatest repercussion comes from damage to the MM because these patients demonstrate a 3.2% decrease in the SKV and a 3.6% decrease in the IKDC score, while LM injuries have similar values to isolated ACLR. This could explain the significant 7.5% reduction in the SKV for BM injury concomitant with ACLR compared with isolated ACLR. On the other hand, although our results show significant differences, the clinical effect may be difficult to assess, as the minimal clinically important difference has been shown to differ by at least 11.5% for IKDC 39 and has not yet been defined for SKV.
In a short-term follow-up, 2 large cohorts (Svantesson et al 64 in the KOOS Symptoms subsection, LaPrade et al 42 in the KOOS Symptoms and KOOS Quality of Life subsections) showed worse PROMs when a meniscal repair was performed during ACLR. These results are in contrast to those of a large Norwegian national cohort, which found no such effects but instead worse outcomes for meniscal resections associated with ACLR. 58 In view of these highly controversial results, Sarraj et al 61 carried out a systematic review that revealed, after 2 years of follow-up, better outcomes for ACLR combined with meniscal resection compared to meniscal repair, but after 4 years of follow-up, meniscal repair improved PROMs. Our study does not reveal any other significant differences between the treatments carried out on both the medial and lateral menisci in terms of PROMs. However, these results remain to be clarified with more focused studies, 23 but given the absence of adverse effects of meniscal repair at 5 years, meniscectomy should be avoided whenever possible to prevent the risk of osteoarthritis. 7
Graft failure,24,32,48 contralateral rupture,1,13 and reintervention rate are not affected by meniscal tears and treatments. Our results are comparable to those reported in the literature and were not affected by meniscal injuries, regardless of meniscal involvement in ACLR. However, to our knowledge, no study has specifically examined these results in relation to the presence of meniscal lesions, which makes the results of our study interesting.
The main strengths of this study are its large cohort; standardized, reproducible surgical technique; and follow-up. All surgeons used the same operating and meniscal repair material. This study also has some limitations. Notably, the characterization of injuries did not include some pathological details regarding incidence cartilage injuries and precise type of meniscal tear, which limited the multivariate analyses and may have generated confounding bias in our subgroup analysis. The limited number of patients with BM injury means that the results for this group must be interpreted with caution. Moreover, the size of the groups for the treatment of meniscal injuries could have underestimated a statistical difference for graft failure, contralateral rupture, and reintervention. Based on the recommendations for the inclusion period, only a few patients benefited from ALL reconstruction, and these were athletes and patients with the highest risk of recurrence.
Meniscal lesions continue to appear over time, and to assess how these menisci behave in the long term after trauma, we currently continue the prospective follow-up of these patients to analyze the evolution of both the meniscal repairs and the traumatized meniscus.
Conclusion
At the time of ACLR, damage to the MM is associated with poorer Tegner score, RTS rates, and worse PROMs in the medium term. However, a better RTS rate has been observed in the case of MM repair compared with patients undergoing medial meniscectomy. LM injuries and their meniscal treatment do not seem to have any repercussions at the last follow-up, as they present results similar to those of isolated ACLR. Our findings suggest that MM injuries at the time of ACLR are associated with poorer RTS and PROMs, highlighting the importance of identifying and repairing MM tears whenever possible to improve outcomes in patients undergoing ACLR.
Footnotes
Final revision submitted April 1, 2025; accepted April 14, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Vivalto Santé (CERC-VS-2024-10-2).