
Abstract
Background:
Evaluation of medial meniscal extrusion (MME) under physiological loads is crucial because of the influence of MME on meniscal function. Reducing the MME is essential for meniscal function. Few studies have compared the extent of MME in cases of complete radial tears of the posterior segment of the medial meniscus (MM) treated using basic meniscal repair techniques: the inside-out and all-inside techniques.
Purpose:
To compare the extent of MME after the treatment of complete radial tears of the posterior segment using inside-out and all-inside meniscal repair techniques in a cadaveric model.
Study Design:
Controlled laboratory study.
Methods:
Six fresh-frozen human cadaveric knees were subjected to a compression load of 250 N using a 6 degrees of freedom robotic system under ultrasound evaluation. The MME was evaluated at 30° and 90° knee flexion in 4 meniscal conditions: (1) intact; (2) complete radial tear in the posterior segment of the MM; (3) inside-out repair technique; and (4) all-inside repair technique using 1 horizontal suture. Conditions 3 and 4 were performed on the same knee in a randomized order. Measurements were obtained at the center of the superficial medial collateral ligament (MCL) (central image) and 1 cm posterior to the superficial MCL (posterior image). Statistical analysis was conducted using a 2-factor repeated-measures analysis of variance with Bonferroni post-hoc correction, with significance level set at P < .05.
Results:
The amount of MME under compression load after inside-out repair was significantly lower than that after all-inside repair (mean ± SD values for the central image: 30°, 1.93 ± 0.26 mm vs 2.45 ± 0.34 mm; 90°, 2.02 ± 0.29 mm vs 2.53 ± 0.42 mm; for the posterior image: 30°, 1.98 ± 0.30 mm vs 2.43 ± 0.35 mm; 90°, 2.45 ± 0.26 mm vs 3 ± 0.42 mm; P < .001 for all comparisons).
Conclusion:
Although the inside-out repair technique reduced the amount of MME to a greater extent than the all-inside repair technique using a single horizontal stitch for MM posterior segment tears, neither technique was able to reduce MME to the same level as that of the intact state; furthermore, the change in MME was relatively small.
Clinical Relevance:
The findings indicate that the inside-out repair technique should be used to repair complete radial tears in the posterior segment of the MM.
Keywords
Meniscal repair techniques have recently undergone many advancements. The all-inside and inside-out techniques are the 2 most commonly used methods for meniscal repair. The all-inside repair technique uses suture devices placed arthroscopically, while the inside-out repair technique involves threading sutures through the meniscus and the capsule, securing them on the outside.13,24 Over the past 2 decades, all-inside repair has increasingly replaced the traditional inside-out technique because of its less invasive approach and positive results.11,25 Consequently, the use of all-inside devices for meniscal repair has increased by 50%. However, the overall failure rate of meniscal repair remains25,33 high (22.6%), necessitating further investigation of standard meniscal repair techniques, including inside-out and all-inside repair techniques.
Complete radial tears present a notable challenge in this context. 29 These tears usually originate in the central part of the meniscus and extend outward toward the periphery, leading to loss of load transmission, shock absorption, and resistance to meniscus hoop force.10,19,22,38 Several meniscal repair techniques have been reported for radial tears; however, many of these techniques are complex. 29 To develop a simplified and effective strategy for managing complete radial tears, it is important to examine and compare the 2 fundamental repair techniques—the all-inside and inside-out repair techniques.
Biomechanical studies comparing all-inside and inside-out repair techniques for radial tears have shown similarly good outcomes with both techniques.28,29,37 However, most of these studies assessed tensile strength or rigidity by extracting the meniscus from cadaveric or animal knees, which represents a non-physiological scenario.2,3,22,28,29,37 Evaluation of the meniscus states under physiological loads, such as meniscal extrusion, is essential.
Meniscal extrusion has become an important factor in osteoarthritis (OA).7,20 In Japan, where medial-type OA is particularly common, medial meniscal extrusion (MME) plays a critical role and is often caused by tears in the posterior segment of the medial meniscus (MM).5,15,18,19,20,30 Reducing meniscal extrusion is essential for preserving meniscal function; thus, evaluating meniscal extrusion under physiological loads is crucial. Meniscal extrusion also varies dynamically depending on the weightbearing status and knee flexion angle.17,27 Therefore, dynamic evaluation of meniscal extrusion is necessary. Conventional magnetic resonance imaging can only assess meniscal extrusion under nonweightbearing conditions, whereas ultrasonography allows evaluation during weightbearing and knee flexion.9,17,26
This study aimed to compare the amount of MME for MM posterior segment complete radial tears between all-inside and inside-out meniscal repair techniques. We hypothesized that (1) the all-inside and inside-out repair techniques would have different results on MME; (2) both techniques would restore MME to a level comparable to that of the intact state in the sutured position under the valgus load, but would not achieve the same level under compression load; and (3) the amount of MME might vary according to the knee flexion angles and measurement locations.
Methods
Specimen Selection and Preparation
The study protocol for obtaining, using, and disposing of fresh-frozen human cadaveric knees was approved by the ethics committee of our institution (approval No. 1-2-68). All cadaveric specimens used in this study were donated to a body donation program (Shiragiku-kai) run by our university for medical and scientific research. Informed consent was obtained from all participants before their death. Ten fresh-frozen knee specimens were obtained from donations to the university anatomy program. Direct visualization and manual physical examination were performed before biomechanical testing. Specimens were visually inspected for signs of previous surgery, bony abnormalities, severe osteoarthritic changes, or meniscal damage. Manual assessment was conducted to evaluate the range of motion (ROM) from full extension to 130° of flexion and assess ligamentous stability—including checks for extension deficits and increased joint gap opening. Specimens with instability, restricted ROM, or severe cartilage damage (International Cartilage Regeneration & Joint Preservation Society grade 4) were excluded. Four knees were excluded, 2 had severe cartilage damage, and the other had loss of ROM. Six fresh-frozen knee specimens (mean age at death, 86.8 years; range, 81-95 years; men: n = 4, women: n = 2) were selected. The specimens were thawed at room temperature for at least 24 hours before testing. Each specimen was kept wet to preserve tissue integrity during the test. The femur and tibia were cut at least 15 cm above and below the joint line, respectively, and the fibula was cut 5 cm below the proximal tibiofibular joint. The soft tissues, including all muscles except the popliteus, were excised, whereas the ligaments, posterior capsule, and meniscus were left intact. Both ends of the tibia and femur were fixed using acrylic resin (Ostron II; GC) and poured into cylindrical molds. The fibula was fixed in its original position using a resin. The femoral and tibial cylinders were fixed with aluminum clamps and connected to the end effector of a robotic testing system (FRS-2015; Technology Service) (Figure 1).

The left specimen was placed in the robotic system with 6 degrees of freedom under ultrasound evaluation.
Surgical Procedure
The MM posterior segment tear was modeled by creating a complete radial tear at the 10-mm posterior segment of the MM from the root using a No. 11 scalpel blade under arthroscopic guidance. Both the inside-out and all-inside meniscal repair techniques were performed on the same knee, and the testing order of the 2 techniques was randomized. Both repairs were performed in a horizontal and single-stitch fashion with a knee flexion angle of 30° and valgus rotation torque of 5 Nm. 24 The sutures were placed on the femoral side of the MM, 5 mm on either side of the tear, and at the midway between the central and peripheral rim (Figure 2). The all-inside meniscal repair technique was performed using an AIR meniscal repair system (Stryker) that deploys anchors to the periphery of the meniscus and the capsule. The all-inside repair technique was tightened manually to the maximum load using a dedicated knot pusher. Inside-out meniscal repair was performed using inside-out sutures utilizing the Henning meniscal suture kit with 2-0 WAYOLAX (Stryker). The inside-out repair technique was secured using 2 square knots and 5 throws on the capsular side of the meniscus. After the first meniscal repair and subsequent tests were completed, the first suture was removed, and the second meniscal repair surgery was performed using the same route within the meniscus. We arthroscopically confirmed proper reduction of the tear site.

Schematic representation of meniscal repair. (A) The inside-out technique. (B) The all-inside technique. (C) Suture position in the sagittal image.
Testing Apparatus
A robotic testing system with a custom-made manipulator having 6 degrees of freedom, equipped with a universal force-torque sensor (DELTA IP65, SI-660-60; ATI Industrial Automation), was used (Figure 1). The robotic system could simulate physiological knee joint motion based on the joint coordinate system developed by Grood and Suntay in vitro. 12 This system, which characterizes the displacement and force/torque applied to knee joints, was controlled in real time by a LabVIEW Version 1.0.0.0 (National Instruments Corp)-based program running on a Windows personal computer (Microsoft).
Testing Protocol
First, the flexion-extension axis of the knee was defined as 0° of flexion when a 0.5-Nm extension moment was applied to the intact knee. Next, passive flexion-extension was performed starting from the hyperextended position, with a 5-Nm extension moment applied to ensure full knee extension. Knee flexion was then gradually increased to a maximum of 120° to ensure that full knee flexion was achievable. This was applied at a rate of 0.5°/sec and repeated 3 times as preconditioning. Ultrasound evaluation was performed on the knee at 30° and 90° of knee flexion under 250 N of compression load.
We also performed evaluations only at 30° and 90° of knee flexion for the following reasons: first, we aimed to evaluate deep flexion; second, previous studies showed no significant difference in MME between 0° and 30° knee flexion. 9
MME was evaluated in 4 meniscal conditions utilizing ultrasound: (1) intact; (2) complete radial tear in the posterior segment of the MM; (3) inside-out repair technique; and (4) all-inside repair technique. Conditions 3 and 4 were performed on the same knee in a randomized order. Figure 3 presents a schematic diagram of the location of the complete radial tear in the posterior segment of the MM and the ultrasound probe.
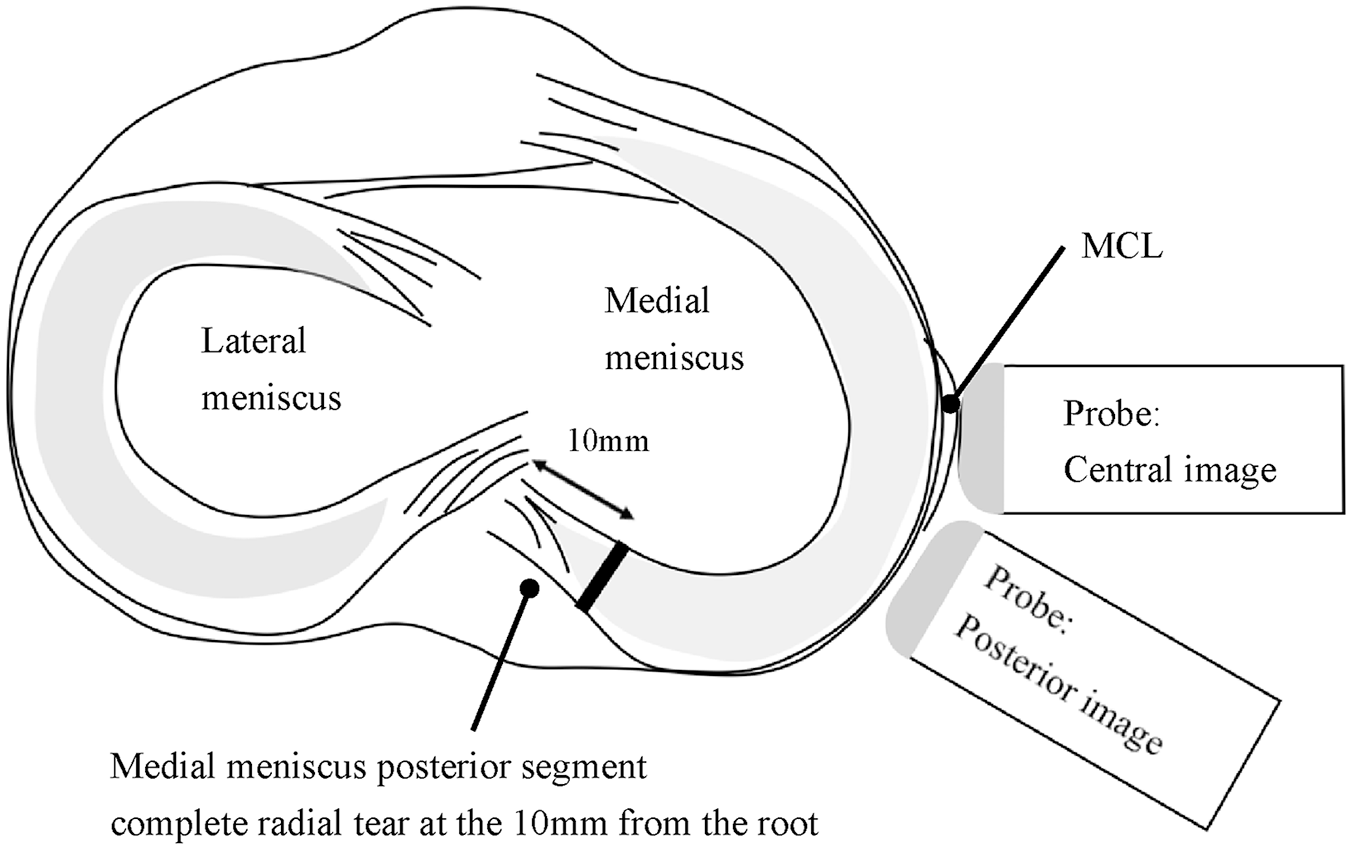
Schematic representation of the locations of the complete radial tear of the posterior segment of the MM and the ultrasound probe. A complete tear of the posterior segment of the MM was made 10 mm from the MM posterior root. MCL, medial collateral ligament; MM, medial meniscus.
Before each knee status test, preconditioning using an axial load of 250 N at 30° and 90° was performed to minimize the effects of creep.
Ultrasound Evaluation of MME
A 10–2 MHz linear transducer (SuperSonic MACH 20 system; SuperSonic Imagine) was used to evaluate the amount of MME. The probe was preset for normal knee musculoskeletal ultrasound evaluations with a standardized depth of 2.5 cm. 31
Measurement Procedure
Ultrasound examinations and measurements were performed by 2 orthopaedic doctors trained in ultrasound (K.H. and Y.M.). One doctor (K.H.) conducted the ultrasound examination and captured still images, while the other (Y.M.) independently measured MME using ultrasound software. The software had a measurement accuracy of 0.1 mm, as specified by the manufacturer. Examiners were blinded to each other’s measurements. Measurement protocols—including knee flexion angle and probe position—were randomized to prevent recall bias.
Reliability Assessment
Pilot testing was performed on 2 test specimens to calculate the inter- and intraclass correlation coefficients for anterior and posterior MME measurements under a 250 N axial load using central and posterior probe positions, with a 2-way random-effects model. Examiners were blinded to each other’s measurements. Each test condition was assessed 3 times: twice by examiner K.H. for intrarater reliability and once by examiner Y.M. for interrater reliability. For each knee, 16 measurements were performed (4 meniscal conditions × 2 knee flexion angles × 2 probe positions), resulting in 32 measurements across both knees. One examiner (K.H.) performed the initial measurements, followed by additional random measurements by the other examiner (Y.M.).
Measurement Protocol
To enhance the reliability of our ultrasound measurements, we performed the following procedure. 14 Initially, we marked the entire width of the medial collateral ligament (MCL) with a permanent surgical skin marker. A K-wire was inserted at the MCL attachment site on the medial femoral epicondyle as a guide. By aligning the midpoint of the probe’s short-axis width with the K-wire and the knee in extension, we ensured that the probe’s long axis was parallel to the MCL. For the posterior image, the probe was moved 1 cm behind the central position, with its front edge almost aligned with the marked posterior edge of the MCL. The examinations were repeated 3 times for each knee condition, and the median values of the measured data were calculated.
MME Measurement
We measured the MME according to the protocol outlined in a previous study. 9 The long axis of the probe was maintained parallel to the long axis of the tibia. Images were acquired in 2 areas at the level of the joint line for each test state—over the MCL (“central” image) and 1 cm posterior to the MCL (“posterior” image). To measure the MME from the ultrasound images, a reference line connecting the innermost borders of the femur and tibia within the joint space was drawn. After determining the reference line, a second line was drawn from the outermost portion of the MM perpendicular to the reference line. The distance measured along this second line was considered the MME (Figure 4).

Ultrasound image of the MM in the central image. MME (dotted line) is defined as the perpendicular distance from the tangent line (solid line) connecting the medial edge of the femur and tibia to the outermost edge of the MM. MM, medial meniscus; MME, medial meniscal extrusion.
Statistical Analysis
The MME values under compression or valgus loads in the intact knee, complete radial tear, inside-out repair, and all-inside repair states were analyzed using a 2-factor repeated-measures analysis of variance (ANOVA) to compare the state of the knee and knee flexion angle. Post-hoc pairwise comparisons were performed using Bonferroni correction. The difference in the MME between the measurement locations (central and posterior image) was assessed using paired t tests, independent of the 2-way repeated ANOVA. Statistical significance was set at P < .05. All data were analyzed using EZR Version 1.60 (Saitama Medical Center; Jichi Medical University), a graphical user interface for R (The R Foundation for Statistical Computing), which is a modified version of R Commander designed to add statistical functions frequently used in biostatistics. 16
An a priori power analysis was performed using G*Power (Universität Düsseldorf, Germany). Based on mean values and standard deviations from a previous study, 9 it was concluded that a sample size of 6 knees would allow detection of meaningful differences in MME (effect size/Cohen’s d = 1.45). The analysis was conducted with a significance level of P < .05 and a statistical power of 80%.
Results
The calculated intraclass coefficients for intra- and interobserver reliability in the pilot study were 0.979 (95% CI, 0.965-0.987) and 0.967 (95% CI, 0.946-0.980), respectively, demonstrating excellent agreement.
Compression Load—Central and Posterior Images
The interaction effects were not significant under compression load (central: P = .924; posterior: P = .971). Among the main effects, the knee state demonstrated a significant influence in both regions (P < .001), while the flexion angle was significant only in the posterior region (P < .001 for posterior; P = .598 for central).
The MME values for different knee states are illustrated in Figure 5 A and B, with detailed group comparisons, including absolute differences and 95% CIs, presented in Table 1.

(A) The MME in the central image and (B) the posterior image under a compression load of 250 N at knee flexion angles of 30° and 90° for each knee state. The boxes represent the IQR, with a line inside the box indicating the median. The connecting lines represent the mean values. Whiskers extend up to 1.5 times the IQR from the top and bottom of the box. Significant differences are indicated by asterisks (*). IQR, interquartile range; MME, medial meniscal extrusion.
Absolute Difference in the MME Between the Previous and Subsequent Conditions Under Compression Load a

Mean values are presented with 95% CIs in square brackets. P values are adjusted using the Bonferroni correction, with statistical significance set at P < .0083. Bold values indicate significant results. MD, mean difference; MME, medial meniscal extrusion.
The amount of MME in the intact state was significantly lower than in the complete radial tear state of the posterior segment of the MM. The mean differences (MDs) were as follows: the central image at 30° (MD, 1.30 mm [95% CI, 1.10-1.50]; P < .001) and 90° (MD, 1.27 mm [95% CI, 1.04- 1.49]; P < .001), and the posterior image at 30° (MD, 1.33 mm [95% CI, 1.06-1.60]; P = .004), and 90° (MD, 1.35 mm [95% CI, 0.99-1.71]; P = .006).
MME after the inside-out repair was significantly lower than that in the radial tear state and also lower than that after the all-inside repair. Compared with the complete radial tear state of the posterior segment of the MM, the MDs were as follows: the central region at 30° (MD, 0.80 mm [95% CI, 0.58 to 1.02]; P < .001) and 90° (MD, 0.82 mm [95% CI, 0.55 to 1.08]; P < .001), and the posterior region at 30° (MD, 0.75 mm [95% CI, –0.54 to 0.96]; P = .003) and 90° (MD, 0.83 mm [95% CI, 0.59 to 1.08]; P < .001). Compared with the all-inside repair state, the MDs were as follows: the central image at 30° (MD, 0.52 mm [95% CI, 0.22 to 0.81]; P < .001) and 90° (MD, 0.52 mm [95% CI, 0.22 to 0.81]; P < .001), and the posterior region at 30° (MD, 0.45 mm [95% CI, 0.16 to 0.74]; P = .005) and 90° (MD, 0.55 mm [95% CI, 0.24 to 0.86]; P = .007). MME after the inside-out repair was significantly higher than that in the intact state. The MD was as follows: the central region at 30° (MD, 0.50 mm [95% CI, 0.31 to 0.69]; P = .004).
Direct Comparison of MME at Different Knee Flexion Angles and Measurement Locations
The posterior image demonstrated significantly greater MME at 90° of knee flexion than at 30° of knee flexion (30° vs 90°; 2.14 ± 0.60 vs 2.67 ± 0.65; P = .006), while the central image demonstrated no significant difference (30° vs 90°; 2.14 ± 0.56 vs 2.24 ± 0.57; P = .55) (Figure 6).

(A) Direct comparison of MME in the central image and (B) the posterior image at 30° and 90° of knee flexion. The bar plots represent the mean ± standard deviation for each condition. MME, medial meniscal extrusion.
Discussion
The most important finding of this study was that the inside-out repair technique resulted in less MME than the all-inside repair technique using a single horizontal stitch for complete radial tears of the MM posterior segment. However, neither technique could achieve the MME at the intact level under compression load. The amount of MME at 90° of knee flexion in the posterior image was also greater than that at 30°. These results support our hypotheses.
Sukopp et al 35 investigated incomplete radial tear models in a porcine knee, where the tear extended two-thirds of the meniscus depth from the inner edge, leaving the peripheral edge intact. Using roentgen stereophotogrammetric analysis, they observed that the tear gap at the inner edge could not be restored to an intact state even after repair. In contrast, Shiwaku et al 34 studied complete radial tears of the lateral meniscus under valgus loading using ultrasonography and found that the inside-out repair technique was superior to the all-inside technique in controlling the peripheral gap of the tear. They attributed this superiority to the ability of the inside-out technique to stabilize the periphery of the tear site more effectively, whereas the all-inside technique, relying on capsule anchoring, was less effective in maintaining tear margin stability. This improved stabilization of the peripheral gap was also associated with a reduction in the meniscal extrusion, highlighting the critical role of peripheral gap control in meniscal repair. Similarly, our results showed that the inside-out technique reduced the MME more effectively than the all-inside technique in radial tears of the posterior MM, likely because of its better stabilization of the peripheral edge (Figure 7).

The schema of our results. (A) Unloaded MM with a complete radial tear. The tear is closed from the center to the outer edge. (B) A loaded MM with a complete radial tear. The tear is open from the center to the outer edge, and MME has arisen. (C) A loaded MM during knee flexion with a complete radial tear. The MM translates posteriorly and extrudes in the posteromedial region. (D) An unloaded MM after inside-out repair. The tear is closed from the center to the outer edge. (E) A loaded MM after inside-out repair. The tear is mostly closed, and MME has been prevented. (F) A loaded MM during knee flexion after inside-out repair. The MM translates posteriorly but does not extrude. (G) An unloaded MM after all-inside repair. The tear is closed from the center to the outer edge. (H) A loaded MM after all-inside repair. The tear is mostly closed in the center but open at the outer edge. MME has arisen. (I) A loaded MM during knee flexion after all-inside repair. The MM translates posteriorly and extrudes in the posterior medial region. MM, medial meniscus; MME, medial meniscal extrusion.
Rowland et al 32 investigated the lateral meniscal extrusion using ultrasound in fresh-frozen cadaveric specimens, evaluating only in the extended knee position. They reported no significant difference in the extrusion between the intact and repaired states under both unloaded and axial compression conditions. However, while the difference under compression load was statistically significant, the repaired state exhibited greater extrusion (1.86 mm) than the intact state (1.60 mm). However, our results demonstrated that under compression load, neither technique achieved the same level of MME reduction as the intact state, thus varying from the findings of Rowland et al. This discrepancy may be attributed to several factors. First, our study evaluated a different knee flexion angle. MME tends to increase with greater knee flexion angles.9,27 Second, the suture strength in our study might have been insufficient for repairing radial tears with a single stitch. Multiple stitches are typically required to ensure adequate stability for these types of tears.21,29
The MME is considered to vary depending on the knee flexion angle and measurement location.9,27 In this study, the amount of MME was significantly greater at 90° of knee flexion than at 30°, particularly when measured posterior to the MCL. This finding aligns with those of previous studies. Farivar et al 9 demonstrated that MME increased at deeper knee flexion angles and was most pronounced in the posterior region of the MCL when measured using ultrasound and fresh-frozen cadavers. Amano et al 1 also reported the importance of decreasing MME at the posteromedial corner. Similarly, Melugin et al 23 reported that increased knee flexion angles heightened medial shear forces on the posterior root of the MM in a porcine model. Furthermore, Sukopp et al 36 demonstrated in a human cadaveric model that limiting knee flexion in the early postoperative phase reduced the mechanical stress on meniscal repairs, thereby minimizing shear forces and extrusion. This underscores the need to evaluate knee flexion angles and measurement locations under physiological conditions and adopt controlled rehabilitation strategies. Limiting excessive knee flexion during rehabilitation may help reduce shear forces and extrusion, preserving repair integrity.
Abnormal MME is often defined as exceeding 3 mm.4,6 In our study, MME in complete radial tears of the posterior MM did not exceed this threshold. Similarly, Farivar et al 9 reported that medial meniscus posterior root tears (MMPRT) alone did not result in abnormal MME unless combined with a meniscotibial ligament (MTL) tear, which caused MME to exceed 3 mm in a cadaveric model. Doan et al 8 found that the mean MME in MMPRT with an MTL tear was approximately 2.5 mm and associated with increased contact pressure and reduced contact area in the medial tibiofemoral compartment. They also noted that the MMPRT with MTL tear state caused greater contact pressure and a smaller contact area compared with the MTL tear state alone. Debieux et al 7 demonstrated that MME >4 mm significantly decreased the medial tibiofemoral contact area, while 3 mm did not result in a significant reduction. Although the posterior tear of the MM in our study did not reach abnormal MME levels and the observed differences were relatively small, these findings are clinically significant, as they provide insight into the meniscal repair techniques under physiological conditions. While the inside-out repair technique demonstrated superior performance in reducing MME, it requires a posteromedial approach for the posterior segment, adding to the clinical complexity. This trade-off should be weighed carefully in clinical decision-making.
Limitations
This study had some limitations. First, we used only a single horizontal stitch for tears in the medial meniscal posterior segment, which may have been insufficient. However, we aimed to examine the effect of individual sutures, and we believe this objective was achieved. Future studies should investigate the effects of multiple and more complex meniscal repair techniques. Second, the needles for the all-inside and inside-out techniques were passed twice through the meniscus. Therefore, random suturing was performed to reduce the effect of passing the needle twice. While randomization was performed to reduce the potential effect, we acknowledge that it might still have influenced the measured MME values. Third, although no macroscopic degeneration or damage to the meniscus or cartilage was observed during the experiments, the use of specimens from older donors with low-quality bone and degenerative tendons may have introduced bias. Fourth, because the study relied on cadaveric tests, the results did not account for biological healing or muscle activity. Fifth, differences in suture tightening between the all-inside and inside-out techniques may exist, and this potential variation could be a confounder. However, the all-inside technique is tightened with the maximum load that can be applied manually using a dedicated pusher, whereas the inside-out technique is not tightened with manual maximum force, but with the natural tension of the knots.
Conclusion
The inside-out repair technique decreased the amount of MME more than the all-inside repair technique using a single horizontal stitch for MM posterior segment tears. However, neither repair was able to decrease the MME to the same level as that in the intact state, and the change in MME was relatively small.
Footnotes
Final revision submitted March 5, 2025; accepted April 7, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.