
Abstract
Background:
Recurrent anterior shoulder instability often requires surgical intervention, with 2 prominent approaches: anatomic (eg, Bankart) and nonanatomic (eg, Latarjet) procedures. While most surgeons favor arthroscopic Bankart, the open Latarjet procedure offers advantages such as quicker recovery and lower redislocation rates. On the other hand, complications include postoperative pain due to an impingement between hardware and soft tissue, resolved through screw removal.
Purpose/Hypothesis:
The purpose of this study was (1) to assess the Walch-Duplay score for functional outcomes and (2) to examine Subjective Shoulder Value (SSV), Single Assessment Numeric Evaluation (SANE), and visual analog scale (VAS) scores, as well as satisfaction and return-to-sports rate. It was hypothesized that screw removal does not significantly affect functional outcomes.
Study Design:
Cohort study; Level of evidence 3.
Methods:
Clinical data from a single-operator series of 692 shoulders treated for anterior instability with Latarjet technique between 2007 and 2021 were analyzed. Those who underwent revision surgery, previously underwent surgery on the shoulder, and had concomitant shoulder injuries were excluded. A total of 530 shoulders were eligible, and of these, 41 shoulders needed screw removal (7.7%). Propensity score matching yielded 41 pairs of shoulders split between the screw removal and no revision group.
Results:
At a mean follow-up of 85.0 months, the Walch-Duplay functional score was 76 ± 19 (median, 80; range, 15.0-100.0) and 81 ± 22 (median, 85; range, 0.0-100.0) ) in patients for no revision and screw removal, respectively (P = .15); SSV was 82 ± 15 (median, 85; range, 40.0-100) and 86 ± 14 (median, 90; range 40.0-100.0) (P = .14), respectively; SANE was 89 ± 19 (median, 100; range 0.0-100.0) and 89 ± 14 (median, 95; range 50.0-100) (P = .16), respectively; and VAS was 0.7 ± 1.3 (median, 0; range, 0-5) and 1.1 ± 1.5 (median, 1; range 0-5) (P = .06). Satisfaction and return-to-sport rates were statistically significantly lower in the screw removal group (P = .03 and P = .04, respectively).
Conclusion:
Our results confirm that screw removal after the open Latarjet procedure does not substantially affect functional outcomes. However, we acknowledge a lower return to sports and worse satisfaction scores in the screw removal group.
Recurrent anterior shoulder instability is considered a common indication for surgical intervention, particularly among young adults and athletes. 3 Within the spectrum of surgical techniques for anterior shoulder instability, the 2 most prominent approaches are the “anatomic,” involving the repair of soft tissue to the glenoid, such as the arthroscopic Bankart, 18 and the “nonanatomic,” which entails the placement of a bone block, using coracoid process bone graft typically on the anteroinferior edge of the glenoid through a division in the subscapularis muscle, as seen in the open Latarjet procedure. 9
For many surgeons, there is a notable preference for the arthroscopic Bankart procedure. 24 However, when compared with the arthroscopic Bankart procedure, open Latarjet procedure has shown faster recovery times with quicker return to sports, a lower redislocation rate (<5%), and favorable long-term outcomes.4,21 Some complications include malpositioning of the bone graft, malunion, neurological dysfunction, anterior pain with focal sensitivity, and lysis of the graft. 8 These last 2 complications can be attributed to the impingement arising between the head of the upper screw, exposed due to the lysis of the bone block, and the soft tissues (subscapularis), leading to anterior shoulder pain. And in the case of a screw’s being too long, the tip of the screw could impinge on the infraspinatus or the suprascapular nerve, which could be responsible for posterior shoulder pain.6,16 This “complication” can be effectively resolved through screw removal, a procedure conducted in 3% to 5% of all Latarjet patients.11,19
Contemporary literature features numerous descriptive studies, case series, meta-analyses, and even arthroscopic techniques that describe both short-term and long-term outcomes resulting from screw removal because of anterior pain.11,14,15,17,23 To date, there have been no published cohort studies that have examined and compared whether patients undergoing screw removal surgery after Latarjet surgery exhibit similar functional outcomes to unrevised patients.
The objective of this study was to compare the long-term clinical results between patients undergoing screw removal versus patients who did not require screw removal. The first endpoint of this study was to evaluate the functional outcome of the Walch-Duplay score between the 2 groups. The second endpoint was to evaluate the outcomes of the Subjective Shoulder Value (SSV), Single Assessment Numeric Evaluation (SANE), and visual analog scale (VAS) scores as well as the satisfaction and return-to-sport rate. Our hypothesis was that removing material due to anterior or posterior shoulder pain would not adversely affect the final functional outcomes of patients.
Methods
Study Design
This is a retrospective, single-center, single-operator cohort study. A registry composed of 692 shoulders operated between 2007 and 2021 with the surgical procedure of open Latarjet in the context of anterior shoulder instability were analyzed. 2 The registry complies with French regulations on research involving human participants in accordance with the Jardé Law and the referenced MR-004 methodology (CNIL). A retrospective evaluation protocol was established and approved by the institutional review board of the SOciété Française de Chirurgie Orthopédique et Traumatologique).
The inclusion criteria for this study were any patient operated for anterior shoulder instability with the Latarjet procedure between the years 2007 and 2021. From this cohort, the following patients were excluded: those with <1-year follow-up, revision surgery for instability, revision surgery for other reasons (hematoma, infection, and malunion), patients who had previous shoulder surgery, and patients with any known concomitant injury of the shoulder.
The aim was to create 2 comparable groups with balanced confounding factors. Matching was carried out according to the following criteria: sex, age at inclusion (categorized as ≤40 or >40 years), type of surgery (open Latarjet or arthroscopic Latarjet), time from first dislocation to surgery (<2, 2-5, or >5 years), number of dislocations before surgery (<2, 2-4, or >4), sports classification (according to the American Academy of Professional Coders) 20 and dominant arm operated. Shoulders within the no revision group (n = 489) were matched to those from the screw removal group (n = 41) by nearest neighbor matching, with a caliper value of 0.2 of the pooled standard deviation of the logs of the propensity score. Standardized mean differences (SMDs) were calculated to compare baseline characteristics after matching. A postmatching SMD <0.1 was considered an acceptable difference.
Database
Postoperative follow-up was conducted by the surgical team in collaboration with the department’s sports physician at 1 month and 3 months, until the shoulder regained full range of motion, allowing for a gradual return to sports activities. A questionnaire was sent by email to collect the clinical evolution at the last follow-up with an evaluation of the range of motion in external and internal rotations, forward elevation, pain (VAS), functional scores (Walch-Duplay, SSV, SANE),10,25,27 satisfaction (yes or no), return to sport (same level, lower level, no more sport), complications, and whether a surgical revision was needed. In case of complications, recurrences, or discrepancies found in the questionnaire, a telephone call or a telemedicine consultation was organized with the patient. All data were collected by junior surgeons (J.E.C. and M.H.).
Statistical Analysis
Statistical analysis was carried out using EasyMedStat software (Version 3.42; www.easymedstat.com). A Fisher exact test was used to evaluate the differences between the 2 groups after matching. Data were expressed as mean ± SD. The significance level was set at P < .05.
Assessment and Screw Removal
All patients were reoperated because of persistent pain ≥1 year after the Latarjet procedure. Screw impingement was suspected clinically when the belly press test was painful and associated with anterior pain. Suprascapular nerve irritation was suspected if the screws were too long outside the posterior cortex of the glenoid on the Bernageau view and were associated with posterior pain. 14 Some patients who experienced residual unexplained pain were also proposed to remove hardware as suggested by Godenèche et al. 11
Out of the 41 reviewed patients, 25 underwent screw removal using an arthroscopic technique: the arthroscope was introduced through the posterior portal at the soft point, and instruments were inserted through the anterolateral portal within the rotator interval and or through a subscapularis split. A systematic evaluation was performed to assess the position of the bone block, signs of glenoid cartilage injuries, or rotator cuff tears, but no additional procedures were performed except debridement of the anterior capsule to locate the screws. Twelve patients underwent screw removal via open surgery with the resumption of the 4-cm vertical deltopectoral approach. The former horizontal split in the subscapularis muscle belly was identified and recreated with respect to the conjoined tendon medially. The anteroinferior glenoid and the 2 screws in the bone block were exposed without capsulotomy. Then, the 2 screws were removed. Four patients needed a switch from arthroscopic extraction to an open technique due to difficult access to the screws. 17
Postoperative Instructions
All patients underwent routine anteroposterior and lateral radiographs of the shoulder to confirm that screw removal was complete, and a simple sling support was utilized for 2 days or until pain relief was achieved. Patients were instructed to begin self-rehabilitation exercises following a standard protocol starting 1 day after surgery.
Results
Main Characteristics of the Population
A total of 692 shoulders were operated for anterior instability with the Latarjet procedure, and 530 shoulders were eligible for this study, including 521 open Latarjet and 9 arthroscopic Latarjet. Of these eligible shoulders, 41 were revised for screw removal (7.7%). The mean time to screw removal after the Latarjet procedure was 3.7 ± 3.0 years. These 41 shoulders were matched to those free from any revision surgery. The final population consisted of 41 matched pairs, giving a total of 82 shoulders (Figure 1).

Study flowchart.
Table 1 describes the general characteristics of the population and shows that the matching process balanced the covariates between the 2 groups.
Descriptive and Epidemiologic Characteristics of the Study a

Data are presented as mean ± SD or No. (%).
Classification of the American Academy of Pediatrics Committee (AAPC) on Sport Medicine and Fitness
Functional Results
At a mean follow-up of 85.0 months, the functional score Walch-Duplay in patients in the no revision and screw removal groups was 76 ± 19 (median, 80; range, 15.0-100.0) and 81 ± 22 (median, 85; range, 0.0-100.0), respectively (P = .15). Similarly, SSV was 82 ± 15 (median, 85; range, 40.0-100) and 86 ± 14 (median, 90; range, 40.0-100.0) (P = .14), SANE was 89 ± 19 (median, 100; range, 0.0-100.0) and 89 ± 14 (median, 95; range, 50.0-100) (P = .16), and VAS was 0.7 ± 1.3 (median, 0; range, 0-5) and 1.1 ± 1.5 (median, 1; range, 0-5) (P = .06), respectively, for the no revision and the screw removal groups. Satisfaction and return-to-sport rates were statistically significantly lower in the screw removal group (P = .03 and .04, respectively) (Table 2).
Functional Results at Last Follow-up a
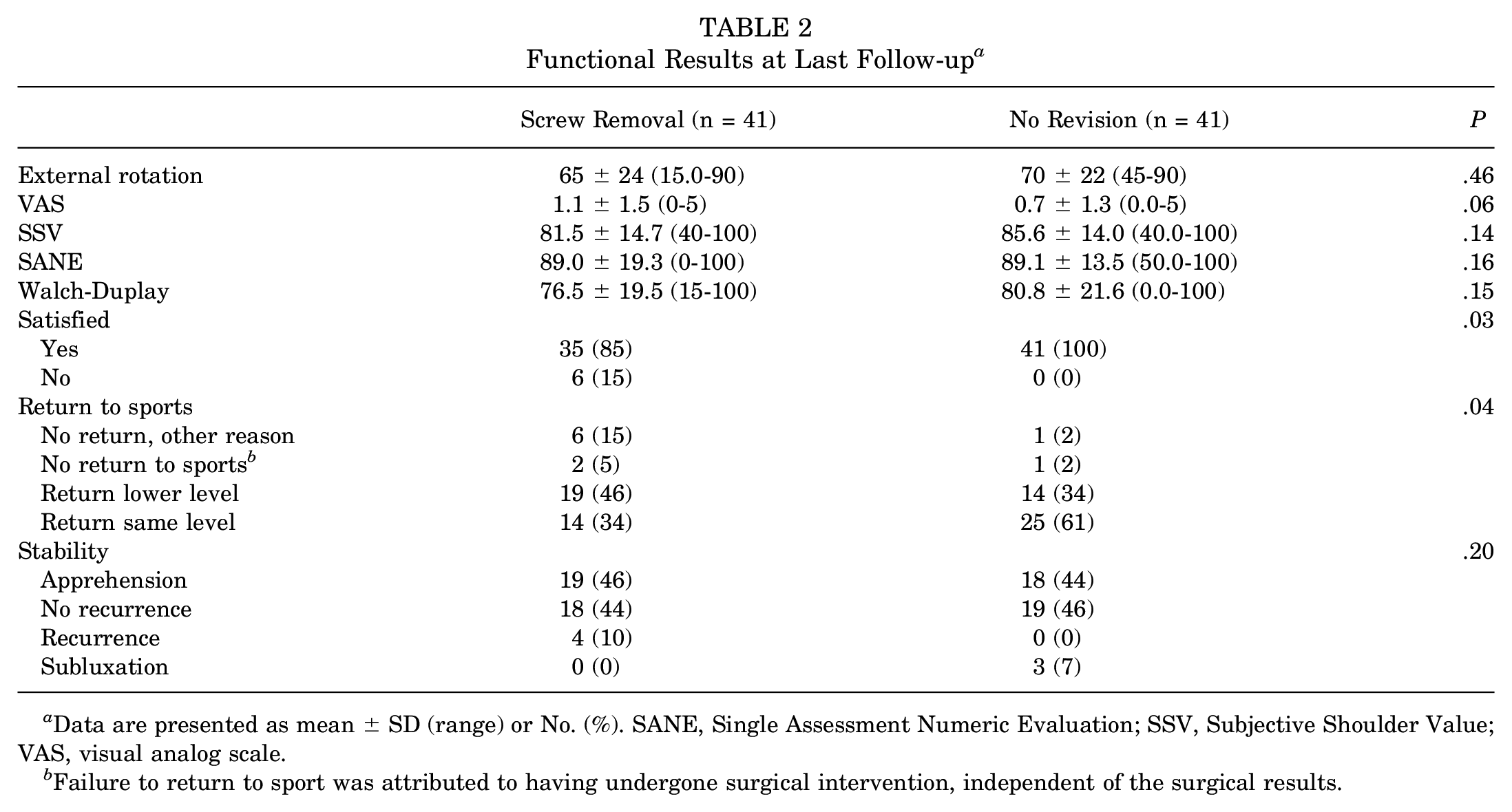
Data are presented as mean ± SD (range) or No. (%). SANE, Single Assessment Numeric Evaluation; SSV, Subjective Shoulder Value; VAS, visual analog scale.
Failure to return to sport was attributed to having undergone surgical intervention, independent of the surgical results.
In the screw removal group median VAS prerevision and VAS postrevision was, respectively, 3.0 (IQR, 2.0) and 1.0 (IQR, 1.0). The median difference was 2.0 (IQR, 3.0; 95% CI, 2.0-3.5; P < .001) (Figure 2).
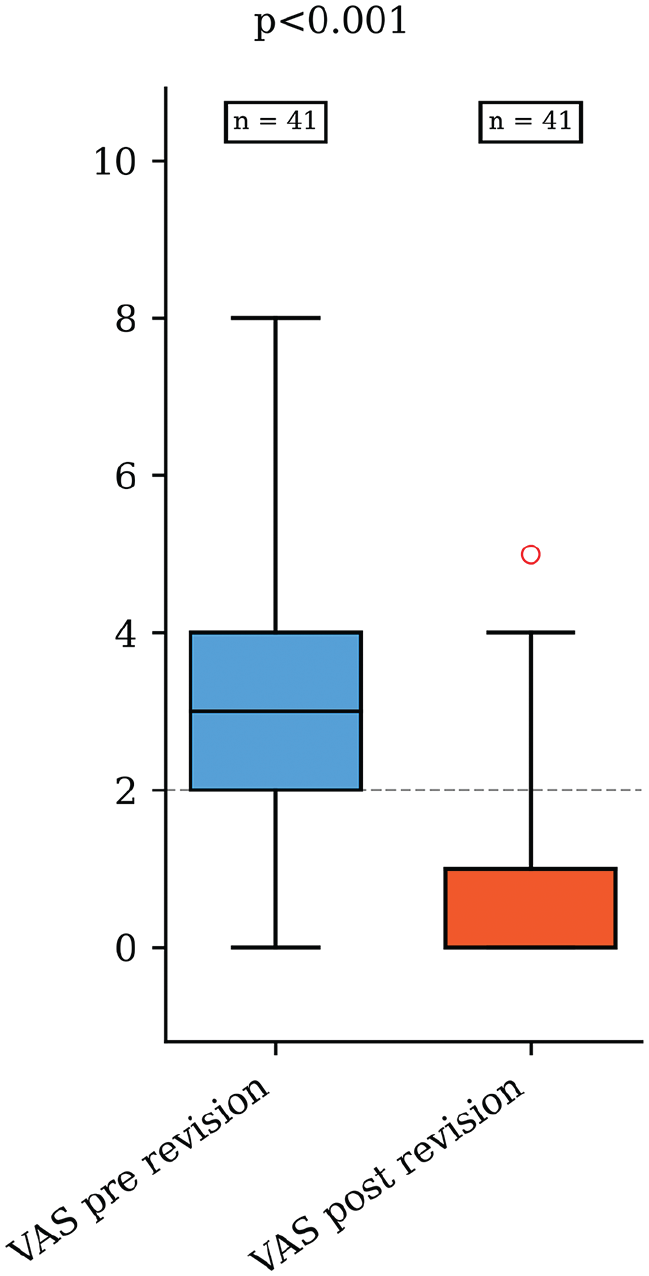
Comparison of pre- and postrevision pain for the screw removal group.VAS, visual analog scale. The central line within each box represents the median, the boxes indicate the interquartile range (25th–75th percentiles), and the whiskers extend to the minimum and maximum values within 1.5× the IQR. The red dot represents an outlier, defined as a value greater than 1.5 times the interquartile range above the third quartile. In this case, one patient reported a higher post-revision VAS score than the rest of the cohort.
Complications
In the screw removal group, superior bone lysis around the screw was observed in 33 patients (80%), with only 3 having complete lysis. Recurrent dislocation occurred in 4 patients in the screw removal group.Of the 2 patients with epilepsy, 1 experienced dislocation after screw removal, while the other did so before. The mean time from screw removal to dislocation was 2 months.
Discussion
The main finding in our study largely supports our initial hypothesis that screw removal in patients undergoing a Latarjet surgery would not negatively affect their functional outcomes. However, we acknowledge a lower return to sports and worse satisfaction scores in the screw removal group. With a mean follow-up of 85 months, ranging from 17 to 171 months, no significant difference was found between the screw removal group and the no revision group regarding the Walch-Duplay score. Moreover, we did not observe any significant differences in the other functional outcomes, such as SSV, SANE, and VAS. Therefore, the need for screw removal did not have major long-term detrimental effects. However, return-to-sport rates and patient satisfaction scores were lower in those who underwent screw removal. This may be due to persistent discomfort before the revision, psychological apprehension about shoulder stability, or a longer recovery period that discouraged a full return to preinjury activity levels. In general, after screw removal, no postoperative restrictions are required, and patients may resume all sports activities after 2 weeks, once the wound has healed.
A systematic review described by Griesser et al 12 showed that the number of Latarjet patients requiring reoperation was low (7%) (132 of 1913 shoulders) and that 2.4% (46 of 1913 shoulders) were related to symptomatic hardware removal, supporting the results of our study where there was a 7.7% reoperation due to symptomatic hardware removal. This rate is slightly higher than what has been previously reported in the literature.11,12 The higher proportion of screw removals in our study compared with the published range in the literature could be attributed to the long-term follow-up and the possibility for the patients to show up late with their pain.
Although there is no statistical significance, it is relevant that patients in the screw removal group experienced slightly higher levels of pain than the no revision group, 0.7 ± 1.3 (median, 0; range, 0-5) and 1.1 ± 1.48 (median, 1; range 0-5) (P = .06), respectively. Some of the higher VAS scores in the screw removal group may have been due to the source of pain being something other than the screw, such as chondral damage or scar tissue, and so forth. It should also be noted that the no revision group was selected based on the “best Latarjet cases” without any complications or revision. Godenèche et al 11 reported on 461 shoulders treated for anterior instability by open Latarjet, in which 21 (5%) experienced anterior focal pain without recurrence of instability. Of this partial cohort, screw removal alleviated pain in 14 of 21 shoulders (67%) and reduced pain in the remaining 7 (33%). In contrast, in our cohort, 56% still had some pain at the end of the follow-up. It is worth noting that only 5 patients (12%) reported a pain score greater than 3 on the visual analog scale (VAS), of which 1 suffered several episodes of recurrence due to seizures. Notice that when comparing VAS prerevision versus VAS postrevision within the screw removal group, the difference was statistically significant for VAS postrevision.
On the other hand, the satisfaction rate in the screw removal group was statistically lower than that in the non-revision group. It seems that the necessity for a second surgery (even if minor) was perceived negatively by the patients. It is important to note, however, that partial lysis of the coracoid, which was observed in 80% of the revised patients, was a frequent finding and did not increase the apprehension rate. Di Giacomo et al 7 reported that graft resorption rarely leads to persistent apprehension and unsatisfactory outcomes. However, it should be clarified that no hardware removal patients were evaluated in his work. It is also important to note that satisfaction is a subjective indicator and can be influenced by various factors, including pain, which was slightly higher in this group.
When analyzing the return-to-sports activity, we observed a statistically significant difference between the no revision group and the screw removal group (P = .04). We have limited evidence on this topic, which makes it difficult to compare our results with existing literature, and our limited data do not allow us to draw any conclusions.
Based on a study with a follow-up of 3.8 years, it was found that the rate of return to sports after open Latarjet procedure varied depending on the level of sports practiced. The study showed that all 57 (100%) competitive athletes and 34 (69.4%) recreational athletes were able to resume their previous level of sports participation or a lower level than before their injury (78.9% vs 42.9%; P= .004). 3 Unfortunately, we found no significant differences to support our hypothesis on this subject. Further research is needed to explain these results.
To avoid the need for screw removal, it is possible to look at resorbable screws. However, these resorbable screws present 2 notable drawbacks: first, fixation is more fragile 26 ; second, coracoid graft osteolysis appears to be exacerbated with a risk of complete disappearance. 1 Resorbable screws are no longer recommended. To avoid screw- and met al-related complications in Latarjet procedures, several bone block fixations have been described, such as suture buttons, suture cerclage, and suture anchors. 22 The suture button is especially interesting under the arthroscopy technique, as it does not require a posterior approach. The button fixation significantly reduces the number of revision surgeries, whereas 6% of screw fixations require revision surgery to remove the implant. However, recurrent instability is more frequent in suture button fixation than screw fixation (8.3% vs 2.5%; P = .02) 13 and bone block fusion requires more time using suture button fixation compared with screw fixation, delaying the return to sports. 5
Strengths and Limitations
The strengths of our study include the large number of patients we were able to analyze who underwent hardware removal after an open Latarjet procedure, as compared with a control group of nonrevised patients. Another strength is the 7-year follow-up period, which is longer than previous clinical studies on this complication, to the best of our knowledge. The study has some limitations, including its retrospective, nonrandomized design and treatment selection bias. The other limitations included a lack of data on the amount of bone absorption in the no revision group, no matching based on chondral injury, and no preoperative evaluation ensuring pain was coming from prominent screw impingment (ie, diagnostic injection). The treatment and control groups in this study were matched based on preoperative criteria before the original Latarjet procedure. The results and conclusions were presented and made based on final follow-up functional scores for each group.However, we could address these limitations by successfully using propensity matching. Another important limitation was the proportion of patients lost to follow-up.Additionally, we could not conduct physical examinations or radiological follow-ups at the final check-up due to the geographical relocation of many patients.
Conclusion
In this long-term medical study, our key findings largely support our initial hypothesis that screw removal after Latarjet surgery does not significantly impair functional outcomes or recurrence rate. No significant differences were observed in functional parameters such as Walch-Duplay, SSV, SANE, and VAS scores. However, patient satisfaction and the return-to-sports activity were significantly lower in the screw removal group.
Footnotes
Final revision submitted March 9, 2025; accepted March 17, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.B. has received consulting fees from Arthrex, SBM, and Move Up and royalties from SBM and Move Up. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from SOciété Française de Chirurgie Orthopédique et Traumatologique (No. IRB-SOFCOT 14-2023).