
Abstract
Background:
Osteochondral allograft (OCA) transplantation is an established surgical intervention for full-thickness chondral defects. Standard preservation (SP) protocols currently allow for OCAs to be stored for a maximum of 28 days after procurement before significant chondrocyte death. An alternative protocol, the Missouri Osteochondral Allograft Preservation System (MOPS), has been shown to allow for grafts to be stored for twice the maximum time allotment as SP.
Purpose:
To compare clinical outcomes in patients who have undergone OCA transplantation utilizing the extended storage capabilities of the MOPS versus SP protocols.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent OCA transplantation from 2012 to 2018 were retrospectively identified. Patients without appropriate follow-up, postoperative outcomes, or necessary preoperative imaging were excluded. All patients had at least 2 years of follow-up data. Patient characteristics, outcomes, and graft information were compared between patients who received grafts preserved by MOPS versus SP as previously defined.
Results:
In total, 64 patients were included: 25 were in the MOPS group and 39 in the SP group. Members of the MOPS group were significantly younger at the time of surgery than those in the SP group (28.6 ± 10.7 years vs 36.7 ± 10.9 years; P = .005). In total, 78 grafts were analyzed with 39 grafts in the MOPS group and 39 in the SP group. Grafts in the MOPS group had significantly longer (mean, 50.03 days) storage duration than grafts in the SP group (mean, 23.18 days) (P < .001). Preoperative patient-reported outcomes showed no statistically significant differences between the Knee injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS, JR) values, International Knee Documentation Committee (IKDC) scores, Physical Component Summary (PCS-12) scores, and Mental Component Summary (MCS-12) scores. Two-year outcome between groups showed no statistically significant differences in mean KOOS, JR values (81.4 ± 14.1 in the MOPS group vs 78.5 ± 16.2 in the SP group; P = .467), IKDC scores (74.3 ± 19.8 in the MOPS group vs 66.4 ± 18.4 in the SP group; P = .128), PCS-12 scores (48.7 ± 9.94 in the MOPS group vs 48.0 ± 9.83 in the SP group; P = .683), and MCS-12 scores (53.4 ± 8.92 in the MOPS group vs 50.6 ± 11.8 in the SP group; P = .583). There were no statistically significant differences in failure rates (20% in the MOPS group vs 17.95% in the SP group; P = .838) or complication rates (8% in the MOPS group vs 5.13% in the SP group; P = .643).
Conclusion:
OCAs preserved using the MOPS can be stored at greater than twice the storage duration of grafts preserved with SP techniques without a significant difference in postoperative outcomes.
Keywords
Full-thickness cartilage defects of the knee commonly involve the surface, subchondral bone, and articular cartilage. 11 Treatment options for management vary based on factors such as location, size, depth, patient activity level, patient age, and concomitant knee pathologies. 8 After nonoperative management fails, surgical intervention is utilized because articular cartilage has limited regenerative capacity due to poor vascularity. Surgical options include chondroplasty, marrow stimulation techniques, osteochondral autograft transfer, osteochondral allograft (OCA) transfer, and cell-based repair such as autologous chondrocyte implantation.3,8,13,15,26 OCA transplantation uses size-matched allograft cartilage and subchondral bone to repair focal chondral and osteochondral defects with a goal of restoring function and decreasing pain. OCA transplantation has several advantages, including implantation of immediately viable hyaline cartilage, restoration of the entire osteochondral unit, no donor site comorbidities, and earlier return to sport than autologous chondrocyte implantation.3,7,8,13,15,27
Despite advantages, OCA transplantation carries limitations such as allograft availability. 8 Previous studies have demonstrated that a 70% chondrocyte viability is essential for successful outcomes with OCA transplantation.5,6,9,17,19 Standard preservation (SP) methods demonstrate significant declines in viability 14 days after procurement and further declines below the 70% threshold by 28 days after procurement. This 28-day window becomes further limited by mandatory disease screening protocols that take a minimum of 14 days to complete before the OCAs can be released for use by the surgeon.1,5,6,10,12,14,18,22,25 In lieu of this, a novel preservation technique was developed to maintain chondrocyte viability above that 70% threshold for longer periods of time as compared with SP. The Missouri Osteochondral Allograft Preservation System (MOPS) utilizes a serum-free tissue preservation method in which grafts are stored in a solution at room temperature (approximately 25°C). MOPS has been validated through several studies to maintain chondrocyte viability >70% for at least 56 days after procurement.5,6,21 A recent study by Buyuk et al 2 found that patellofemoral shell OCA grafts preserved with MOPS had better short-term outcomes, with a 98% 2-year graft survival rate, compared with 83% for those preserved with SP. OCA transplantations in this study were performed to treat the entire articular surface of the patella, trochlea, or both. 2 Stannard and Cook 20 also found that grafts prepared via the MOPS protocol were associated with lower revision and failure rates along with better 3-year postoperative International Knee Documentation Committee (IKDC), Single Assessment Numeric Evaluation, and Patient-Reported Outcomes Measurement Information System Mobility scores compared with those preserved with SP. OCA transplantations in this study were performed as primary unipolar, multisurface, or bipolar depending on patient indication. 20
The purpose of this study was to compare outcomes in patients who have undergone OCA transplantation utilizing the extended storage capabilities of the MOPS versus SP protocols. We hypothesized that there would be no difference in outcomes between MOPS and SP techniques for OCA transplantation.
Methods
Inclusion and Exclusion Criteria
Our study protocol was approved by our institutional review board. This was a retrospective study reviewing all patients who underwent OCA transplantation between January 1, 2012, and December 31, 2018, with a minimum 2-year follow-up at a single institution. Patients were identified by Current Procedural Terminology code 27412 from our institutional records and excluded if they did not have appropriate follow-up, postoperative outcomes, or necessary imaging. Demographic information was collected via chart review for age, sex, race, ethnicity, and body mass index (BMI).
Data Collection
Chart review was performed on all eligible OCA transplant patients to collect injury information, lesion characteristics, and operative details including graft information and preservation, as well as subjective and objective outcome scores. Clinic notes were reviewed to determine primary etiopathogenesis, date of injury, and preoperative treatments. Outcome scores including the Knee injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS, JR), IKDC score, Physical Component Summary (PCS-12) score, and Mental Component Summary (MCS-12) score were submitted via patient-reported surveys and collected from the Outcomes Based Electronic Research Database. Subjective reports of range of motion, crepitation, and any complications or revisions were also collected from patient charts and follow-up reports.
Data Analysis
Outcomes were compared in patients who received grafts that were preserved utilizing SP and MOPS methods for OCA. Chi-square analysis and t tests were used for the appropriate categorical and continuous variables. All statistical analysis was done using R (Version 3.6.3). Statistical significance was set at a P value <.05, and power was set to 0.80.
Patient Management
Preoperative Management
Preoperative patient management does not vary based on type of graft used. Patients are prescribed and follow a specific physical therapy regimen to prepare them for surgery. Therapists take patients through specific exercises to ensure patients gain full range of motion, decreased swelling, and overall increased lower extremity strength/stability when compared with previously. Areas of primary attention are paid to the lower core muscles, hip stabilizers (emphasis on the gluteus medius), quadricep muscles, hamstring muscles, and gastrocnemius muscles. These goals function as a checkpoint before a patient is considered appropriate for elective surgery.
Procedure
The procedure does not vary based on type of graft used.
Once the site is fully exposed with adequate preparation of the area of the chondral defect, the process of transplantation occurs in the sequence shown in Figure 1.

Transplantation technique. OCA, osteochondral allograft.
Postoperative Management
Postoperative patient management does not vary based on type of graft used. Patients start performing physical therapy on postoperative day 2. The main goal of postoperative therapy is to regain full range of motion and stability by taking the patient through a set of regimented checkpoints. Therapists take patients through straight leg raises and isometric strengthening with Russian electric stimulation and blood flow restriction for 6 weeks and then progressive resistance exercises of the leg and hips. For the first 6 weeks after surgery, patients are nonweightbearing or toe-touch weightbearing only. After the first 6 weeks, patients are then transitioned to weightbearing as tolerated with both crutches, then weightbearing as tolerated with 1 crutch, and then no crutches. During this time, pain management is set as needed with over-the-counter acetaminophen and ibuprofen for breakthrough pain. Patients remain in a total range of motion brace for 4 to 6 weeks postoperatively until good quadriceps, leg, and hip control.
Results
Study Population
A total of 64 patients were identified for analysis based on appropriate inclusion and exclusion criteria. Of these, 25 patients belonged to the MOPS group with 41 defects identified requiring 39 total grafts, and 39 patients belonged to the SP group with 61 defects identified requiring 39 total grafts (Figure 2).

CONSORT (Consolidated Standards of Reporting Trials) flow diagram. MOPS, Missouri Osteochondral Allograft Preservation System; OCA, osteochondral allograft; SP, standard preservation.
The mean age of all included patients in the study was 33.5 ± 11.4 years, and 51.6% were female. Members of the MOPS group were significantly younger at the time of surgery than those in the SP group (28.6 ± 10.7 years vs 36.7 ± 10.9 years; P = .005) and had a significantly lower mean BMI (25.1 ± 3.53 kg/m2 vs 27.9 ± 4.28 kg/m2; P = .007). Members of the MOPS group had significantly more patients with bone cyst pathology than the SP group at 14 (58.3%) and 10 (27.8%), respectively (P = .036). The groups had no statistically significant differences in other demographics such as sex, multisurface transplantations, Outerbridge classification, the mean number of defects, or follow-up time (Table 1). Graft selection was surgeon dependent, and most grafts were selected based on graft offer availability for the surgery.
Patient Characteristics a

Data are presented as n (%) or mean ± SD. Bold P values indicate significance. BMI, body mass index; MOPS, Missouri Osteochondral Preservation System; SP, standard preservation.
Data missing for both groups.
Graft Characteristics
A total of 78 grafts were identified and analyzed among the study population: 39 grafts were preserved before surgery using the MOPS protocol and 39 grafts were preserved using SP. The mean graft areas were similar between groups (401.76 ± 211.64 mm2 in the MOPS group vs 425.06 ± 161.79 mm2 in the SP group; P = .590), as was the mean diameter of the grafts (20.03 ± 3.99 cm in the MOPS group vs 18.73 ± 3.31 cm in the SP group; P = .127). The mean storage time of grafts was significantly different, with grafts preserved using MOPS being stored for longer (50.03 ± 4.01 days in the MOPS group vs 23.18 ± 3.81 days in the SP group; P < .001). Graft source location was identified and stratified as well and did not demonstrate a significant difference between groups (Table 2).
Graft Characteristics a
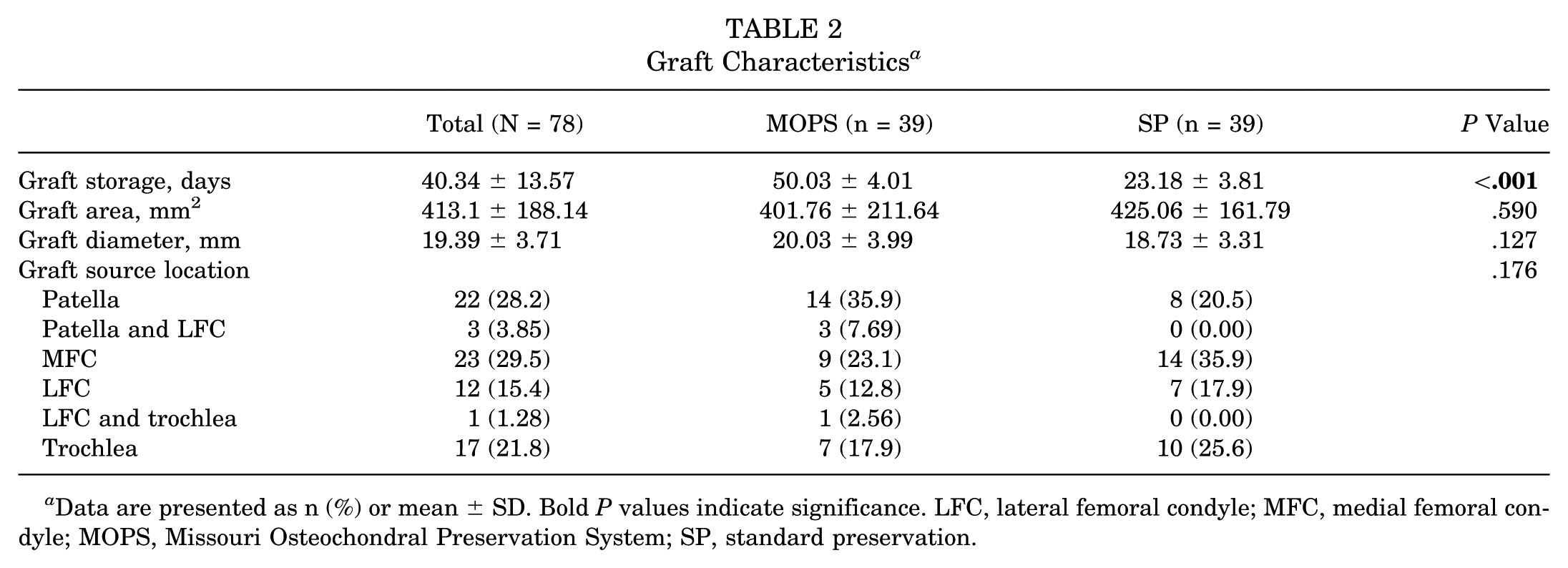
Data are presented as n (%) or mean ± SD. Bold P values indicate significance. LFC, lateral femoral condyle; MFC, medial femoral condyle; MOPS, Missouri Osteochondral Preservation System; SP, standard preservation.
Defect Characteristics
A total of 102 defects were identified and analyzed among the study population. In total, 41 defects were identified as belonging to the MOPS group and 61 defects were identified as belonging to the SP group. The mean defect size at time of implantation was similar between groups (3.81 ± 2.39 cm2 in the MOPS group vs 3.57 ± 2.02 cm2 in the SP group; P = .609), with no significant differences found in the location of defects (Table 3).
Defect Characteristics a

Data are presented as n (%) or mean ± SD. MOPS, Missouri Osteochondral Preservation System; SP, standard preservation.
Outcomes
Outcomes were recorded for the 64 patients and analyzed based on preservation technique utilized for the graft they received. Four patient-reported outcome measures (PROMs) were used for postoperative assessment: KOOS, JR, IKDC score, PCS-12 score, and MCS-12 score. The mean PROM scores did not statistically differ between treatment groups in either the preoperative or postoperative scoring. Within both treatment groups, there was statistical improvement from preoperatively to postoperatively, except for in the MCS-12 score (Table 4).
Outcomes a
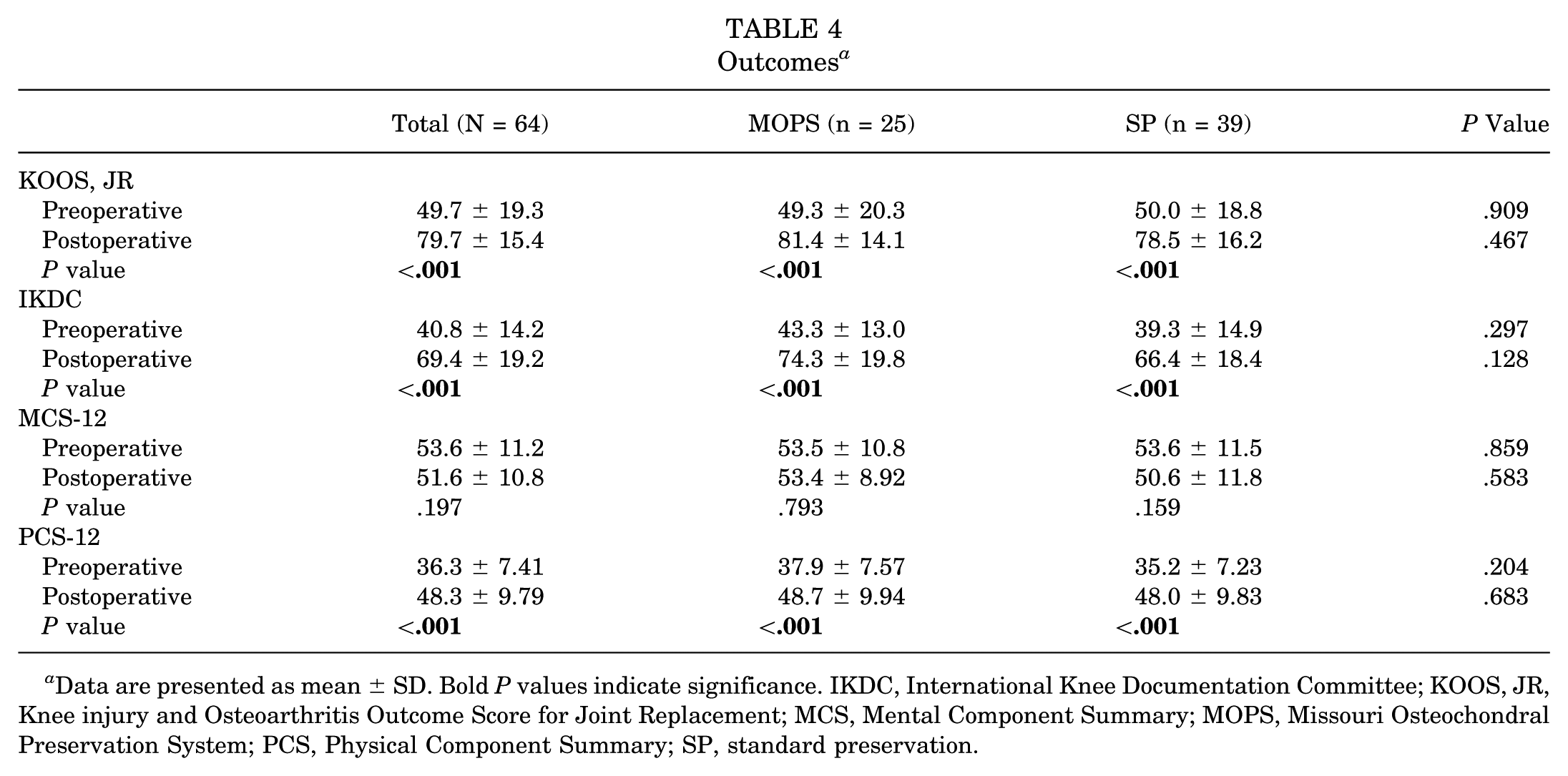
Data are presented as mean ± SD. Bold P values indicate significance. IKDC, International Knee Documentation Committee; KOOS, JR, Knee injury and Osteoarthritis Outcome Score for Joint Replacement; MCS, Mental Component Summary; MOPS, Missouri Osteochondral Preservation System; PCS, Physical Component Summary; SP, standard preservation.
Failures and Complications
Failures and complications were collected for the defined follow-up period. Treatment failures are defined as revisions, reoperations, and conversions to arthroplasty. Treatment complications are defined as any other unexpected outcome. There was no statistical difference identified between treatment groups when assessed for failures and complications. MOPS group failures included 1 revision for graft failure, 2 revisions for the graft failing to incorporate, 1 conversion to total knee arthroplasty, and 1 instance of chondroplasty. MOPS group complications included 2 instances of arthrofibrosis not requiring reoperation. SP group failures included 2 revisions for graft failure, 2 conversions to total knee arthroplasty, and 3 instances of chondroplasty. SP group complications included 1 instance of deep vein thrombosis and 1 instance of pulmonary embolism (Table 5).
Complications and Reoperations a

Data are presented as n (%). MOPS, Missouri Osteochondral Preservation System; SP, standard preservation.
Discussion
This study serves to support the consensus that grafts preserved using the MOPS protocol perform similarly to those preserved using the SP protocol across key patient-reported outcomes and objective complications regardless of defect characteristics. These findings should aid orthopaedic surgeons in the decision-making process when considering which graft types are most appropriate and accessible. With similar outcomes regardless of graft type, there is an increased potential for improving graft reserves with longer storage life.
Studies have reported OCA transplantation to show survivorship between 71% and 85% at 10 years and up to 74% at 15 years, with additional studies showing an 88% return-to-sport rate, with 79% returning to preinjury level of play.5,6 Chondrocyte viability plays a crucial role in the success of an OCA transplantation, and long-term survival hinges on an intact extracellular matrix, functional chondrocytes, and incorporation into host bone. 27 SP methods recommend a storage time <28 days before OCA transplantation. 23 Studies have shown increased rates of survival if grafts are implanted within 25 days of procurement (93% survival) as opposed to days 25 to 28 (70.4% survival). 14 Stoker et al22,23 utilized the MOPS protocol and a 56-day storage time and demonstrated a chondrocyte viability density maintained at nearly 90% with viable chondrocytes found in the entirety of the graft from the surface to the deep zone. In the present study, the mean interval between graft harvest and OCA implantation for the SP group was 23.18 days, while the MOPS group had a mean of 50.03 days (P < .001). This difference in storage time ultimately allows for more flexibility for the patient and surgeon when it comes to the timeline for repair and an overall increased cache of possible grafts, with more than twice the viability.
In their 2023 study, Buyuk et al 2 analyzed the differences in OCA transplantation for patellofemoral lesions using grafts preserved by MOPS or SP. The authors reported a significantly lower reoperation rate of 7% in the MOPS group (0% revisions, 2% chondroplasty, and 2% arthroplasty) versus 50% in the SP group (17% revisions, 0% chondroplasty, and 8% arthroplasty). Stannard and Cook 20 further reported significantly decreased reoperation rates of 7% in their MOPS group compared with 21% in their SP group in their 2020 study analyzing prospective outcomes after OCA transplantations. Our study revealed no significant difference between the groups, with reoperation rates of 12% in the MOPS group (4% revisions, 4% chondroplasty, and 4% arthroplasty) and 18% in the SP group (5% revisions, 8% chondroplasty, and 5% arthroplasty). The differences seen in statistical outcomes of reoperation rates between our study and those of Buyuk et al and Stannard and Cook can be explained partially by cohort sizes. Buyuk et al reported a MOPS cohort size of 46 and a SP cohort size of 12, and Stannard and Cook reported cohort sizes of 137 and 57, respectively; this is compared with our respective cohort sizes of 39 and 25.
Stannard and Cook 20 went on to report that regardless of graft type, patients with successful clinical outcomes showed significant improvements in PROMs at 3 to 4 years of follow-up. The authors reported an overall mean IKDC score of 74.3 at the 3-year follow-up (90.8 for the MOPS group vs 69.8 for the SP group). Our study showed no significant difference in follow-up time between the 2 groups, with a mean follow-up time of approximately 3 years, similar to the study by Stannard and Cook. At 3 years of follow-up, we found no significant difference between the PROMs of the 2 groups, with an overall mean IKDC score of 69.4 (74.3 for the MOPS group vs 64.4 for the SP group; P = .128). 20 Cook et al 4 also evaluated PROMs in their 2022 study; however, they solely evaluated the differences between the preoperative and postoperative scores of the MOPS versus SP groups and did not analyze the postoperative scores of the 2 groups against each other. They reported significant improvements in the postoperative PROMs of the MOPS group but not the SP group, with final follow-up IKDC scores of 71.1 for the MOPS group and 54.2 for the SP group. Buyuk et al 2 only collected PROMs for the MOPS group in their study, but they reported a 3-year follow-up mean IKDC score of 70.3.
Observational differences in age and BMI can be seen between our study and those reported in the previous studies. Buyuk et al 2 reported an overall mean age and BMI of 36.7 years and 28.9 kg/m2, respectively, between their 2 groups, Stannard and Cook 20 reported 37.9 years and 28.9 kg/m2, respectively, and Cook et al4 reported 37.2 years and 27.7 kg/m2, respectively. Our study reported an overall mean age and BMI of 33.5 years and 26.8 kg/m2, respectively; however, there was a significant difference found in age at the time of surgery and BMI between the 2 groups in our study. The MOPS group was both younger and had a lower BMI than the SP group (28.6 vs 36.7 years and 25.1 vs 27.9 kg/m2, respectively). Nevertheless, we do not believe that differences in age and BMI contributed to the results of our study when compared with those previously mentioned. Zouzias and Bugbee 27 showed that athletes <25 years have better outcomes after OCA transplantation compared with other age groups, but in 2018 Wang et al 24 showed adequate graft survival of 73% at 4 years with clinically significant results in outcome measures for patients >40 years. These findings suggest that the differences in age seen in our cohorts would not affect the outcomes reported within this study. Furthermore, in a 2019 systematic review, Mistry et al 16 found that OCA transplantations in patients with a BMI >30 kg/m2 are comparable to those in patients with a lower BMI, with 83% graft survival at 5 years.
Limitations
The main limitations of this study stem from its retrospective design, which required extensive chart review of existing documentation. Because of this, we were unable to including chondrocyte viability assessments, assessment of patient compliance, return to sport, or overall postoperative satisfaction. These considerations prohibit definitive statements of significance and impact. With regard to radiographic limitations, the vast majority of patients did not have radiographs conducive for variable collection such as joint space or Kellgren-Lawrence grading. Furthermore, the study lacked advanced imaging reports postoperatively, preventing the assessment of graft survival at the final follow-up. Given the constrained cohorts, a power analysis was not conducted, limiting our ability to demonstrate the significance of differences. Retrospective designs inherently include biases, and while efforts were made to mitigate these, selection bias remains. The decision to include only patients with complete data resulted in a relatively small sample size, making the study susceptible to type 2 errors and raising questions about its generalizability. Additionally, within the smaller sample size of our cohort, there were differences in cohort sizes and the number of grafts used between groups. These concerns should be addressed in future studies with larger patient cohorts; however, the findings of this study demonstrate similar KOOS, IKCD, PCS-12, and MCS-12 values between the MOPS group and the SP group, with more than twice the storage life with the MOPS.
Conclusion
OCAs preserved using the MOPS can be stored at greater than twice the storage duration of grafts preserved with SP techniques without a significant difference in postoperative outcomes.
Footnotes
Final revision submitted February 17, 2025; accepted March 17, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.T. has received research support from DePuy, GID, and Pacira; consulting fees from Mitek, DePuy, Pacira, and Medical Device Business Services; is an unpaid consulting for Mitek Knee Creations; and holds stock or stock options in Johnson & Johnson. K.F. has received consulting fees from DePuy and Vericel. AOSSM checks author disclosures against the open payments database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Thomas Jefferson University (IRB 2022-0989).