
Abstract
Background:
The Gaelic games, specifically Gaelic football, hurling, and camogie, are high-intensity, level 1 field sports. However, there is a lack of data regarding the outcomes of anterior cruciate ligament reconstruction (ACLR) in Gaelic games players.
Purpose:
To evaluate the rates of return to play (RTP), ACL graft reinjury, contralateral ACL injury, and patient-reported outcome measures (PROMS) in a cohort of Gaelic footballers and hurling/camogie players at 2 years after ACLR.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A consecutive cohort of 1891 Gaelic games players who underwent primary ACLR between 2014 and 2018 was included. Patients were contacted at 2 years postoperatively with an overall follow-up rate of 93.4%. The rate of RTP, subsequent ACL injury, and PROMS were recorded. The PROMS evaluated were the Marx score, the ACL-Return to Sport after Injury (ACL-RSI), and the International Knee Documentation Committee (IKDC) score.
Results:
The mean age was 23 ± 6 years, and 73.3% of athletes were male. RTP rates were 87.8% for Gaelic football and 89.5% for hurling/camogie, with 72.7% and 76.3% of athletes returning to an equivalent or higher level of performance, respectively. Female Gaelic footballers had a slightly lower RTP rate than males (83.8% vs 89.1%; P < .016). The mean time to RTP was 10.8 ± 4 months. The rate of bone-patellar tendon-bone (BPTB) autograft reinjury was 3.3% (51/1547) versus 15.3% (33/216) for hamstring (HT) autografts (P < .001). Senior intercounty (elite) players had the lowest rate of contralateral ACL injury (8.1%, 14/173). Gaelic footballers and hurling/camogie players reported good outcomes with mean IKDC scores of 86.9 ± 9.8 versus 87.9 ± 8.9, (P = .064), mean Marx scores of 11 ± 4.7 versus 11.3 ± 4.6 (P = .309), and mean ACL-RSI scores of 74.1 ± 23.5 versus 75.8 ± 24.2 (P = .321), respectively.
Conclusion:
RTP rates among Gaelic games players were high, with the majority returning to an equivalent/higher level of performance. The rate of BPTB graft reinjury was low, considering the injury risk associated with returning to level 1 sport. Younger patients and those who underwent HT autograft reconstruction were at the highest risk of ACL graft reinjury. Overall, Gaelic games players reported good knee function and outcomes after ACLR.
Anterior cruciate ligament (ACL) injuries are common in pivoting sports such as soccer, American football, rugby, and the Gaelic games. 25 These sports are referred to as level 1 sports because they frequently involve high-intensity movements such as hard-cutting and jumping.8,13
The Gaelic games are Ireland’s traditional and most widely played sports, with >587,000 players participating across >2000 clubs in 32 county regions. 33 In addition, the Gaelic games have a significant international presence with >500 international clubs located in Great Britain, the United States, South America, mainland Europe, the Middle East, and Australasia. The male sports of the Gaelic games, which include Gaelic football and hurling, are governed by the Gaelic Athletic Association (GAA). In contrast, the female sports, Ladies Gaelic football and camogie, are overseen by the Ladies Gaelic Football Association (LGFA) and the Camogie Association (CA), respectively. Matches are contested between 2 teams of 15 players on a rectangular pitch measuring 145 × 90 metres, over 70 minutes (2 × 35–minute halves). 4 Hurling is one of the fastest and oldest field sports in the world. 7 Players use a wooden stick (“camán”) to hit a small ball (“sliotar”) into the opponent’s goal (3 points) or over a crossbar (1 point). During matches, the sliotar can reach speeds up to 160 km/h.7,26 Camogie is the female equivalent of hurling. Gaelic football and Ladies Gaelic football share similar rules, with players aiming to kick or punch the ball into an opponent’s goal or between 2 upright posts. 4 The athleticism of Gaelic football players is often compared with that of Australian Football League (AFL) players, and the 2 sports converge in a hybrid event known as the “International Rules Series” in which the best players from each code compete.15,22
The Gaelic games are deeply embedded in Irish communities, and are structured in a way that allows involvement at various levels. At the time of this study, players were divided primarily by age into: Adults, U21 (<21 years), Minor (<18 years), and Underage (<16 years). The Adult category is further divided into Senior, Intermediate, and Junior, representing different levels of competition. The best players from each club are selected to play for their respective county teams at the “intercounty” (elite) level and participate in prestigious competitions such as the All-Ireland Championship. Despite the Gaelic game’s core ethos of preserving its amateur status, intercounty players demonstrate a professional commitment by dedicating up to 31 hours per week to the sport, which includes 3 pitch training sessions and 2 gym sessions, along with team workshops/squad meetings. 9
It is estimated that ACL injuries account for 13% of knee injuries in Gaelic football and have an incidence comparable with other high-demand sports such as the AFL. 27 An analysis of the GAA injury database revealed that, over 3 years, male players made 1062 ACL injury claims, representing 5.9% of all injury claims. 31 Similarly, among female Gaelic footballers, ACL injury claims represented only 7.8% of claims but accounted for 46.7% of the injury fund’s total expense. 28
While outcomes of ACL reconstruction (ACLR) have been investigated across various sports, there is a distinct gap in the literature focusing on outcomes within the Gaelic games. The primary objective of this study was to define the rates of return to play (RTP), ACL graft reinjury, contralateral ACL injury, and patient-reported outcome measures (PROMS) after ACLR in Gaelic games players at a 2-year follow-up.
Methods
This study evaluated a consecutive cohort of Gaelic games players who underwent ACLR under 2 orthopaedic knee surgeons (R.M. and M.J.) between January 2014 and December 2018. Participants were eligible if they played Gaelic football, hurling, or camogie, were between the ages of 13 and 49 years old, and underwent primary ACLR. Patients were excluded if they had revision ACL surgery, multiligament knee surgery, or were outside of the age range. Data were collected prospectively and analyzed retrospectively. A preoperative questionnaire was completed to gather information about each patient’s characteristics, mechanism of injury, footwear type, level of sports participation, expectation for RTP, Marx Activity Score, 23 and ACL Return to Sport after Injury Scale (ACL-RSI). 36 All participants provided informed consent before their involvement in this research, and our institution granted ethical approval to undertake this study.
The Gaelic games are classified as level 1 sports according to the Cincinnati Sports Activity Scale (CSAS). Specifically, athletes engaging in sports requiring jumping, pivoting, or hard-cutting 3 to 4 days per week (CSAS score of 100) or 1 to 2 days per week (CSAS score of 85) were classified as level 1 athletes. 24 This classification also aligned with the definitions for level 1 sports previously established by Hefti et al 13 and Daniel et al. 8
Both surgeons used equivalent arthroscopic techniques during ACLR. Graft selection was determined by the surgeons based on their assessment of a patient’s characteristics and physical examination findings. Bone-patellar tendon-bone (BPTB) grafts were predominantly used, given the surgeon’s preference for this graft type in patients returning to high-demand sports. Tunnel positions were placed at the anatomic footprints of the original ACL, and femoral drilling was performed through an anteromedial portal. BPTB grafts were secured using met al interference screws (Softsilk; Smith & Nephew), while hamstring (HT) grafts were secured using an EndoButton (CL Ultra; Smith & Nephew) for femoral fixation and a nonbioabsorbable screw (Biosure PK; Smith & Nephew) for tibial fixation. Lateral extra-articular tenodesis (LEAT) was performed as an augmentation procedure for patients exhibiting significant laxity on clinical examination (2%), regardless of the graft type. This was performed using a 10-cm strip of the Iliotibial band, which was tunneled under the lateral collateral ligament and secured to the femur with staple fixation. Routine arthroscopy was performed in all cases, and any coexisting intra-articular pathology was treated accordingly.
Postoperatively, patients were immediately permitted to weight bear as tolerated without a brace. Crutches were used for approximately the first 2 weeks. Because of the geographical distribution of the participants, the majority underwent rehabilitation with local physical therapists. Throughout the rehabilitation period, patients attended our institution every 3 months to undergo a series of physical tests to guide their rehabilitation. These tests included isometric strength and dynamic strength tests before progression to more complex change of direction and sport-specific tasks. The exact testing protocols have been previously described. 17 During these follow-up assessments, a minimum criteria was set for participants to focus on before returning to sports. These included the absence of joint effusion, restoration of quadriceps strength with effective control during single-leg squat, and normal patterns in running and limb symmetry index of at least 90%. These criteria were not evaluated as part of a formal RTP testing protocol. This study defined RTP as the unrestricted resumption of a patient’s preinjury sport in accordance with the definition from the 2016 consensus statement on RTP. 1
PROMS—ACL-Return to Sport after Injury (ACL-RSI), International Knee Documentation Committee (IKDC) score, and Marx Activity Scale—were completed at a 2-year follow-up. An additional questionnaire was administered to record information regarding the participants’ ability and timing of RTP, level of participation, and any subsequent injuries to either the ACLR knee or the non-ACLR knee. Those who experienced a subsequent ACL injury to either knee were identified during the follow-up period, or if they returned to the clinic before the scheduled follow-up time with a confirmed diagnosis of ipsilateral or contralateral ACL injury on magnetic resonance imaging.
Statistical Analysis
Continuous variables were displayed as means and standard deviations or medians and interquartile ranges, whereas categorical variables were reported as numbers and percentages. We compared the proportions of categorical variables using the χ2 test and compared the means of continuous variables using the analysis of variance test. Logistical regression was used to differentiate the effect of age, graft type, and other independent variables on the rates of graft reinjury and contralateral ACL injury. The predicted probability of ACL reinjury was graphed for each participant. This was done using the enter method and odds ratios (ORs) with 95% confidence intervals to quantify the strength of association between the significant predictors and outcomes. The overall model significance was calculated, as well as the Cox & Snell R2 statistic to estimate the proportion of variance explained by the model. The threshold for statistical significance was set at P < .05. Data analysis and graphical presentation were performed using SPSS Version 29 (IBM).
Results
Overall, 2092 Gaelic games players underwent ACLR between January 2014 and December 2018. Of these, 201 patients were excluded for having revision ACL surgery, multiligament knee surgery, or for being outside of the age range. This resulted in a final cohort of 1891 Gaelic games players who met the inclusion criteria. At 2 years, follow-up data were available for 93.4% (1767/1891) of patients (Figure 1). Information regarding RTP rate and level of performance was available for 92.7% (1752/1891) of athletes, and PROMS were analyzed for 78.1% (1477/1891).
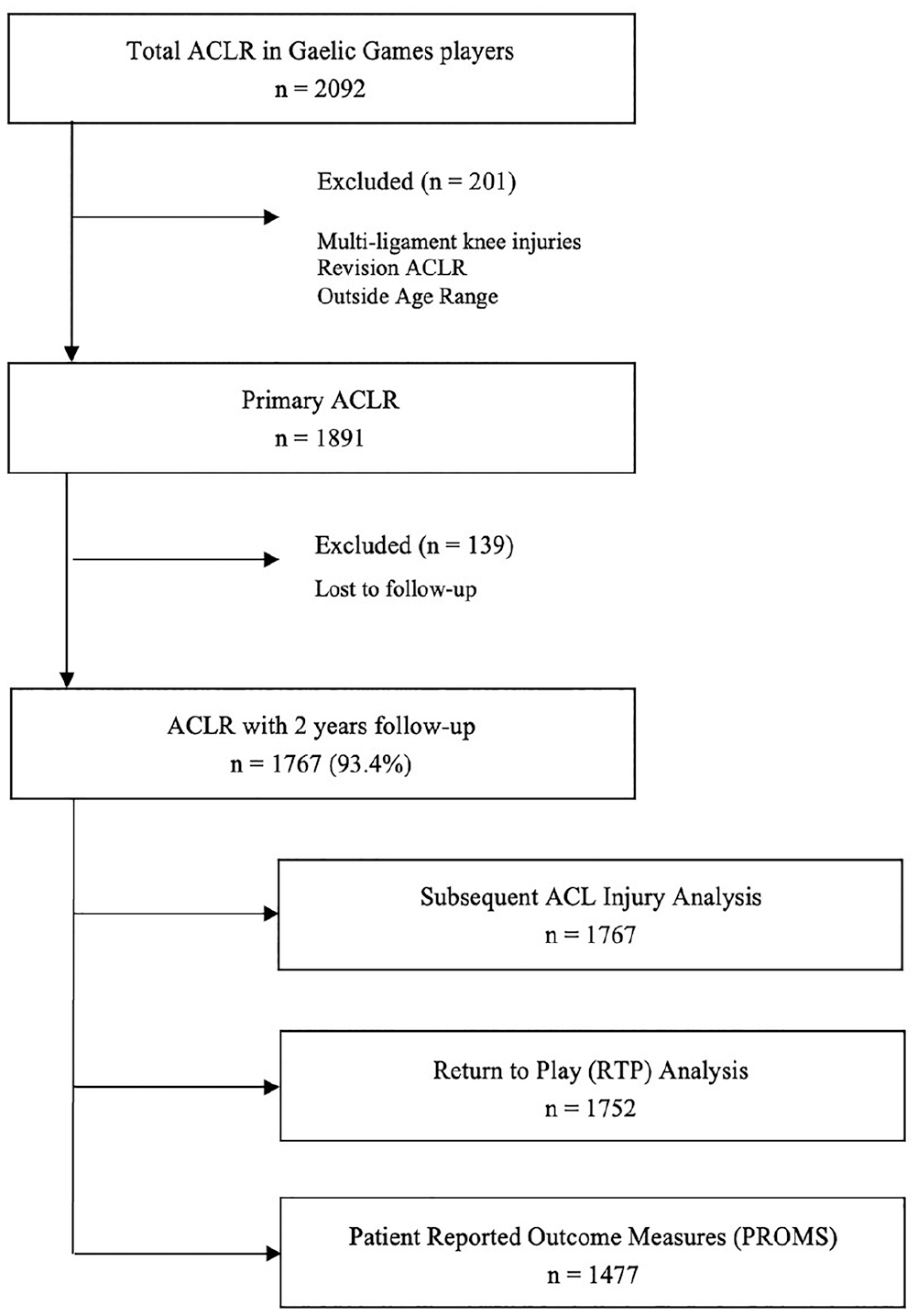
Flowchart of participant inclusion in the analysis. ACLR, anterior cruciate ligament reconstruction; PROMs, patient-reported outcomes Measures; RTP, return to play.
The mean age of patients was 23 ± 6 years, and the majority were men (73.3%; n = 1386) (Table 1). Most players were right-leg dominant (83.9%). The mechanism of initial injury was primarily noncontact (62.7%), with 50% of all injuries observed during pivoting/sidestepping. ACL injuries typically occurred during competition/match play (74.4%) as opposed to during training. There was a variety of footwear worn at the time of injury, including molded boots (51.8%), studs (31%), and blades (16.4%).
Baseline Patient Characteristics and Preoperative Data a
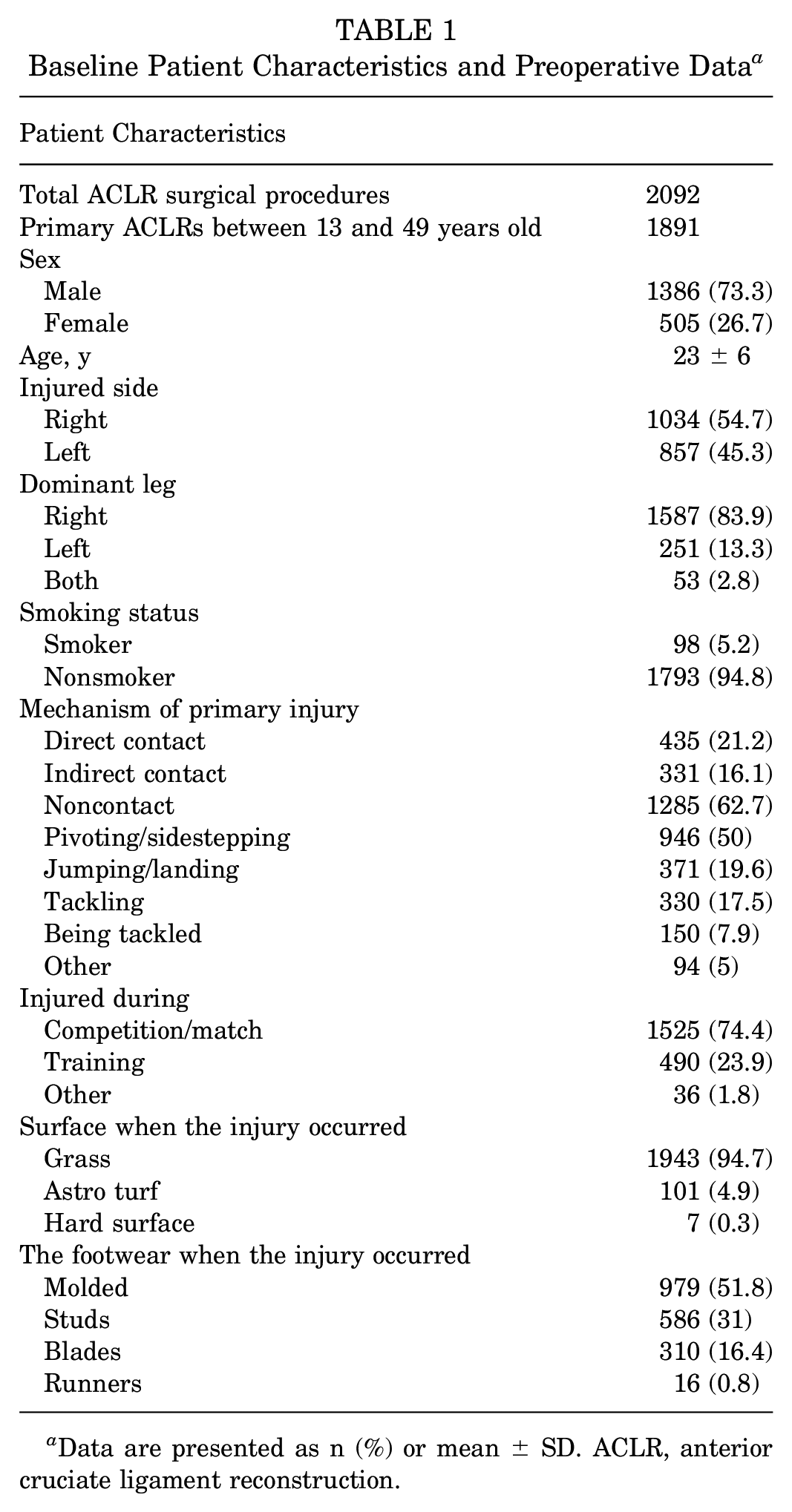
Data are presented as n (%) or mean ± SD. ACLR, anterior cruciate ligament reconstruction.
Gaelic football was the primary sport for 71.5% (n = 1353) of participants, while hurling/camogie accounted for 28.5% (n = 538) (Table 2). There was a significant difference in sex distribution between the sports, with men comprising 75.9% of Gaelic footballers and 66.7% of hurling/camogie players (P < .001). The proportion of athletes playing at the intercounty (elite) level was similar for both sports (23.4% and 22.9%) (Table 2).
Details of Participants’ Sporting Level a

Data are presented as n (%) or mean ± SD. Bold P values indicate significance. ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury; Preop, preoperative; RTP, return to play; U, under; U21, ≤21 years old.
The arthroscopic findings, including the rate of associated meniscal and cartilage injury, noted at the time of surgery, are detailed in Table 3. The most common graft type used was BPTB grafts (87.7%, n = 1658), followed by HT grafts, which were used in 12% (n = 226) of participants. Male athletes constituted 73.3% of the BPTB group and 71.7% of the HT group. HT grafts were generally used for younger patients compared with the BPTB group (mean age, 21.4 ± 6.9 years vs 23.2 ± 5.9 years; P < .001).
Intraoperative Characteristics at the Time of ACLR a

ACLR, anterior cruciate ligament reconstruction; BPTB, bone-patellar tendon-bone.
Return to Play
The RTP rate at 2 years was 87.8% (1096 athletes) for Gaelic footballers and 89.5% (451 athletes) for hurling/camogie players (Table 4). Furthermore, 72.7% (797/1096) of Gaelic footballers and 76.3% (344/451) of hurling/camogie players indicated they were performing at an equivalent or higher level than their preoperative level. The RTP rate was higher in male Gaelic footballers compared with females (89.1% [847/951] vs 83.8% [249/297]; P < .016) and was higher in hurlers (male) compared with camogie (female) players (89.7% vs 84.4%; P < .040). Among senior, intercounty (elite) players, the RTP rate was 97% (97/100) for male players and 94.5% (69/73) for female players at 2 years, (P < .427).
Level of RTP for Gaelic Games Players at 2 Years After ACLR a

Data are presented as n (%) or mean ± SD. ACLR, anterior cruciate ligament reconstruction; RTP, return to play.
The mean time to RTP from surgery for Gaelic footballers (10.9 ± 4.1 months) was equivalent to that of hurling/camogie players (10.6 ± 3.8 months). Overall, by 9 months, 58% reported a return to their preinjury sport level, and by 12 months, this had increased to 80.1% (Figure 2). There was no statistically significant difference in the mean time to RTP between male and female Gaelic games players (10.7 ± 4 months vs 11 ± 4.1 months; P = .278).

Timing of RTP after ACLR in Gaelic football and hurling/camogie players. ACLR, anterior cruciate ligament reconstruction; RTP, return to play.
ACL Graft Reinjury
The rate of graft reinjury was significantly lower in the group who underwent BPTB autograft reconstruction versus HT autograft reconstruction, 3.3% (51/1547) versus 15.3% (33/216), P < .001. The incidence of graft reinjury was lower in Gaelic footballers (4.5%) versus hurling/camogie players (5.7%; P <.001) (Table 5). There was no statistically significant difference between male and female Gaelic footballers (4.7% [45/957] vs 3.7% [11/300]; P=.448) or between hurlers (male) and camogie (female) players (6.7% [23/342] vs 3.6% [6/168]; P = .148). Patients who returned to play before 6 months postoperatively, had a higher incidence of ACL graft reinjury (7.6%) compared with those who returned between 6 and 9 months (5.3%), 9 and 12 months (5.4%), or after 12 months (5%), although the difference between groups was not statistically significant (P = .87).
Rate of Second ACL Injury and PROMs for Gaelic Games Players at 2 Years After ACLR a
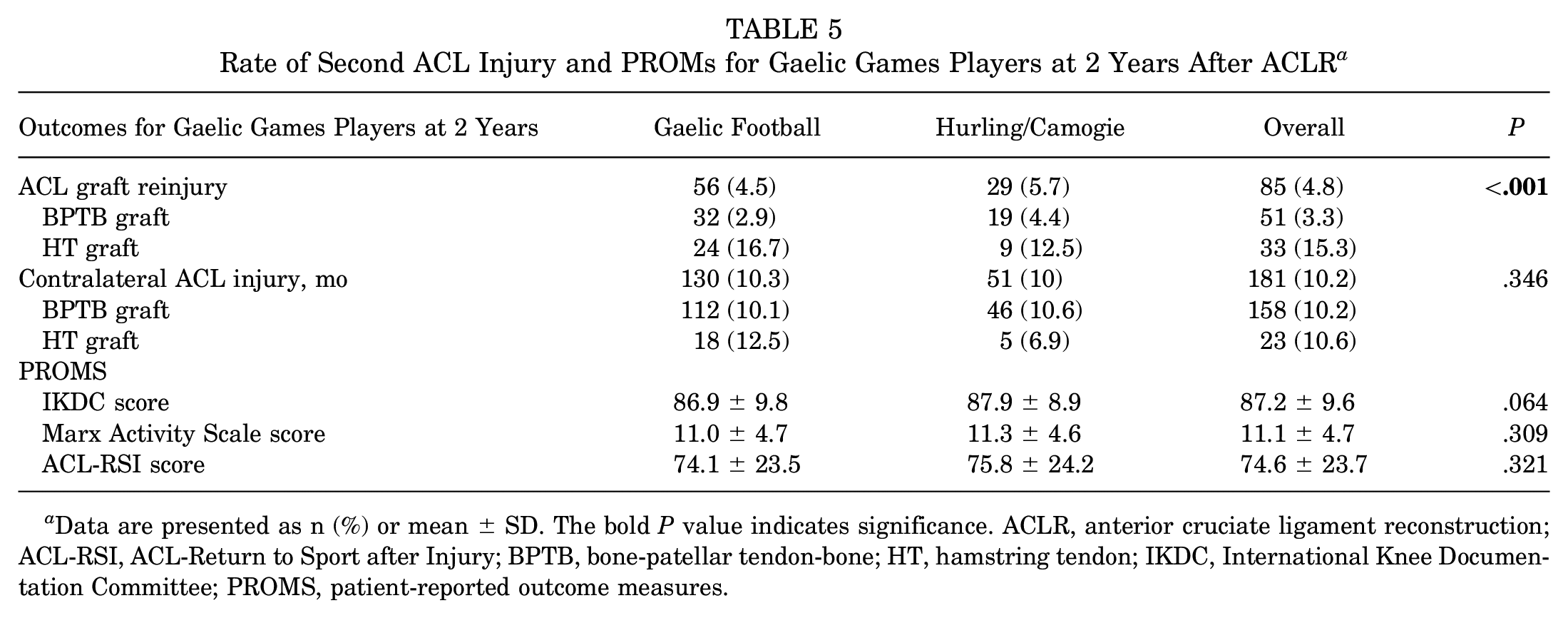
Data are presented as n (%) or mean ± SD. The bold P value indicates significance. ACLR, anterior cruciate ligament reconstruction; ACL-RSI, ACL-Return to Sport after Injury; BPTB, bone-patellar tendon-bone; HT, hamstring tendon; IKDC, International Knee Documentation Committee; PROMS, patient-reported outcome measures.
The most statistically significant predictor of ACL reinjury was HT autograft use (OR, 4.6 [95% CI, (2.8-7.5]; P < .001). The risk of reinjury was also higher for each year of decreasing age (OR, 0.92 [95% CI, 0.87-0.98]; P < .005). Patients were controlled for sport played, level of sport participation, leg dominance, side-injured, and presence of meniscal or chondral injury. The overall model was statistically significant—χ2 (16) = 63.785, P <.001; R2 = .045 (Figure 3).

Scatterplot displaying the predicted probability (%) of ACL graft reinjury for BPTB and HT grafts by age for Gaelic Games players. ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; HT, hamstring tendon.
Among adult intercounty players, the overall rate of graft reinjury was 3.2% (7/217). The lowest rate of graft reinjury was seen among intermediate intercounty level players at 0% (0/30) and senior intercounty level players at 3.5% (6/173). The highest rate was in the underage (U16) group at 13.1% (8/61) (Figure 4A). At the club level, graft reinjury rates were comparable for all groups, except for higher rates seen in the underage group (10.9%; 10/92) (Figure 5A).

(A) ACL graft reinjury rate for intercounty Gaelic games players at a 2-year follow-up.(B) Contralateral ACL injury for intercounty Gaelic games players at a 2-year follow-up.Note: The senior, intermediate, and junior categories are all played by adults but differ in terms of competition level—minor: <18 years; underage: <16 years. ACL, anterior cruciate ligament.

ACL graft reinjury rate for intercounty Gaelic games players involved at the club level at a 2-year follow-up.(B) Contralateral ACL injury rate for intercounty Gaelic games players involved at the club level at a 2-year follow-up.Note: The senior, intermediate, and junior categories are all played by adults but differ in terms of competition level—minor: <18 years; underage: <16 years. ACL, anterior cruciate ligament.
Contralateral ACL Injury
There was no difference in the rate of contralateral ACL injury between sports (Gaelic football, 10.3% [130/1257] vs hurling, 10% [51/510]; P = .830) (Table 5). There was no statistically significant difference between male and female Gaelic footballers (10.1% [97/957] vs 11% [33/300]; P = .668) or between hurlers and camogie players (8.5% [29/342] vs 13.1% [22/168]; P = .102). Graft type and contralateral ACL injury were not associated (BPTB, 10.2% [158/1547] vs HT, 10.6% [23/216]; P = .844). The only statistically significant predictor of contralateral ACL injury was younger age (OR, 0.91 [95% CI, 0.87-0.95]; P < .001). The overall model was statistically significant—χ2 (16) = 90.188; P < .001; R2 = .050—(Figure 6).
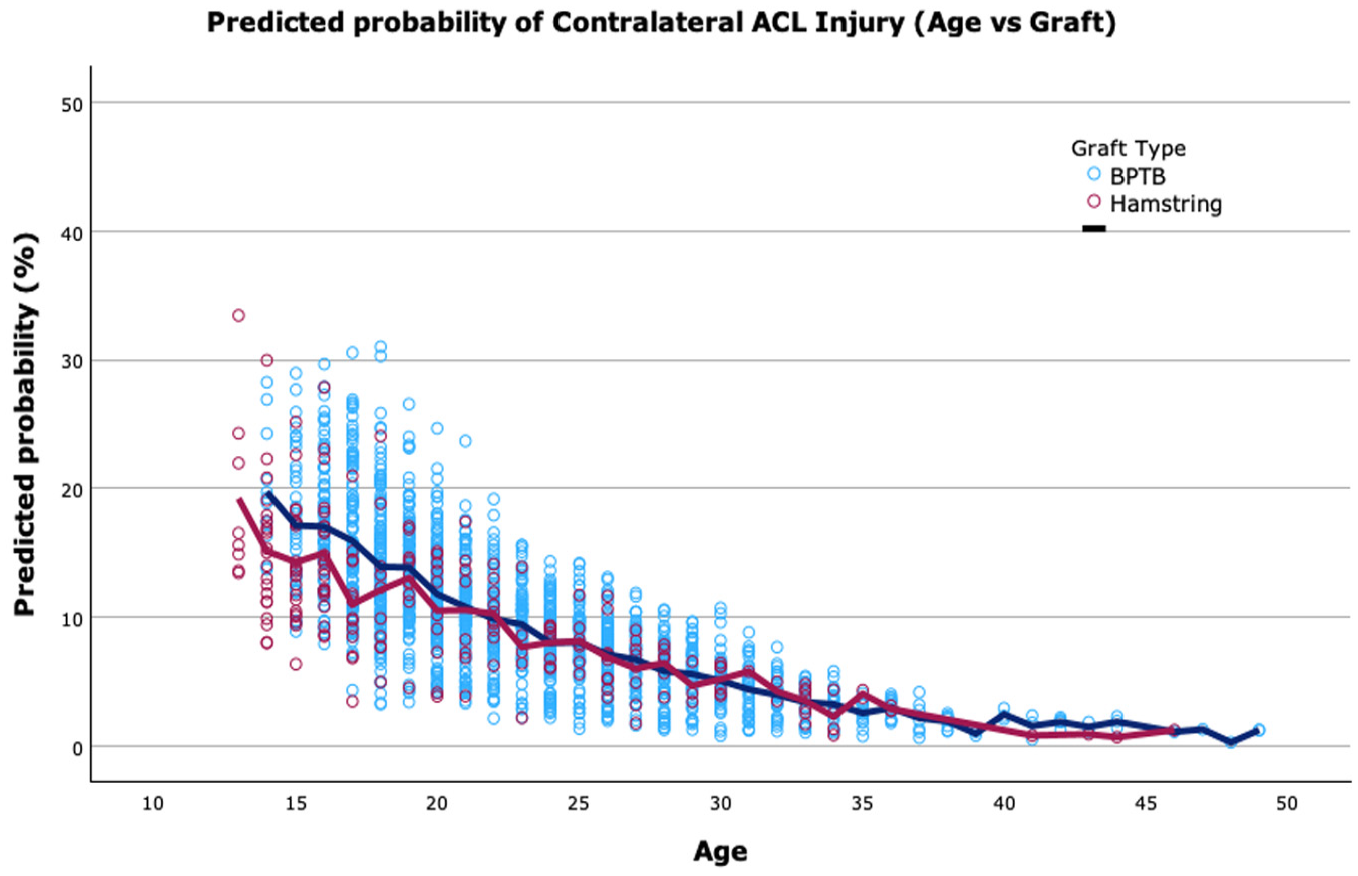
Scatterplot displaying the predicted probability (%) of contralateral ACL injury for BPTB and HT grafts by age for Gaelic games players. ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; HT, hamstring tendon.
The contralateral ACL injury rate was generally higher among intercounty level players compared with club players (Figures 4B and 5B). The rate of contralateral injury was greater than 20% for intercounty players at the intermediate (20%; 6/30), junior (21.4%; 3/14), and underage levels (21.3%, 13/61). However, senior intercounty players had the lowest rate of contralateral injury (8.1%; 14/173) (Figures 4B and 5B).
PROMS/Knee Function
We included 1477 (78.1%) patients in our analysis of PROMS at a 2-year follow-up. The mean IKDC score for Gaelic footballers at 2 years was 86.9 ± 9.8 compared with 87.9 ± 8.9 for hurling/camogie players (P = .64) (Table 5). There was no statistically significant difference in ACL-RSI score between Gaelic footballers and hurling/camogie players at 2 years (74.1 ± 23.5 points vs 75.8 ± 24.2 points,respectively). The postoperative Marx activity rating score was also comparable in both groups of athletes (see Table 5).
Discussion
This study demonstrates high rates of return to level 1 sport among Gaelic football players (87.8%) and hurling/camogie players (89.5%). Furthermore, a significant proportion of athletes participating in these sports (72.7% and 76.3%, respectively) attained or exceeded their preinjury performance level. It is also important to note the significant difference in graft reinjury rate between BPTB autografts (3.3%) and HT autografts (15.3%) in this large cohort of level 1 athletes.
The RTP rates in our study are particularly noteworthy given that athletes involved in level 1 sports are generally less likely to RTP.3,19,20 Moreover, the rates of RTP among Gaelic games players are substantially higher than those seen in similar football codes. For example, Webster et al 38 performed a study of non-elite AFL players and found that, although 96% of players anticipated returning to their preinjury level, the actual RTP rate was 78%, with only 64% of players regaining their preinjury level of performance at a mean follow-up of 3.1 years. Similarly, a study of elite AFL players demonstrated that only 74% returned to an elite level after ACLR, with just 48% returning within 12 months of surgery. 20 It is also noteworthy that despite the amateur status of the sports, both elite and non-elite Gaelic games players demonstrated RTP rates comparable with professional athletes in several sports. 18 It is likely that the high RTP rates among Gaelic games players can be attributed to the cultural importance of the sports and their central role in the social fabric of Irish communities. In addition, GAA clubs cultivate a strong sense of team identity, which likely helps to sustain their players’ motivation throughout the rehabilitation process.
Although RTP rates were high among female Gaelic games players compared with other sports, 10 these rates were lower than male athletes in Gaelic football (83.8% vs 89.1%) and hurling (84.4% vs 89.7%). However, at the elite level, female athletes had an equivalent RTP rate (94.5%) compared with their male counterparts (97%). This aligns with previous research encompassing various sports, which has identified a 10% lower RTP rate for female players participating in nonprofessional sports but similar RTP rates for female and male players in elite sports.2,34 Previous authors have hypothesized that the decreased RTP rates among female players in nonprofessional sports may be due to different attitudes toward risk, different social roles, or different motivations for sports participation compared with male players.2,32 However, this has been highlighted as an area that requires future research as female participation in sport grows. 10
Importantly, our findings show that most Gaelic games players returned to their preoperative performance levels after ACLR. This contrasts the results of several studies, which indicate that performance in level 1 sports generally declines or that athletes often switch to non-pivoting sports.3,29 Therefore, assessing sport-specific performance after ACLR is crucial, as athletes are affected differently due to the varying physical demands of each sport. 21 In addition, there is no standardized measure of performance that allows comparison between sports. 18 Lindanger et al 19 studied a cohort of 234 athletes who played handball, basketball, and soccer, finding that although 83% of patients returned to Level 1 sports after ACLR, only 53% managed to return to their preinjury performance levels. On the other hand, an analysis of ACLR using BPTB autografts in rugby players demonstrated an RTP rate of 84.9% at 2 years, with 75.4% returning to their preinjury performance level or higher. 14 Return to performance is also dependent on the level of preinjury sports participation and is generally higher in professional sports. 18 For example, Jones et al 16 studied a cohort of 420 ACLRs in elite athletes, predominantly soccer and rugby players, and found an overall RTP rate of 95%, with 90.1% performing at the same or an even higher level.
Our results show that Gaelic games players RTP earlier than athletes in similar level 1 sports. 3 In our cohort, 58% of players had returned to play at 9 months, and 80.1% had returned by 12 months. In comparison, studies have found that 35% of non-elite AFL players and 48% of elite AFL players have returned within 12 months.20,38 Another study of high-demand, level 1 athletes found that 48% of athletes <25 years old had resumed sports within 12 months, which was twice the odds compared with athletes >25 years old. 35 Interestingly, when Liptak and Angel 20 analyzed elite-level Australian rules players, they found an increased rate of ACL reinjury among the players who returned to play within 12 months of surgery. They advised athletes to be cautious about returning to elite-level sports too soon. Similarly, we would advise players to exercise caution with an early RTP, as insufficient biological maturation of the graft increases the risk of graft reinjury, regardless of rehabilitation progress.5,30 However, what defines “too early” must be considered, and it may vary depending on the graft type and fixation method used. For example, our study demonstrates a low rate of reinjury for BPTB grafts with interference screws, despite high rates of RTP before 12 months. This suggests that RTP within this time frame is appropriate, once a patient is fully rehabilitated.
One of the most important findings of this study was the significantly lower rate of reinjury for BPTB autografts (3.3%) compared with HT autografts (15.3%) in a cohort of high-risk athletes. Gaelic games players are vulnerable to ACL injury, given that they are returning to a level 1 sport, which involves exposure to explosive, high-risk movements such as pivoting and jumping. It is estimated that participation in these types of sport increases the odds of graft reinjury and contralateral reinjury by 3.9 times and 5 times, respectively. 37 The rate of BPTB graft reinjury in our study was significantly lower than the 15% reinjury rate reported among a cohort of 354 non-elite AFL players at 3.1 years follow-up. 38 The high reinjury rate in this cohort of AFL players may be due to patients undergoing HT autograft ACLR before returning to a similar level of sport exposure. This indicates that returning to a level 1 sport is a relative indication for using a BPTB autograft.
Only a small proportion of patients in this study underwent augmentation with lateral extra-articular tenodesis, a procedure shown in the Stability 1 trial to reduce the risk of HT graft reinjury in high-risk, young patients of reinjury. 11 Nonetheless, the rates of isolated HT graft reinjury in the Stability 1 randomized trial at 2 years (11%) were similar to our cohort, who are also recognized as “high-risk.” The addition of LEAT in Stability 1 reduced HT graft reinjury rates down to 4% at 2 years. 11 The ongoing Stability 2 trial will detail the role of LEAT high-risk patients who undergo ACLR using BPTB. 6
When both sports were compared, the rate of ACL graft reinjury was higher in hurling/camogie (5.7%) players than in Gaelic footballers (4.5%). This likely reflects the higher speed of play and the increased occurrence of actions that occur in hurling/camogie, such as catching the ball above the eyeline and twisting upon landing. Importantly, we found no statistically significant sex difference in reinjury rates for either sport in our cohort.
We did find that “underaged” athletes (U16) were particularly vulnerable to reinjury of either knee, in keeping with the findings of Webster et al, 37 which highlighted the higher risk of reinjury in younger athletes. Our results are also consistent with other research showing that the rate of a contralateral knee injury after ACLR is as high as 2-fold the risk of graft reinjury. 12 Importantly, the overall rate of both graft reinjury and contralateral ACL reinjury was higher among intercounty Gaelic games players compared with club-level players. This perhaps reflects the increased exposure time to higher-intensity sports for these athletes. Of note, one exception to this was players at the highest level of the sport—senior intercounty players—who had low rates of both graft reinjury and contralateral injury. This may reflect several factors, including a higher preoperative fitness level and access to rehabilitation facilities.
Limitations
There are several limitations in this study. Most notably, there were a variety of approaches to postoperative rehabilitation used, given the size and geographical distribution of this cohort; therefore, conclusions cannot be made regarding the influence of rehabilitation on these outcomes. This study only included patients who underwent ACLR at our hospital, and thus, we recognize the need for improved injury surveillance in the Gaelic games, given the high incidence of ACL injuries. Finally, patients were asked to record when they achieved an unrestricted return to their previous sport, although the exact definition of unrestricted may be influenced by individual interpretation.
Conclusion
The RTP rate for Gaelic games players was high, with most athletes returning to an equivalent or higher level of performance. Female athletes demonstrated a slightly lower RTP rate at club level but comparable rates to male athletes at the intercounty (elite) level. The rate of BPTB reinjury was low considering the risk associated with a high RTP rate in a level 1 sport. This indicates that returning to a level 1 sport is a relative indication for using a BPTB autograft. The ACL graft reinjury rate in this study was low compared with other studies on similar, level 1 sports such as AFL, soccer, and rugby. Gaelic games players who participate at the intercounty level, other than at senior level, have a higher rate of ACL graft and contralateral ACL injury compared with club-level players. Overall, patients involved in both sports reported good knee function and outcomes after ACLR.
Footnotes
Final revision submitted February 15, 2025; accepted March 17, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.M. receives research funding under the Strategic Academic Recruitment (StAR) Programme of the Royal College of Surgeons Ireland. The content of this manuscript is solely the responsibility of the authors and was not influenced by the funding entity. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Sports Surgery Clinic (25-AFM-010).