
Abstract
Background:
Injuries of the medial ulnar collateral ligament (MUCL) among baseball pitchers are increasing. Surgical treatment is evolving to optimize outcomes.
Purpose/Hypothesis:
This study’s purpose was to highlight trends in MUCL repair and reconstruction in professional pitchers, describe outcomes such as return to any level of play (RTP), and identify factors impacting these outcomes. It was hypothesized that primary and revision MUCL surgery is increasing, with revision surgery requiring greater RTP time.
Study Design:
Case series; Level of evidence, 4.
Methods:
The Major League Baseball (MLB) Health and Injury Tracking System database was used to procure data during the study period (2010-2023). All professional pitchers who underwent MUCL surgery during this period were included. RTP was defined as a pitcher returning to at least 1 professional game after index surgery. Return to the same level of play (RTSL) was defined as return to at least 1 game in the same league of play as before surgery. Because of the coronavirus pandemic, the year 2020 was considered an outlier and omitted from time-trend analysis.
Results:
A total of 2281 pitchers who underwent MUCL surgery during the study period were included for analysis. The number of MUCL surgeries for pitchers increased yearly (R2 = 0.821; P < .001), as did the number of reconstructions with internal brace augmentation (R2 = 0.896; P < .001). The RTP rate for MLB pitchers was significantly higher than the RTSL rate (93% vs 71%; P < .001). This difference was not observed in Minor League Baseball (MiLB) pitchers (RTP 76% vs RTSL 74%; P = .142). RTP rates after revision surgery were lower than those after primary surgery (71% vs 80%; P = .020). The mean time to RTP was shorter (470 ± 135 days) than the mean time to RTSL (499 ± 153 days; P < .001).
Conclusion:
The incidence of MUCL surgery and revision surgery is increasing among professional pitchers. Overall, 79% of pitchers returned to any level of play at a mean of 470 days, while 74% returned to the same level of play at a mean of 499 days, but this varied based on level of play. This study will guide athlete expectations and surgeon decision-making.
The medial ulnar collateral ligament (MUCL) is the primary stabilizer of valgus forces across the elbow. As a result, it is pivotal to maintain elbow stability during the throwing motion. Consequently, injury to the MUCL has a large effect on the throwing athlete, particularly in baseball. The repetitive stress on the medial elbow experienced by baseball pitchers often leads to adaptive changes, attenuation, and, commonly, MUCL insufficiency.18,20 This mechanism of chronic failure, often visually characterized on imaging or surgical inspection, is encountered more often than acute traumatic ruptures. 28 Collectively, the incidence of MUCL injury in baseball players is on the rise, and much of this is attributed to overuse, particularly in youth athletes. 27 As many as 20% of all professional pitchers have undergone MUCL reconstruction based on data collected in 2018; this proportion has increased from 16% in 2012. 24 This trend is even more apparent in younger pitchers. In particular, the 15- to 19-year age group is seeing a rise in reconstruction surgery.10,14,31 Furthermore, an analysis of MUCL reconstruction in professional baseball players between the years 1974 and 2016 demonstrated that the annual rates of primary and revision reconstructions have been increasing as well. 5 It is prudent to continue investigating these trends, as doing so will help surgeons understand and better prepare for a further increase in downstream revision surgery.
Classically, reconstruction of the MUCL has provided the most reliable path to satisfactory and reproducible outcomes. 32 Attempts to improve outcomes, increase rates of return to any level of play (RTP), and decrease the time to RTP have led to continuous innovations in surgical constructs. One such advance is the incorporation of an internal brace (IB) with repair and/or reconstruction, which provides increased stiffness and enhanced time-zero failure strength.3,33 Biomechanical data have proven this benefit in investigations comparing various docking reconstruction techniques with and without an IB.3,29,33 Also noteworthy is that repair constructs with IB augmentation demonstrate similar biomechanical properties to reconstruction using the docking technique. 4 It has also been demonstrated that repair with IB augmentation provides consistent biomechanical results among several surgeons, without overconstraining the joint. 21 Older studies have demonstrated that reconstruction is better than repair.2,6 While older studies favored reconstruction, newer studies utilizing IB augmentation favor repair, with >90% RTP rates and quicker return. 7
A comprehensive understanding of epidemiological data in elite-level pitchers coupled with an update on the trends in surgical technique serves to guide team physicians and sports surgeons in the decision-making process. This study’s purpose was to highlight trends in MUCL repair and reconstruction in professional pitchers, describe outcomes such as RTP, and identify factors impacting these outcomes. The primary hypothesis was that the incidence of surgical intervention continues to increase. The secondary hypothesis was that reconstruction likely remains the most common surgical intervention with high rates of RTP, and revision surgery demonstrating lower rates of RTP compared with primary surgery.
Methods
After approval from our institutional review board (No. 17-006455), a search was performed to identify all baseball pitchers who have undergone MUCL reconstruction or repair while they were active on a Major League Baseball (MLB) or Minor League Baseball (MiLB) team roster. Specifically, the MLB Health and Injury Tracking System (HITS), a centralized, league-wide injury database, was used to procure data. Where necessary, these results were cross-referenced using online publicly available data (eg, team injury reports and press releases). Each surgical intervention was only included once, with duplicates removed. All players were de-identified and assigned a study number in random order. All male professional pitchers, regardless of age, who underwent MUCL surgery within the study period were included. Pitchers were excluded from the analysis if there were incomplete data with respect to demographics and surgical construct. The initial MUCL surgery was considered the index procedure, and all subsequent surgeries were considered revisions. Surgeries before professional baseball were also documented, and thus subsequent surgeries were considered revisions.
Demographic data were compiled for each player and included age at beginning of career, age at time of surgery, age at retirement, career length, and level of play at time of injury and return from injury. Surgical variables included date of procedure, RTP status, time required to RTP, career length before and after surgery, revision surgeries, and time between surgeries. Successful RTP was designated if a pitcher had returned in at least 1 professional game after index surgery, whereas return to the same level of play (RTSL) was classified if a pitcher had returned at or above the level of play at the time of surgery (eg, A, AA, AAA, or MLB). Data were collected and analyzed from 2010 to 2023. The RTP analysis only included data from 2010 to 2021 to allow 2 years of time for follow-up. To account for outliers in the time from professional career to surgery, and RTP analysis, data points were removed if they were >1.5 times the interquartile range.
Targeted comparisons were made among MLB pitchers, MiLB pitchers, and MUCL surgery types (repair, reconstruction, reconstruction with IB augmentation, and revisions), looking for differences in demographic factors, playing career, and RTP. Of note, all repairs were performed with IB augmentation. Epidemiological trends with respect to time were analyzed by level of play at time of surgery, surgery type, and revision status. The year 2020 was excluded from time-trend analysis due to the effect of the coronavirus pandemic on sporting events, creating an outlier.
Statistical Analysis
Descriptive statistics such as number, median, mean, standard deviation of the mean, range, and frequency are reported for epidemiology. The significance of the change in trends with respect to time was assessed by using linear regression on the slope of a best-fit line. Pairwise comparisons for continuous variables that were normally distributed were performed using a Student independent-samples t test, and P values were calculated to assess for statistically significant differences. A Fisher exact test was performed to determine differences in frequencies in categorical variables, when needed. P values <.05 were considered statistically significant.
Results
All pitchers who had an MUCL injury with subsequent surgery included in the study totaled 2287. Surgical and return-to-play data on 6 pitchers were incomplete and removed from subsequent analysis. The mean age at the time of surgery was 23.9 ± 3.8 years for all pitchers. On average, MUCL surgery occurred 3.2 ± 2.3 years into their professional career. Further breakdown on age and timing of surgery by level of play and surgical construct is detailed in Table 1.
Summary of Age and Timing of Surgery for MLB and MiLB Pitchers Undergoing Medial Ulnar Collateral Ligament Surgery a
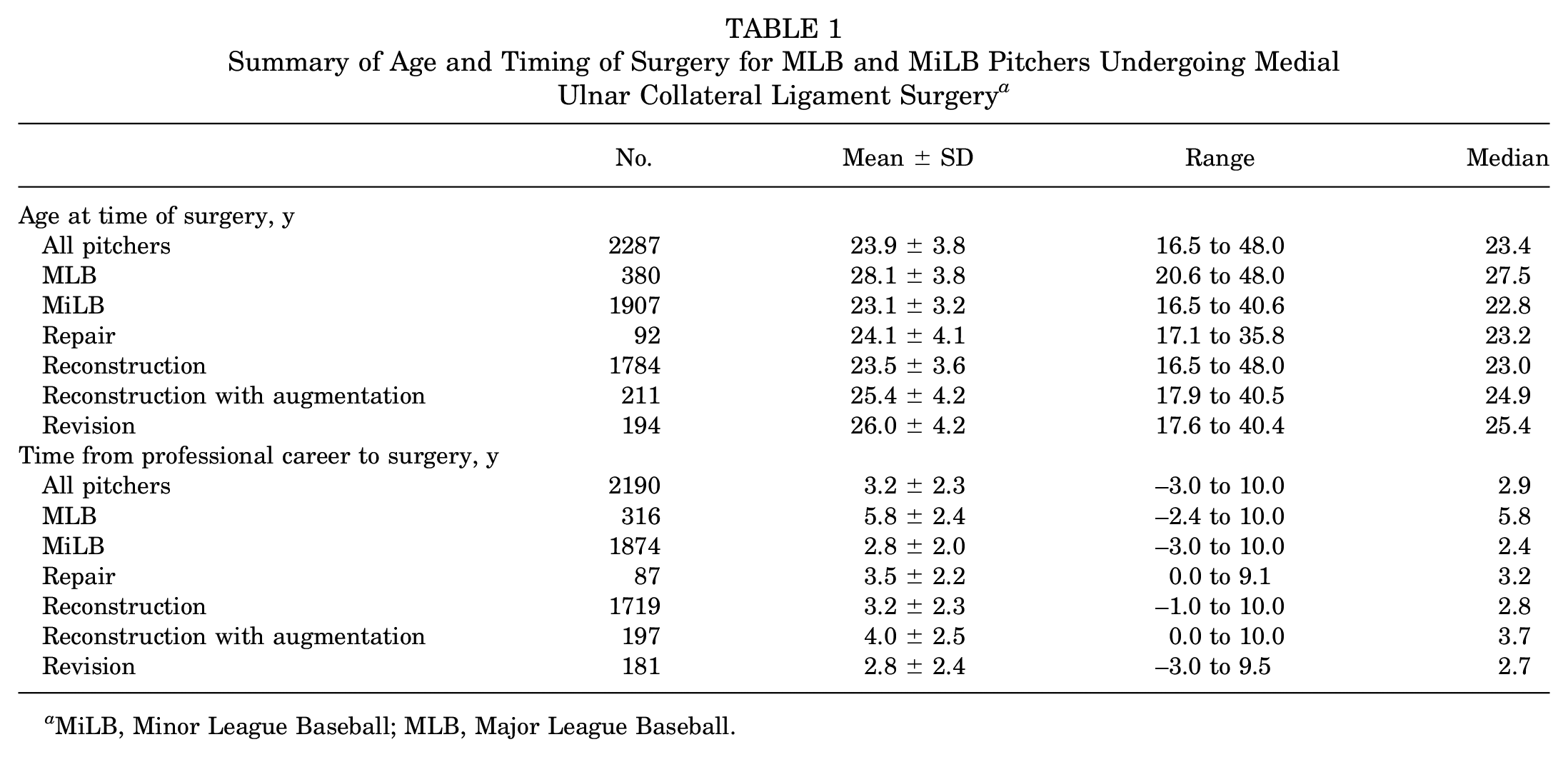
MiLB, Minor League Baseball; MLB, Major League Baseball.
The annual number of MUCL surgeries in all pitchers from 2010 to 2023 has increased year over year (R2 = 0.821; P < .001) (Figure 1). The first documentation of IB augmentation with MUCL reconstruction was in 2016, with a consistent and significant increase year over year (R2 = 0.896; P < .001). Although not as dramatic, there has been an increase in the utilization of repairs as well (R2 = 0.434; P = .108). The percentage of MUCL surgeries performed on MiLB pitchers has also increased (R2 = 0.539; P = .004) (Figure 2).

The annual number of medial ulnar collateral ligament surgeries performed on Major and Minor League Baseball pitchers from 2010 to 2023 (R2 = 0.821; P < .001).
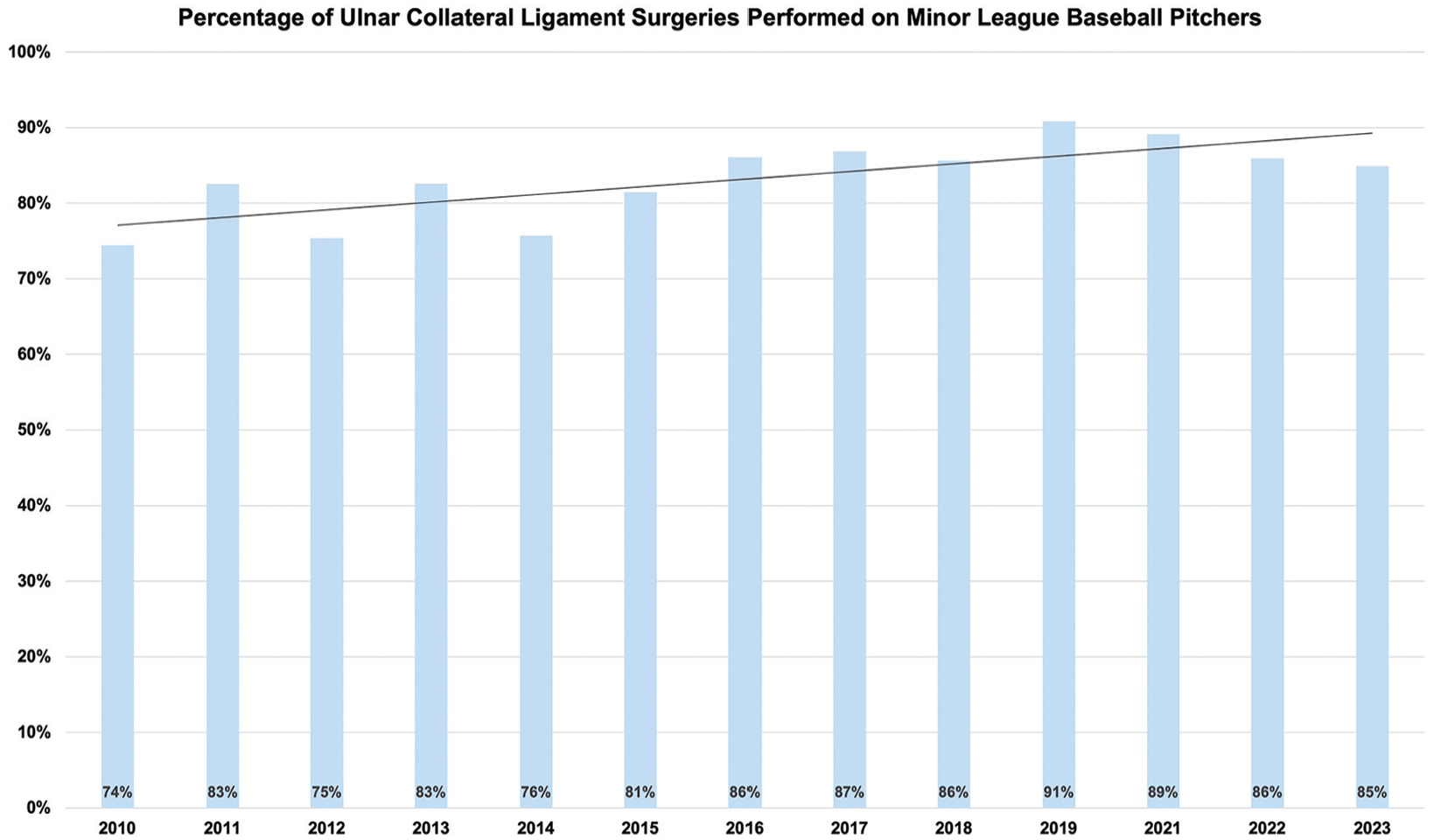
The annual percentage of medial ulnar collateral ligament surgeries performed on Minor League Baseball pitchers relative to all baseball pitchers from 2010 to 2023 (R2 = 0.539; P = .004).
Rates of RTP were compared across groups. For all pitchers included, the RTP rate was 79.1%, while a significantly lower proportion (73.5%) were able to RTSL (P < .001) (Table 2). A similar significant difference was noted in MLB pitchers (RTP 93.2% vs RTSL 71.4%; P < .001). This difference was not noted in MiLB level of play (RTP 76.3% vs RTSL 73.9%; P = .142). For all pitchers at any level, only the ones who had undergone MUCL reconstruction or revision surgery experienced significantly lower RTSL rates compared with RTP (reconstruction: RTP 79.3% vs RTSL 74.4%, P < .001; revision: RTP 71.1% vs RTSL 57.7%, P < .001) (Table 2). Those who underwent revision MUCL surgery experienced the lowest RTSL across all surgical interventions/constructs. MLB pitchers demonstrated RTP at a higher proportion than MiLB pitchers (93.2% vs 76.3%; P < .001). However, there was no difference in RTSL between MLB and MiLB pitchers (71.4% vs 73.9%; P = .410) (Table 2). RTP after revision surgery was significantly lower compared with that after primary surgery (71.1% vs 79.8%; P = .020) (Table 2). A graphical representation of the proportion of pitchers able to return to competition by level of play and surgery type is available in Figure 3.
Return-to-Play Rates After Medial Ulnar Collateral Ligament Surgery in MLB and MiLB Pitchers a

Bold values represent statistical significance (P < .05). MiLB, Minor League Baseball; MLB, Major League Baseball; RTP, return to any level of play; RTSL, return to the same level of play.

Percentage of Major League Baseball (MLB) and Minor League Baseball (MiLB) pitchers able to return to professional play at any level and their prior level of performance. *Statistically significant difference (P < .05).
Time to RTSL is significantly longer for all pitchers compared with time to RTP (499 ± 153 days vs 470 ± 135 days; P < .001). This significant finding was also present in both MLB pitchers (RTSL 551 ± 154 days vs RTP 459 ± 130 days; P < .001) and MiLB pitchers (RTSL 489 ± 151 days vs RTP 473 ± 137 days; P = .009) (Table 3). Among the various surgical approaches, only MUCL reconstruction demonstrated a significantly longer RTP compared with RTSL (469 ± 133 days vs 498 ± 151 days; P < .001). A graphical comparison of RTP and RTSL is depicted in Figure 4.
Time to Return to Play for MLB and MiLB Pitchers a

Bold values represent statistical significance (P < .05). MiLB, Minor League Baseball; MLB, Major League Baseball; RTP, return to any level of play; RTSL, return to the same level of play.

Mean time (days) for Major League Baseball (MLB) and Minor League Baseball (MiLB) pitchers to return to professional play at any level and their prior level of performance. *Statistically significant difference (P < .05).
From 2010 to 2023, revision surgery was also on the rise (Figure 5). In total, 194 professional pitchers required revision surgery. The percentage of MUCL surgeries performed each year that was revision surgery has shown an increasing trend year over year (R2 = 0.322; P = .043) (Figure 5). A significantly higher proportion of MLB pitchers underwent revision surgery compared with MiLB pitchers (16.3% vs 6.9%; P < .001) (Table 4). Time to revision surgery was shorter for MiLB pitchers compared with MLB pitchers (991 ± 882 days vs 2068 ± 1164 days; P < .001) (Table 4).

Percentage of revision medial ulnar collateral ligament surgeries performed each year in Major and Minor League Baseball pitchers, as a proportion of all medial ulnar collateral ligament surgeries (R2 = 0.322; P = .043).
Frequency and Time to Revision After Primary Medial Ulnar Collateral Ligament Surgery for MLB and MiLB Pitchers a

aMiLB, Minor League Baseball; MLB, Major League Baseball. Bold values represent statistical significance (P < .05).
Percentage refers to the proportion of pitchers who underwent revision surgery from the total who underwent primary surgery, respective to level of play.
Comparison of means.
Discussion
The main findings of this study are that the annual number of MUCL surgeries in all pitchers from 2010 to 2023 has increased year over year. There has also been an increasing trend in the use of IB augmentation with reconstruction. Similarly, the proportion of MUCL surgeries performed each year that were revision surgeries has shown an increasing trend year over year.
Previous literature has documented MUCL injury and surgery trends over time, but the most comparable study was documented by Camp and colleagues 5 in 2018 using the same MLB HITS database. They demonstrated, at that time, an increasing annual rate of MUCL reconstruction and revision reconstruction. During their study period from 1974 to 2016, they found that MUCL surgery, including revision, at the Major League and Minor League levels increased for all surgeries (R2 = 0.674; P < .001), for all revisions (R2 = 0.639; P < .001), for MLB pitchers (R2 = 0.821; P < .001), and for MiLB pitchers (R2 = 0.569; P < .001). In fact, much of their findings remain consistent with the current study, with the added benefit that the current study has a greater sample size, includes data from more recent years, and takes a more granular look at various surgical constructs with the addition of repairs and reconstructions with IB augmentation. Furthermore, in their series, the RTP rate for all pitchers was 83.7%, and that for pitchers at the MLB level was 94.6%. Both values were comparable with the current study’s findings of 79.1% and 93.2%. While there are other studies looking at RTP in professional pitchers, studies with smaller series of pitchers (n < 200) tend to have higher RTP rates, ranging from 82% to 97%.9,11,18,26 Studies with larger series of pitchers (n > 200) document slightly lower RTP rates, ranging from 72% to 79%.8,13 The variability in published RTP rates has been summarized in a recent systematic review. 35 The authors of the systematic review speculate that multiple factors contribute to the variability in RTP rates, such as age, role in the organization, and additional concomitant injuries.
Consistent with prior literature, the rate of RTSL was significantly lower at 74%. MLB pitchers had a very high rate of RTP (93%) but had lower rates of RTSL (71%). On the other hand, MiLB pitchers did not demonstrate any difference in the rate of return to play between RTP and RTSL. There are likely many factors (age, player performance, talent bias, psychological impediments, etc) that affect why professional pitchers at the MLB level have such a large gap between returning to the same level and any level of play despite having high-quality medical, surgical, and rehabilitation resources.1,16,18 The initial thought is that pitcher performance declines despite surgery, which has been documented. 9 However, many other studies have not shown a decline in pitching performance after MUCL reconstruction.12,16,18,25 Another factor could be a decrease in pitcher workload for some pitchers, which has been documented after return from MUCL surgery. 35 Yet the most obvious reason is the rehabilitation process for MLB pitchers. It almost always involves an initial assignment to Minor League play first, in preparation for Major League play. MiLB pitchers do not always have a lower level of play to return to first. This inherently affects the difference in the rate of RTP compared with RTSL. Ultimately, MLB play is the highest level of baseball, and returning to this level can be difficult after having significant injury and surgery with long rehabilitation of any kind.
Revision cases demonstrated the lowest percentage of RTP (71%) and RTSL (58%) and were significantly lower compared with cases of primary surgery. Previous literature supports this finding, with RTP ranging from 77% to 85% and RTSL from 55% to 78% after revision MUCL reconstruction. 35 Reconstructions, alongside revisions, also had significantly lower rates of RTSL compared with RTP. Meanwhile, this difference was not significant in the repair, or reconstruction with IB augmentation groups. While this difference is expected in revision surgery, it is harder to explain in the reconstruction group. We surmise that traditional reconstructions have a longer and established rehabilitation timetable that is typically longer in length than that for repairs and augmented reconstructions.15,19 Greater length of missed time can make return more difficult. Additionally, the reconstruction group has the largest sample size; therefore, it is possible that the repair and augmented reconstruction groups were underpowered to detect a significant difference.
The first 6 years of the study period did not include any repairs or augmented reconstructions, which were first performed in 2016 in this cohort. While the number of repairs in recent years has remained relatively stable, the annual incidence of augmented reconstructions with an IB is increasing substantially, with almost 84 of these surgeries performed of a total of 232 UCL surgeries in 2023. The added benefit of IB augmentation is increased time-zero strength. Increased time-zero strength in biomechanical studies illustrates superior stiffness and load to failure in constructs augmented with a suture tape IB in docking techniques, 3-strand docking techniques, and hybrid fixation techniques.3,23,29 This is appealing to surgeons and pitchers as it may accelerate rehabilitation protocols and potentially bring players back to competition sooner. Comparative data investigating RTP between reconstructions with and without IB augmentation are not yet well published and represent an opportunity for further study.
The number of athlete-exposures for athletes was impacted by quarantine measures. This decrease in sports-related injuries during the pandemic has been well documented across a variety of sports and competitive levels.17,34,37 Moreover, the year 2020 produced about one-half as many pitchers who underwent MUCL surgery than in 2019 and about one-third as many pitchers who underwent MUCL surgery than in 2021. Not only did it represent a significant outlier, but it also likely stresses the importance of conditioning for athletes that compete at an elite level, as there was such a sharp increase in MUCL surgeries immediately after, in 2021, followed by a substantial decrease in 2022. This “rebound” phenomenon after a pandemic-related hiatus has been documented in other sports.22,30,36
Limitations
This study is not without limitations. Primarily, the study sample consisted of only professional pitchers with access to high-quality medical care and resources, thus making some of these data not generalizable to amateur or high school–aged pitchers. Furthermore, this study is subject to the limitations of the data input to the database. Therefore, it is difficult to account for variability in physical therapy, surgical technique, team need for player to return, and so forth. Moreover, situations in which players reinjure their elbow during rehabilitation would prolong their return to play. These situations are rare and are not adequately captured by the broad scoping epidemiological review in this study, as we have accounted for outliers by removing them if they fell outside of anything >1.5 or <1.5 times the interquartile range. Although this database study represents one of the largest collections of MUCL surgery outcomes, the overwhelming majority are traditional reconstructions, and as such, it is possible that the repair and augmented reconstruction groups are underpowered to detect significant differences in return-to-play rates and timelines. As previously mentioned regarding the time-trend analysis, the year 2020 was impacted by the coronavirus pandemic, and thus access to surgery and rehabilitation could have been impacted by social distancing and quarantine in addition to lower athlete-exposures and games. Additionally, both MLB and MiLB pitchers were pooled in the time-trend analysis. Although pooling these groups together has limitations in homogeneity of treatments, contracts, and incentives to return to play, it provides a broad epidemiological trend for all pitchers at an elite level. RTP was defined by playing in at least 1 competitive game after surgery, and the clinical/athletic meaningfulness of this could be debated, especially if there was subsequent reinjury or missed time. Lastly, player performance before and after surgery was not analyzed in this study, which represents an area of future study as it could highlight a more meaningful outcome for pitchers after MUCL surgery.
Conclusion
The incidence of MUCL surgery and revision surgery is increasing among professional pitchers. Overall, 79% of pitchers returned to any level of play at a mean of 470 days, while 74% returned to the same level of play at a mean of 499 days, but this varied based on level of play. Surgical techniques are evolving as MUCL repairs and reconstructions with IB augmentation have also increased. This study will guide athlete expectations and surgeon decision-making.
Footnotes
Final revision submitted February 6, 2025; accepted March 17, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.B.G. has received travel and lodging and food and beverage from United Orthopedics LLC. P.N.C. has received consulting fees from DePuy Synthes Products, Exactech, Medical Device Business Services, and Smith & Nephew. C.L.C. has received travel and lodging, food and beverage, and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mayo Clinic Institutional Review Board (No. 17-006455).