
Abstract
Background:
Despite the increasing utilization of hip arthroscopy and identification of predictors of poor outcomes, the effect of short-term improvement on long-term functional outcomes has been understudied.
Purpose:
To determine whether improvements in patient-reported outcomes (PROs) 6 months after hip arthroscopy predict 5-year outcomes.
Study Design:
Case-control study.
Methods:
A retrospective review of prospectively collected data identified patients ≥18 years who underwent primary hip arthroscopy by a single surgeon for the treatment of symptomatic labral tears. Included patients had a Tönnis grade <2 and completed PROs at baseline, 6-month, and minimum 2-year follow-up, and annually thereafter. The minimal clinically important difference (MCID) for the modified Harris Hip Score (mHHS), 8 points, was used to stratify patients into cohorts based on high improvement (HI) versus low improvement (LI) at 6 months. PROs were compared at 1, 2, 3, 4, and 5 years postoperatively by rates of MCID achievement and linear mixed-effects modeling. Subsequent surgery rates were compared by chi-square or Fisher exact tests, as appropriate.
Results:
Overall, 175 patients (age, 37.2 ± 11.4 years; 52.0% female) met inclusion criteria. Of these, 131 HI patients were compared with 44 LI patients. At 5 years, 88.3% of HI patients reached MCID, versus 42.1% of LI patients (P < .001). By multivariable logistic regression, achievement of 6-month MCID (adjusted odds ratio [AOR], 17.43; P < .001) and labral management (augmentation, relative to debridement: AOR, 14.5; P = .01) predicted achievement of 5-year MCID. mHHS scores were greater for HI versus LI patients through 3-year follow-up (P < .05) but were not significantly different at 4 and 5 years. Subsequent surgery rates were 9.9% and 11.4% in HI versus LI patients, respectively (P > .05).
Conclusion:
The study demonstrates that early functional improvements after hip arthroscopy, assessed by 6-month MCID, predicted clinically meaningful outcomes at 5-year follow-up, underscoring the importance of early cautious recovery to prioritize labral healing while also meeting appropriate, stepwise rehabilitation milestones to advance functionally during these 6 months. Despite this, LI patients continued improving for 5 years, demonstrating that late functional improvements are still possible for certain patients in the event of a poor 6-month rehabilitation period.
Keywords
Acetabular labral tears secondary to femoroacetabular impingement (FAI) cause reduced range of motion (ROM), hip and groin pain, stiffness, and reduced function in nondysplastic patients. 50 While initial nonoperative management, including activity modification, physical therapy, nonsteroidal anti-inflammatory drugs or acetaminophen, and intra-articular corticosteroid injections, remains the first-line treatment for these injuries, 51 hip arthroscopy has become the standard of care, particularly among younger patients who fail to achieve adequate symptomatic relief from nonoperative management.26,32,48 As the utilization of hip arthroscopy for acetabular labral tears secondary to FAI continues to rise,9,29 identifying predictors of and strategies for optimizing and addressing poor outcomes becomes increasingly important.
Previous studies have identified older age18,20 and more advanced radiographic (ie, higher Tönnis grade)13,25,55 and/or arthroscopic (ie, higher Outerbridge grade)20,25 osteoarthritis as risk factors for inferior patient-reported outcomes (PROs) and conversion to total hip arthroplasty (THA) after hip arthroscopy. Other predictors of poor outcomes include high body mass index (BMI), female sex, longer duration of symptoms, extent of labral damage, acetabular lesions requiring microfracture, and joint space narrowing.11,18,31,53
However, relatively few studies have examined the effect of improvements in functional outcomes during the initial, rehabilitation-focused months after hip arthroscopy on long-term outcomes. One study of 340 consecutive hip arthroscopies found that not achieving the Patient Acceptable Symptom State (PASS) for the modified Harris Hip Score (mHHS) by 6 months was associated with 2.4-times greater odds of requiring reoperation at 50 months after primary hip arthroscopy. 61 Separately, Lin et al 37 examined the likelihood of achieving the minimally clinically important difference (MCID) for mHHS at 2 years after hip arthroscopy, stratified by whether or not patients achieved MCID for mHHS at 6 months; they found that only 52% of those not achieving 6-month MCID had reached MCID at 2 years, compared with 88% that did achieve 6-month MCID. 37 However, these authors only assessed outcomes up to 2 years and, importantly, did not control for key covariates (eg, age, sex, BMI, and baseline score) in their analyses. 10 Finally, in a study of 753 hip arthroscopy patients with 2-year follow-up, McGovern et al 42 found that 78.5% of patients did not improve in functional status (based on International Hip Outcome Tool–12 [iHOT-12] score) between 1 and 2 years after hip arthroscopy.
Collectively, the literature underscores the importance of functional improvements during the initial months after hip arthroscopy and suggests that this period could have a key association with functional scores for years to come. Postoperative rehabilitation programs after hip arthroscopy typically extend for 3 to 6 months,2,34,44,58 highlighting the delicate balance between achieving functional improvement and pain reduction while simultaneously being compliant and cautious with progression to avoid a potential setback that could harm recovery. 16 Furthermore, early identification of patients not improving adequately in the early postoperative period may allow for early intervention, with modalities such as extended patient-tailored formal rehabilitation and return-to-sport timelines modified in conjunction with the surgeon and physical therapist. 54 Thus, the purpose of this study was to determine whether early PRO improvements in the first 6 months after hip arthroscopy are predictive of functional outcomes at 5-year follow-up. We hypothesized that patients achieving 6-month MCID would have significantly greater rates of achieving 5-year MCID and overall superior PROs at final follow-up.
Methods
Study Design
Data were prospectively collected and retrospectively reviewed for patients enrolled in a hip arthroscopy registry who underwent surgery by a single, fellowship-trained sports medicine surgeon (S.D.M.). Patient inclusion criteria were (1) age ≥18 years; (2) primary hip arthroscopy for the treatment of symptomatic acetabular labral tears between May 2014 and January 2022; (3) completed preoperative, baseline PROs; (4) completed 6-month PROs; (5) and follow-up PROs at minimum 2 years. Exclusion criteria were (1) previous surgery on the ipsilateral hip; (2) advanced hip osteoarthritis (Tönnis grade ≥2); (3) radiographic evidence of hip dysplasia (lateral center-edge angle [LCEA] <20°); and/or (4) previous hip conditions (eg, fracture, inflammatory arthropathies, Legg-Calve-Perthes disease, slipped capital femoral epiphysis, or avascular necrosis).
Study Population
During the study period, patients who presented to the clinic of the senior author (S.D.M.) with hip pain underwent a standardized, preoperative evaluation, consisting of hip and pelvic radiographs (ie, anteroposterior [AP] pelvic, AP of affected hip, and Dunn lateral views) and physical examination with provocative testing of the labrum and assessment for impingement-related symptoms (eg, pain and/or limited ROM with flexion, adduction, and internal rotation or flexion, abduction, and external rotation). 28 Patients with positive clinical and radiographic findings underwent magnetic resonance arthrography to evaluate labral pathology, coupled with a diagnostic and therapeutic intra-articular hip joint injection (ie, combined local anesthetic with a low-dose corticosteroid). 38 Finally, all patients trialed initial nonoperative management, including activity modification and formal physical therapy, for ≥3 months. Patients who failed to achieve adequate symptom and functional improvement from nonoperative management and consented to undergo hip arthroscopy were offered enrollment in this prospective hip arthroscopy registry. 51 This study received institutional review board approval.
Functional Outcomes Evaluation
Survey questionnaires were distributed to patients before surgery (baseline), postoperatively at 6 and 12 months, and annually thereafter. Hip-specific PROs included the International Hip Outcome Tool–33 (iHOT-33), mHHS, and Nonarthritic Hip Score (NAHS). The percentages of patients who achieved MCID at various time points for these PROs were assessed. The MCID is defined as the smallest difference that patients perceive as beneficial and which would cause a change in management27,33; thus, applied to surgery, it represents the smallest or most conservative improvement in functional outcomes that a patient perceives before versus after surgery.30,33,46 It is also the most commonly employed metric of clinical relevance in arthroscopic surgery.12,17,30 For after hip arthroscopy, Kemp et al 35 defined the MCID as an 8-point improvement in the mHHS. Among the most frequently used PROs in hip arthroscopy,3,60 the mHHS has high validity because of its good correlation with the bodily pain and physical function subscales of the 36-Item Short Form Health Survey and its excellent test-retest reliability and construct validity demonstrated in heterogeneous hip arthroscopy patient populations.35,60 Thus, to determine the adequacy of functional improvement for the first 6 months after hip arthroscopy, the MCID value of 8 points for the mHHS was utilized to stratify patients into cohorts that achieved 6-month MCID, or had high improvement (HI), versus those that did not achieve 6-month MCID, or had low improvement (LI). 35
The percentages of patients who achieved threshold PRO scores for the MCID at 2 and 5 years postoperatively, as defined by Nwachukwu et al 46 and Rosinsky et al, 52 were calculated. Finally, patient satisfaction, rates of revision hip arthroscopy and incidence of conversion to THA were tracked via survey responses and review of the electronic medical record and compared between HI and LI cohorts.
Abbreviated Surgical Technique
After the administration of general anesthesia, all patients were positioned supine on a hip distraction table (Smith & Nephew) with a silicone-padded perineal post. Intra-articular access was first established with the anterolateral portal using intra-articular fluid distention under fluoroscopic guidance to avoid iatrogenic damage to the labrum. 1 Next, under direct arthroscopic visualization, the anterior, midanterior, and Dienst portals were placed to complete the puncture capsulotomy approach that avoids disruption of the iliofemoral ligament.15,21,24 Then, a thorough diagnostic survey was performed to assess the extent of damage to the labrum, chondrolabral junction, acetabulum, and femoral head articular cartilage. Elements of the surgical technique utilized included intermittent traction, pulsed intra-articular lavage to maintain ambient intra-articular temperatures, and an emphasis on chondrolabral junction preservation.45,47,57,59
As clinically indicated, capsular elevation and acetabuloplasty were performed to address underlying pincer deformities. 59 For labral lesions, simple repair was performed if adequate, healthy tissue was amenable to suture anchor fixation. Conversely, labral augmentation via capsular autograft was employed if the labrum was irreparable (eg, insufficient tissue, advanced degeneration, or complex tears).36,45,47 If the labrum was severely damaged, 5 to 10 mm of capsule was elevated with a knife rasp from the acetabular shelf, with careful, meticulous maneuvering to preserve capsulolabral blood supply. After acetabular osteoplasty (as indicated), the elevated capsular tissue was brought together with remaining labral tissue and seated to the acetabular ream with bioabsorbable compositive suture anchors. Western knots were dynamically tensioned with concurrent release of traction to ensure an “in-round” repair, with the knots tied away from the articular surface of the joint.14,36,45,47 During the study period, the senior surgeon (S.D.M.) transitioned from use of microfracture to a standardized method of bone marrow aspirate concentrate (BMAC) augmentation to address focal Outerbridge grade ≥2 lesions.39,40 Operative notes were reviewed to record which patients received microfracture, BMAC augmentation, or no additional chondral treatment. No other substantial changes or variations in surgical technique were applied within the study period. After addressing pincer impingement and labral lesions, traction was released to ensure restoration of the hip suction seal and confirm an in-round labral repair. As appropriate, cam deformities were resected via femoroplasty while the hip was flexed to 45°. Finally, a dynamic ROM examination ensured restoration of the labral seal and adequacy of the femoroacetabular decompression and was followed by closure of all incisions. Capsular closure was not performed, given the minimally invasive nature of the puncture capsulotomy technique, which does not significantly disrupt the hip capsule.
Postoperative Rehabilitation
Postoperatively, all patients followed the same 5-step, 6-month patient-guided rehabilitation program. First, patients were permitted immediate weightbearing as tolerated using a flat-foot gait with crutches for the first 6 weeks; for the first 3 of these weeks, they were prescribed daily deep vein thrombosis prophylaxis (aspirin; 81 mg). At 6 weeks postoperatively, patients began using a stationary bicycle with minimal resistance. At 10 weeks, patients could begin using an elliptical trainer on low resistance or swimming (with or without a pull buoy) while avoiding intense flutter kicking. At 4 months, patients resumed light strengthening exercises, including short arc leg presses and hamstring curls. Finally, at 6 months postoperatively, patients were permitted to resume impact-loading activities as tolerated. 44
Preoperative and Intraoperative Data Collection
Demographic and descriptive data were collected preoperatively, including age, sex, BMI, laterality, Tönnis grade, Tönnis angle, LCEA, alpha angle, and type of FAI. Intraoperative variables collected included traction time, Outerbridge grade for articular cartilage, labral tear size, Beck classification of labral damage and transition zone cartilage,5,6,41 type of osseous decompression performed for FAI, labral management (debridement vs repair vs augmentation), and use of additional treatment for cartilage defects (microfracture or BMAC).
Statistical Analysis
An a priori power analysis was performed based on previous literature to identify the number of patients necessary to achieve 80% power for our primary, 5-year outcome. Using an estimated standard deviation of the mHHS score of 14.4 and the 5-year MCID threshold of 11.4, 46 52 HI patients and 18 LI patients were necessary to achieve 80% power.
Categorical variables were analyzed with chi-square or Fisher exact tests, as appropriate. Continuous variables collected at a single time point (eg, age) were compared using 2-tailed independent t tests, while those collected longitudinally (ie, improvement in PRO scores) were assessed using linear mixed-effects models. 4 Mixed-effects models provide greater statistical power by linking repeated observations for each participant, accounting for interpatient variability, and incorporating all available data rather than excluding participants missing a single follow-up time point, as would occur with a t test or repeated-measures analysis of variance. Each regression clustered observations at the patient level; modeled time, achievement of 6-month MCID, age, sex, Tönnis grade, labral tear size, labral management (debridement vs repair vs augmentation with capsular autograft), use of additional chondral treatment (BMAC or microfracture), and baseline PRO score as fixed effects; and included random by-participant intercepts. Time was modeled as a continuous variable for all analyses. Parameter estimates and descriptive statistics for continuous variables are presented with 95% CIs.
Rates of achieving MCID at 2- and 5-year time points for each PRO were assessed. Predictors of achieving 5-year MCID for each PRO were assessed by multivariate logistic regression. The fixed effects used in linear mixed-effects modeling (ie, HI vs LI, age, sex, Tönnis grade, labral tear size, labral management, use of additional chondral treatment, and baseline PRO score) were each modeled in binary logistic regression; variables were chosen for final multivariate regression based on those achieving or approaching statistical significance (P < .10) in univariate analysis as well as consideration of clinically relevant predictors. Adjusted odds ratios (AORs), 95% CIs, and P values based on the Wald test approximation for each predictor were reported.
Frequency statistics are reported for all noncontinuous variables. A P value of <.05 was considered statistically significant. All statistical analyses were performed using R Version 4.3.1 (R Foundation for Statistical Computing).
Results
Patient Characteristics
Of the 391 consecutive patients prospectively enrolled in this study, 306 underwent primary hip arthroscopy for the treatment of symptomatic labral tears secondary to FAI between May 2014 and January 2022. After applying eligibility criteria, 175 (57.2%) of these 306 patients were included and are the basis of this study (Figure 1).

Flowchart detailing patient selection criteria. LCEA, lateral center-edge angle; PRO, patient-reported outcome.
Based on 6-month mHHS scores, 131 (74.9%) patients achieved 6-month MCID (HI cohort), while 44 (25.1%) patients did not achieve 6-month MCID (LI cohort); these groups formed the basis for all analyses. HI patients did not significantly differ from LI patients in any assessed demographic and radiographic variables including age, sex, BMI, laterality affected, Tönnis grade, Tönnis angle, LCEA, alpha angle, and type of radiographic FAI (P > .05 for each) (Table 1).
Baseline Patient Demographics and Radiographic Findings a

Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). FAI, femoroacetabular impingement; HI, high improvement; LCEA, lateral center-edge angle; LI, low improvement.
All patients had minimum 2-year follow-up. The mean lengths of follow-up were 3.81 ± 1.25 years for the HI cohort (n = 131) versus 3.68 ± 1.27 years for LI cohort (n = 44) (P > .05), with mean follow-up of 3.78 ± 1.25 years for all patients (N = 175) included in the primary analysis. Across the study cohort, 79 patients had 5-year follow-up.
Intraoperative Parameters
Various intraoperative parameters were assessed for differences between groups. Of those, only labral tear size differed significantly, with LI patients having on average larger labral tear sizes than HI patients (86.3° vs 78.9°; P = .04). There were no significant differences between groups with respect to traction time, Outerbridge grade of articular cartilage, Beck classification of labral damage, Beck classification of transition zone damage, FAI treatment, labral management, or use of additional chondral treatment (P > .05 for each) (Table 2).
Intraoperative Findings and Procedures Performed a

Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). BMAC, bone marrow aspirate concentrate; FAI, femoroacetabular impingement; HI, high improvement; LI, low improvement.
Achievement of 2- and 5-Year MCID
Rates of achieving clinically meaningful results, as assessed by attaining MCID, were assessed at 2 and 5 years after surgery for all PROs analyzed. At 2 years, 90.8% (n = 119) of HI patients achieved MCID for mHHS, compared with 56.8% (n = 25) of LI patients (P < .001). For iHOT-33, 88.5% (n = 116) of HI patients achieved MCID at 2 years, compared with 61.4% (n = 27) of LI patients (P < .001). Finally, for NAHS, 85.5% (n = 112) of HI patients achieved the MCID at 2 years, compared with 59.1% (n = 26) of LI patients (P < .001). These differences were all statistically significant (P < .001).
At 5 years, for mHHS, 88.3% (n = 53) of HI patients attained MCID, compared with 42.1% (n = 8) of LI patients (P < .001). For NAHS, 80.0% (n = 48) of HI patients reached MCID at 5 years, compared with 50.0% (n = 9) of LI patients (P = .02). There was no significant difference in rates of achieving 5-year MCID for the iHOT-33 score, with 86.7% (n = 52) of HI patients versus 77.8% (n = 14) of LI patients reaching 5-year MCID (P =.46) (Table 3).
Comparison of 2- and 5-Year MCID Achievement Between HI and LI Patients a
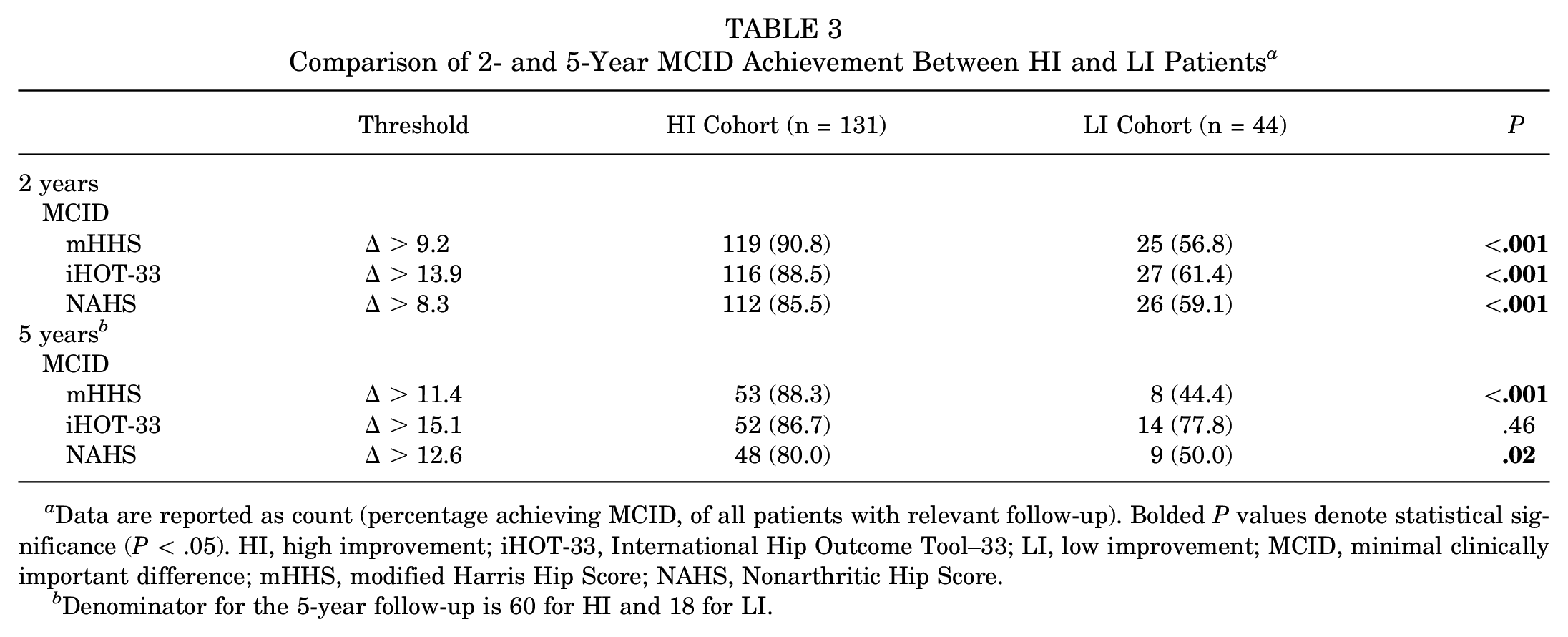
Data are reported as count (percentage achieving MCID, of all patients with relevant follow-up). Bolded P values denote statistical significance (P < .05). HI, high improvement; iHOT-33, International Hip Outcome Tool–33; LI, low improvement; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score.
b Denominator for the 5-year follow-up is 60 for HI and 18 for LI.
Multivariate logistic regression for achieving 5-year MCID for each PRO was performed, using achievement of 6-month MCID, sex, and labral management as predictors (Appendix Table A1). For mHHS, achieving 6-month MCID (AOR, 17.43; 95% CI, 3.81-79.72; P < .001) and labral augmentation (vs debridement; AOR, 14.50; 95% CI, 1.88-111.72; P = .01) were significant predictors of achieving 5-year MCID; sex was not a significant predictor (AOR, 3.31; 95% CI, 0.78-14.02; P = .10).
For iHOT-33, only labral augmentation (vs debridement; AOR, 10.61; 95% CI, 1.57-71.75; P = .015) was a significant predictor; achievement of 6-month MCID (AOR, 2.47; 95% CI, 0.54-11.38; P = .25) and sex were not significant predictors (AOR, 1.39; 95% CI, 0.35-5.51; P = .64).
Finally, for NAHS, achievement of 6-month MCID was a significant predictor of reaching 5-year MCID (AOR, 4.42; 95% CI, 1.34-14.57; P = .015). Labral treatment (augmentation vs debridement; AOR, 4.45; 95% CI, 0.74-26.61; P = .01) and sex were not significant predictors (AOR, 1.88; 95% CI, 0.63-5.62; P = .26).
PRO Scores
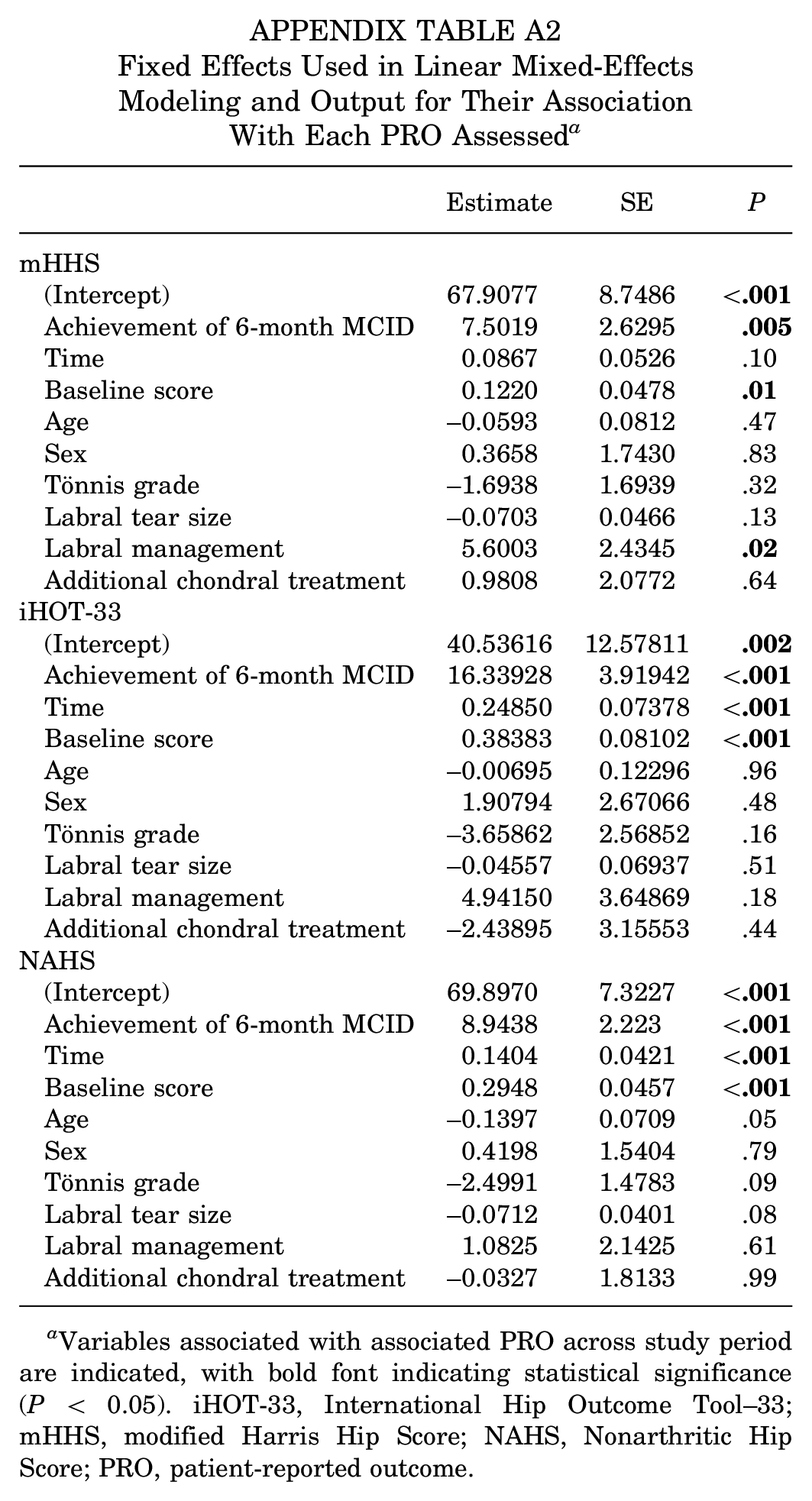
Mean PRO scores between HI and LI groups were compared at 1, 2, 3, 4, and 5 years with linear mixed-effects models controlling for potential covariates (ie, achievement of 6-month MCID, age, sex, Tönnis grade, labral tear size, labral management, use of additional chondral treatment, and baseline PRO score). HI patients had significantly greater mHHS scores at 1 year (87.5 vs 81.0; P = .005), 2 years (87.6 vs 82.0; P = .009), and 3 years (87.6 vs 83.1; P = .03); differences were not significant at 4 and 5 years (P > .05) (Table 4). Apart from achievement of 6-month MCID, labral procedure and baseline mHHS score were the only significant covariates in this model (Appendix Table A2). A plot of mHHS scores over 5-year follow-up is depicted in Figure 2.
Mean PRO Scores Through at Interval Time Points Through 5-Year Follow-up a
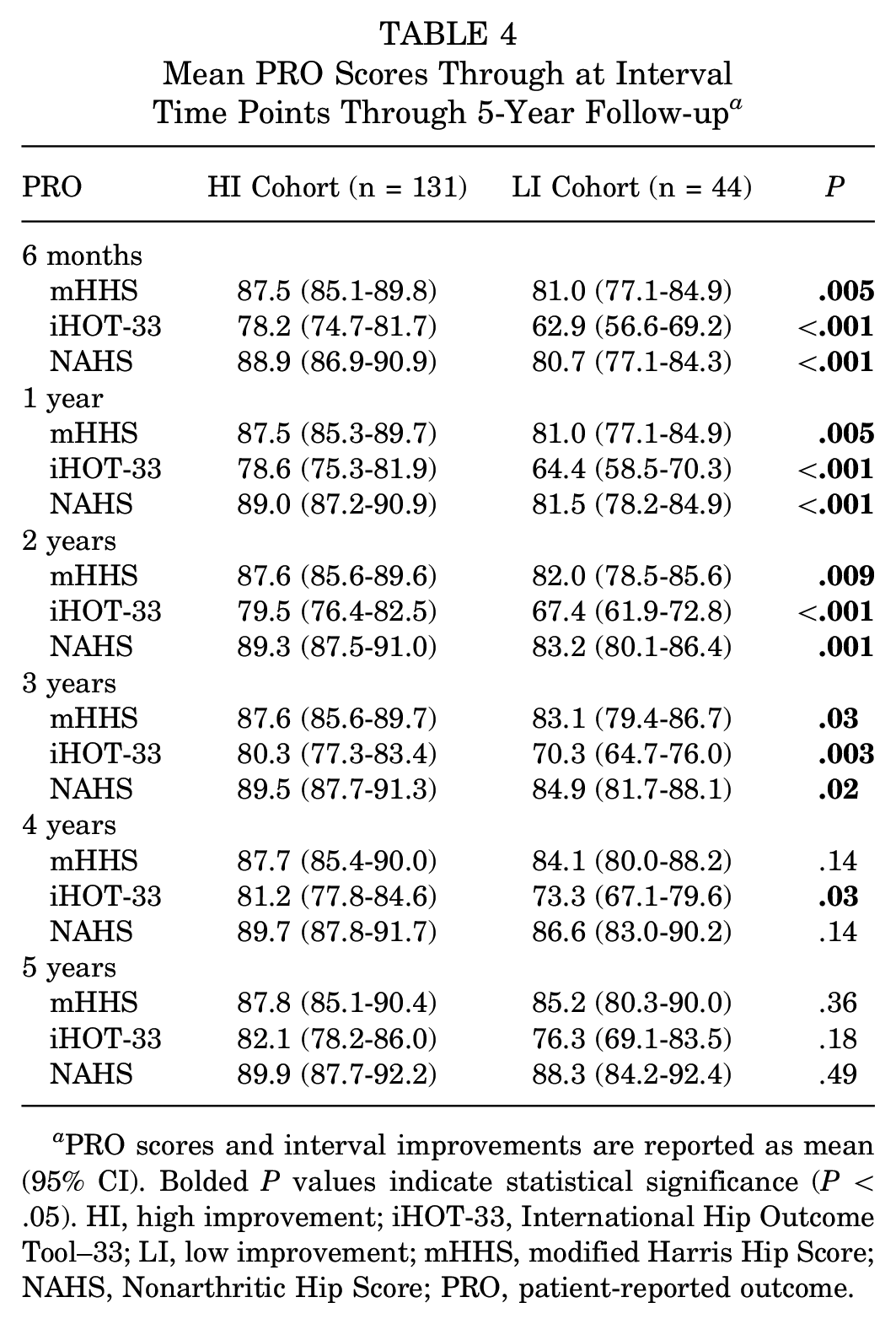
PRO scores and interval improvements are reported as mean (95% CI). Bolded P values indicate statistical significance (P < .05). HI, high improvement; iHOT-33, International Hip Outcome Tool–33; LI, low improvement; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; PRO, patient-reported outcome.

Scatterplot of modified Harris Hip Score (mHHS) values over 5-year follow-up for patients who did versus did not achieve 6-month minimal clinically important difference (MCID), with lines of best fit included.
For iHOT-33, HI patients had significantly greater scores at 1 year (78.6 vs 64.4; P < .001), 2 years (79.5 vs 67.4; P < .001), 3 years (80.3 vs 70.3; P = .003), and 4 years (81.2 vs 73.3; P = .03) (Table 4). Achievement of 6-month MCID and baseline iHOT-33 scores were the only significant predictors in the model (Appendix Table A2). A plot of iHOT-33 scores over 5-year follow-up is depicted in Figure 3.

Scatterplot of International Hip Outcome Tool–33 (iHOT-33) scores over 5-year follow-up for patients who did versus did not achieve the 6-month minimal clinically important difference (MCID), with lines of best fit included.
Finally, for NAHS, HI patients had significantly greater scores at 1 year (89.0 vs 81.5; P < .001), 2 years (89.3 vs 83.2; P = .001), and 3 years (89.5 vs 84.9; P = .02). Achievement of 6-month MCID and baseline NAHS scores were the only significant predictors of NAHS scores in this mixed-effects model (Appendix Table A2). A plot of NAHS scores over 5-year follow-up is depicted in Figure 4.

Scatterplot of Nonarthritic Hip Score (NAHS) scores over 5-year follow-up for patients who did versus did not achieve the 6-month minimal clinically important difference (MCID), with lines of best fit included.
In mixed-effects modeling, only achievement of 6-month MCID and baseline PRO scores were consistently associated with inferior PRO scores after controlling for fixed effects across all models (P < .05). Statistical output for all variables included in mixed-effects modeling is depicted in Appendix Table A2.
Patient Satisfaction and Subsequent Surgeries
Patient satisfaction, rates of revision hip arthroscopy, and rates of conversion to THA were tracked for all patients through the maximum available follow-up (mean follow-up for HI cohort, 3.81 years; LI cohort, 3.68 years). When evaluating postoperative patient satisfaction via a binary metric (ie, yes/no—are you satisfied with the treatment you received?), no significant difference was found between groups regarding percentage of satisfied patients (HI, 91.6%; LI, 81.8%) between cohorts (P = .09). With regard to rates of revision hip arthroscopy, no significant difference was found (HI, 4.6%; LI, 0%) between groups (P = .34). In addition, no significant difference was found in rates of conversion to THA (HI, 5.3%; LI, 11.4%) between groups (P = .18). Finally, overall rates of subsequent surgery were 9.9% in HI patients and 11.4% in LI patients (for 10.3% of all patients in aggregate), a difference that was not statistically significant (P = .78).
Discussion
The principal finding of the present study was that patients who did not achieve MCID for mHHS at 6 months after primary hip arthroscopy (25.1% overall) had significantly lower rates of achieving MCID at 5 years (42.1% vs 88.3%). Furthermore, achievement of 6-month MCID, along with labral management (augmentation vs repair vs debridement), was a significant predictor of achieving 5-year MCID. PRO scores were significantly lower through 3-year follow-up for patients who did not achieve 6-month MCID versus those that did. Finally, there was no statistically significant difference in rates of secondary surgeries at final follow-up between patients who did versus did not achieve 6-month MCID.
The most notable finding of the present study was that patients who did not achieve MCID for mHHS in the first 6 months after hip arthroscopy had significantly lower rates of achieving MCID at 5 years. Limited previous literature has explored the relationship between achieving clinical thresholds within the first 6 months after primary hip arthroscopy and mid- and long-term outcomes. In a study of 340 consecutive hip arthroscopies, Wolfson et al 61 found that not achieving PASS for mHHS by 6 months was associated with a 2.4-times greater odds of requiring reoperation at mean 50 months, but the authors did not assess the association between achieving 6-month PASS on subsequent clinically relevant outcomes. Lin et al 37 explored achievement of MCID for mHHS at 2 years after hip arthroscopy, stratified by achievement of MCID at 6 months, and found that a significantly lower proportion of patients who did not achieve 6-month MCID for mHHS achieved 2-year MCID (52%) relative to those that did achieve the 6-month threshold (88%). Assessing outcomes out to 5 years, the present study found a significantly decreased rate of achieving 5-year MCID for those patients who did not achieve the 6-month threshold (42.1%) relative to those that reached the 6-month threshold (88.3%). In fact, achievement of 6-month MCID was associated with 17.4-times greater odds of achieving 5-year MCID.
Given this significantly depressed 5-year MCID rate among patients failing to achieve 6-month MCID, the present study calls to attention the significance of addressing contributors to poor early outcomes and implementing proactive interventions that alter the outcome trajectory of patients exhibiting poor early improvements. First, a multitude of factors could contribute to patients’ not achieving satisfactory outcomes at 6 months, ranging from those associated with an overly ambitious return to activity (ie, because of noncompliance with rehabilitation protocol or rapidly returning to activities), not adequately progressing through rehabilitation (ie, due to lack of surgeon follow-up to ensure positive improvements, inadequate follow-up and/or communication with the physical therapist regarding rehabilitation protocol, or inadequate pain management), and/or socioeconomic determinants associated with any of these factors that may hinder recovery in various ways22,54,56; these effects could linger and limit achievement of clinically meaningful outcomes at 5 years after surgery. As shown in the present study, not achieving 6-month MCID was associated with 17.4-times lower odds of achieving 5-year MCID, and patients should be counseled accordingly. The effect of poor 6-month improvement on long-term functional outcomes underscores the importance of successful progression through the appropriate stages of postoperative rehabilitation after hip arthroscopy. Previously established postoperative protocols2,34,44,58 highlight the exercises and stages of improvement that a patient should achieve at various time points. For instance, our group employs a gradual, 5-step, 6-month patient-guided rehabilitation program 44 ; after weaning from crutches at 6 weeks, stage 3 (weeks 6-10) emphasizes increased ROM in a pain-free manner with light stationary biking, stage 4 (weeks 10-16) emphasizes gluteal and core trunk strength with exercises including clam shells, use of an elliptical trainer, and light swimming, and stage 5 (4-6 months) adds hip twisting activities. 44
Although the majority of patients achieve good outcomes at 6 months and may be able to begin gradual return to sport, surgeons should reevaluate a patient’s improvements at 6 months and assess whether further, early intervention may be needed. For surgeon protocols in which patients are assigned formal physical therapy in the acute postoperative period, communication with the physical therapist is essential to comprehensively assess the patient’s progress, setbacks, and reasons for lack of response to therapy. After assessment and addressing of such factors, extended physical therapy with patient-tailored modifications beyond 6-month follow-up may be warranted.44,54 This may include targeted retraining and strengthening of the deep hip rotator muscles (quadratus femoris, the gemelli, and obturator internus), muscles that have short lever arms and thus contribute dynamic hip stability to the femoral head in the acetabulum. 7 Such focus may accelerate rehabilitation following hip arthroscopy. For protocols that do not involve formal postoperative physical therapy, poor improvement may prompt consideration of prescribing formal physical therapy at this 6-month time point. 44 Furthermore, throughout the postoperative period, the physical therapist—in concert with the surgeon—should provide careful guidance regarding potentially delayed, patient-specific graduated return to sport by introducing sports-specific drills when appropriate.7,54 Given that most postoperative protocols end at around 6 months after surgery,2,34,44,58 this represents the most crucial time to intervene if patients are progressing poorly.
This study also found that PROs were significantly lower through 3-year follow-up for LI versus HI patients, but they did not significantly differ at 4- and 5-year follow-up. Mean scores for all PROs that were assessed—mHHS, iHOT-33, and NAHS—were significantly lower for LI patients for mHHS for all time points through 3 years. However, by 4- and 5-year follow-up, LI patients improved substantially relative to HI patients, such that only iHOT-33 was significantly inferior for these patients at 4 years and no PROs differed significantly between patients at 5-year follow-up. Previously, Bodendorfer et al 8 found that 70% of patients were “early progressors” after hip arthroscopy, demonstrating early improvement in iHOT-12 scores that persisted between 12 and 24 months. Similarly, McGovern et al 42 found that 78.5% of patients did not improve significantly in functional status (ie, iHOT-12 score) between 1 and 2 years after hip arthroscopy. In assessment of 5-year minimum clinical outcomes, Domb et al 19 reported that PRO score improvements at 2 years were sustained at 5 years; similarly, Perets et al 49 reported that the mHHS scores in athletes undergoing hip arthroscopy were not significantly different at 2- (86.3 ± 13.7) versus 5-year follow-up (87.0 ± 14.8). Finally, when assessing likelihood of achieving MCID, Nwachukwu et al 46 found that the number of patients achieving clinically significant outcomes (MCID, PASS, and substantial clinical benefit) increased through 2 years postoperatively, but that, interestingly, a lower percentage of patients achieved MCID at 5 relative to 2 years, suggesting potential for “some decline between 2 and 5 years.” In aggregate, these data suggest that the majority of patients experience improvements in functional outcomes early after hip arthroscopy; indeed, this group reaching 6-month MCID made up 74.8% of the present cohort. While previous literature suggests that PRO scores may continue improving up to 2 years postoperatively, when stratifying by achievement of 6-month MCID, the present study found negligible improvement in PROs for HI patients (ie, 0.3 points improvement in mHHS from 6 months to 5 years). In contrast, however, LI patients demonstrated notable functional improvements through 5 years despite initially poor 6-month progression, improving a mean of 4.2 points in mHHS from 6 months to 5 years—including 3.2 points after 2 years—when controlling for all fixed effects in linear mixed-effects modeling. This steady, late improvement was substantial enough such that, despite a difference in rates of 5-year MCID achievement, there was no significant difference in mean mHHS, iHOT-33, or NAHS scores at 4 and 5 years between cohorts. These data provide the novel insight that, despite differences in rates of achieving 5-year MCID, substantial functional improvement does occur beyond 2 years postoperatively after hip arthroscopy; a subset of patients may be “late progressors.” Consequently, in the event of an unfavorable 6-month outcome, those patients may be counseled that late improvements in functional outcomes can continue until ≥5 years postoperatively.
Finally, the present study assessed rates of patient satisfaction and subsequent surgeries in patients who did versus did not achieve 6-month MCID, finding no difference between groups. To date, only 1 study 23 that stratified patients by achievement of 6-month clinical threshold assessed incidence of subsequent surgery; the dearth of literature on this topic may be due to generally low rates of secondary surgery after hip arthroscopy and longer time frames needed to observe revision or conversion to THA. 23 The 1 study that reported on secondary surgery had a significantly larger sample size (N = 340), with a total of 51 patients (15%) undergoing subsequent surgery; not achieving PASS for mHHS at 6 months was associated with a 2.4-times greater odds of requiring reoperation at a mean 50-month follow-up after primary hip arthroscopy. The present study of 175 patients had only 18 (10.3%) subsequent surgeries at mean 46.3-month follow-up and found no significant difference in rate of revision hip arthroscopy, conversion to THA, or any subsequent surgery based on achievement of 6-month MCID; a larger sample size and longer follow-up could allow for more thorough assessment of effect of 6-month outcome on subsequent surgery rate.
Limitations
While this is the first study to assess the relationship between achievement of 6-month MCID and 5-year functional outcomes after hip arthroscopy, certain limitations should be noted. First, the findings reported are those of the senior author, who had already performed >1000 hip arthroscopies before May 2014. While this previous experience mitigated any risk of expert bias within the study cohorts, the outcomes of the present study may not be generalizable to all surgeons who use different techniques, particularly with regard to capsular management, method of labral reconstruction, and treatment of chondrolabral/chondral injury.21,39,43,45,47 Second, a number of patients (n = 124) could not be analyzed due to missing baseline, 6-month, or minimum 24-month PRO scores, which could have introduced the possibility of selection bias. Third, false-profile views were not obtained as part of the senior author’s preoperative radiograph series; thus, it is possible that patients with dysplasia based on low anterior center-edge angles were missed. Fourth, while the mHHS is widely used and has high construct validity and excellent test-rest reliability in hip arthroscopy research,3,35,60 questions have emerged regarding ceiling effects between 12 and 24 months. 35 Importantly, however, stratification by HI versus LI patients and constant improvements in the LI group suggest mitigation of this risk. Finally, while rates of 5-year MCID achievement significantly differed between HI and LI cohorts, metrics including subsequent surgery and patient satisfaction rates were similar at 5 years, suggesting that similarly favorable 5-year outcomes can occur despite not meeting 6-month MCID. Additional studies with larger cohorts at follow-up through 5 years are necessary to support this finding.
Conclusion
Our study demonstrates that early functional improvements after hip arthroscopy, assessed by 6-month MCID, predicted clinically meaningful outcomes at 5-year follow-up, underscoring the importance of early cautious recovery to prioritize labral healing while also meeting appropriate, stepwise rehabilitation milestones to advance functionally during these 6 months. Despite this, LI patients continued improving for 5 years, demonstrating that late functional improvements are still possible for certain patients in the event of a poor 6-month rehabilitation period.
Footnotes
Appendix
Fixed Effects Used in Linear Mixed-Effects Modeling and Output for Their Association With Each PRO Assessed a
| Estimate | SE | P | |
|---|---|---|---|
| mHHS | |||
| (Intercept) | 67.9077 | 8.7486 |
|
| Achievement of 6-month MCID | 7.5019 | 2.6295 |
|
| Time | 0.0867 | 0.0526 | .10 |
| Baseline score | 0.1220 | 0.0478 |
|
| Age | –0.0593 | 0.0812 | .47 |
| Sex | 0.3658 | 1.7430 | .83 |
| Tönnis grade | –1.6938 | 1.6939 | .32 |
| Labral tear size | –0.0703 | 0.0466 | .13 |
| Labral management | 5.6003 | 2.4345 |
|
| Additional chondral treatment | 0.9808 | 2.0772 | .64 |
| iHOT-33 | |||
| (Intercept) | 40.53616 | 12.57811 |
|
| Achievement of 6-month MCID | 16.33928 | 3.91942 |
|
| Time | 0.24850 | 0.07378 |
|
| Baseline score | 0.38383 | 0.08102 |
|
| Age | –0.00695 | 0.12296 | .96 |
| Sex | 1.90794 | 2.67066 | .48 |
| Tönnis grade | –3.65862 | 2.56852 | .16 |
| Labral tear size | –0.04557 | 0.06937 | .51 |
| Labral management | 4.94150 | 3.64869 | .18 |
| Additional chondral treatment | –2.43895 | 3.15553 | .44 |
| NAHS | |||
| (Intercept) | 69.8970 | 7.3227 |
|
| Achievement of 6-month MCID | 8.9438 | 2.223 |
|
| Time | 0.1404 | 0.0421 |
|
| Baseline score | 0.2948 | 0.0457 |
|
| Age | –0.1397 | 0.0709 | .05 |
| Sex | 0.4198 | 1.5404 | .79 |
| Tönnis grade | –2.4991 | 1.4783 | .09 |
| Labral tear size | –0.0712 | 0.0401 | .08 |
| Labral management | 1.0825 | 2.1425 | .61 |
| Additional chondral treatment | –0.0327 | 1.8133 | .99 |
Variables associated with associated PRO across study period are indicated, with bold font indicating statistical significance (P < 0.05). iHOT-33, International Hip Outcome Tool–33; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; PRO, patient-reported outcome.
Acknowledgements
The authors thank the Conine Family Fund for Joint Preservation for their continued research support.
Final revision submitted February 18, 2025; accepted March 17, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.D.M. has received funding from the Conine Family Fund for Joint Preservation and education payments from Kairos Surgical and honoraria from Allergan. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Partners HealthCare (No. 2019P002191/No. 2013P001442).