
Abstract
Background:
Readiness for return to sport (RTS) after surgery is often evaluated with strength and functional performance tests. However, relationships between RTS and patient-reported outcome measures (PROMs) after arthroscopic shoulder stabilization in adolescents and young adults is limited.
Purpose/Hypothesis:
The purpose of this study was to compare objective RTS testing in adolescent and young adult patients after arthroscopic shoulder stabilization with PROMs at time of testing. It was hypothesized that better PROM scores would correlate with better results in RTS testing.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Medical records of adolescent and young adult patients (13 – 21 years) who underwent arthroscopic shoulder stabilization at a single institution between 2017 and 2024 were reviewed. Data on patient demographics, operative details, PROMs [Tegner; American Shoulder and Elbow Surgeons (ASES) Shoulder Score; shortened version of Disabilities of the Arm, Shoulder and Hand (QuickDASH)], and RTS testing were collected. Data for each individual RTS assessment was categorized as “pass” or “fail” based on specified criteria. A Wilcoxon rank-sum test was used to compare differences in PROMs between those patients who passed versus those who failed a given test. Multivariate regression adjusted for age and body mass index.
Results:
A total of 59 patients were included (64.4% male; mean age, 16.1 ± 1.7 years); 66.1% underwent surgery on their dominant shoulder. RTS testing was performed at a mean of 6.4 ± 1.9 months postoperatively. Patients who passed the isometric external rotation strength test reported higher postoperative ASES scores (P = .04), while those who passed the isometric internal rotation strength test reported better QuickDASH scores (P = .009). Patients who passed the upper quarter Y-balance test reported significantly higher ASES (P = .005) and lower VAS (P < .05) and QuickDASH (P = .04) scores, postoperatively. Postoperative QuickDASH scores were also significantly better in those patients passing the grip strength test (P = .009). Multivariate analysis showed a 9.5-point difference in postoperative ASES scores between those who passed versus those who failed the upper quarter Y-balance test (P = .002), and a 7.1-point difference in QuickDASH scores between those who passed versus failed the grip strength test (P = .002).
Conclusion:
PROMs are associated with the ability to pass some RTS assessments, suggesting their potential utility in guiding clinical decision making regarding RTS readiness.
Arthroscopic labral repair or capsulorrhaphy is commonly utilized to manage shoulder instability in adolescent and young adult patients. After surgery, patients typically go through a structured rehabilitation program to regain strength and function in their shoulder. One important aspect of rehabilitation is determining when the patient is physically capable of safely returning to sport activities. In a systematic review of adolescents and young adults, Kim and Saper 12 revealed that considerable variation is reported in postoperative rehabilitation guidelines that follow arthroscopic Bankart repair for traumatic shoulder instability. All studies in the review used time-based criteria for determining return to sport (RTS), but patient-reported and objective criteria were lacking in most studies.
Strength and functional performance testing are objective components of RTS testing. Although there is currently no universally accepted RTS testing protocol, following completion of the patient’s rehabilitation program, patients undergo a series of objective tests in categories including strength testing, range of motion (ROM) testing, and functional testing. 7 However, limited data are available regarding RTS testing outcomes after arthroscopic shoulder stabilization, specifically in adolescent and young adult patients. Therefore, the purpose of this investigation was to assess the results of strength and functional RTS testing in adolescent and young adult patients who underwent arthroscopic stabilization. Additionally, this study sought to examine associations between RTS testing results and patient-reported outcome measures (PROMs) at the time of testing. We hypothesize that there is a correlation between better PROM scores and RTS testing results.
Methods
Study Design and Population
Institutional review board approval was obtained before the initiation of this retrospective study. The medical records of patients who underwent arthroscopic labral repair and/or capsulorrhaphy and subsequent RTS testing between April 2017 and March 2024 were reviewed. The inclusion criteria for this study were patients aged between 13 and 21 years who underwent arthroscopic surgery and completed RTS testing postoperatively. Arthroscopic procedures included anterior and/or posterior labral repair/capsulorrhaphy, and superior labrum anterior to posterior (SLAP) repairs. Patients with SLAP repair were included in this analysis because they had subjective instability and underwent arthroscopic labral repair with a similar rehabilitation protocol to those with labral repairs for objective instability. Revision cases, patients with a history of shoulder instability or surgical stabilization on the contralateral shoulder, and those with any ipsilateral or contralateral upper extremity condition or previous surgery that could potentially affect the outcomes of the RTS testing or PROMs were excluded from the study.
Surgical Technique
All surgical procedures were performed by a single sports medicine and pediatric fellowship–trained surgeon at a single institution (M.S.). Operative treatment was individualized to each patient; the surgical plan was based on the preoperative examination, diagnostic imaging, and intraoperative findings. Surgeries were performed under general and regional anesthesia 9 with the patient in the lateral decubitus position using modern arthroscopic techniques.
Postoperative Rehabilitation
Slight variations in ROM benchmarks, specific exercises utilized, and timing of initiation of closed kinetic chain exercises existed in rehabilitation protocols between arthroscopic posterior labral repair, arthroscopic anterior and posterior labrocapsulorrhaphy, and arthroscopic Bankart repair (Figure 1). Generally, during the maximal protection phase (weeks 1-6 postoperatively), the focus was on preventing muscle atrophy, reducing inflammation, and countering immobilization effects. Weeks 1 to 2 involved gentle passive ROM exercises, stretches, stabilization drills, isometrics, and cryotherapy. Weeks 2 to 3 introduced active assisted ROM (AAROM) exercises, scapular stabilization, rows, extensions, and thoracic mobility exercises. By 4 to 5 weeks, exercises progressed with ROM, isotonic strengthening, scapular stabilization, and additional exercises as needed.

Postoperative rehabilitation protocol. AAROM, active assisted range of motion; AROM, active range of motion; PROM, patient-reported outcome measure; ROM, range of motion; RTS, return to sport; UE, upper extremity.
The intermediate ROM and strengthening phase (weeks 6-13 postoperatively) aimed to restore ROM and improve neuromuscular control. Weeks 6 to 8 included gradual ROM increase, active ROM (AROM), AAROM, isotonic strengthening, stretches, and scapular stabilization. Weeks 9 to 13 focused on functional demands, advancing exercises, closed kinetic chain exercises, and a return to jogging/running program for runners and nonrunners alike.
In patients who underwent arthroscopic posterior labral repair or Bankart repair, the minimal protection phase (weeks 14-19 postoperatively) aimed to maintain AROM, improve strength and endurance, and gradually return to demanding activities. Relevant exercises progressed, light impact training and restricted sports activities were introduced, and interval sport programs began at week 16 if appropriate. In patients who underwent arthroscopic anterior and posterior labrocapsulorrhaphy, they were advanced to the dynamic strengthening phase (weeks 14-21) given they had full nonpainful ROM, no pain or tenderness, and ≥70% strength in internal rotation (IR) and external rotation (ER) compared with the unaffected limb measured via hand-held dynamometry. Goals were to maintain full AROM and functional reach capacity, to improve muscular strength and endurance, and to gradually return to more demanding functional activities. Relevant exercises were continued, plyometric upper extremity training for athletes was introduced, and an emphasis was placed on eventual return to restricted recreational activities. The advanced strengthening phase (weeks 20-23 postoperatively) focused on enhancing strength, power, endurance, and shoulder mobility with progression through relevant interval sports programs (eg, interval throwing program), when applicable.
RTS Testing
Based on multiple factors (eg, age, sport, competition level, physical therapy progress, and surgeon discretion) in a shared decision-making manner between the patient/family and surgeon, RTS testing was typically scheduled around 5 to 6 months postoperatively. RTS assessments were performed at the primary institution’s sports rehabilitation clinic by licensed physical therapists. Quality of movement, symmetrical body movement, comprehensive scores, and upper extremity testing were evaluated before endorsing a return to full competition. To complete upper extremity testing, various assessments were utilized. The uninvolved upper extremity was assessed first for each test, followed by the involved one. Each test was assessed in both upper extremities before transitioning to the next assessment. The ultimate decision for RTS clearance was determined by the senior author (M.S.) based on the overall performance on the RTS assessments, discussions with the patient/family and rehabilitation team, and consideration of the patient’s sport and activity level. Passing all (or a specific percentage of) components of the RTS test was not required for RTS clearance.
Passive ROM
Glenohumeral joint IR and ER passive ROM was measured using a goniometer with the shoulder abducted to 90° and a towel rolled under the shoulder while stabilizing the scapula to maintain neutral position. A side-to-side difference of ≤10° in both IR and total arc of motion was the criterion for passing the test.20,24
Isometric Strength
Isometric strength was assessed using a hand-held digital dynamometer (MicroFET 2; Hoggan Scienctific). Peak torques for shoulder ER and IR were collected with the patient lying prone and the shoulder in 90° of abduction and neutral rotation. The hand-held digital dynamometer was placed just proximally to the wrist (Figure 2). 2 Two maximal efforts were completed in each direction, and the mean torque (in lbs) of the 2 attempts was recorded.

Shoulder external rotation (left panel) and internal rotation (right panel) isometric strength testing with a hand-held digital dynamometer (right arm assessment).
Isokinetic Strength
Isokinetic strength was assessed using a biodex System 3 (Biodex Medical Systems) computerized robotic dynamometer. The patients were in the seated position (10°-15° reclined) and their arm was placed at 90° of abduction and 10° scaption. 23 Peak torque for shoulder IR and ER was evaluated at angular speed of both 180 and 300 deg/s. 23 Muscle strength was assessed using a limb symmetry index (LSI); both isometric and isokinetic strength testing with LSIs of ≥90% and ≥70% ER:IR ratio were considered passing criteria.2,23 The strength component of LSI and the ER:IR ratios were compared as separate entities.3,18
Grip Strength
Grip strength was assessed using a Jamar dynamometer, with hand position on the second smallest setting, the shoulder at neutral position, and elbow flexed to 90°. All assessments were performed bilaterally. The pass criterion for grip strength was achieving the ≥25th percentile of age and gender match normative values. 1
Functional Strength and Stability
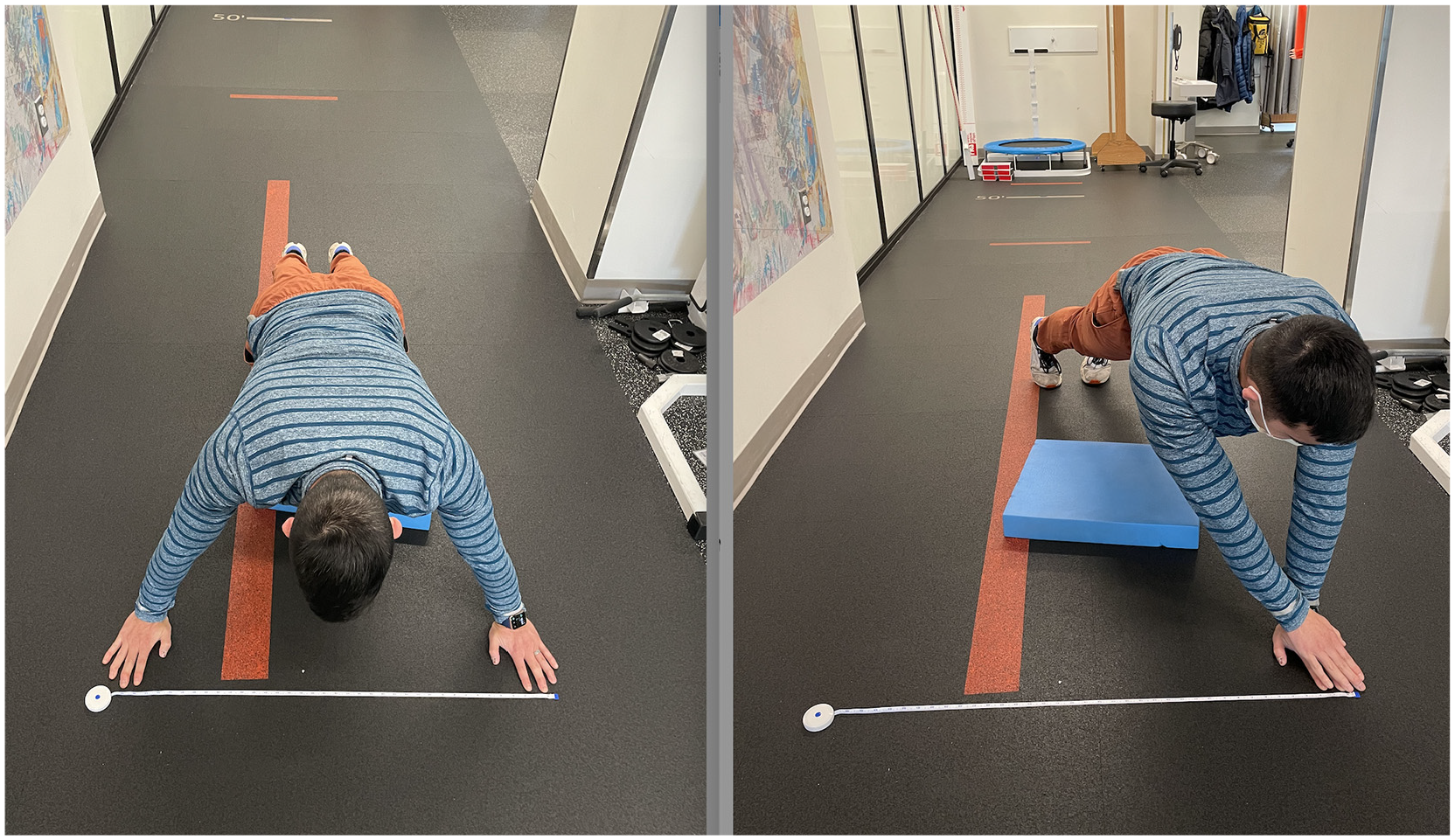
Functional strength and stability were assessed with a push-up test, Upper Quarter Y-Balance Test (YBT-UQ), Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST), and unilateral seated shotput test. Before the YBT-UQ and CKCUEST usage, the patient’s upper extremity weightbearing tolerance for test execution was screened with a push-up assessment. For this assessment, patients performed the maximal number of push-ups they could finish, to 90° of elbow flexion. For YBT-UQ, the patient’s arm length was measured in the upright position from the spinous process of the C7 vertebra to the distal tip of the right middle finger with the arm in 90° of abduction. The patient assumed a push-up position with all fingers, including the thumb, lateral to the line on the YBT kit. The shoulders began directly above the stance hand, with the feet perpendicular to the test kit approximately shoulder width apart. Once the patient lifted the reaching hand, he or she would push the reach indicators as far as possible in the following sequence without returning the hand to the ground: medial, inferolateral, superolateral (Figure 3). The patient was required to not lift or move the feet, touch only the front edge of the reach indicator, and then return to the starting position with control. If the patient lost balance, the sequence would start again from the beginning. All patients were given 2 practice trials followed by 3 reach trials. Patients who failed the trials due to faults were allowed up to 6 trials, and the maximal reach distance was taken for each direction. Faults included placing a hand on top of the reach indicator, touching the floor, lifting/moving one’s feet, shoving the reach indicator, or being unable to return to the starting position under control. It was not considered a fault if the patient elevated or lowered the hips. Shoes were optional and noted. A side-to-side difference of ≤4 cm in each direction and a composite score of ≥80 on each limb were the criteria for passing.5,22

Upper Quarter Y-balance Test assessment.
For the CKCUEST, the patient assumed a push-up position with the hands positioned on a marking 36 inches apart. Patients were instructed to lift 1 hand and touch it to the other hand, resulting in a shift in weight toward the static hand, with the objective of achieving as many touches as possible in 15 seconds (Figure 4). Each successful touch was recorded. The passing criterion for CKCUEST was ≥21 touches in 15 seconds. 22 The only exception to this criterion was if the patient had a small wingspan or was unable to perform 1 push-up. A modified test procedure transitioned patients to their knees with hands starting at shoulder width and reaching across their body to reach the 36-inch width markers.
Closed Kinetic Chain Upper Extremity Stability Test assessment.
Unilateral seated shotput test assessed the postoperative arm’s power using a 2-kg medicine ball. When compared with the nonsurgical limb, LSI of ≥90% was the criterion for passing the unilateral seated shotput test. 16 Comparative LSI was not adjusted for hand dominance.
Data Collection
Patient information and operative details, including age, sex, and hand dominance, were collected from medical records. PROMs including visual analog scale (VAS), Tegner activity score, American Shoulder and Elbow Surgeons (ASES) score, and the shortened version of Disabilities of the Arm, Shoulder, and Hand (QuickDASH) score were collected at the time of the RTS test. RTS testing results were also collected, including muscle strength and functional performance testing results.
Statistical Analysis
All the demographic information and clinical data including RTS testing were observed descriptively. Continuous variables were reported as means ± SD, and categorical variables were expressed as percentages and counts. Data for each individual RTS assessment was categorized as “pass” or “fail” based on previously described criteria. A Wilcoxon rank-sum test was used to compare differences in PROMs between those patients who passed versus those who failed a given test. Generalized linear regression analysis was conducted if there were significant differences observed in the bivariate analysis adjusting for age and body mass index (BMI). Predicted marginal means (least squares means) along with 95% CI were reported, and P< .05 determined significance. All the analyses were conducted in SAS Version 9.4 (SAS Institute Inc).
Results
A total of 59 patients were included in the study (Table 1). Overall mean age was 16.1 ± 1.7 years, and most patients (64.4%) were male. Football was observed to be the most common primary sport played by patients (33.9%). A total of 39 (66.1%) underwent surgery on their dominant shoulder. Patients underwent RTS testing approximately 6.4 ± 1.9 months after surgery.
Patient Demographics a

Data are reported as mean ± SD or n (%). BMI, body mass index; DOS, date of surgery; SLAP, superior labrum anterior to posterior.
Overall, there were statistically significant (P < .05) differences in VAS, ASES, and QuickDASH scores among patients who passed versus those who failed certain components of the RTS test, including YBT-UQ, isometric ER tests, and isometric IR tests (Table 2). Only testing components with significant differences in PROMs are displayed in Table 2, and all other test assessments were not statistically significantly different between those who passed and those who failed the measure. All patients failed ≥1 component of RTS testing.
Bivariate Comparison of PROMs per RTS Testing Component Between Pass and Fail Groups a

Data are reported as mean ± SD. Bold P values indicate statistical significance. ASES, American Shoulder and Elbow Surgeons; ER, external rotation; IR, internal rotation; PROM, patient-reported outcome measure; QuickDASH, shortened version of Disabilities of the Arm, Shoulder and Hand; RTS, return to sport; VAS, visual analog scale; YBT-UQ, Upper Quarter Y-Balance Test.
A statistically significantly lower mean postoperative VAS score was observed in patients who passed the YBT-UQ (0.4 ± 1.1 vs 1.2 ± 1.7; P = .045). In all test components, there were no statistically significant differences in mean Tegner scores in pass versus fail groups. In the bivariate analysis, mean postoperative ASES scores were observed to be statistically significantly higher in patients who passed YBT-UQ compared with those who failed (93.9 ± 8.2 vs 85.6 ± 12.6; P = .005). The multivariate analysis adjusted for age and BMI showed a statistically significant difference of 9.5 (95% CI, 3.6 to 15.3; P = .002) in ASES marginal means between those who passed versus failed the YBT-UQ. (Table 2). A similarly statistically significant difference was seen in ASES scores between those who passed versus failed the isometric ER strength test in the bivariate analysis (92.0 ± 11.1 vs 88.3 ± 10.6; P = 0.044); however, no statistically significant difference was seen in the multivariate analysis. Among patients who passed grip strength, postoperative QuickDASH scores were observed to be lower than those who failed (3.2 ± 5.1 vs 10.5 ± 11.3; P = .009). The estimated mean difference in postoperative QuickDASH between those who passed versus those who failed the grip strength test adjusted for age and BMI was also statistically significant (−7.1; 95% CI, −11.5 to −2.7; P = .002). Similarly, mean postoperative QuickDASH scores were statistically significantly lower in those patients who passed the YBT-UQ (3.6 ± 7.2 vs 7.1 ± 8.2; P = .044). A similar difference in means was seen in isometric IR strength testing (2.7 ± 5.5 vs 6.9 ± 8.8; P = .009). Multivariate analyses are shown in Table 3.
Multivariate Comparison of Pass and Fail Means Adjusted for Age and BMI, Reported for Significant Bivariate Models a

Bold P value indicates statistical significance. ASES, American Shoulder and Elbow Surgeons; BMI, body mass index; ER, external rotation; IR, internal rotation; PROM, patient-reported outcome measure; QuickDASH, shortened version of Disabilities of the Arm, Shoulder and Hand; VAS, visual analog scale; YBT-UQ, Upper Quarter Y-Balance Test.
Discussion
This study aimed to investigate the results of strength and functional RTS testing after arthroscopic shoulder stabilization in adolescent and young adult patients with shoulder instability and analyze the associations between PROMs and RTS testing results. We found that PROMs differed significantly between patients who passed certain components of RTS testing and those who failed the same components. This finding indicates a possible association between patients’ perception of their shoulder function and objective findings during functional testing. The results of this study can provide important insights into the effectiveness of arthroscopic shoulder stabilization surgery and the subjective and objective success of rehabilitation programs in adolescent patients with shoulder instability. It can also offer health care providers an additional tool when performing a holistic assessment of recovery to develop personalized treatment plans. For example, if a patient reports low functional capacity despite good objective strength, the provider may focus on interventions to improve confidence or address psychological barriers.
Our findings revealed no statistically significant difference in mean Tegner scores between patients who passed and those who failed tests. The scale was a measure of activity level at the time of the survey. Considering that at the time of administration, all patients were deemed ready for RTS testing by the surgeon but had yet to be cleared for full RTS, all the patients would be expected to be around the same level of activity. Conversely, there were statistically significant associations between particular PROMs and RTS test results. Specifically, higher 6-month postoperative ASES and lower QuickDASH scores were linked to better performance in certain strength and functional tests. The differences in those patients who passed and failed various tests suggest that PROMs can serve as valuable indicators of shoulder function and patient readiness to return to activities. Higher ASES scores and lower QuickDASH scores indicated better perceived shoulder function and reflected reduced disability.8,12,14 These subjective improvements in conjunction with objective test outcomes underscored the multifaceted nature of recovery and readiness in this patient population.
The most used criterion for determining RTS postoperatively is time elapsed since surgery,10,15 despite a lack of functional or individualized assessment of readiness to return. In a study by Wilson etal 25 investigating functional and strength readiness of 43 patients 6 months after arthroscopic shoulder stabilization surgery, only 5 patients successfully passed the battery of tests for strength or function. Strength testing revealed that only 7 achieved 90% of the nonoperative extremity strength; 26 patients successfully met functional test goals, and only 2 achieved strength goals but not functional goals, whereas 21 passed functional tests without meeting strength goals. In our assessment of RTS readiness at 6 months, using time frame and functional assessments alone for determining RTS readiness failed to consider potentially remaining strength deficits based on these results. Incorporating PROMs into the RTS assessment protocol may provide a more comprehensive evaluation of patient readiness. An integrated approach may enhance accuracy of readiness assessments and guide clinical decisions aimed at improving patient outcomes. A criterion-based RTS readiness approach may demonstrate promise with reduced injury recurrence and strength deficit. In a previous study evaluating the use of criteria-based RTS testing as the indicator for determining RTS readiness, Drummond etal 6 found that the risk of recurrent instability in the control group (n = 36) was 4.85 times higher at 22% recurrence rate. In the group with patients who underwent an objective RTS testing battery before being released for sports participation (n = 36), recurrence rate was 5%. These findings stress the importance of objective standards for determining RTS readiness. Otley etal 17 proposed a phased approach to assessing RTS readiness. Their proposal outlines a systematic approach that prioritizes functional ROM, absence of pain, and scapular and shoulder strength before moving on to performance-based strengthening and sports-specific training. Based on individual progress, these tests are introduced between 4 and 6 months. During the final phase, the athlete then undergoes a gradual and controlled process of practicing and participating in scrimmage games. They must meet specific criteria-based tests before being cleared to return to unrestricted competition. This stepwise progression ensures that the body is properly prepared for the demands of sports activities and helps to prevent injury. Although our stepwise rehabilitation framework was not directly based on Otley etal’s approach, our findings at the time of RTS testing explore the interplay of a patient’s perception of shoulder function and objective RTS tests. Based on the expanding pool of knowledge surrounding the importance of a holistic and individualized assessment for RTS readiness after arthroscopic shoulder surgery, further research should uncover the potential utility of Otley etal’s proposed approach.
Our findings are consistent with previous literature reporting that PROMs improve significantly after arthroscopic shoulder stabilization surgery19,21 and that strength deficits may persist at the 6-month postoperative benchmark. However, our study adds to the current body of knowledge by highlighting the utility of postoperative PROMs in correlating the objective strength and stability of the surgical limb. The persistence of shoulder strength and stability deficits at 6 months postoperative emphasizes the need for continued rehabilitation and monitoring of adolescent patients before allowing them to return to sporting activities. These results support the expansion of RTS protocols for this population to include PROMs to ensure safe and effective RTS activities.
Strengths and Limitations
There are several strengths of this study. Our study focused on a specific patient population: adolescent and young patients who underwent arthroscopic shoulder stabilization. Adolescents and young adults are at especially high risk of traumatic instability4,13 with some estimates of anterior shoulder dislocation incidence in adolescents participating in contact sports as high as 15%. 11 This study provides insight into the recovery and readiness for RTS testing in this population. Next, the study collected a comprehensive set of data points including demographics, operative details, PROMs, and objective RTS test results. This allows for a more thorough analysis of the factors that contribute to recovery and readiness for RTS. Additionally, the study utilized objective measures of strength and recovery, including limb symmetry index, to assess the patients’ recovery. Fourth, the study found statistically significant correlations between PROMs and objective strength and stability measurements, providing further evidence of the validity of these measures as predictive tools as well as potentially useful for setting realistic expectations with patients. Last, the study provides important clinical implications for the management of adolescent patients after arthroscopic shoulder stabilization, highlighting the need for expanded RTS readiness and tailored rehabilitation to address persistent deficits and ensure safe and successful RTS.
There are several limitations to our study. First, the cohort size, although adequate, was relatively small and had a follow-up period limited to approximately 6 months postoperatively. Future research should aim to validate these findings in larger cohorts with long-term RTS outcomes in patients who underwent arthroscopic shoulder stabilization. Additionally, the design as a small series with a single sports medicine fellowship–trained surgeon and a single physical therapy practice with heterogeneous procedures and techniques, where minor variations in technique, facilities, equipment, and other parameters may limit the generalizability of our findings. Furthermore, the scoring systems utilized were not specific or validated to the pediatric population for the most part. Our study used the unaffected limb as the comparison of full strength, which may not accurately represent the involved limb’s healthy baseline. Also, the study includes a variety of pathologies—anterior instability, posterior instability, combined anterior and posterior instability, and SLAP tears—which could be considered distinct groups with different criteria for RTS and PROM assessment; however, these pathologies were collectively analyzed under the broader category of instability, potentially limiting the specificity of our findings. Moreover, our study did not include a control group of uninjured athletes for comparison, and the study did not account for potential confounders such as level of competition or psychological factors affecting recovery. Although not the particular focus of this study, complications such as recurrence were not included in the analyses, nor was information such as whether patients returned to sport or not and, if so, at what level. Future studies will examine these questions to determine relationships between PROMs at various follow-up periods and RTS status, competition level, and complication rates.
Conclusion
Shoulder strength and functional deficits frequently persist in the surgical limb of adolescent and young adult patients who underwent arthroscopic shoulder stabilization surgery. VAS, QuickDASH, and ASES scores were associated with some objective shoulder strength and stability measurements. These findings highlight the importance of comprehensive RTS testing and continued rehabilitation for adolescent and young adult patients before allowing them to RTS. Further research is needed to understand the associations between PROMs and RTS testing and RTS outcomes and to establish optimal RTS testing protocols and reevaluate time frames in this population.
Footnotes
Acknowledgements
The authors would like to thank Shing Varakitsomboon for his assistance with this project.
Final revision submitted March 4, 2025; accepted March 17, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research reported in this article was supported by Seattle Children’s ASPIRE program. M.S. has received support for education from Arthrex Inc, Summit Surgical Corp, and Smith & Nephew; hospitality payments from Arthrex Inc and DJO; nonconsulting fees from Arthrex Inc; and a grant from DJO. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seattle Children’s Hospital (No. STUDY00004152).