
Abstract
Background:
Tennis is a popular sport among adolescents, but the repetitive overhead motions can lead to shoulder injuries. The risk factors for shoulder injuries in this population are not well understood.
Purpose:
To identify risk factors for shoulder injuries in adolescent tennis players and examine potential interactions between these factors.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Adolescent tennis players (N = 350; aged 12-18 years) were followed for 24 months. Baseline data on demographics, tennis experience, training volume, physical characteristics, and psychological factors were collected. Shoulder injuries (defined as any shoulder pain or dysfunction requiring ≥48 hours of time loss from tennis participation and medical attention) were recorded monthly. Cox proportional HR analysis with univariate and multivariate models was used to identify risk factors, with statistical significance set at P < .05.
Results:
A total of 88 players (25.1%) sustained shoulder injuries. Significant risk factors included age (hazard ratio [HR], 1.42; 95% CI, 1.16-1.74), years of playing tennis (HR, 1.25; 95% CI, 1.10-1.42), weekly training hours (HR, 1.18; 95% CI, 1.09-1.28), shoulder external/internal rotation strength ratio (HR, 3.12; 95% CI, 1.63-5.98), scapular dyskinesis (HR, 2.76; 95% CI, 1.46-5.22), and high levels of competitive anxiety (HR, 2.15; 95% CI, 1.24-3.73). Playing on hard courts increased injury risk compared with clay (HR, 1.68; 95% CI, 1.05-2.69) or grass courts (HR, 1.92; 95% CI, 1.14-3.24). Significant interactions were found between age and training volume (P = .01) and between shoulder strength ratio and scapular dyskinesis (P = .02).
Conclusion:
Our study demonstrated that multiple interacting factors contribute to shoulder injury risk in adolescent tennis players. Age, tennis experience, training volume, shoulder muscle imbalance, scapular dyskinesis, competitive anxiety, and playing surface were identified as significant risk factors. These findings can guide the development of targeted prevention strategies to reduce shoulder injury risk in adolescent tennis players.
Tennis is a popular athletic pursuit enjoyed by millions of youths globally. 36 However, the repetitive overhead motions, high-velocity serves, and demanding training schedules in tennis can lead to shoulder injuries.25,27 Adolescent tennis players are particularly vulnerable to these injuries because of their developing musculoskeletal systems, hormonal changes, and increasing training demands.11,22 Shoulder injuries can result in pain, absence from sports participation, and possible long-term repercussions.24,29 Identifying risk factors for shoulder injuries is essential for developing targeted prevention strategies and promoting the long-term health and performance of adolescent tennis players.3,43
Previous studies have explored risk contributors for shoulder injuries in adult tennis players,13,23 but limited research has focused on adolescent players. 8 Elements contributing to the risk of shoulder ailments in tennis athletes may encompass years lived, sex, proficiency degree, training quantity, playing area, arm mobility range, muscle force disparities, and abnormal scapular movement, as well as psychological elements.1,18,24,33 However, the relative contributions of these factors to shoulder injury risk in adolescent tennis players remain unclear, and potential interactions between risk factors have not been thoroughly explored.
The purpose of this study was to thoroughly examine the risk elements linked with shoulder injuries in adolescent tennis athletes, taking into account demographic, tennis-related, physical, and psychological factors, as well as potential interplays between risk elements. We hypothesized that both physical and psychological factors would contribute to shoulder injury risk, with significant interactions between age, training volume, and biomechanical parameters.
Methods
Study Design and Participants
This prospective cohort study included 350 adolescent tennis players (210 male, 140 female) aged between 12 and 18 years. The study was conducted as a collaborative effort between the Department of Sports Medicine, Sichuan University, and the Sichuan Provincial Institute of Physical Education. The participants were recruited from tennis clubs, academies, and high school teams across multiple regions within the province using a stratified sampling method to ensure representative distribution of age, sex, skill level, and playing surface. The inclusion criteria were (1) age between 12 and 18 years; (2) regular participation in tennis training and competitions (≥6 hours per week); (3) no history of shoulder injuries in the past 12 months; and (4) written authorized approval from participants and their parents/legal representatives. The study was sanctioned by the institutional ethics board and carried out in alignment with the Declaration of Helsinki. 46
Data Collection
At baseline, comprehensive data were collected through questionnaires, physical examinations, and performance tests. The questionnaires gathered information on demographic characteristics, tennis experience, training volume, playing surface, and psychological factors. Physical examinations and performance tests assessed shoulder range of motion (ROM), muscle strength, scapular dyskinesis, core stability, and flexibility.
Personal data encompassed years lived, sex, stature, body mass, and body mass index. Tennis background was appraised by the quantity of years partaking in tennis, proficiency level (club, county, state, or national), and hand dominance. Training quantity was evaluated by the amount of weekly practice hours, number of tournaments joined per year, and mean match duration in hours. 6 Playing surface was categorized as hard court, clay court, or grass court.
Shoulder ROM was assessed utilizing a digital inclinometer for internal rotation, external rotation, and total arc of motion. 7 Shoulder external/internal rotation strength ratio was ascertained employing a handheld dynamometer, with the player recumbent on his or her back and the shoulder abducted to 90°. 7 Scapular dyskinesis was appraised using the Scapular Dyskinesis Test, which entails observing scapular motion during weighted shoulder flexion and abduction movements. 32
Core stability was assessed using the prone plank test and the side plank test, measuring the maximal duration the player could sustain each position. 42 Flexibility was measured using the sit-and-reach assessment for hamstring and lower back mobility and the shoulder ROM test for shoulder internal rotation and horizontal adduction. 44
Psychological factors were assessed using validated questionnaires. Competitive anxiety was evaluated using the Sport Anxiety Scale–2, a 15-item survey instrument that measures somatic anxiety, apprehension, and concentration disruption. 41 Mental toughness was gauged using the Sports Mental Toughness Questionnaire, a 14-item survey that assesses self-assurance, consistency, and command. 39 Coping strategies were evaluated using the Athletic Coping Skills Inventory–28, a 28-item questionnaire that measures dealing with adversity, excelling under pressure, goal setting/mental preparation, focus, freedom from worry, confidence and achievement motivation, and coachability. 40 To account for changes related to growth, maturation, and ongoing tennis loading, we repeated musculoskeletal assessments (shoulder ROM, muscle strength, and scapular dyskinesis) at 6-month intervals throughout the 24-month study period.
Outcome Measures
The primary outcome measure was the incidence of shoulder injuries during the 24-month follow-up period. A shoulder injury was defined as any pain, discomfort, or dysfunction in the shoulder region that met all of the following criteria: (1) resulted in time loss from tennis training or competition for ≥48 hours, (2) required medical attention from a health care professional, and (3) led to a modification in normal training activities in terms of duration, intensity, or type of activity for at ≥1 week.
Injury data were collected monthly through online surveys and telephone interviews. At each monthly check-in, if an athlete reported a shoulder issue, we recorded the following and these variables were incorporated into the multivariate analyses.
Date of injury onset
Mechanism of injury (acute traumatic event, overuse, or insidious onset)
Time missed from full tennis participation
Effect on tennis performance (player’s self-report on a 0-10 scale)
Diagnosis and severity assessment by a sports medicine physician
All reported shoulder injuries were evaluated by a sports medicine physician to confirm the diagnosis and assess severity. Injuries were classified as mild (1-7 days of time loss), moderate (8-28 days of time loss), or severe (>28 days of time loss).
Statistical Analysis
Summarizing measures were utilized to condense the introductory characteristics of the participants. Continuous variables are exhibited as arithmetic means and standard deviations, whereas categorical variables are presented as frequencies and percentages. Cox proportional risks regression was employed to pinpoint risk factors for shoulder injuries. Univariate analysis was conducted initially, and variables with P < .10 were incorporated into the multivariate analysis. HR (95 % CI) were computed. Statistical significance was established at P < .05. Interaction effects between significant risk factors were also explored using Cox regression models with interaction terms. All analyses were executed using SPSS Version 26.0 (IBM Corp).
Sample size calculation was founded on an anticipated shoulder injury incidence of 20%, 20 with a strength of 80% and a significance threshold of .05. Presuming a 20% attrition rate, a sum of 350 participants was necessitated to discern a hazard ratio of 2.0 or greater for significant risk factors. 2
Results
During the 24-month follow-up, 88 (25.1%) players sustained shoulder injuries. The mean age of the injured players was 16.3 ± 1.4 years, and the mean tennis experience was 8.1 ± 2.2 years. The injured players had a higher weekly training volume (14.6 ± 3.2 hours) compared with the uninjured players (11.4 ± 2.6 hours). The most prevalent mechanism of injury was overuse (54%), followed by sudden onset during tennis strokes (36%), and traumatic events (10%). Of the 88 shoulder injuries recorded, 47 (53.4%) were classified as overuse injuries, 32 (36.4%) as acute injuries related to a specific tennis stroke, and 9 (10.2%) as acute traumatic events. The median time loss from full tennis participation was 14 days (IQR, 7-28 days). Regarding severity, 31 (35.2%) injuries were classified as mild, 42 (47.7%) as moderate, and 15 (17.0%) as severe. The mean effect on tennis performance, as reported by players, was 6.8 out of 10 (SD, 1.7). The most common diagnoses were rotator cuff tendinopathy (41%), shoulder impingement syndrome (27%), and labral tear (14%). Regarding the temporal distribution of injuries, we observed that 37 (42.0%) injuries occurred during the first 8 months of the study period, 29 (33.0%) during months 9 to 16, and 22 (25.0%) during months 17 to 24. A slight increase in injury incidence was noted during the summer months (June-August) across both years, accounting for 31 (35.2%) of all injuries. At the time of each reported injury, we collected data on recent training load, playing surface, and any recent changes in equipment or technique, which were incorporated into our risk factor analysis. All 88 reported shoulder injuries met our revised injury definition, requiring ≥48 hours of time loss from tennis, mandatory evaluation by a sports medicine physician, and ≥1 week of modified training.
Univariate analysis identified age, sex, years of playing tennis, skill level, weekly training hours, playing surface, shoulder external/internal rotation strength ratio, scapular dyskinesis, competitive anxiety, mental toughness, and coping strategies as potential risk factors (P < .10). In the multivariate analysis, age (HR, 1.42; 95% CI, 1.16-1.74), years of playing tennis (HR, 1.25; 95% CI, 1.10-1.42), weekly training hours (HR, 1.18; 95% CI, 1.09-1.28), shoulder external/internal rotation strength ratio (HR, 3.12; 95% CI, 1.63-5.98), scapular dyskinesis (HR, 2.76; 95% CI, 1.46-5.22), and high levels of competitive anxiety (HR, 2.15; 95% CI, 1.24-3.73) remained significant risk contributors for shoulder injuries (Table 1).
Multivariate Cox Proportional Hazards Regression Analysis of Risk Contributors for Shoulder Injuries in Adolescent Tennis Players

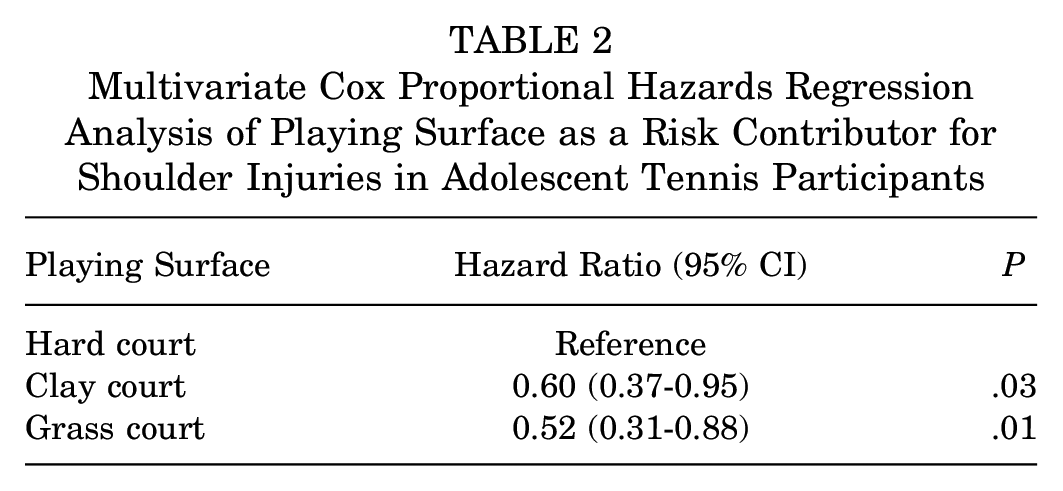
Additional analyses unveiled significant associations between shoulder injury risk and playing surface (Table 2). Players who primarily trained and competed on hard courts exhibited an elevated risk of shoulder injuries in comparison with those who played on Clay court HR 0.60 (0.37-0.95); Grass court HR 0.52 (0.31-0.88).
Multivariate Cox Proportional Hazards Regression Analysis of Playing Surface as a Risk Contributor for Shoulder Injuries in Adolescent Tennis Participants
Interaction effects were found between age and training volume (Table 3) and between shoulder strength ratio and scapular dyskinesis (Table 4). The risk of shoulder injury increased more steeply with higher training volumes in older players compared with younger players (interaction P = .01). Similarly, the presence of scapular dyskinesis amplified the effect of shoulder strength imbalance on shoulder injury risk (interaction P = .02).
Interaction Effect Between Age and Training Volume on Shoulder Injury Risk in Adolescent Tennis Players

Interaction Effect Between Shoulder Strength Ratio and Scapular Dyskinesis on Shoulder Injury Risk in Adolescent Tennis Players

Other factors, such as sex, skill level, shoulder ROM, core stability, flexibility, mental toughness, and coping strategies, were not significantly linked to shoulder injury risk in the multivariate analysis.
Longitudinal analysis of musculoskeletal parameters revealed significant changes over the 24-month study period. The mean shoulder external rotation strength decreased relative to internal rotation strength by 8.3% ± 3.2% (P < .001). Players who experienced a decrease in shoulder external/internal rotation strength ratio >15% had a significantly higher risk of shoulder injury (HR, 1.89; 95% CI, 1.24-2.87; P = .003).
Scapular dyskinesis was observed to develop in 18.3% (n = 64) of players who did not exhibit it at baseline. The development of scapular dyskinesis during the study period was associated with an increased injury risk (HR, 2.31; 95% CI, 1.42-3.76; P < .001).
Core stability, as measured by the prone plank test, improved on average by 14.2% ± 5.7% (P < .001) over the study period. However, this improvement was not significantly associated with shoulder injury risk (HR, 0.93; 95% CI, 0.78-1.11; P = .42).
Discussion
The major findings of our prospective cohort study identified several key risk contributors for shoulder injuries in adolescent tennis players and explored their interactions. Older age (HR, 1.42; 95% CI, 1.16-1.74), longer tennis experience (HR, 1.25; 95% CI, 1.10-1.42), higher training quantity (HR, 1.18; 95% CI, 1.09-1.28), shoulder muscle imbalance (HR, 3.12; 95% CI, 1.63-5.98), scapular dyskinesis (HR, 2.76; 95% CI, 1.46-5.22), competitive anxiety (HR, 2.15; 95% CI, 1.24-3.73), and playing on hard courts (HR, 1.68; 95% CI, 1.05-2.69) were associated with an elevated risk of shoulder injuries.
The findings regarding age, tennis experience, and training quantity suggest that the cumulative load on the shoulder from repetitive tennis movements over time may contribute to the development of injuries.12,35 The interaction effect between age and training quantity indicates that older players may be more vulnerable to the adverse effects of high training loads on shoulder health. Coaches and parents should monitor the training load of adolescent tennis players and ensure adequate rest and recovery to prevent overuse injuries. 4 Gradual progression of training intensity and quantity, as well as adherence to age-appropriate training recommendations, could assist in diminishing the risk of shoulder injury in this population. 26
Muscular imbalances in shoulder external/internal rotation strength ratio and scapular dyskinesis were recognized as major risk contributors, and their interaction effect suggests that the presence of both factors may synergistically heighten shoulder injury risk. These factors may alter shoulder biomechanics and lead to abnormal loading patterns, increasing the risk of injuries.24,28 Incorporating shoulder and scapular strengthening exercises, as well as movement pattern corrections, into training regimens could assist in mitigating the risk of shoulder injuries.9,14 Regular screening for muscular imbalances and scapular dyskinesis should be conducted to identify players at risk and provide targeted interventions. 31 Proper technique instruction and feedback on serving and overhead motions may also help optimize shoulder mechanics and reduce injury risk.37,38,45
Psychological factors, particularly competitive anxiety, also played a significant role in shoulder injury risk. High levels of competitive anxiety may lead to altered motor control, increased muscle tension, and altered biomechanics, increasing the likelihood of injury.15,34 Mental training techniques, such as relaxation, imagery, and self-talk, ought to be integrated into the comprehensive training regimen to assist players in managing competitive anxiety and mitigating injury risk.30,41 Fostering a supportive and positive team atmosphere, as well as providing resources for stress management and mental well-being, may further contribute to diminishing the influence of psychological factors on injury risk. 10
The association between playing surface and shoulder injury risk highlights the importance of surface-specific conditioning and injury prevention strategies. Hard courts, which are known to be less forgiving and produce higher impact forces, were linked to an elevated risk of shoulder injuries in comparison with clay and grass courts. 19 Coaches and trainers should consider incorporating surface-specific training and conditioning programs to help players adapt to the demands of different playing surfaces. 5 Proper shoe selection and the use of shock-absorbing insoles may also help reduce the impact forces transmitted to the shoulder during tennis play on hard courts.16,17
Interestingly, factors such as sex, skill level, shoulder ROM, core stability, flexibility, mental toughness, and coping strategies were not significantly linked to shoulder injury risk in this investigation. While these factors have been proposed to influence injury risk in other studies,21,37 their relative contributions may vary depending on the specific population and context. Future research should further investigate the role of these factors in shoulder injury risk among adolescent tennis players, as well as potential interactions between risk factors.
The inclusion of longitudinal musculoskeletal data in our study allowed us to account for changes due to growth, maturation, and tennis-specific adaptations. This approach provided a more comprehensive understanding of the musculoskeletal parameters associated with shoulder injury risk. For instance, we observed that players who experienced a decrease in shoulder external rotation strength relative to internal rotation strength over time were at a higher risk of injury (HR, 1.89; 95% CI, 1.24-2.87). Additionally, the development of scapular dyskinesis during the study period was associated with an increased injury risk (HR, 2.31; 95% CI, 1.42-3.76). These findings highlight the importance of regular monitoring and intervention to address adverse musculoskeletal changes in adolescent tennis players.
Strengths of this investigation include the prospective design, sizable sample, comprehensive data gathering, and extended follow-up duration. The utilization of validated questionnaires and standardized physical evaluations bolsters the dependability and legitimacy of the findings. The exploration of interaction effects provides valuable insights into the complex interplay between risk factors in shoulder injury development.
Limitations
We acknowledge several limitations in our study that affect the interpretation and effect of our findings. These include an initially imprecise injury definition, reliance on self-reported data introducing potential recall bias, limited data on functional impairment and return-to-play timelines, lack of real-time musculoskeletal data in relation to injury occurrence, and insufficiently precise load parameters (particularly regarding acute:chronic workload ratios). These constraints limit our ability to make highly specific recommendations for injury prevention and fully characterize the nature and severity of reported injuries. Future research should address these limitations by incorporating objective injury assessments, regular clinical evaluations, and wearable technology for accurate, continuous monitoring of player load and biomechanics. Studies should focus on determining optimal load management strategies, developing and validating tennis-specific conditioning programs addressing identified risk factors, and conducting intervention studies to test their effectiveness. In the interim, coaches and health care providers should emphasize gradual load progression, balanced strength training for the shoulder complex, and regular screening for musculoskeletal imbalances and technique flaws.
Conclusion
Our study demonstrated that multiple interacting factors contribute to shoulder injury risk in adolescent tennis players. Age, tennis experience, training volume, shoulder muscle imbalance, scapular dyskinesis, competitive anxiety, and playing surface were identified as significant risk factors. These findings can guide the development of targeted prevention strategies to reduce shoulder injury risk in adolescent tennis players.
Footnotes
Final revision submitted February 14, 2025; accepted March 11, 2025.
The author has declared the following potential conflict of interest or source of funding: This study was supported by the project “Research on the Introduction of Extension Training into Physical Education Classroom on Cultivating Comprehensive Quality Talents in Private Colleges and Universities” (No. MBXH20YB354). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Deyang Key Research Base of Philosophy and Social Sciences, Sichuan, China. (No. XLYXW2022005).