
Abstract
Background:
Pelvic control and pelvic-trunk coordination are essential for efficient energy transfer during a baseball pitch. Proper pelvis control ensures the smooth transmission of forces from the lower extremities through the trunk to the upper body. Although the importance of pelvic control has been acknowledged in baseball mechanics, its specific role during pitching remains underexplored.
Purpose/Hypothesis:
The purpose of this study was to examine the relationship between pelvic control, pelvic-trunk coordination, and pitching velocity in baseball pitchers. It was hypothesized that better pelvic control and coordination would significantly correlate with higher pitching velocity.
Study Design:
Descriptive laboratory study.
Methods:
A total of 34 asymptomatic male baseball pitchers were recruited from high school and collegiate teams. Pelvic control was assessed using inertial measurement units during a single-leg balance with movement test and the pitching motion. Pelvic-trunk coordination, assessed from foot contact to maximal external rotation and from maximal external rotation to maximal internal rotation, was analyzed using angle-angle plots of pelvic and trunk rotation. Coupling angles are categorized as in-phase (same direction) and anti-phase (opposite direction) coordination, with percentages calculated for each phase. Pitching velocity was measured using a radar gun.
Results:
Significant correlations were found between pelvic control in the axial plane in the single-leg stance test condition and pitching velocity (stride leg: r = −0.76, P < .01; drive leg: r = −0.65, P < .01). During pitching, pelvic angle variation in the axial plane also had a strong negative correlation with velocity (r = −0.78, P < .01). In addition, pelvic control showed distinct coordination patterns at different phases of the pitching motion. A higher percentage of anti-phase coordination from foot contact to maximal external rotation was positively correlated with pitching velocity (r = 0.74, P < .01), while a higher percentage of in-phase coordination from maximal external rotation to maximal internal rotation showed a positive correlation with pitching velocity (r = 0.58, P < .01).
Conclusion:
This study highlights the role of pelvic control and pelvic-trunk coordination in achieving higher pitching velocities, particularly in the axial plane. The findings highlight the significance of these factors in maximizing pitching velocity.
Clinical Relevance:
These findings highlight the importance of incorporating specific pelvic control and coordination exercises into training regimens for baseball pitchers to optimize pitching velocity.
Registered at ClinicalTrials.gov (NCT05644704).
Pelvic control is a critical factor in preventing injuries during the explosive mechanics of a baseball pitch. The force generation begins in the legs and progresses sequentially through the trunk to the upper extremities, forming a kinetic chain.9,29 Disruptions in this chain can result in excessive strain on joints, significantly elevating the risk of injury.7,16,28 Poor pelvic control, characterized by exaggerated pelvic deviations during movement, has been strongly associated with an increased likelihood of injury.4,18,19
In addition to injury prevention, effective pelvic control is essential for optimizing pitching performance. 8 The pelvis contributes over 50% of the kinetic energy and force required for a pitch, serving as a pivotal link in the kinetic chain.10,19 Pitchers with superior pelvic control achieve smoother and more efficient energy transfer from the lower limbs to the upper body, enhancing both mechanical efficiency and overall performance. In contrast, inadequate pelvic control results in energy leaks, which reduce performance and increase susceptibility to injury.4,5 Proper multi-joint coordination, 15 particularly between the pelvis and trunk, 24 also plays a vital role in effective pitching.6,21 However, previous research has not extensively addressed the coordination between these 2 regions. To bridge this gap, this study investigated pelvic-trunk coordination to gain deeper insights into pelvic control mechanisms during pitching.
Accurately measuring pelvic control is crucial for monitoring performance and preventing injuries. In previous studies, pelvic control has been assessed using an inertial measurement unit (IMU).18-20 A device was positioned at the middle of the posterior superior iliac spines, encircling the patient’s waist.18,20 The evaluation included 2 commonly used tests: the single-leg balance with movement test and the static single-leg bridge test.5,18,19 These assessments used a horizontal plane as a reference point to measure and calculate deviations from the starting pelvic neutral position in the sagittal and axial planes.4,5,18 These measurements provide valuable information about one’s ability to maintain pelvic control. The reliability analyses, which are expressed in terms of the intraclass correlation coefficient (ICC) and the standard error of measurement (SEM), showed promising results for the static single-leg bridge test (ICC = 0.91; SEM = 0.61°) and the single-leg balance with movement test 20 (ICC = 0.88; SEM = 0.93°). These findings demonstrate the tests’ consistent and precise nature in assessing pelvic control. While previous studies have evaluated pelvic control in controlled laboratory settings, these assessments do not fully capture the complexities of pitching in real-world scenarios. The lack of research evaluating pelvic control during actual pitching motions represents a significant gap in our understanding of its effect on energy transfer and injury risk.
IMUs have become indispensable tools in sports biomechanics, providing a wearable and wireless solution for analyzing dynamic pitching motions. IMUs can precisely capture critical kinematic parameters such as joint trajectories, angular velocity, and acceleration throughout the pitching sequence by integrating accelerometers, gyroscopes, and magnetometers. 31 Previous studies have successfully utilized IMUs to detect and analyze pitching mechanics.12,17 This technology enables researchers to identify inefficiencies in movement patterns and design individualized training programs to improve athletic performance.
Despite the recognized importance of pelvic control, no studies have directly evaluated pelvic control during the pitching motion. This limitation restricts our understanding of how pelvic control influences performance in dynamic settings. Therefore, this study aimed to explore the relationship between pelvic control, pelvic-trunk coordination, and pitching velocity in baseball pitchers. We hypothesized that superior pelvic control and effective pelvic-trunk coordination would significantly correlate with increased pitching velocity, offering a more comprehensive understanding of their roles in pitching mechanics.
Methods
Participants
Baseball pitchers were recruited from the high school and collegiate baseball leagues. This study was approved by the research ethics committee of the university hospital. Participants who met the following inclusion criteria were eligible for the study: (1) age between 15 and 25 years; and (2) asymptomatic male baseball pitchers. The exclusion criteria were as follows: (1) history of shoulder or elbow surgery; (2) injury to the shoulder or elbow within 3 months before this study; (3) history of brachial plexus injury.
A power analysis was conducted using G*Power 3.1 software to ensure adequate statistical power. Based on a target power of 0.80, an alpha level of .05, and an effect size of 0.5, the analysis indicated that a minimum of 29 participants was required for the study. 24
Experimental Setup
The data were collected in a single session at the baseball field, including the prepitching and pitching stages. At the prepitching stage, demographic information and single-leg balance with a movement test were assessed for each participant to determine pelvic control. A single IMU (IMU; Xsens MVN Awinda, Xsens Technologies BV) was attached to the pelvis to measure such pelvic control. The sensor has 3 triaxial sensors: a 3-dimensional (3D) accelerometer (scale: ±160 m/sec2), a 3D gyroscope (scale: ±2000 deg/sec), and a 3D magnetometer (scale: ±1.9 Gauss). After the measurements, participants were given sufficient time to warm up. At the pitching stage, each pitcher was instructed to throw 10 fastballs with maximum effort toward a catcher at the home plate. During the pitching stage, 3 additional IMUs were attached to the sternum, the upper arm of the pitching arm side, and the thigh of the stride leg to capture the acceleration and gyroscope signals. To ensure the reliability of the data, all IMUs were consistently attached by the same licensed physical therapist following a standardized protocol. At the same time, pitching velocity was measured using a radar gun (Ball Coach Radar, Pocket Radar Inc).
Pelvic Control in Single-leg Balance With Movement Test at the Prepitching Stage
A wireless IMU was utilized to evaluate pelvic control. The IMU was securely fastened to an elastic belt around the participant’s waist, covering the anterior and posterior superior iliac spines (IMU 1; Figure 2). 20 To define the zero position, a licensed physical therapist positioned the participant’s pelvis in a neutral position, which was set as the 0° of reference for subsequent measurements.
The single-leg balance with movement test measured the pelvic control. 19 In the first step, every participant adopts a balanced stance, positioning their feet at a distance equal to the width of their shoulders. In the second step, they were instructed to transfer their entire body weight onto the testing leg, concurrently flexing the hip of the nontesting leg to lift the foot 10 cm above the ground. In the third step, participants maintained this posture for 2 seconds, ensuring that all their weight was supported by the leg being tested and then reverting to the starting position.18,19 This entire sequence was repeated 3 times for the participant’s drive and stride legs. Each participant’s drive leg is called the back leg during pitching, while the stride leg is the front leg.
A total of 4 variables were calculated for each leg during the single-leg balance with movement test, including deviation angle in the sagittal plane, deviation angle in the axial plane, variation angle in the sagittal plane, and variation angle in the axial plane. The angles were calculated directly using the roll, pitch, and yaw values provided by the IMUs, where the pitch value represents the rotation in the sagittal plane, and the yaw value represents the rotation in the axial plane. The deviation angles in the sagittal and axial planes were calculated as the maximum peak absolute pelvic tilt from the zero-position using the IMU sensor (Figure 1).5,18 Moreover, the variation of pelvic angle was determined as the mean of the squared deviations of the pelvic angle from its mean value across the pitching motion. Specifically, the difference between the measured pelvic angle and its mean value was squared for each data point, and the mean of these squared differences was computed. The pelvic angle deviation was included to enable comparisons with previous studies, while pelvic angle variation reflects the dynamic control of pelvic motion.

Measurement of pelvic angle deviations in the axial and sagittal planes with IMU sensor. IMU, inertial measurement unit.
Pelvic Control at the Pitching Stage
Pelvic control was measured using 4 IMUs during the pitching motion. The 4 IMUs were attached to the pelvis (IMU1) (Figure 2), sternum (IMU2), upper arm of the pitching arm side (IMU3), and thigh of the stride leg (IMU4). The IMUs attached to the thigh and the upper arm were used to detect the pitching events, including the foot contact, the maximal shoulder external rotation, and the maximal shoulder internal rotation. The IMU attached to the pelvis and sternum recorded pelvic and trunk angles continuously throughout the participant’s pitching movement, encompassing 10 pitches.
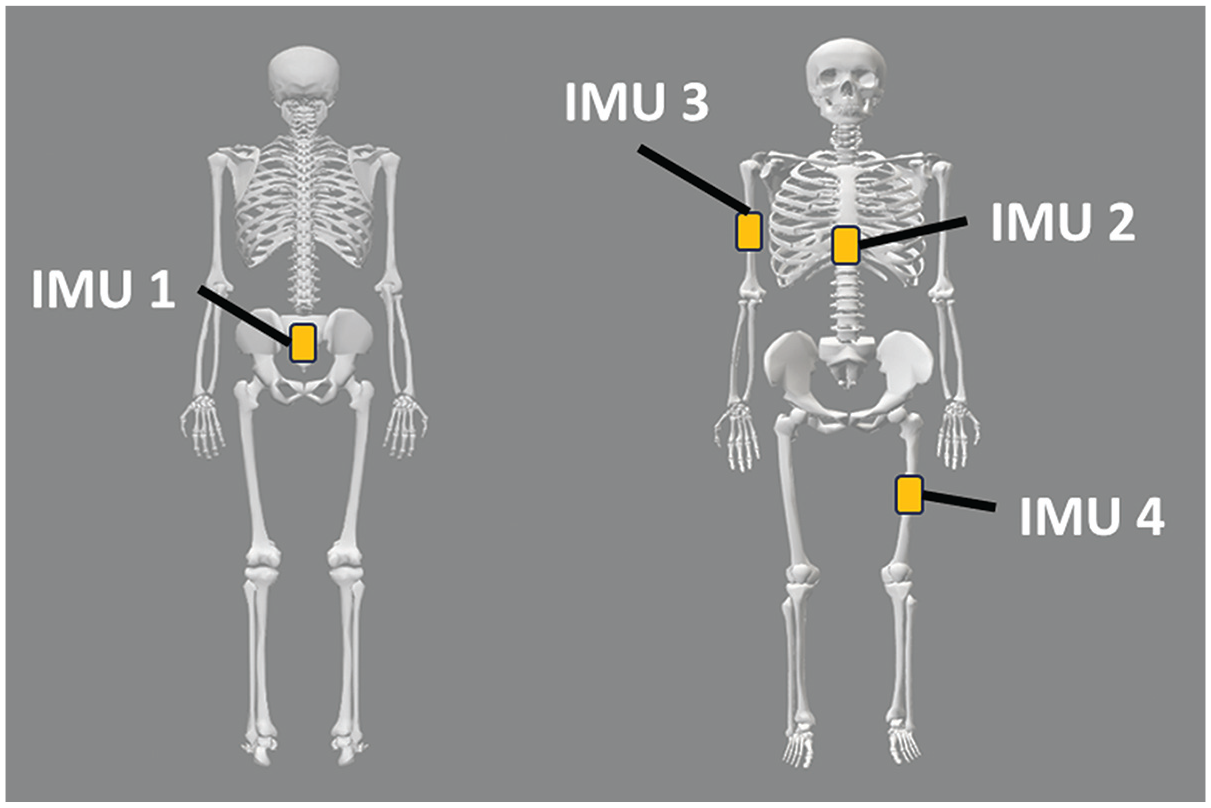
IMU locations for a right-handed pitcher; IMU 2 and IMU 4 on the opposite limb for a left-handed pitcher. IMU 1, on the pelvis; IMU 2, on the sternum; IMU 3, on the upper arm of the pitching arm side; IMU 4, on the thigh of the stride leg. IMU, inertial measurement unit.
The peak angular velocity of the gyroscope signal was recorded to measure pelvic control during pitching. Each peak in the gyroscope signal from the IMU attached to the pelvis represented a single pitch. The signal processing included a 100 Hz sampling rate and a 4th-order Butterworth filter to ensure data quality. 17 To segment the data, 10 peaks were identified throughout the gyroscope signal, with each corresponding to an individual pitch. In the analysis of each pitch, the “foot contact (FC)” event marks the beginning of the pitching motion, defined as the point when the angular velocity of the stride leg’s thigh reaches its peak. Conversely, the “maximal internal rotation (MIR)” event represents the end of the pitching motion, occurring when the shoulder’s rotation angle achieves its maximum internal rotation.
Pelvic control was measured during the pitching motion (from FC to MIR) as indicated by the pelvic angle variation in both the sagittal and axial planes using data from the IMU.3,13
Pelvic-Trunk Coordination in Pitching Movement
To gain a detailed understanding of the coordination between the pelvis and trunk during pitching, the motion was divided into 2 phases. The first phase was from the FC event to the “maximal external rotation (MER)” event, defined as the point where the shoulder reaches its maximal external rotation. The second phase was from the MER event to the MIR event. To assess coordination, angle-angle plots were generated to represent the relationship between pelvis and trunk rotation throughout the pitching motion, focusing specifically on the phases between FC and MER, as well as between MER and MIR. Coupling angles were derived from these plots using the following equation:

Where t represents each time instant, and β and θ represent time-series data for the pelvic and trunk angles, respectively. 25 These coupling angles ranged from 0° to 360° and were categorized into 2 patterns: in-phase (both joints rotating in the same direction) and anti-phase (joints rotating in opposite directions). The percentage of in-phase and anti-phase coordination was calculated for both phases 25
Pitching Velocity
A catcher was positioned behind home plate, located 18.4 meters distant. A total of 10 fastball trials were conducted. The velocity of the ball (m/sec) during each pitching trial was recorded using a speed radar gun (Ball Coach Radar; Pocket Radar Inc) positioned behind the home plate. The mean values of the pitching velocity were evaluated.
Statistical Analysis
PASW Statistics 26.0 for Windows (SPSS) was used to analyze this study’s statistical analysis. In single-leg balance with movement test during the prepitching stage, factors to consider include the deviation angle in the sagittal plane, the deviation angle in the axial plane, the variation angle in the sagittal plane, and the variation angle in the axial plane in both the stride leg and the drive leg. In pitching movement, factors to consider include pelvic angle variation in both the sagittal and axial planes during the pitching motion and the percentage of in-phase and anti-phase coordination in the phases between FC and MER and between MER and MIR. The significance threshold was set at .05, and the Shapiro-Wilk test was used to determine the normality of all variables. The parametric method was used in this study because the data followed a normal distribution. The Pearson correlation coefficient was employed to evaluate the correlation between the variables and ball velocity. Pearson correlations <0.30 are considered weak, between 0.31 and 0.39 are moderate-weak, between 0.40 and 0.60 are moderate, between 0.61 and 0.69 are high-moderate, and between 0.70 and 1 are high.2,32
Results
A total of 34 baseball pitchers were recruited. The pitchers were (mean ± SD) 19 ± 2.6 years old, 179.4 ± 5 cm tall, 77.5 ± 9.9 kg in mass, and had a training duration of 8 ± 2.8 years. A total of 26 pitchers were right-handed, while the remaining 8 pitchers were left-handed.
Pelvic Control in Single-leg Balance With Movement Test at the Prepitching Stage
In Pelvic Angle Deviation
When the stride leg was being tested, a significant negative correlation was observed between pelvic angle deviation in the axial plane (mean ± SD: 0.9°± 1.2°) and pitching velocity (mean ± SD: 35.5 ± 1.7 m/sec) (r = −0.76, P < .01). A moderate negative correlation was found between pelvic angle deviation in the sagittal plane (mean ± SD: 4.5°± 3.4°) and pitching velocity (r = −0.37, P = .03) (Figure 3).
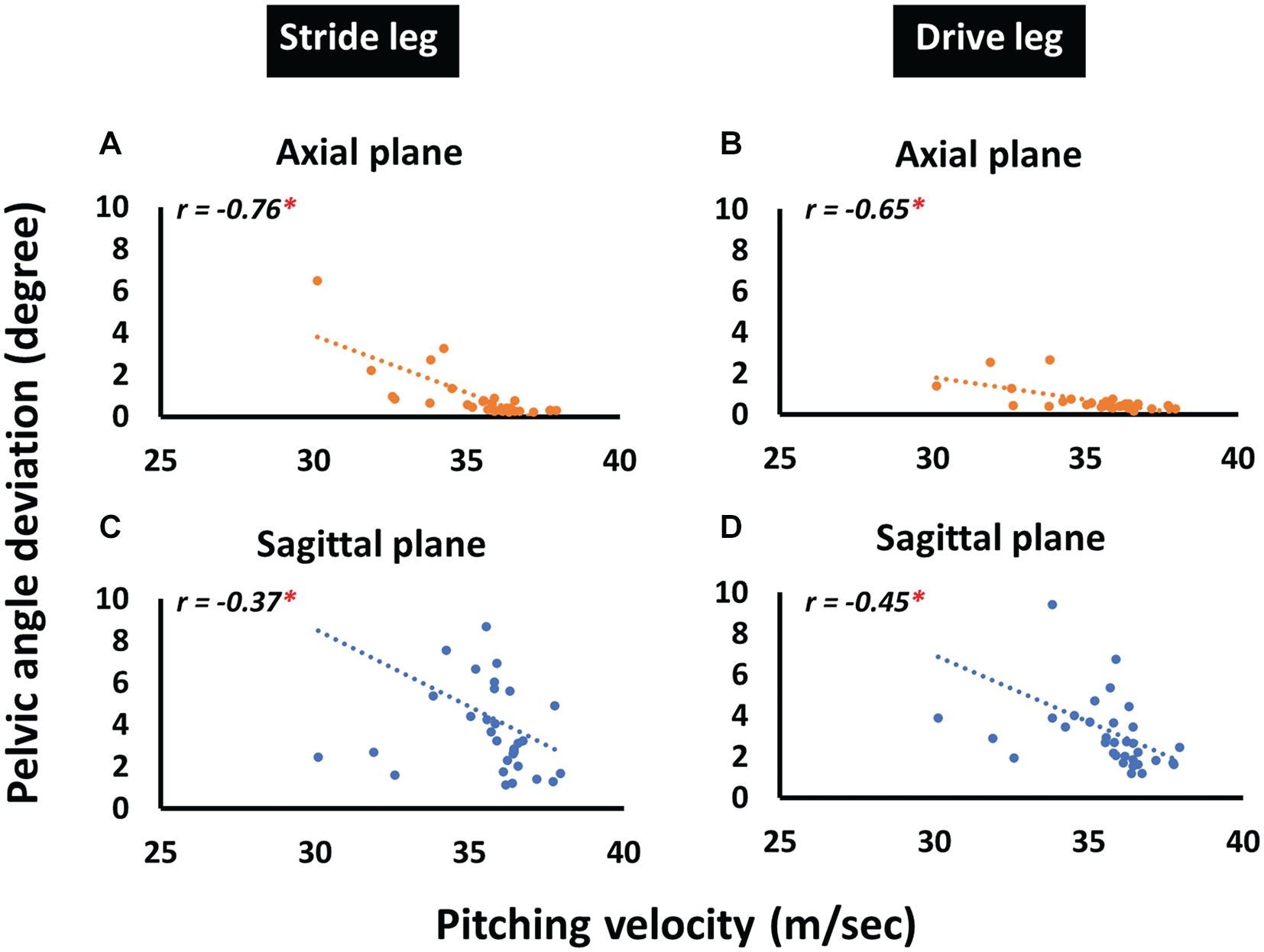
Correlation between pelvic angle deviation and pitching velocity in single-leg balance with movement test. (A) Axial plane on the stride leg. (B) Axial plane on the drive leg. (C) Sagittal plane on the stride leg. (D) Sagittal plane on the drive leg. *Statistically significant correlation at P < .05.
When the drive leg was being tested, a strong negative correlation was found between pelvic angle deviation in the axial plane (mean ± SD: 0.6°± 0.5°) and pitching velocity (r = −0.65, P < .01). Moreover, a moderate negative correlation was observed between pelvic angle deviation in the sagittal plane (mean ± SD: 3.3°± 2.4°) and pitching velocity (r = −0.45, P < .01) (Figure 3).
In Pelvic Angle Variation
When the stride leg was tested, a significantly high-moderate negative correlation was found between pelvic rotation variation in the axial plane (mean ± SD: 3.2°2± 3.1°2) and pitching velocity (r = −0.68, P < .01). However, no significant correlation was found between pelvic rotation variation in the sagittal plane (mean ± SD: 4.9°2± 8.9°2) and pitching velocity (r = −0.32, P = .07) (Figure 4).

Correlation between pelvic angle variation and pitching velocity in the single-leg balance with movement test. (A) Axial plane on the stride leg. (B) Axial plane on the drive leg. (C) Sagittal plane on the stride leg. (D) Sagittal plane on the drive leg. * Statistically significant correlation at P < .05.
When the drive leg was being tested, a significant moderate-weak negative correlation was found between pelvic rotation variation in the axial plane (mean ± SD: 4.4°2± 4.2°2) and pitching velocity (r = −0.38, P = .03). However, no significant correlation was found between pelvic rotation variation in the sagittal plane (mean ± SD: 4.7°2± 9°2) and pitching velocity (r = −0.32, P = .07) (Figure 4).
Pelvic Control in Pitching Movement
The relationship between pelvic control and pitching velocity during the pitching motion is illustrated in Figure 5. A significantly high negative correlation was found between the variation angle in the axial plane (mean ± SD: 77.1°2± 53.4°2) and pitching velocity (r = −0.78, P < .01), while no significant correlation was observed between the variation angle in the sagittal plane (mean ± SD: 146.1°2± 89.6°2) and pitching velocity (r = 0.08, P = .65).
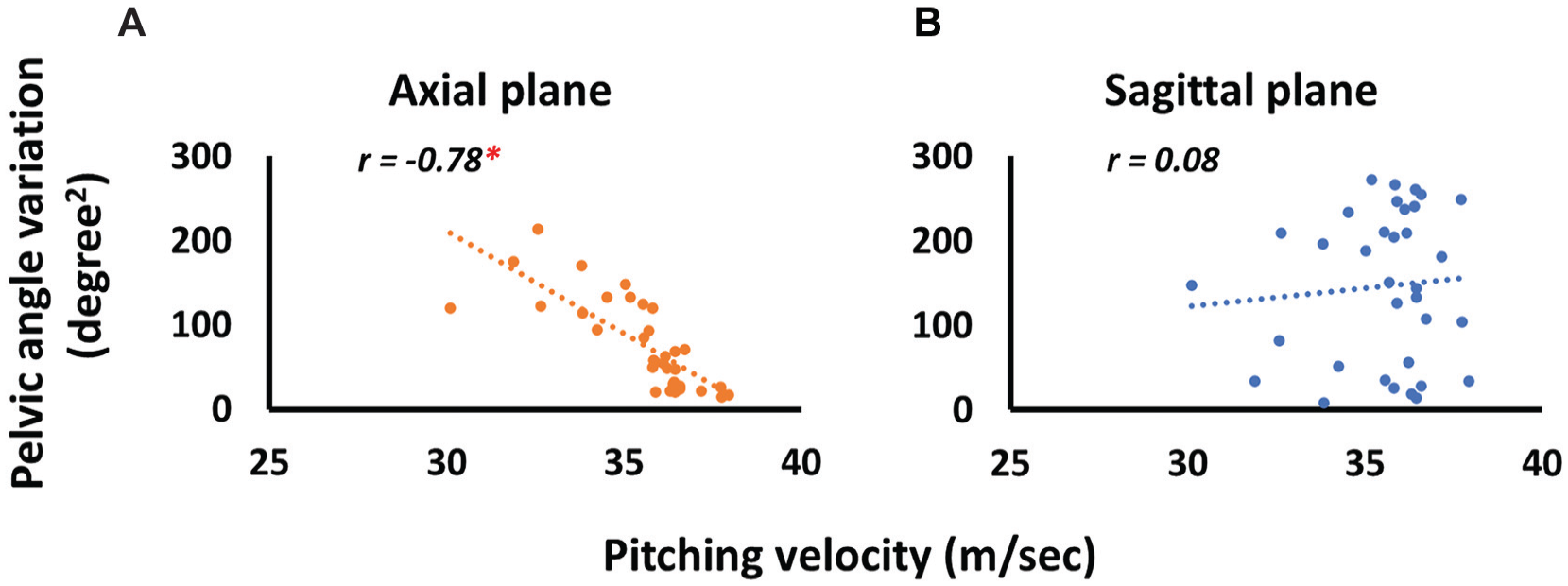
Correlation between pelvic angle variation in pitching movement and pitching velocity. (A) Axial plane. (B) Sagittal plane. * Statistically significant correlation, P < .0).
Pelvic-Trunk Coordination in Pitching Movement
The results showing the relationship between pelvic-trunk coordination and pitching velocity in the pitching motion are illustrated in Figure 6. From FC to MER, a significant positive high correlation was found for anti-phase (mean ± SD: 67.3% ± 23.8%) (r = 0.74, P < .01). From MER to MIR, in-phase coordination (mean ± SD: 51% ± 32.5 %) showed a positive moderate correlation with velocity (r = 0.58, P < .01).

Correlation between pelvic-trunk coordination in pitching movement and pitching velocity: (A) from FC to MER; (B) from MER to MIR. * Statistically significant correlation at P < .05. FC, foot contact; MER, maximal external rotation; MIR, maximal internal rotation.
Discussion
The purpose of this study was to explore the relationship between pelvic control, pelvic-trunk coordination, and pitching velocity in baseball pitchers. Our findings revealed a significant correlation between pelvic control in the axial plane of the drive leg and pitching velocity during the single-leg balance with movement test. Similarly, pelvic control in the axial plane on the stride leg also showed a significant correlation in the same test. In addition, a significant correlation was observed between pelvic control in the axial plane during the pitching motion and pitching velocity. Regarding pelvic-trunk coordination, a positive correlation was found for anti-phase coordination from FC to MER, and in-phase coordination also showed a positive correlation with velocity from MER to MIR.
This study demonstrated a significant correlation between pelvic angle deviation during a single-leg balance with movement test and pitching velocity, supporting pelvic angles as reliable indicators of pelvic control. 4 In the present study, pelvic control during single-leg stance on the stride leg was strongly associated with pitching velocity (r = −0.68, P < .01). Earlier research has shown that stride leg shear forces, reaching 0.72 body weight in the landing leg, facilitate energy transfer through the kinetic chain. 23 The pelvic control on the stride leg plays a critical role in power generation, which is essential for trunk rotation and the efficient transfer of energy, as demonstrated in youth pitchers. 27 These findings highlight the importance of pelvic control on the stride leg in optimizing performance and minimizing injury risk.
The findings of this study also underscore the critical role of pelvic control on the drive leg, which showed a significant correlation with pitching velocity (r = −0.65, P < .01) by enabling efficient kinetic energy transfer during the pitching motion. Previous research 18 has highlighted that reduced lumbopelvic control on the drive leg, observed during single-leg balance tests, has been associated with an increased risk of upper extremity injuries and diminished performance (deviation angle in the axial plane, P = .04). These findings emphasize the importance of targeted training programs aimed at enhancing drive leg pelvic control to optimize performance and reduce injury risks.
This study identified a significant association between stable pelvic control during pitching and higher pitching velocity (r = −0.78, P < .01). A stable pelvis plays a key role in minimizing energy dissipation along the kinetic chain,14,22 thereby reducing compensatory movements that place additional strain on the upper extremities. As shown in the previous study, 4 an impaired lumbopelvic control has been correlated with increased shoulder horizontal torque (r = 0.44, P = .003) and elbow valgus torque (r = 0.46, P = .002), both of which elevate the risk of injury. These findings highlight the pivotal role of pelvic control in optimizing force transfer, enhancing pitching velocity, and reducing the risk of injury.4,19,30 Consequently, implementing targeted interventions to improve lumbopelvic control could provide substantial benefits for baseball pitchers by enhancing performance and preventing injuries.
Our study shows that controlling the pelvis, especially in the axial plane during pitching, from FC to MIR, is associated with pitching velocity. Efficient energy transfer through the kinetic chain relies heavily on maintaining stable pelvic control. Research indicates that controlling the pelvic region is crucial for effective force transmission.1,4,20 Previous studies found that the gluteus medius muscle controls axial rotation movement of the hip, and its activity increases throughout the pitching motion. 26 This increase is expected as the body’s weight shifts from the drive leg to the stride leg after FC. 26 Therefore, our results suggest that after FC, controlling the pelvis in the axial plane is more important than in the sagittal plane. This indicates that pelvic control in the axial plane is important in determining pitching velocity.
Pitchers with a higher percentage of anti-phase coordination from FC to MER and a higher percentage of in-phase coordination from MER to MIR achieved better pitching velocity. Anti-phase coordination from FC to MER generates torsional force, storing energy, while in-phase coordination from MER to MIR releases this energy, accelerating the arm and ball. These findings align with research showing that effective pelvic-trunk rotations enhance pitching velocity, reduce upper limb stress, and predict elbow valgus torque, a key factor in performance and injury prevention. 11 Targeting these coordination patterns in training programs can optimize force transfer, enhance pitching velocity, and reduce injury risk by minimizing compensatory movements.
One limitation of this study is the variability within the sample, as participants included high school and collegiate pitchers, leading to differences in age and skill level. This diverse sample was chosen to capture a broader range of pitching mechanics and performance characteristics. However, the absence of a minimum velocity threshold may have introduced variability in the dataset, as pitchers with lower velocity might exhibit different movement patterns than those with higher velocity. This could have influenced the observed correlations by increasing data dispersion.
Our findings emphasize the critical role of pelvic control, particularly in the axial plane, where the gluteus medius is key. Prioritizing this in training can enhance performance and reduce injury risk. Pitchers with a higher percentage of anti-phase coordination from FC to MER and in-phase coordination from MER to MIR achieved better pitching velocity by efficiently storing and releasing energy to accelerate the arm and ball. Targeted exercises to strengthen pelvic-trunk coordination and improve pelvic control in the axial plane should be integrated into training and rehabilitation programs.
Conclusion
This study emphasizes the complex interaction between pelvic control and pelvic-trunk coordination in pitching velocity. By enhancing these factors, pitchers can improve velocity. Future research should further explore these coordination patterns and pelvic control strategies to provide more comprehensive guidelines for clinical practice and training.
Footnotes
Acknowledgements
The authors extend special thanks to the players who participated in this study.
Final revision submitted February 25, 2025; accepted March 10, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a grant from the National Science and Technology Council (NSTC 114-2425-H-028-004). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the National Taiwan University Hospital (NTUH-REC No. 202210101RIND).