
Abstract
Background:
Less experienced surgeons have an increased risk for tunnel malpositioning as a predominant risk factor for failure of anterior cruciate ligament reconstruction (ACLR). Fluoroscopic guidance can improve the precision of tunnel positioning.
Purpose:
To investigate whether low-volume surgeons can achieve precise femoral tunnel placement in ACLR under fluoroscopic control comparable to that of experienced mid- and high-volume surgeons.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study retrospectively included 150 patients who underwent primary ACLR between January 2021 and March 2023 and were prospectively enrolled in an in-clinic registry. Three groups were defined: high-volume surgeon (1 surgeon with >100 ACLRs per year; 50 images), mid-volume surgeon (1 surgeon with >10 to <50 ACLRs per year; 50 images), and low-volume surgeon (5 surgeons with ≤10 ACLRs per year; 50 images). The analysis of the femoral tunnel position was performed digitally on strictly lateral fluoroscopic images by determining the depth and height relations according to the quadrant method of Bernard and Hertel.
Results:
All surgeons, regardless of experience, achieved high precision of femoral tunnel placement (depth relation: SD, 3.41% [1.58 mm]; height relation: SD, 5.33% [1.33 mm]). The variances of the tunnel placements did not show significant differences between the 3 groups with the Brown-Forsythe test (depth relation: probability (Pr) > F = 0.332; height relation: Pr > F = 0.081; P < .05). The precision of the high-volume surgeon (depth relation: SD, 3.29%; height relation: SD, 4.92%) was comparable to that of the mid-volume surgeon (depth relation: SD, 2.98%; height relation: SD, 5.9%) and low-volume surgeon (depth relation: SD, 3.58%; height relation: SD, 4.62%).
Conclusion:
In this study, fluoroscopically guided tunnel placement allowed low-volume surgeons to achieve a level of precision comparable to that of the experienced surgeons. Fluoroscopy might especially help low-volume surgeons to achieve a standardized and highly reproducible femoral tunnel position and thus avoid tunnel malpositioning.
Keywords
Malpositioning of the femoral tunnel is one of the most common reasons for failure of anterior cruciate ligament reconstruction (ACLR).2,7,29,33,45 An ACLR failure with a recurrent anterior knee instability is accompanied by a worse functional outcome with long-term functional impairments and a delayed or absent return to work and preinjury level of sport.5,10,12,18,28,34,46 Anatomic landmarks, such as the anterior cruciate ligament (ACL) remnant, the anterior border of the femoral footprint, the lateral intercondylar ridge (“resident’s ridge”), or the lateral bifurcate ridge, as well as aiming devices are used to guide femoral tunnel placement.9,15,21,27,41,47,49 Bony landmarks alone can be difficult to differentiate and could lead to relevant malpositioning.26,38 Especially, less experienced surgeons have an increased risk for tunnel malpositioning.20,42
In clinical routine, there is often a trade-off between the desire to improve accuracy, practicality, and the time required to achieve it. For this reason, a fast, easy, and reliable method is necessary. Fluoroscopy-controlled ACLR as a visual method is an already introduced technique, although it is still not widely used. Studies found varying results regarding the use of fluoroscopic control for femoral tunnel placement.1,6,23,36,37,42,44
As early as 1988, in a cadaveric study, fluoroscopy-guided tunnel placement in ACLR was introduced. 11 In 1993, the advantage of using a fluoroscopic intensifier to verify tunnel positioning and angulation was technically described without assessing the accuracy of the method. 13 In a clinical study by Hughes et al 19 using fluoroscopy for tibial tunnel placement, repositioning the K-wire to optimize tunnel position was performed in 15% of the case. The authors concluded that intraoperative fluoroscopy could substantially enhance the precision of tunnel placement.
The purpose of this study was to investigate whether low-volume surgeons can achieve precise femoral tunnel placement under fluoroscopic control comparable to that of experienced mid- and high-volume surgeons. It was hypothesized that all surgeons, regardless of their experience level, would reach a high degree of precision in femoral tunnel placement under fluoroscopic control.
Methods
This study retrospectively included anonymized strictly lateral, intraoperative fluoroscopic images of knee joints with femoral condyle overlap, obtained from patients who underwent ACLR between January 2021 and March 2023 and were prospectively enrolled in an in-clinic registry for knee ligament injuries. The primary inclusion criterion was that the surgical procedure was conducted autonomously by the surgeon without guidance from a senior surgeon with a higher level of experience.
Second, 3 groups, depending on the experience of the surgeon, were defined:
- High-volume surgeon (>100 ACLRs per year)
- Mid-volume surgeon (>10 to <50 ACLRs per year)
- Low-volume surgeon (≤10 ACLRs per year)
Patients were excluded for lack of written informed consent for participation in the in-clinic registry, missing or inadequate intraoperative fluoroscopic imaging, or revision surgery or multiligamentous injuries.
Scans had to meet the following inclusion criteria:
- Strict lateral projection with a discrepancy <2 mm between the femoral condyles
- High-quality images for accurate differentiation of anatomic landmarks
- Closed growth plate
In total, 364 patients were primarily screened. Surgical procedures were carried out by either 1 high-volume surgeon, 1 mid-volume surgeon, or 1 of 5 low-volume surgeons. In total, 150 intraoperative, fluoroscopic pictures (50 images in each group) met the inclusion and exclusion criteria and were analyzed for this study.
The study design was approved by the local ethics committee, and informed consent was obtained from each patient participating in the study (PV7518, Aerztekammer Hamburg).
Surgical Technique
In all cases, hamstring or quadriceps grafts were used in an anteromedial portal technique as described previously. 8 Fluoroscopy-guided femoral tunnel positioning was performed as follows. Via a 6-mm offset aiming device (Arthrex Inc), a 2.4-mm guide wire was inserted into the center of the ACL near the footprint of the anteromedial bundle under arthroscopic visualization. The guide wire was drilled through the femur until the tip was flush with the corticalis, marking the intended femoral tunnel position. The position of the guide wire was checked visually and, if not placed in the intended region, repositioned under fluoroscopic control analogous to the method of Robinson et al 36 (mobile C-arm; Ziehm Imaging GmbH) in an anteroposterior and true lateral view with overlapping femur condyles (Figures 1 and 2).

Fluoroscopic image with true lateral view of a right knee with overlapping femur condyles and inserted K-wires marking the femoral (and tibial) tunnel. The star indicates the distal femur, the circle the proximal tibia, the triangle the patella, and the arrow the intended femoral tunnel position.

Example of a fluoroscopic intraoperative image with bad quality and no strict lateral view of a left knee, which should not be used for femoral tunnel position analysis and was excluded during this study. The star indicates the distal femur, the circle the proximal tibia, the triangle the patella, and the double arrow the >2-mm discrepancy between the femoral condyles.
Repositioning of Incorrectly Placed Guide Wires
For 1 surgeon, the number of guide wire repositions per surgery during femoral tunnel placement was documented.
Digital Analysis of the Femoral Tunnel Position
The femoral tunnel position was analyzed retrospectively on fluoroscopic imaging without influencing therapeutic interventions. The anonymized fluoroscopic images were digitally measured with the medical app ACL-X (Version 1.0.2 from May 21, 2020; Linova Software GmbH; available in the Apple App Store [https://Apps.apple.com/de/app/acl-x/id1439731734]), as described previously.17,32
For the digital quadrant analysis, based on the radiological landmarks defined in the original paper by Bernard and Hertel3,4 (line of Blumensaat, posterior and anterior condylar contour, distal tangent to the condyle), digital lines were positioned on the radiograph of the femoral condyle. The intended position of the femoral tunnel indicated by the tip of the K-wire was marked, and the relative position (in percentage) in the quadrant in the posterior-anterior direction along the line of Blumensaat, described by the depth relation, and the height orthogonal to the line of Blumensaat, described by the height relation, were analyzed by the app.
We used 3 further criteria for positioning the digital lines to enhance our measurements, in addition to those originally proposed by Bernard and Hertel3,4,32:
If the line of Blumensaat was broad, the red line was positioned centrally in the line of Blumensaat.
If line of Blumensaat was curved, the direction and shape of the line of Blumensaat were geometrically averaged.
The geometric center of condyle contours was marked if the condyles did not exactly overlap.
Absolute Size of the Femoral Condyle on the Lateral Radiograph
Based on previous results, the mean absolute femur condyle size (size of the Bernard and Hertel quadrant) was assumed to be 46.32 mm in the depth relation (distance of the ventral to dorsal condylar contour along the line of Blumensaat) and 24.8 mm in the height relation (distance between the line of Blumensaat and a tangent line parallel to the line of Blumensaat at the femoral condyle) (Figure 3). 32 Describing the absolute and not the relative femoral tunnel position in the quadrant, 1 mm corresponds to approximately 2% in the depth relation and 4% in the height relation.

Digital quadrant analysis based on the radiological landmarks defined by Bernard and Hertel. Digital lines are positioned on the radiograph of the femoral condyle. The red line indicates the line of Blumensaat, the blue line the anterior and posterior contours of the condyles, and the green line the distal tangent to the condyle parallel to the line of Blumensaat. Afterward, the tip of the K-wire indicating the intended tunnel position is marked and the analysis for depth relation and height relation is completed. Depth relation is the relative distance (percentage of total anterior-posterior distance) from the posterior condyle along a line parallel to the line of Blumensaat. Height relation is the relative distance (percentage of total condyle height) between the line of Blumensaat and a tangent parallel to the line of Blumensaat at the femoral condyle along an axis parallel to the blue lines.
Definition of the Precision of Tunnel Placement
The precision of the tunnel positioning was rated based on the calculated standard deviation in the depth relation and height relation as follows. The precision was graded as excellent if the SD in the depth relation was <3.3% (<1.5 mm) and the SD in the height relation was <6.0% (<1.5 mm). An SD between 3.3% and 4.3% in the depth relation (1.5-2 mm) and 6.0% and 8% (1.5-2 mm) in the height relation was rated as high. A moderate precision was defined as an SD between 4.3% and 5.4% (2.0-2.5 mm) in the depth relation and between 8% and 10% (2.0-2.5 mm) in the height relation.
Statistical Analysis
As part of the study design, a sample size analysis was conducted. According to already published studies on this topic, a mean difference of 2% in the depth relation and 4% in the height relation, as well a difference in the standard deviation between 2 surgeons of 0.5% in the depth relation and 1% in the height relation, was expected. With a significance level of α = .05, a medium effect size (Cohen d = 0.6), and a power of 0.8, 45 cases per group are required.
All data in this study are expressed as mean ± standard deviation. Normality of distribution of the samples was tested using the Shapiro-Wilk test. Variances of the 3 groups were compared using the Brown-Foresythe test and Levene test (P < .05). If the variances exhibited no significant differences, a single-factor analysis of variance (ANOVA) followed by a Tukey-Kramer post hoc test was performed.
All statistical analyses were performed using the SPSS statistical package (Version 20.0; IBM Corp) and RStudio (Version 1.2.1335; Posit).
Results
The mean femoral tunnel position of all included patients was 28.22% in the depth relation and 17.72% in the height relation. The mean range between the 3 groups was 2.3% (1.07 mm) in the depth relation and 3.2% (0.79 mm) in the height relation (Table 1).
Overview of the Obtained Measurements a

Data are presented as mean ± SD.
The variances of the tunnel positions did not show significant differences between the 3 groups (Table 2). All groups achieved high precision with an overall standard deviation of tunnel placement of approximately 1.5 mm. The overall SD in the depth relation was 3.41% (1.58 mm), and that in the height relation was 5.33% (1.33 mm). The precisions of the high-volume surgeon (depth relation: SD, 3.29%; height relation: SD, 4.92%) and mid-volume surgeon (depth relation: SD, 2.98%; height relation: SD, 5.9%) were excellent in the depth relation and height relation. The low-volume surgeon had a high precision in the depth relation and an excellent precision in the height relation (depth relation: SD, 3.58%; height relation: SD, 4.62%) (Table 1).
Analysis of Variance a

Data are presented as P values. Bold P values indicate statistical significance (P < .05). ANOVA, analysis of variance.
The single-factor ANOVA showed a significant difference in the means (depth relation: P = .003, height relation: P = .005) among the 3 groups. The Tukey-Kramer post hoc test revealed a significant difference in the means of the depth relation and height relation (depth relation: P = .002, depth relation: P = .007) between the high-volume and mid-volume surgeons and a significant difference in the height relation (P = .028) between the mid-volume and low-volume surgeons. No significant difference in the means was found between the high-volume and low-volume surgeons (Table 2).
Figure 4 visualizes the differences in the obtained femoral tunnel positions with a substantial degree of congruence in the comparison between the 3 groups.
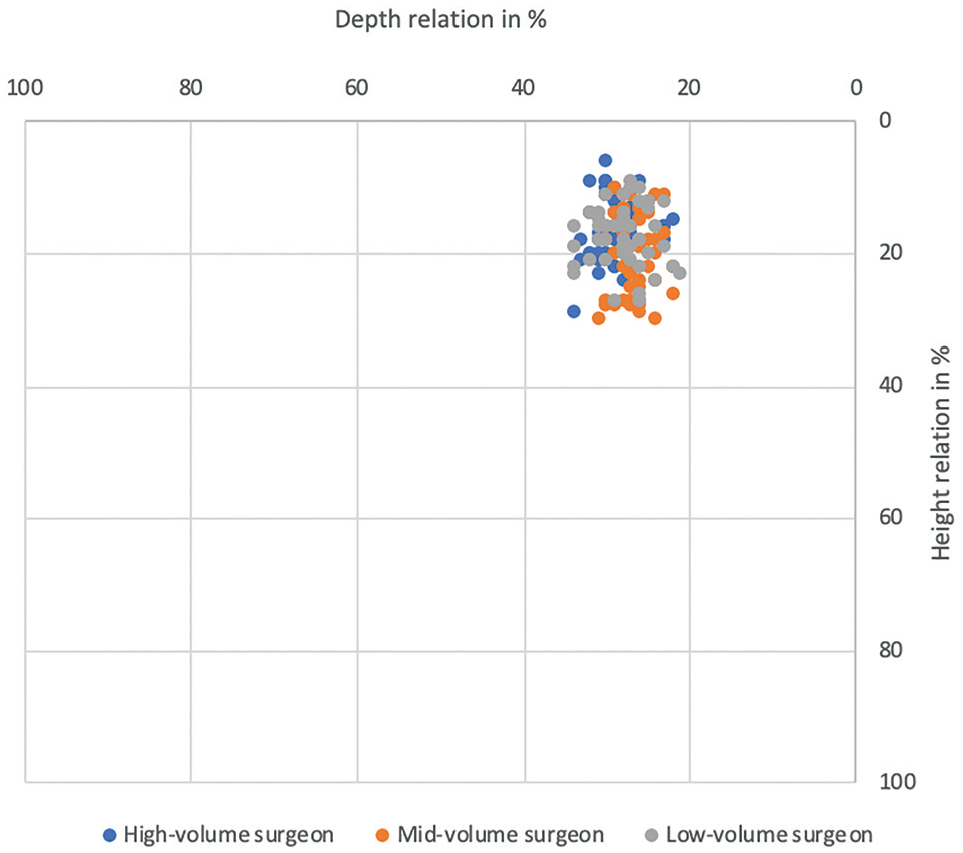
Achieved femoral tunnel positions of the 3 groups. Blue represents a high-volume surgeon, orange a mid-volume surgeon, and gray a low-volume surgeon.
The number of femoral guide wire repositions was recorded by the mid-volume surgeon in 50 cases. In 28 surgeries, at least 1 repositioning was performed. The mean number of femoral guide wire repositions for the mid-volume surgeon was 0.72 times per surgery.
Discussion
The most important finding of this study was that the fluoroscopy-controlled tunnel placement results in high precision of femoral tunnel positioning, regardless of the surgeon’s experience.
The variance between femoral tunnel positions was comparably small for low-volume surgeons and medium- and high-volume surgeons and was within a range of approximately 1.5 mm. The respective mean values of the tunnel position in the depth relation and height relation were individually different for each of the 3 groups of surgeons, with a statistically significant difference between the high-volume surgeon and the mid-volume surgeon. Expressed in absolute distances, however, this deviation was <1.1 mm. All surgeons positioned the femoral tunnel in the anteromedial insertion area of the femoral ACL footprint, so the different tunnel positions with a deviation of <1.1 mm are unlikely to be clinically relevant. To the best of our knowledge, the precision of fluoroscopy-controlled femoral tunnel positioning of surgeons with different experience levels has not been investigated yet.
Consistent with the results of this study, Moloney et al 31 observed a significant improvement in femoral and tibial tunnel placement in a cadaveric study using a fluoroscopic overlay system. These results have been clinically confirmed in a single-surgeon study comparing conventional tunnel placement with fluoroscopy-guided tunnel placement, where more accurate femoral tunnel placement was achieved using fluoroscopy. 23 Based on the research of Shafizadeh et al, 40 a mean accuracy of about 1 mm in an experimental setting should be possible. More complex fluoroscopy-based and fluoroscopy-free navigation systems could also increase accuracy in anterior-posterior femoral tunnel placement.16,24,35,48 In this study, fluoroscopy-guided tunnel placement achieved a comparable level of accuracy to fluoroscopy-assisted navigation or fluoroscopy-free navigation, but with significantly less technical effort.
In the present study, each surgeon had an individual, intended femoral tunnel position, and it appears that fluoroscopy can minimize the variation around this individual position. Thus, fluoroscopy can improve the reproducibility of tunnel placement. This is supported by the findings of Seo et al, 37 who noted that the significant improvement with fluoroscopic guidance may not be in the exact tunnel position, but rather in the variability of tunnel placement. Klos et al 25 found a significant reduction in the standard deviation of femoral tunnel (nonassisted: 9%; fluoroscopy: 5%; fluoroscopy + computer navigation: 3%) and tibial tunnel (nonassisted: 6%; fluoroscopy: 4%; fluoroscopy + computer navigation: 3%) positioning when fluoroscopy was used.
In the present study, the attained mean tunnel positions of all groups differed <1.1 mm in the depth relation and height relation. This observation aligns with previously published results (variability approximately 1 mm), in which it was hypothesized that this level of variability would not exert a significant clinical effect. 39 Fluoroscopic control can be a technically simple way of achieving greater accuracy in ACL tunnel positioning, especially for less experienced surgeons.
In a controlled laboratory study conducted by a large international group of experienced ACL surgeons, Robinson et al 36 showed that the deviation between intended and achieved femoral tunnel positions, as well as the spread of the tunnel positions, was lowest with the fluoroscopy-assisted technique compared with conventional techniques. Experienced surgeons achieved variations in the depth relation and height relation of 6.7% and 13.7%, respectively, with a purely visual technique. With an offset aiming device, the variations in the depth relation and height relation were 6.4% and 12.7%, and with a ruler 4.8% and 6.8%, respectively. 36 In this study, less experienced low-volume surgeons achieved less variation in tunnel positions (depth relation: SD, 3.6%; height relation: SD, 4.6%) using fluoroscopic assistance than experienced surgeons in the study by Robinson et al 36 (all techniques: depth relation: mean SD, 6.3%; height relation: mean SD, 12%).
Femoral tunnel positions were retrospectively assessed using the digital quadrant method with the ACL-X smartphone application, which was introduced by Hoeher et al, 17 who described the intraoperative use of the app. The reliability of the digital quadrant method was demonstrated recently. 32 The benefits of an intraoperative use of the ACL-X app need to be clarified by further research.
Hughes et al 20 showed that tunnel location differs depending on the experience of the surgeon, resulting in more anterior femoral tunnel placements of inexperienced surgeons. Surgeons with lower surgical case numbers often face greater challenges related to technical issues, resulting in extended operating times and a higher incidence of complications.14,30 Especially for less experienced surgeons, fluoroscopic control of the tunnel placement is a simple tool to increase their precision. The intraoperative feedback has the potential to enhance the learning curve for novice knee surgeons or in the case of revision surgery. 22 In this study, the intraoperative fluoroscopic control of the tunnel positions led to a correction in 56% of cases by the mid-volume surgeon. In other studies, reposition rates to improve the tunnel placement in 11% to 40% of the cases were reported.19,37,42,44 Intraoperative monitoring of fluoroscopic images with the ACL-X app could additionally provide helpful, intraoperative, objective feedback, especially for less experienced and low-volume surgeons.
Limitations
The analysis of tunnel positioning was conducted by a single observer, potentially introducing a systematic error in the retrospective evaluation of tunnel position. Earlier published studies have reported a strong inter- and intraobserver reliability when using the quadrant method, so no great influence on the measurements is expected.39,43 The comparison among the 3 groups would remain unaffected regardless of a potential systematic error.
One surgeon in each of the high- and mid-volume groups might not fully represent the different experience levels. Furthermore, the frequency of correction of the tunnel placement after fluoroscopic control was only recorded for the mid-volume surgeon. It can be expected that the incidence of malpositions depends to some degree on the surgeon’s experience. Nevertheless, the results show the importance of an intraoperative control to prevent relevant misplacement even for an already experienced surgeon.
In addition, there was no investigation into how the tunnel placement was improved after misplacement or the extent of such corrections. The focus of this study was to compare the reproducibility of femoral tunnel positioning among different surgeons, necessitating analysis of the final fluoroscopic images. The correction process itself could be evaluated in further studies focusing on the surgical technique and strategy.
The effect on the learning curve was not assessed in this study. However, it can be expected that instant, objective control of the tunnel position as direct feedback facilitates rapid adjustments of the surgical technique to improve the quality of care and thus individual learning curves.
Conclusion
In this study, fluoroscopically guided tunnel placement allowed low-volume surgeons to achieve a level of precision comparable to that of experienced surgeons. Fluoroscopy might especially help low-volume surgeons to achieve a standardized and highly reproducible femoral tunnel position and thus avoid tunnel malpositioning.
Footnotes
Acknowledgements
The authors thank Birgitt Kowald for advice on experimental design and statistical analysis.
Final revision submitted October 23, 2024; accepted November 20, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Financial support for measurement costs was provided by Zukunft Sporttrauma–Verein zur Forderung und Weiterbildung in der Sporttraumatologie e.V. J.H. is the originator/copyright holder of the ACL-X app and receives financial benefits from user fees (Apple App Store). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Arztekammer Hamburg (2020-10259-BO-ff).