
Abstract
Background:
Ice hockey players experience groin pain and imbalances in the muscles of the hip joint, possibly because of the condition of the intercartilage space (ICS).
Purpose:
To describe the lateral differences in size of the articular ICS, range of motion, and adductor/abductor muscle strength between elite and subelite ice hockey players and a control group of participants who did not play ice hockey.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
33 elite hockey players, 26 subelite hockey players, and 30 non–ice hockey player controls were compared in terms of ICS thickness, isometric hip abductor muscle strength, hip range of motion, functional test results, and pain score. Two-way analysis of variance was used to identify differences in laterality and performance levels.
Results:
The ICS of the hip joint was smaller (P < .001) in both groups of ice hockey players than in the control group (0.97 ± 0.11 mm) and smaller (P = .005) on the backhand side (elite 0.66 ± 0.24 mm; subelite 0.65 ± 0.15 mm) than on the forehand side (elite 0.78 ± 0.18 mm; subelite 0.74 ± 0.24 mm) in both groups of hockey players. Compared with the control (41.6°± 4°) and subelite groups, the elite group had less (P < .001) hip external rotation (elite 30.4°± 6.1°; subelite 35°± 6.5°) and internal rotation (elite 31.5°± 5.1°; subelite 35.1°± 6.5°), with no differences in laterality (P > .05). Both hockey groups had positive hip pain provocation tests and greater (P < .001) hip adduction (elite 457 ± 85 N; subelite 450 ± 82 N) and abduction (elite 429 ± 60 N; subelite 422 ± 63 N) muscle strength than the controls (adduction 347 ± 70 N; abduction 346 ± 75 N). Elite players had a greater (P = .008) adductor strength ratio on the backhand side (1.16 ± 19) than the control group (1.02 ± 0.15).
Conclusion:
Ice hockey players had a smaller ICS of the hip joint, particularly on the backhand side. These structural changes were accompanied by reduced range of motion in the hip joint, increased pain, and asymmetries in muscle strength. Hip range of motion and symmetry of adductor/abductor muscle strength should be considered when diagnosing ice hockey players. ICS assessment via sonography might become a useful tool for the evaluation of structural changes in the hip. Research on ice hockey–related injuries should focus more on the structural and functional condition of the backhand side of the hip.
Unilateral sports like tennis, cricket, golf, and ice hockey are associated with health complications because of long-term bilateral functional and structural differences in the musculoskeletal system.18,20,38 These complications include hip joint osteoarthritis, low back pain, groin injuries, and femoroacetabular impingement, all of which can be prevented with proper compensation during athlete training.9,28,44 Ice hockey is a typical unilateral sport, in which the use of skates and specific skating techniques in addition to a high volume of training, frequent match loads, and frequent changes in direction overload the hip joint,5,13,34 potentially causing changes in its structural and kinesiological qualities.
A significant issue with skating is the fact that solid skates are used at the elite and subelite levels.6,45 Because solid skates reduce ankle movement, greater propulsion from the knee and hip is required.6,33,37 Elite players exhibit greater knee extension, hip flexion, and external rotation range of motion (ROM) than do subelite players during acceleration, sprints, and steady skating. 5 Skating with solid skates increases the load on lower limbs, possibly resulting in adductor muscle strain,22,46 pubic bone edema,15,21 and/or intra-articular injuries such as femoroacetabular impingement, 42 labral injury, and osteoarthritis.2,12,16,32 Lower extremity loading during ice hockey has been shown to decrease hip rotation by 14° to 23° as well as reduce hip adductor strength by 4.6 to 8.6 kg, 43 which may cause structural changes21,43 and groin pain.11,27
Osteoarthritis is a common structural change in the hip, and the development and severity of osteoarthritis are determined on the basis of the condition of the intercartilage space (ICS). 17 The ICS of the hip joint is the gap between the articular cartilage of the femoral head and the acetabulum, where structural changes such as thinning of the articular cartilage and narrowing of the articular ICS may occur, 8 resulting in intra-articular lesions. 26 Moreover, the ICS does not narrow with age and is reported to be present in an asymmetric lateral fashion in 5.9% of individuals on average. 25 Although researchers in a previous study of ICS reported a minimum value for the ICS, they also reported high intraindividual variations and the need for further research. 25 Despite the findings mentioned above, we could not find a study describing the relationship between lower extremity loading during hockey and the articular cartilage status or ICS measurement of the hip joint in hockey players.
In ice hockey players, groin pain is associated with injuries to the hip joint, strength of the hip adductors/abductors, and external/internal rotation of the hip joint and might be related to performance level and absolute or lateral differences in the size of the ICS of the hip joint.3,4,31 Therefore, the aim of this study is to describe the lateral differences in the size of the articular ICS, ROM, and adductor/abductor muscle strength between elite and subelite ice hockey players and a control group of participants who did not play ice hockey. We hypothesized that elite ice hockey players would have a smaller ICS, greater differences in lateral ICS, greater hip adductor/abductor muscle strength, less ROM of the hip joint, and worse functional test results compared with subelite ice hockey players and non–ice hockey player controls.
Methods
Study Design
The participants were sorted into 3 groups. The elite group consisted of players participating in the first Czech ice hockey league, and the inclusion criteria were at least 2 previous seasons with >30 games in the first Czech league or international equivalent and full participation in an ongoing seasonal training program (5 on-ice trainings and 3 matches per week).
The subelite group consisted of members of the Czech varsity hockey team who trained 4 times per week and played 1 game per week. The control group consisted of non–ice hockey athletes who played football, volleyball, or basketball <4 times a week (Table 1).
Basic Anthropometric Characteristics of the Participants a

Data are presented as mean ± SD. ANOVA, analysis of variance.
The cross-sectional measurements started with medical history, laterality, and a pain questionnaire, and measurements included bilateral conditions of the ICS, ROM of the hip joint, the results of functional tests, and the isometric strength of the hip adductors/abductors (Figures 1 and 2). Participants first underwent a sonographic examination (USG) of the hip joint, a goniometric examination of the hip joint ROM, and functional tests. The functional tests included the hip flexion–adduction–internal rotation test (FADDIR) and the hip flexion–abduction–external rotation (FABER, Patrick) test.10,48 The participants were subsequently asked to perform 4 exercises to warm up, activate, and stretch the hip rotators, adductors, and abductors before the dynamometer was used to measure hip adductor and abductor strength14,47 (Figure 2, J-N). A laterality questionnaire was used to identify the forehand and backhand sides of the groups of hockey players. In the control group, the laterality of the lower limb was determined by the preferred kicking leg.
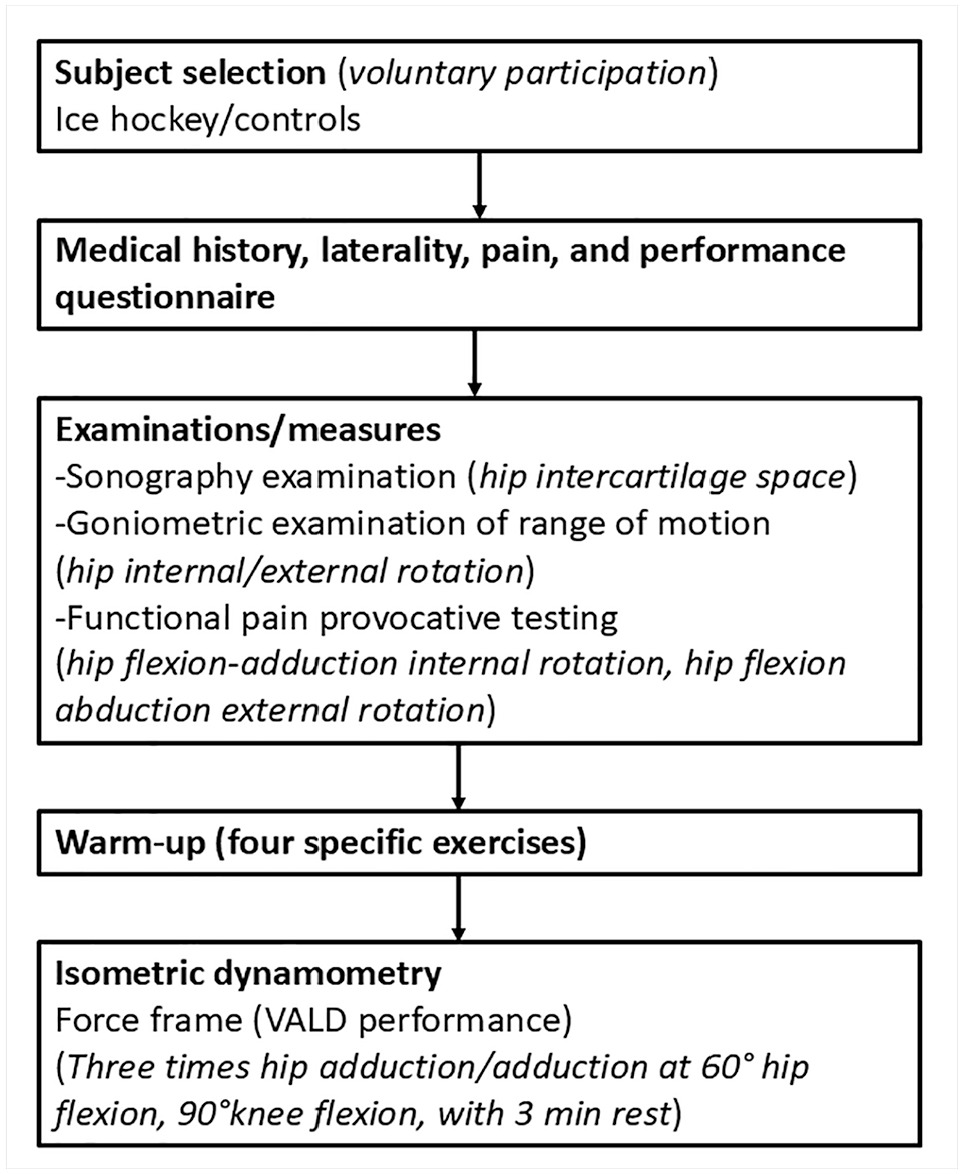
Flow chart of procedures during the structural and functional evaluation of the ice hockey and control hip. The photo shows the participant and probe during sonographic examination of the intercartilage space of the hip. Specific exercises were performed to warm up the hip joint before hip adduction/abduction strength measurement. (A) Lateral motion into internal and external rotation in the standing position. (B) Transitioning from hip external rotation to the lunge. (C) Sideways steps with TheraBand around the knees. (D) Gym ball squeeze by the knees.

The procedure during the structural and functional evaluation of the hip. (A) Probe position during measurement of intercartilage space (ICS). (B) Body position and rotation change during external rotation of the hip. (C) Body position and rotation change during internal rotation of the hip. (D-F) Body positions of participant and tester during hip flexion–adduction–external rotation test. (G-I) Body positions of participant and tester during hip flexion, adduction, internal rotation test. (J) Circular motion into internal and external rotations in the standing position. (K) Standing, passive external rotation of the hip joint with support of the tibia on the femur and subsequent transition to the lunge position and bilateral stance. (L) Sideways steps in the quarter-square position with a TheraBand around the knee joints. (M) Squeezing a gym ball while in the supine position with the hips and knees angled at 80°. (N) Body position during isometric hip adduction/abduction test (supine position, with 60° of hip flexion and 90° of knee flexion). ROM, range of motion.
This observational experiment was approved by the regional institutional committee at Charles University Faculty of Physical Education and Sport (No. 115/22) and was registered as a controlled trial involving humans in the database of Clinical Trials.gov in the National Library of Medicine (No. NTC05788419). Informed consent was obtained from all participants, and the rights of the subjects were protected.
Participants
All participants were free of current injury, and the ice hockey players were tested at least 24 hours after the last ice hockey game of the season. The participants were randomly assigned to a testing schedule, and each test was performed by 1 physical therapist familiar with all the testing procedures. The physical therapy testing was performed by the same experienced therapist with certified professional competence to work without supervision and who was blinded to the participant's group allocation. The study population was diverse and not artificially manipulated. Only data related to the experiments were collected and used for the analysis.
Sonographic and Range of Motion Procedure
USG examination of the anterior area of the ICS of the hip was performed with an Alpinion E-CUBE i7 device (Alpinion Medical System), in which the probe settings were as follows: resolution 12 MHz, depth 4 cm, and focus 1.5 cm. The probe was positioned vertically to the medioclavicular line 27 by a therapist who was trained in musculoskeletal ultrasound and was blinded to the participant's group allocation (Figure 2A).
The participants were positioned supine, with the hip flexed and externally rotated 45°, knee flexed 120°, and foot resting on the inner surface of the contralateral knee joint (Figure 2A). The examined lower limb was supported below the knee joint by a bolster of approximately 20 cm. The monitored parameter was the vertical height of the ICS between the 2 edges of the articular cartilage at the level of the medial-clavicular plane in millimeters. The highest ICS value from 3 consecutive measurements was recorded (to eliminate measurement error).
The goniometric examination of ROM was performed using an international sagittal-frontal-transversal-rotational goniometer in the standardized sitting position.1,30 The examined lower limb was in a sitting position at the hip and knee joint flexed in 90°. Passive external rotation (Figure 2B) and then passive internal rotation (Figure 2C) of the hip joint were measured in degrees and recorded on the datasheet. The bilateral hips and lower extremities were measured in all participants (Figure 2).
Functional Test
The FABER test and the FADDIR test were conducted, and hip adduction/abduction strength was assessed. The FABER test was selected because of its suitability for identifying a lesion of the hip joint, 41 and the result was evaluated as positive (value of 1) or negative (value of 0). Tests were performed with the patient positioned supine with the hip in flexion, external rotation, and abduction, and pressure was applied in with the hip in abduction (Figure 2, D-F).
The FADDIR test was selected because it is a provocation maneuver for femoroacetabular impingement and anterior labral rupture, 35 and the result was evaluated as positive (value of 1) or negative (value of 0). The FADDIR test was performed with the patient in the supine position with the hip in flexion, adduction, and internal rotation, and an expression of pain in the final position indicated test positivity 7 (Figure 2, G-I). The positivity of both tests was noted as a sign of joint dysfunction.
Specific exercises for hip warm-up and ROM were used before isometric dynamometry, which determined the strength of the hip adductors/abductors. The warm-up started with 8 repetitions of circular motion into internal and external rotations in the standing position (Figure 2J). This rotation was followed by standing, passive external rotation of the hip joint with support of the tibia on the femur and subsequent transition to the lunge position and bilateral stance (Figure 2K). This transfer to the lunge was performed 5 times on each side. The next exercise involved sideways steps in the quarter-square position with a TheraBand around the knee joints (Figure 2L). The participants performed 4 sideways lunge movements to each side, and this process was repeated 3 times. The last warm-up exercise involved squeezing a gym ball while in the supine position with the hips and knees angled at 80°. The participants squeezed the gym ball between their knees 6 times in 3 sets (Figure 2M).
Isometric adductor and abductor muscle strengths were measured using the ForceFrame (VALD Performance). Measurements were performed in the supine position, with 60° of hip flexion and 90° of knee flexion14,47 (Figure 2N). Three tests with 3 minutes of rest were performed to measure adductor and abductor muscle strength, and the values were recorded by VALD software in newtons. The best measurement from each set was selected to represent the current muscle strength of the abductors and abductors of the hip joint.
Statistical Analyses
The normality of the data was checked using the Kolmogorov-Smirnov test, and the Pearson correlation coefficient was used to assess the relationships between the measured parameters. One-way analysis of variance (ANOVA) was used to compare the potential differences between the experimental groups via basic anthropometry. Two-way ANOVA was used to compare the differences in laterality between the experimental groups (Measured Value × Group × Forehand/Backhand Side), and both analyses were followed by Bonferroni post hoc correction. One-way ANOVA followed by Bonferroni post hoc correction was used for data describing the differences in laterality or ratios (Measured Value × Group). The effect size in ANOVA was described as a partial eta square, and 0.02, 0.13, and 0.26 were reported as small, moderate, and large effects, respectively. A total of 78 participants were required for an effect size of 0.36 and a power of 0.80 according to G-power software (G-power 3.1.9.4).
The Kruskal-Wallis test was used across all groups and for pair values to compare differences between groups and laterality in the cases of scale values from the FADDIR and Patrick tests.
Pearson correlation was used to describe the relationships between the ICS and all other parameters, and stepwise regression based on the ICS correlation was used to determine the model for ICS prediction. This analysis was performed separately for each group. Statistical significance was set at P < .05 for all analyses.
Results
A total of 89 participants, representing 3 specific groups of athletes, volunteered for measurements. None of the participants had any acute or chronic injuries, had medical prescriptions for pain, or were undergoing treatment for joint pain management, which were exclusion criteria. All participants were between 18 and 30 years of age (Table 1).
All of the data were normally distributed (Table 2; see the supplemental material, available online), with particular group and laterality differences. The group comparison revealed no significant differences in participant age, height, weight, or body mass index (Table 1). The ANOVA revealed differences between the hip ICS (F2,172 = 41.8; P < .001; η2 = 0.32) and the playing side (F1,172 = 8.1; P = .005; η2 = 0.05), and the post hoc test revealed that the hip ICS was smaller in both groups of ice hockey players than in the controls and that the hip ICS was smaller on the backhand side than on the forehand side in both hockey player groups (Figure 3). Lateral differences in the ICS were found (F2,86 = 6.3; P = .003), and the elite group had a greater reported difference than did the controls.
Descriptive Values of Structural and Functional Measures of Ice Hockey and Control Hips a
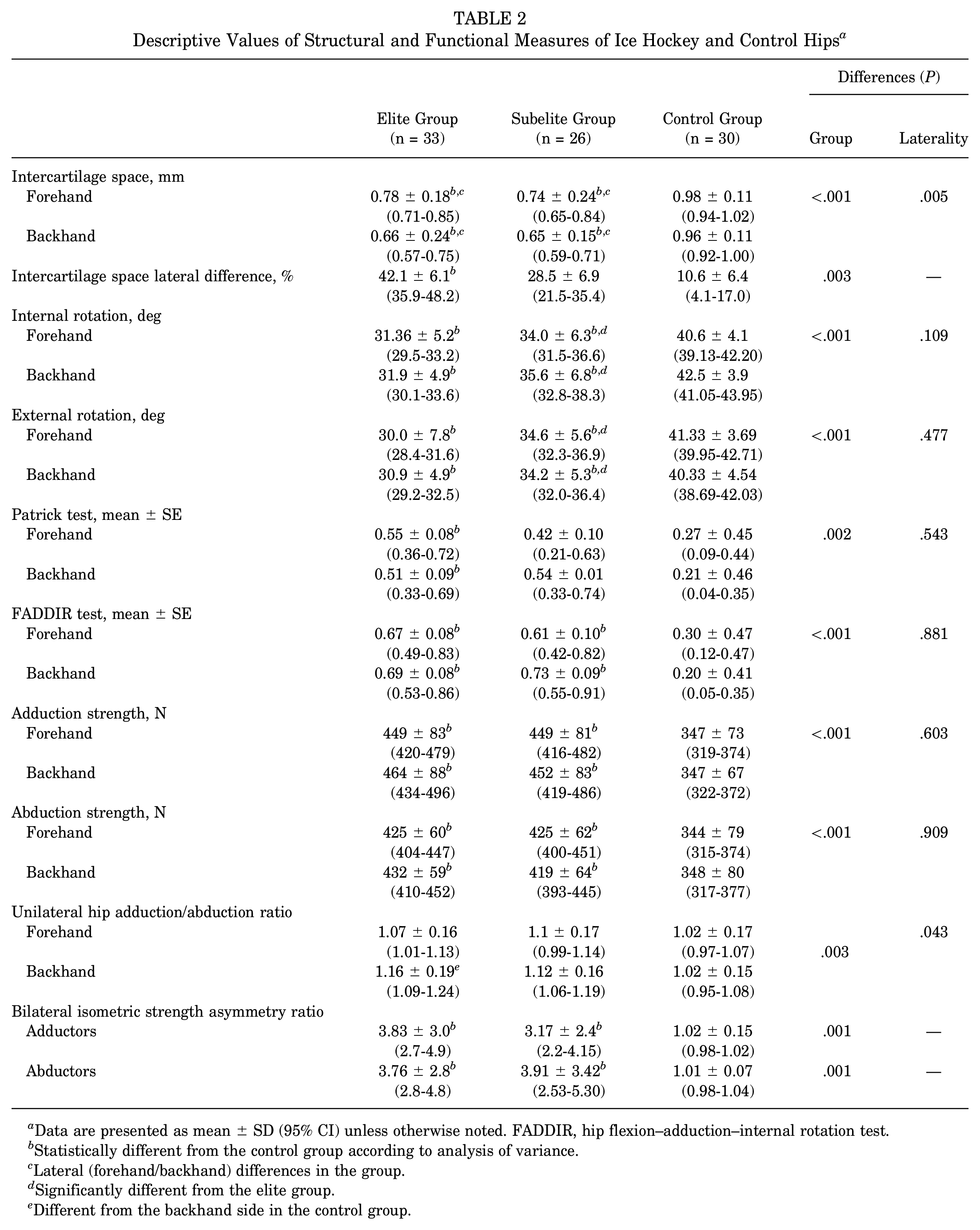
Data are presented as mean ± SD (95% CI) unless otherwise noted. FADDIR, hip flexion–adduction–internal rotation test.
Statistically different from the control group according to analysis of variance.
Lateral (forehand/backhand) differences in the group.
Significantly different from the elite group.
Different from the backhand side in the control group.

Differences in the hip intercartilage space on the playing side between elite and subelite hockey players and controls. *Statistically different from the control group according to analysis of variance. ‡Lateral (forehand/backhand) differences in the ice hockey groups.
Hip joint external rotation differed among all of the study groups (F2,172 = 76; P < .001; η2= 0.47), and post hoc tests revealed that the subelite group had less hip external rotation than the control group and that the elite group had less hip external rotation than the control and subelite groups, with no lateral differences (P = .477) (Figure 4).

Differences in hip internal/external rotation, passive range of motion, and pain provocation tests between elite and subelite hockey players and controls. FADDIR, hip flexion–adduction–internal rotation test. *Significantly different from the control group. †Significantly different from the elite ice hockey group.
Internal rotation of the hip joint differed among the study groups (F2,174 = 77.0; P < .001; η2= 0.47), and post hoc tests revealed that the subelite group had less internal rotation of the hip joint than did the control group and that the elite group had less internal rotation of the hip joint than the control and subelite groups, with no lateral differences (P = .109) (Figure 4).
The results of the FADDIR test differed between the control group and the elite ice hockey group (H2,178 = 29; P < .001), and multiple comparisons revealed that the elite hockey group had a higher score than the control group, with no lateral differences and no differences from the subelite group (P = .881) (Figure 4).
The results of the Patrick test differed between the control group and the elite ice hockey group (H2,178 = 12.6; P = .002), and multiple comparisons revealed that both hockey groups had higher scores than the control group, with no lateral differences (P = .543) (Figure 4).
Hip joint strength differed between adduction (F2,172 = 36.6; P < .001; η2 = 0.23) and abduction (F2,172 = 27.6; P < .001; η2 = 0.21), and elite and subelite players had greater isometric strength than the control group, with no differences between the forehand and backhand sides in any group (P > .05) (Figure 5).

Differences in hip adductor and abductor isometric strength, unilateral strength ratios, and bilateral symmetry between the elite and subelite ice hockey player groups and the control group. *Significantly different from the control group. †Significantly different from the control group on the backhand side.
The unilateral hip adduction/abduction ratio differed between the groups (F2,172 = 5.8; P = .003; η2 = 0.06) and in terms of laterality (F2,172 = 4.1; P = .043; η2 = 0.02), and the post hoc test revealed a greater adductor strength ratio in elite players on the backhand side than on the backhand side in the control group (Figure 5).
The bilateral hip joint strength ratio differed between adduction (F2,86 = 24.3; P < .001; η2 = 0.21) and abduction (F2,86 = 24.5; P < .001; η2 = 0.20), and both elite and subelite players presented greater percentage differences than did the control group, with no differences between adduction and abduction (Figure 5).
The Spearman correlation was used to assess the relationships between age and the ICS in the elite group (r = 0.32) of ice hockey players. The ICS in the subelite group was correlated with hip external rotation (r = 0.29) and hip abduction strength (r = −0.27), and the ICS in the control group and FADDIR test results were related (r = 0.43). No other correlations were significant. The regression model revealed that the ICS in the elite group was affected by player age, FADDIR test result, and hip abduction and adduction strength (R2 = 0.27; age b = 0.285; FADIR b = 0.270; adduction strength b = 0.558; abduction strength b = −0.62; unilateral hip adduction/abduction ratio b = −0.53; bilateral adduction/abduction asymmetry b = −0.11).
The ICS in the subelite group was determined (R2 = 0.23) by ROM, Patrick test result, abductor strength (Patrick test b = −0.26; external rotation b = 0.220; hip abduction strength b = −0.28), and bilateral adduction/abduction asymmetry (b = −0.16).
The ICS of the control group was determined using the FADDIR test result and ROM (FADDIR backhand side b* = −0.42; hip internal rotation b = −0.16; hip external rotation b* = 0.104).
Discussion
The major findings of our study demonstrate that compared with the control group, both ice hockey player groups had smaller ICS and poorer functional test results. This underlines previous findings that ice hockey causes functional changes in the hip joint 43 and confirms that those changes have a structural effect on the ICS. Moreover, the finding that the backhand side of the ICS was more affected than the forehand side confirmed that laterality is important for ice hockey players in the long term, as well as balancing the ROM 43 and bilateral and unilateral adductor and abductor strength. 40
Our ICS values were lower than those reported in a previous study (3.61 mm superomedial, 4.82 mm superolateral) 25 across all groups. This might be explained by considerable variation in the size and width of the hip joint and inconsistent validation of the measurement of the hip joint width using sonography across different studies.8,19,25 In our study, we evaluated the size of the ICS, as it was imaged from the ventral approach in the clearly defined FABER test position with the knee supported and the linear transducer positioned vertically. Our low ICS value is consistent with that reported in previous studies as well as the fact that the articular cleft is highly variable 19 and has a width <2 mm. Although we did not find a significant difference in the ICS between elite and subelite players, we noted a large difference between the controls and the patients with ICS laterality. All of our groups had larger lateral differences than the 5.9% reported previously, 25 and this difference was highest in elite players (≈42%). This finding indicates that our ICS values could still differentiate between patients with laterality and control participants. Typically, the ICS does not change with age, which was confirmed in our subelite and control groups. However, we found that the ICS in the elite group decreased with age, 26 which indicates that for ice hockey players, loading might be the cause of this effect because of long-term postural loading in specific ice hockey postures. Thus, our study revealed that in elite players, the size of the ICS is decreased (especially on the backhand side), lateral asymmetry is increased, and the condition of the ICS worsens over time, which is related to playing time.
The ROM has been associated with ice hockey skating speed,5,37 hip groin injuries, 23 femoral-acetabular shape, 24 and structural changes in the ICS. Our data revealed greater hip internal rotation than that reported in a previous study (26.1°± 6.6°) and less hip external rotation (44.2°± 8.6°). 24 These changes can be explained by a variable ROM due to the loading volume during the season, because loading for 1 day can alter the ROM of the hip by 7.32°. 43 This might also explain the difference in lower hip ROM between subelite and elite players, who had trained more often and had higher match loading during the season. Compared with subelite players, elite players exhibit less hip ROM, which is consistent with function during skating; however, elite players exhibit greater knee and hip flexion/extension and greater hip abduction.7,36,37 This might be explained by possible differences between passive and active ranges of motion, where higher forces acting during more powerful skating might allow a greater hip ROM. Moreover, hip strength at specific skating angles ranging from 25° to 50° combined with power can be strongly related to skating acceleration and change of directional speed performance.39,40
As expected, hip abductors and adductors were stronger in ice hockey players than in controls, and this result was highly significant (P < .001) (Table 2). The functional need is the same for abductors and adductors, and loading during ice hockey causes hip adductor exhaustion (reported −4.41 kg decrease for 24 hours). 43 This training exhaustion causes hip adductor strengthening, which manifests as an increased hip adduction/abduction ratio in elite players. Therefore, elite players should balance unilateral adductor/abductor strength on the backhand side. In contrast to the lateral ICS differences between performance levels, the lateral differences between the adductors and abductors did not differ between the ice hockey groups and were still within the 10% difference limit recommended for injury prevention 29 and were >0.8, which is a borderline indication of injury prediction. 46 Our study revealed a unilateral adduction/abduction ratio between 1.06 and 1.14, whereas a previous study revealed a ratio between 1.00 and 1.53, depending on the measured hip abduction position. 40 Other studies reported a hip adductor strength (≈470 N) similar to ours, and a lower adductor ratio has been related to hip pain. 31 In our report, we observed similar results in pain provocation tests in both groups of hockey players, which agreed with the strength level findings. Therefore, we can confirm that not only the whole Copenhagen Hip and Groin Outcome Score 49 or hip ROM but also the ratio of adductor/abductor strength can be a good indicator of impending hip pain.3,4,31
Limitations
The main limitation of this study was the study population, because we included only ice hockey players and some other mixed athletes who were used as controls, meaning that the findings are generalizable only to ice hockey players. However, similar analyses might be performed for different athletes. Another limitation is missing measurements for hip adduction and abduction ROM and the use of more advanced analyses. Advanced imaging such as computed tomography or magnetic resonance image was not available to evaluate the intra-articular structures of the hip joint. However, the ICS-specific evaluation used in this study was sufficient and was consistent in our measurements, and ICS-specific differences were found with sufficient practical consequences.
Conclusion
Our study demonstrated that ice hockey players had a smaller ICS of the hip joint, particularly on the backhand side, and that the condition of the ICS worsened with age. These structural changes were accompanied by reduced ROM in the hip joint, increased pain, and asymmetries in muscle strength. Hip ROM and symmetry of adductor/abductor muscle strength should be considered when diagnosing ice hockey players. The internal and external rotation and ROM of the hip joint are reduced more in players with higher training and match loads, whereas their adduction/abduction ratio is increased on their backhand side. Therefore, preventive programs should focus on hip ROM and strength balance between the right and left hips and adductors.
ICS assessment via sonography might become a useful tool for the evaluation of structural changes in the hip. Research on ice hockey–related injuries should focus more on the structural and functional condition of the backhand side of the hip.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251344240 – Supplemental material for Hip Joint Intercartilage Space, Range of Motion, and Lateral Differences in Elite and Subelite Ice Hockey Players: A Case-Control Trial
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251344240 for Hip Joint Intercartilage Space, Range of Motion, and Lateral Differences in Elite and Subelite Ice Hockey Players: A Case-Control Trial by Jitka Mala, Tomas Hybner and Petr Stastny in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted February 13, 2025; accepted March 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Charles University through projects PRIMUS22/HUM/019, UNCE24/SSH/012, and Cooperation–Sport Science Biomedical and Rehabilitation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Charles University, Faculty of Physical Education and Sport (No. 115/22).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.