
Abstract
Background:
The ulnar collateral ligament (UCL) plays a vital role in maintaining the stability of the elbow joint during overhead throwing activities. Stress to the UCL may lead to high-grade or full-thickness tears that require reconstruction or repair and lengthy rehabilitation in athletes. Workup of these injuries can sometimes reveal ossification in the ligament. It is unknown if ossification in the UCL affects postoperative outcomes.
Purpose/Hypothesis:
The purpose of this study was to investigate whether different preoperative ossification conditions of the UCL might influence various clinical and return-to-play (RTP) outcomes in athletes undergoing UCL reconstruction (UCLR). It was hypothesized that patients with preoperative ossification conditions in the UCL who underwent reconstruction would experience comparable rates of RTP and level of competition compared with all players undergoing UCLR.
Study Design:
Case series; Level of evidence, 4.
Methods:
An internal search was conducted to identify all cases of UCLR performed by 3 participating surgeons at the Andrews Institute between 2007 and 2022. Patients who had undergone primary UCLR and showed radiographic evidence of UCL ossification were included for analysis if they were ≥2 years after reconstruction. Retrospective chart reviews were performed for all included patients, and their radiographs were categorized by location of ossification. Differences in age, level of play, range of motion, and RTP status between patients with different ossification types were evaluated.
Results:
Between August 2007 and December 2022, 386 patients who underwent UCLR at the Andrews Institute were identified. Among these patients, 26% (n = 100) were found to have ossified UCLs. However, only 79 of these patients had complete medical records and were included in the analysis. Among the 79 athletes in this study with ossified ligaments, 71 (90%) who underwent UCLR returned to competitive sports. Athletes exhibited various classification conditions, including heavily calcified ligaments, calcified sublime tubercles, and humeral and/or ulnar-sided ossicles. No differences were found in the level of competitive RTP among the ossification groups.
Conclusion:
RTP rates in athletes with ossified ligaments are high and comparable with those in the literature across all ossification conditions.
The ulnar collateral ligament (UCL) plays a vital role in maintaining the stability of the elbow joint during overhead throwing activities. Stresses to the UCL may lead to high-grade or full-thickness tears that require reconstruction, while UCL repair is suitable for partial tears.1,8 Typically, UCL reconstruction (UCLR) has an 85% return-to-play (RTP) rate, but complications such as graft failure, loss of range of motion, and persistent pain can occur. Ossification of the UCL may complicate surgery by limiting flexibility and requiring modifications to technique, which can affect healing. Other risk factors for failure include injury severity, the athlete's age, rehabilitation adherence, and the surgeon’s skill, making careful management essential for optimizing outcomes. Therefore, investigation into factors that may complicate the outcomes of UCLR is warranted. This study aims to investigate whether preoperative ossification of the UCL may affect clinical and RTP outcomes in athletes undergoing UCLR.
A recent study utilized ultrasound imaging to examine the anatomic features of the UCL in a cohort of 127 asymptomatic professional baseball pitchers between 17 and 21 years of age. Investigators measured ligamentous abnormalities, joint space width, and UCL thickness in relation to number of years of pitching experience. Of those with 3 to 4 years of experience, 41% had hypoechoic abnormalities. 1 In a related study that measured echotextural abnormalities in 368 professional pitchers, researchers found that such abnormalities were present in 25% of dominant throwing elbows and at significantly higher rates (P < .001) than in nondominant elbows. 3
Although the exact mechanism of ossification is unclear, investigating the presence of ossification in the UCL of throwing elbows and its effect on surgical outcomes after reconstruction is warranted. We hypothesized that patients with preoperative ossification undergoing reconstruction would have comparable RTP rates to individuals without ossification, as reported in the literature.
Methods
Study Design and Search Strategy
Following institutional review board approval from Baptist Hospital, an internal search was conducted to include all primary UCLR cases with ≥2 years of follow-up that were performed by 3 participating surgeons (J.R.A., R.V.O., and S.J.) at the Andrews Institute in Gulf Breeze, Florida. All cases were performed between 2007 and 2022 following Andrews Tommy John surgical technique. 3 No specific modification was made to our standard surgical technique when ossification was encountered except that the ossification was routinely excised at the time of reconstruction. Search results were filtered using Current Procedural Terminology code 24346. Individuals aged <14 years old, those with a history of UCL repair or reconstruction, and those with a history of elbow surgery at another facility were excluded from this study. We excluded athletes aged <14 because of their skeletal immaturity. Radiographic reviews were then performed for all remaining patients, and initial radiographs were evaluated for ossification involving the UCL. Patients exhibiting radiographic evidence of ossification at the UCL were included in this study.
Radiographic Evaluation
Radiographic evidence of ossification of the UCL was determined using radiographs, which is considered the gold standard for diagnosing ossification. An orthopaedic surgeon (R.V.O) evaluated all radiographs using a picture archiving and communication system DICOM viewer (PACS). Anteroposterior, lateral, and oblique views were reviewed in each player. The radiographs were then categorized based on the location of ossification, and patients were assigned to one of the following groups: humeral-sided ossicle, ulnar-sided ossicle, humeral and ulnar–sided ossicle, ossified sublime tubercle, or heavily ossified ligament. Of note, radiographs demonstrating a heavily ossified sublime tubercle were classified as a heavily ossified ligament if separate ossification proximal to the ossified tubercle was identified. Radiographs were not calibrated, and the size of ossification could not be reliably measured.
Chart Review
Retrospective chart reviews were then performed for all included patients. Patient age, sex, sport, position, handedness, level of play, and preoperative and postoperative elbow range of motion were collected from the medical record. RTP status and the level of RTP after surgery were determined through chart review using 2-year follow-up data. The source of autograft used for reconstruction was also noted. Body mass index was not routinely measured for these young athletes. Autograft choice was due to surgeon preference with the default choice being palmaris autograft with a gracilis autograft being used if there was no acceptable palmaris autograft.
Statistical Analysis
In this study, we employed descriptive statistics (mean, standard deviation, etc) to summarize and present the characteristics of the data collected. Additionally, we conducted hypothesis testing to evaluate specific hypotheses regarding the population, using the insights gained from our sample data. Group comparisons for differences in range of motion, competitive level, autologous graft type, and RTP by ossification level were assessed using the Kruskal-Wallis test due to the non-normal distribution and unequal variance of the ossification groups. No post hoc testing was required because group differences were not detected. In this paper, statistical significance was determined at a 5% level. Fisher exact and Pearson chi-square tests with simulated P value were utilized to compare distributions across categorical variables in contingency table data.
Results
A total of 100 patients underwent UCLR at Andrews Institute from August 2007 to December 2022 and had preoperative radiographs demonstrating ossification of the UCL. Twenty patients were excluded, as they were not ≥2 years after reconstruction. One patient was excluded due to incomplete medical records. A total of 79 patients with radiographic evidence of UCL ossification who were ≥2 years after UCLR were included for analysis (Figure 1).

Flowchart representing chart review inclusion and exclusion. UCL, ulnar collateral ligament.
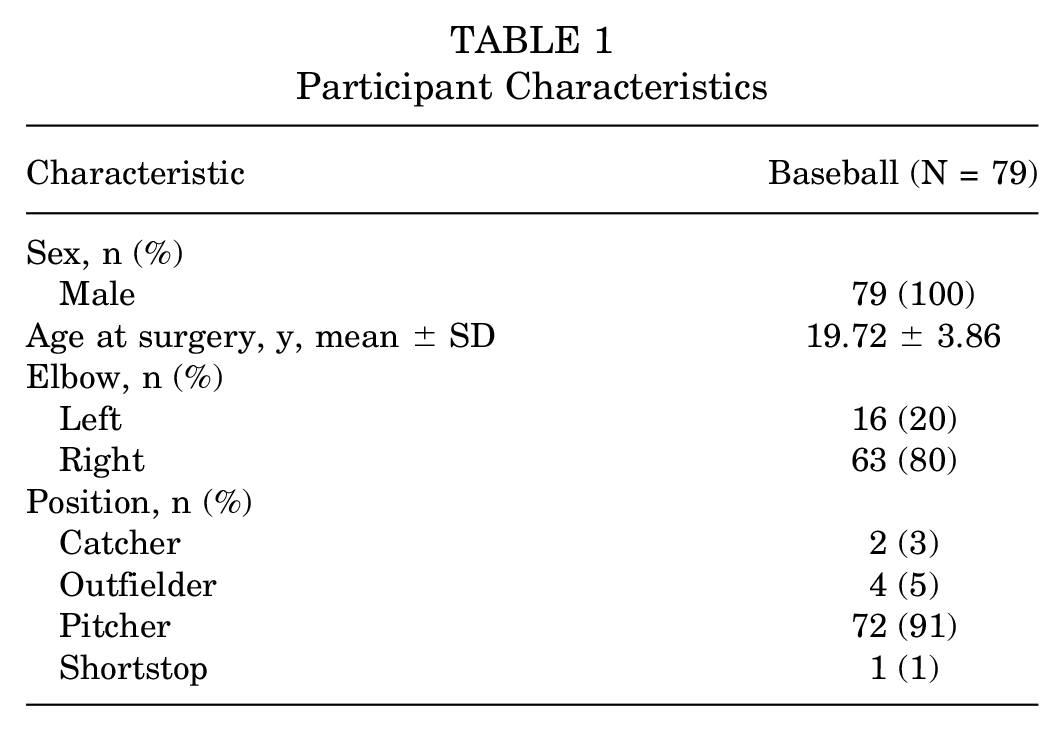
Of the 79 participants, all were male, with a mean age of 19.72 (SD, 3.86), ranging from 14 to 33 years (Table 1). Overall, 63 (80%) were right-handed, and 16 (20%) were left-handed. Among the baseball players, 72 (91%) were pitchers, and 7 (9%) were position players.
Participant Characteristics
Humeral-sided ossification was the most common form of ossification in 51 (65%) players. Twelve (15%) players had isolated ulnar ossicles. Three (4%) players had ossification on the ligament’s ulnar and humeral portions. Eight (10%) had ossified sublime tubercle, and 5 (6%) had a heavily ossified ligament. Figure 2 presents ossification examples across classifications. Of the total cases, 52 (66%) utilized a palmaris autograft, while 27 (34%) utilized a gracilis autograft for UCLR. Group differences in range of motion, competitive level, autologous graft type, and RTP by ossification level are depicted in Table 2. Of note, there was no statistical association between graft type and ossification type (P = .87), no statistical differences in range of motion (preoperative flexion [P = .10], preoperative extension [P = .39], postoperative flexion [P = .07], and postoperative extension [P = .54]) between different categories of ossification. No differences were found between ossification groups when comparing the preoperative competitive level (P = .76) or postoperative competitive level (P = .17).

Representative radiographs of ossified UCL cases. (A) Humeral ossification example of the right UCL. (B) Humeral and ulnar ossification example of the left UCL. (C) Ulnar ossification example of the right UCL. (D) Sublime ossification example of the left UCL. (E) Heavily ossified example of the left UCL. UCL, ulnar collateral ligament.
Group Differences in Range of Motion, Competitive Level, Autologous Graft Type, and Return to Play by Ossification Level a

HS, high school; MiLB, Minor League Baseball; MLB, Major League Baseball.
P < .05.
A key finding was that 90% (n = 71) of athletes ultimately returned to competitive sports, and 95.8% (68/71, excluding 8 unknown records) of athletes returned to the same or higher level of play after surgery. Only 3 athletes returned to a lower level of play, including 1 player who preoperatively played in Minor League Baseball but returned to play in an independent league. Another 2 athletes who were playing Major League Baseball returned to play in the minor league. Additionally, 8 (100%) of the ossified sublime tubercle group returned to play. Within the humeral-sided ossicle group, 46 (90%) returned to play. Eleven (92%) from the ulnar-sided ossicle group returned to play. Four (80%) of the players with a heavily ossified ligament returned to play. Two (67%) players within the humeral and ulnar–sided ossicles group returned to play. There were no statistically significant differences in RTP between groups. This statistical test requires caution due to the significant imbalance in group sizes, ranging from 3 to 46.
Descriptive statistics and comparisons between the gracilis tendon and palmaris longus are presented in Table 3. No statistical associations or differences were found at a 5% significance level. Players with a palmaris longus graft demonstrated higher rates of RTP compared with those with a gracilis tendon, although this difference was not statistically significant.
Group Differences in Range of Motion, Competitive Level, Ossification Location, and Return to Play by Graft Level a

HS, high school; MiLB, Minor League Baseball; MLB, Major League Baseball.
P < .05.
Discussion
Between August 2007 and December 2022, 386 patients who underwent UCLR at the Andrews Institute were identified. Among these patients, 26% (n = 100) were found to have ossified UCLs. However, only 79 of these patients had complete medical records and were included in the analysis. The RTP in this study of UCLR in the context of UCL ossification is similar to findings from other studies on RTP after UCLR. In the current research involving athletes with radiographic signs of ligament ossification, 95.8% (68/71, excluding 8 unknown records) returned to the same or a higher level of play after UCLR. The number of ossified ligaments in the present study is comparable with ultrasound-based studies showing 25% to 41% of ligamentous abnormalities in asymptomatic professional baseball pitchers, suggesting that ossification on imaging is not diagnostic of UCL pathology requiring surgery.1,3 The RTP rate in the present study is similar to the RTP rates reported in the literature after UCLR (79%-95%).2,4,6,7 These studies included both nonossified and ossified ligaments.
In the current review of radiographs of players undergoing UCLR, the most common type of ossification was seen as a small ossicle near the humeral end of the ligament. In our opinion, these are most likely the result of avulsion-type injuries, which can occur when the patient is skeletally immature. Often, there is a history of Little Leaguer's Elbow, but in some cases, the athlete cannot recall a previous episode of elbow pain. We have previously seen these small avulsions on radiographs in adolescents with open physes. Similarly, we speculate that heavily ossified sublime tubercles may be due to an old injury or chronic stress at the periosteum, which leads to bone buildup at that location. We have seen this type of periosteal reaction on radiographs in cases of adolescent throwers with open physes and elbow pain. Elbows with heavily ossified ligaments have the appearance of an enthesophyte, which can occur from repetitive stress. These enthesophytes are seen at other tendon and ligament attachments to bone throughout the body.
Our results, in general, suggest that ossification within the UCL does not result in less successful outcomes after reconstruction. The present retrospective case series data presented imbalanced groups with a few small group sizes ranging from 3 to 51. The post hoc analysis determined the Cramer V coefficient, which ranges from 0 to 1. Zero represents no association, while 1 signifies a complete association between 2 categorical variables. This study has a 5 × 2 contingency table with 5 ossification conditions leading to 10 comparisons. The estimated Cramer V coefficient from the data ranges from 0.02 (humerus: ulna) to 0.52 (humerus and ulna: sublime). Table 4 displays the results of this comparison, revealing wide confidence intervals that indicate the level of uncertainty around the actual effect.
Post Hoc Comparisons

Inf, infinite.
Three players had ulnar and humeral–sided ossifications, and only 2 could RTP (67%). Five patients had heavily ossified ligaments, of which 4 returned to play (80%). The patient with a heavily ossified ligament that did not RTP was a 19-year-old male left-handed collegiate pitcher. The workup revealed a heavily ossified ligament with an ulnar-sided ligament tear. He underwent reconstruction with gracilis autograft due to a lack of the palmaris longus tendon. Four months after surgery, he began an interval-throwing program without any issue and planned to return to baseball 1 year after his surgery. However, he was not able to successfully return to collegiate baseball. He continued to have medial elbow pain and decreased performance, which led him to discontinue his baseball career approximately 1 year after his surgery.
In the current study, gracilis autograft and palmaris autograft were used in patients with ligament ossification. Dugas et al 5 proposed that gracilis autograft should be used in cases of UCLR requiring bony excision due to increased deficiency of the native ligament. A recent systematic review found no difference in RTP between players with palmaris or gracilis autograft after reconstruction in general, but this study did not analyze outcomes associated with ossification of the UCL. 9 In our study, patients with a heavily ossified ligament underwent reconstruction utilizing the gracilis tendon (n = 3) and palmaris tendon (n = 2). One failure occurred from this group, using the gracilis. Our data do not support a recommendation for or against palmaris or gracilis autograft. No definitive recommendation can be made for the appropriate graft choice in the setting of an ossified ligament.
Limitations
There are limitations present in this study. The limitations lie in the study’s retrospective nature and the small number of heavily ossified ligaments. Additionally, the absence of a comparative group and patient-reported outcomes is a limitation of this study. Prospective studies on the reconstruction of heavily ossified UCLs would be difficult due to the relatively small number of throwers seen with these findings. However, patients with heavy ossification should be counseled about the possibility that they may not be able to expect the same chance to RTP as a player with no or limited ossification.
Conclusion
This study examined athletes who showed signs of ossification in their radiographs before undergoing UCLR. A key finding was that 71 out of 79 athletes (90%) successfully returned to competitive sports. Of these, 68 athletes (95.8%) returned to the same or a higher level of performance after surgery. RTP rates in athletes with ossified ligaments are high and comparable with those in the literature across all ossification conditions.
Footnotes
Final revision submitted February 18, 2025; accepted March 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.V.O. has received consulting fees from DePuy Syntheses and hospitality payments from Arthrex. J.K. has received support for education from Smith & Nephew and a grant from Arthrex. A.W.Z. has received consulting fees and royalties or a license from Arthex, support for education from CGG Medical, and a grant from DJO. S.E.J. has received royalties or a license from Arthrex and nonconsulting fees, food, beverage, travel, and lodging from Arthrex and CGG Medical. J.R.A. has received nonconsulting fees, travel, lodging, food, and beverage from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Baptist Hospital institutional review board (No. 1990412).