
Abstract
Background:
Excessive external rotation of the glenohumeral joint during the late cocking phase of throwing is a factor in internal impingement; however, the relationship between maximum external rotation (MER) of the glenohumeral joint and morphological changes in the shoulder joint is unclear.
Purpose:
To clarify whether glenohumeral MER is associated with quantified assessment of morphological changes in the throwing shoulder joint.
Study Design:
Descriptive laboratory study.
Methods:
This study included 15 male university and adult baseball players from a competitive team. The posterior glenohumeral distance (mm) and area of impingement (mm2), reflecting morphological changes in the shoulder joint, were measured using open magnetic resonance imaging. The percent posterior glenohumeral distance (%PGHD) and percent area of impingement (%AOI) were calculated as these values of the throwing shoulder divided by those of the nonthrowing shoulder. With a 3-dimensional motion analysis system, bar markers were affixed to the acromion and humerus, and the glenohumeral MER angle was measured.
Results:
Simple linear regression analysis revealed that the glenohumeral MER angle was associated with the %PGHD (β coefficient = 0.685; P = .005) and %AOI (β coefficient = 0.754; P = .001).
Conclusion:
The glenohumeral MER angle was associated with the %PGHD and %AOI, which reflects morphological shoulder-joint changes.
Clinical Relevance:
Assessment of excessive external rotation of the glenohumeral joint during the late cocking phase contributes to the understanding of morphological changes in the shoulder joint and related throwing injuries.
Keywords
The late cocking phase of the throwing motion leads to a maximum external rotation (MER) of the glenohumeral joints.26,27 Internal impingement occurs as a result of the contact between the posterior glenoid rim and the humeral greater tuberosity ‖ ‖ and causes posterior labral lesions, humeral head cysts, and rotator cuff tears, which result in throwing shoulder disabilities.2,3,14,15,19,22,37 Excessive shoulder external rotation during the late cocking phase represents the most common mechanism underlying the development of internal impingement.17,19,24,32 Therefore, accurate measurement of the glenohumeral MER angle during the late cocking phase is crucial for understanding internal impingement. With respect to the shoulder-joint position during the late cocking phase, previous studies using a 3-dimensional motion analysis system have reported approximately 90° of abduction, with 145° to 180° of external rotation of the shoulder.5-7,30,33 Miyashita et al26,27 were concerned that this measurement method was a shoulder-joint complex that included posterior tilt of the scapula and thoracic extension, and that it did not reflect the MER angle identified for the glenohumeral joint. Thus, a new method was developed to measure the glenohumeral MER angle using a bar with markers at both ends in the acromion and distal humerus, and it was reported to be reliable and valid.
Additionally, cadaveric studies have shown that contact pressure and strain in the joint are associated with an increase in the external rotation angle of the glenohumeral joint.24,32 Nevertheless, because the subject of these studies was a cadaver, the association between the external rotation motion of the shoulder during the late cocking phase and the morphological changes caused by internal impingement has not been clarified.10,38 As repeated microtrauma to musculoskeletal structures contributes to throwing shoulder disabilities, 4 Takahashi et al34,35 used open magnetic resonance imaging (MRI) to determine the posterior glenohumeral distance, defined as morphological changes in the posterior glenoid rim, and focused on the area of the rotator cuff inserted between the humeral greater tuberosity and the posterior glenoid rim. However, the association between morphological changes in the shoulder joint and the MER of the glenohumeral joint angle during the late cocking phase has not been determined. Clarifying the association between morphological changes in the shoulder joint and the glenohumeral MER angle during the late cocking phase is important to understand internal impingement.
Therefore, the present study aimed to investigate whether the glenohumeral MER angle is associated with morphological changes in the shoulder joint. The results of the present study may contribute to the establishment of evidence-based treatment strategies for internal impingement, which relates to throwing shoulder disabilities. We hypothesized that an increase in the glenohumeral MER angle during the late cocking phase would be associated with morphological shoulder-joint changes.
Methods
The study team for this laboratory study was formed between 2021 and 2023.
Participants
Data were collected from September 2022 to May 2023. The inclusion criteria were as follows: university baseball players or adult baseball players who have played university baseball and belong to a competition-level team. The exclusion criteria were previous shoulder surgery and shoulder pain during measurement in this study.
The present study was conducted in accordance with the ethical guidelines and regulations of the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee of the Ibaraki Prefectural University of Health Sciences (approval No. 1041). Written informed consent was obtained from all participants for their inclusion in the study.
Imaging Examination
MRI was performed using a 0.3-T whole-body MRI scanner (AIRIS Vento; Fujifilm Medical Ltd). The imaging conditions were as follows: T2* with gradient echo, horizontal section centered on the glenohumeral joint, and 90°, 100°, and 110° of external rotation from a 90° of abduction of the shoulder-joint position to simulate the late cocking phase. 34 Because the 110° of external rotation position was difficult to maintain for the nonthrowing shoulder, the range of motion (ROM) was not obtained and only the 90° and 100° of external rotation positions were assessed. A 10° or 20° tilt board was used to set the shoulder external rotation angle, and 2 examiners (M.M. and M.T.) changed the shoulder external rotation positions to prevent changes in the imaging section.
To achieve approximate shoulder-joint position in the late cocking phase, MRI values were evaluated on the basis of the external rotation ROM of the nonthrowing shoulder to determine the 90° or 100° of external rotation measurement position. Thus, nonthrowing shoulder-joint external rotation ROM <95° was measured at a 90° of external rotation position and external rotation ROM ≥95° was measured at a 100° of external rotation position. Additionally, the measurement position was fixed with a belt to prevent compensatory motion of the scapulothoracic joint and thoracic vertebrae.
Posterior Glenohumeral Distance of the Throwing Shoulder Normalized by That of the Nonthrowing Shoulder
The posterior glenohumeral distance was defined depending on the measurement method: (1) measurement of the posterior glenohumeral distance of the noncorresponding side-to-side limbs at the same external rotation angle quantified morphological changes in the posterior glenoid rim of the throwing shoulder, and (2) measurement of the corresponding ipsilateral limb at different external rotation angles quantified the interosseous proximity of glenohumeral joint alignment changes associated with internal impingement. The posterior glenohumeral distance had an intraclass correlation coefficient (ICC[1,2]) of 0.942 (95% CI, 0.912-0.962) for intraexaminer reliability (Figure 1A). 35

Methods for measuring the posterior glenohumeral distance (mm) and area of impingement (mm2). (A) Posterior glenohumeral distance: draw a line from the anterior to posterior glenoid rim (a) and a vertical line from the posterior glenoid rim to the humeral head (b), and measure the distance from the posterior glenoid rim to the humeral head (a-b). (B) Area of impingement): determine the area of the triangle connecting the posterior glenoid rim (a’), humeral greater tuberosity (b’), and rotator cuff depth (c’).
With respect to the first definition of this measurement, the percent posterior glenohumeral distance (%PGHD) was calculated as the posterior glenohumeral distance value of the throwing shoulder divided by that of the nonthrowing shoulder (%PGHD = posterior glenohumeral distance of the throwing shoulder/posterior glenohumeral distance of the nonthrowing shoulder × 100). A %PGHD >100% indicates a greater expansion of posterior interosseous distance of the throwing shoulder than that of the nonthrowing shoulder.
Area of Impingement of the Throwing Shoulder Normalized by That of the Nonthrowing Shoulder
The area of impingement was measured as the rotator cuff tendon area depicted by a low signal between the humeral greater tuberosity and the posterior glenoid rim. The area of impingement was defined depending on the measurement method: (1) measurement of the area of impingement of the noncorresponding side-to-side limbs at the same external rotation angle quantified the degreed of insertion of the rotator cuff tendon in the throwing shoulder, and (2) measurement of the corresponding ipsilateral limb at different external rotation angles quantified the degree of compression of rotator cuff tendons involved in internal impingement. The area of impingement had an ICC(1,2) of 0.925 (95% CI, 0.876-0.955) for intraexaminer reliability (Figure 1B). 34
With respect to the first definition of this measurement, the percent area of impingement (%AOI) was calculated as the area of impingement value of the throwing shoulder divided by the area of impingement value of the nonthrowing shoulder (%AOI = area of impingement of the throwing shoulder/area of impingement of the nonthrowing shoulder × 100). A %AOI >100% indicated a large side-to-side difference in morphological changes in the shoulder joint and a greater insertion of the rotator cuff tendon in the throwing shoulder.
Glenohumeral Joint and Shoulder-Joint MER Angles During the Late Cocking Phase
Three-dimensional motion analysis was performed using an 8-camera VICON system (Oxford Metrics Ltd) at a sampling frequency of 200 Hz. On the basis of methods reported by Miyashita et al,26,27 bars with markers at both ends were affixed to the acromion process, dorsal humerus, and dorsal forearm of the throwing side. Moreover, 7 other markers were affixed to the acromion process of the nonthrowing side, C7 spinous process, Th8 spinous process, L1 spinous process, sternum, and posterior superior iliac spine (Figure 2A). Pitching plates were set up indoors on an artificial turf, and full-effort throws were made 3 times to a target located 5 m away. In accordance with previous studies,26,27 the throw perceived by the player as the most accurate one was used to determine the representative values for the glenohumeral and shoulder MER angles. Three high-speed cameras were used for the throws and were synchronized with the VICON motion system using a trigger. Motion data were analyzed using VICON Nexus software (Version 2.0.1; VICON Motion Systems Ltd), and coordinate axes were obtained using Excel (Microsoft) data.

Marker attachment position and neutral position. (A) Marker attachments required for the maximum external rotation (MER) angle: the glenohumeral MER angle was calculated using the acromion bar and humerus bar, and the shoulder MER angle was calculated using the L1, acromion, humerus, and forearm bar midpoints. (B) Neutral position: shoulder joint at 90° of abduction and 0° of rotation.
The glenohumeral MER angle was calculated as the normal vector from (1) the 3-point coordinate axes of the acromion bars (2 anterior and posterior) and humerus bar (1 lateral) and (2) the 3-point coordinate axes of the humerus bars (2 medial and lateral) and acromion bar (1 posterior). The shoulder MER angle was calculated as the normal vector from (1) the 3-point coordinate axes of L1, acromion bar midpoint, and humerus bar midpoint and (2) the 3-point coordinate axes of the humerus bar midpoint, forearm bar midpoint, and acromion bar midpoint. The MER angle was calculated by determining the inner product of these calculated normal vectors, and the angle between 2 planes was calculated from the cosine of these vectors. Additionally, the glenohumeral and shoulder MER angles were estimated using the normalized neutral position at 90° of abduction and 0° of rotation of the shoulder joint (Figure 2B). One examiner (M.T.) securely affixed the markers so that accurate data could be collected, even with a quick throwing motion.
Physical Assessment
An examiner measured the external and internal rotations, and horizontal flexion passive ROM in the supine position. External rotation gain was calculated as the external rotation of the throwing shoulder minus the external rotation of the nonthrowing shoulder, with higher values indicating more anterior shoulder laxity.3,24,28 Glenohumeral internal rotation deficit was calculated as the internal rotation of the nonthrowing shoulder minus the internal rotation of the throwing shoulder, with higher values indicating posterior shoulder tightness.3,11,13,20,24,28 Horizontal flexion deficit was calculated as the horizontal flexion of the nonthrowing shoulder minus the horizontal flexion of the throwing shoulder, with higher values indicating posterior shoulder tightness.14,28
Statistical Analysis
A simple linear regression analysis was conducted to identify factors contributing to morphological changes in the shoulder joint, with the %PGHD and %AOI as the dependent variables and age, height, weight, body mass index, years of competition, external rotation gain, glenohumeral internal rotation deficit, horizontal flexion deficit, glenohumeral MER angle, and shoulder MER angle as the independent variables. Additionally, to clarify the state of proximity of the humeral head to the posterior glenoid rim with increasing shoulder external rotation, comparison of the posterior glenohumeral distances in the throwing shoulder at external rotation angles of 90°, 100°, and 110° was performed using a 1-way repeated-measures analysis of variance and subsequently a Bonferroni multiple comparison test. The posterior glenohumeral distances in the nonthrowing shoulder at external rotation angle of 90° and 100° was compared using a dependent t-test. Finally, the intraobserver reliabilities of the glenohumeral and shoulder MER angle were determined between the most and second accurate throws using the ICC.
Power analysis for the 1-way analysis of variance was conducted using G*Power software (Heinrich Heine University, Germany). With an alpha level of .05 and effect size f of 0.48, a sample size of 45 shoulders (15 participants in each external rotation position) was deemed to be sufficient to achieve a statistical power of 0.80. In the power analysis of the simple linear regression analysis, 13 research participants were required to obtain a statistical power of 0.8 when α and effect size f2 were set to .05 and 0.8, respectively. Statistical analyses were performed using SPSS Statistics (Version 29.0.2; IBM Corp) with a significance level of 5%.
Results
The participants were 15 male baseball players (right dominant, 15; shoulder joints, 30) who did not have throwing pain and belonged to a competition-level university baseball team (n = 12) or the top-prefecture-level adult baseball team (n = 3) of the Japan Amateur Baseball Association. Participants had a mean age of 20.5 ± 1.6 years, height of 173.7 ± 3.1 cm, weight of 71.5 ± 6.9 kg, body mass index of 23.7 ± 2.0 kg/m2, baseball experience of 12.1 ± 2.7 years, and practice frequency of 4.4 ± 1.8 practices per week. There were 5 pitchers, 2 catchers, and 8 fielders.
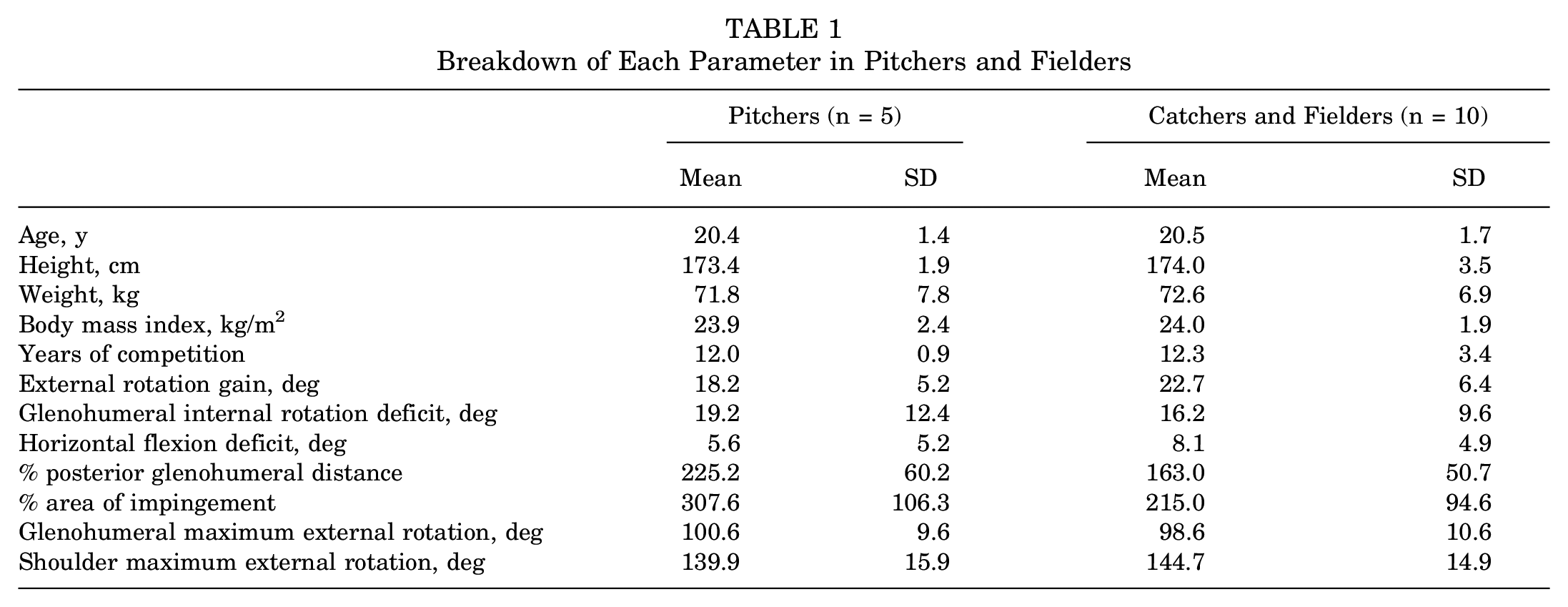
The study participants had a mean representative %PGHD of 178% ± 60%, %AOI of 236% ± 106%, external rotation gain of 18.0°± 10.8°, glenohumeral internal rotation deficit of 21.1°± 6.7°, and horizontal flexion deficit of 7.8°± 5.1°. Details of each parameter for pitchers and fielders are shown in Table 1.
Breakdown of Each Parameter in Pitchers and Fielders
Simple linear regression analysis revealed that the glenohumeral MER angle (β coefficient = 0.685; P = .005) and glenohumeral internal rotation deficit (β coefficient = −0.583; P = .022) were the factors associated with the %PGHD (Table 2), and that the glenohumeral MER angle (β coefficient = 0.754; P = .001), glenohumeral internal rotation deficit (β coefficient = −0.623; P = .013), and external rotation gain (β coefficient = −0.551; P = .033) were the factors associated with the %AOI (Table 3).
Simple Linear Regression With Percent Posterior Glenohumeral Distance as the Dependent Variable a

ERG, external rotation gain; GIRD, glenohumeral internal rotation deficit; HF, horizontal flexion; MER, maximum external rotation.
P < .05.
P < .01.
Simple Linear Regression With Percent Area of Impingement as the Dependent Variable a

ERG, external rotation gain; GIRD, glenohumeral internal rotation deficit; HF, horizontal flexion; MER, maximum external rotation.
P < .05.
P < .01.
A comparison of the posterior glenohumeral distance for the throwing shoulder angles (Table 4) revealed that the posterior glenohumeral distance was significantly lower in the 110° of external rotation position (5.3 mm) than in the 90° of external rotation position (6.7 mm) (P = .011). Additionally, the area of impingement was significantly lower in the 110° of external rotation position (21.0 mm2) than in the 90° of external rotation position (27.6 mm2) (P = .012). In contrast, a comparison of the posterior glenohumeral distance and area of impingement for the nonthrowing shoulder in the 90° and 100° of external rotation positions showed no significant difference (P > .05).
Comparison of the PGHD (mm) and AOI (mm2) in the Throwing and Nonthrowing Shoulder ER Positions a

PGHD, posterior glenohumeral distance; AOI, area of impingement; ER, external rotation.
PGHD in the 110° of ER position is significantly lower than that in the 90° of ER position (P = .011).
AOI in the 110° of ER position is significantly lower than that in the 90° of ER position (P = .012).
P < .05.
P < .01.
The ICC(1,2) values of the glenohumeral and shoulder MER angles were 0.979 (95% CI, 0.942-0.993) and 0.815 (95% CI, 0.545-0.933), respectively. The qualitative evaluation of kinematic data from stride foot contact to ball release, normalized at 100%, showed almost the same results as a previous study (Figure 3). 26

Glenohumeral and shoulder MER angles. GH, glenohumeral; MER, maximum external rotation; REL, ball release; SFC, stride foot contact; SH, shoulder.
Discussion
This study was designed to determine the effects of glenohumeral and shoulder MER on quantified morphological shoulder-joint changes in baseball players, which had not been investigated in previous studies. We hypothesized that the glenohumeral MER angle might be associated with morphological shoulder-joint changes, and the present study's findings confirmed this hypothesis.
Simple linear regression analysis showed that the glenohumeral MER angle was associated with the %PGHD and %AOI, and that the increasing glenohumeral MER angle may be associated with microtrauma and morphological changes of the throwing shoulder joint. Thus, an excessive glenohumeral MER throwing motion might result in an increased joint gap between the humeral head and posterior glenoid rim and a greater insertion of the rotator cuff tendon. Nevertheless, the present study showed an association between morphological changes and the glenohumeral MER angle, but not with the shoulder MER angle. Miyashita et al26,27 reported that the shoulder external rotation motion during the late cocking phase was a complex motion that involved the glenohumeral joint as well as scapular posterior tilt and thoracic extension. Thus, external rotation of the shoulder-joint complex with posterior scapular tilt and thoracic extension may be an important factor for internal impingement prevention.
Multiple comparison test results indicated that the posterior glenohumeral distance and area of impingement for the throwing shoulder were lower in the 110° of external rotation position than in the 90° of external rotation position. Furthermore, increased shoulder external rotation motion was a factor for the proximity of the humeral head to the posterior glenoid rim. Previous studies have identified an excessive glenohumeral external rotation motion as a factor contributing to internal impingement,19,32 which is consistent with the present results, suggesting that throwing at an increased glenohumeral MER angle is associated with contact between the posterior glenoid rim and the humeral head, and impinged rotator cuff tendon. Additionally, this study's results showed no association between the MER angle of the shoulder-joint complex and morphological changes in the shoulder joint, highlighting the importance of preventing regional and excessive glenohumeral external rotation motion during the late cocking phase, including subscapularis muscle training,21,23 thoracic and scapulothoracic joint mobility exercise,23,26,27,40 and scapular muscle training. 3
Finally, with respect to the associations of the %PGHD and %AOI with external rotation gain, glenohumeral internal rotation deficit, and horizontal flexion deficit in the throwing shoulder, fewer morphological changes in the shoulder joint were observed with increased external rotation gain and glenohumeral internal rotation deficit values. External rotation gain8,17,19,33 and glenohumeral internal rotation deficit1,3,9,16,28,29,31 have been regarded as factors for throwing shoulder disabilities; nevertheless, no consensus has yet been reached. In particular, Wilk et al 39 identified a decreased range of throwing shoulder external rotation as a risk factor, and Tyler et al 36 reported that shoulder internal rotation ROM was not associated with throwing shoulder disabilities. Additionally, these physical assessments represent throwing shoulder ROM characteristics based on side-to-side shoulder differences, which are affected by the nonthrowing shoulder ROM. If preexisting anterior laxity or posterior capsular contracture and posterior shoulder tightness are present in the nonthrowing shoulder, even low external rotation gain and glenohumeral internal rotation deficit values may contribute to morphological changes in the shoulder joint.
Limitations
This study has some limitations. First, the study quantified morphological changes in the shoulder joint and revealed a relationship with the glenohumeral MER angle. However, in clinical practice, the external rotation motion is difficult to distinguish between the glenohumeral and shoulder joints, which include the thoracic and scapulothoracic joints. In the future, the development of an assessment tool for clarifying the glenohumeral MER angle during the late cocking phase is warranted. Second, evidence for the %PGHD and %AOI values is limited to a few cross-sectional studies.34,35 Further prospective cohort research should be conducted on the quantitative assessment of morphological changes in the glenohumeral joint and symptoms of throwing shoulder disabilities. Finally, the side-to-side difference in MRI position and physical assessment may be influenced not only by anterior laxity and posterior tightness of the shoulder joint, but also by humeral retroversion.12,18
Conclusion
By using a 3-dimensional motion analysis system and open MRI, this study investigated whether the glenohumeral MER angle during the late cocking phase was associated with morphological shoulder-joint changes. Simple linear regression analysis revealed that the glenohumeral MER angle during the late cocking phase was associated with the %PGHD and %AOI. These findings suggest that assessment of excessive external rotation of the glenohumeral joint during the late cocking phase contributes to the understanding of internal impingement and related throwing injuries.
Footnotes
Acknowledgements
The authors thank S. Hanawa and Y. Nakayama of Inter Reha Corporation for their generous support with the measurement method for the VICON motion system.
Final revision submitted December 7, 2024; accepted February 20, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ethics Committee of the Ibaraki Prefectural University of Health Sciences (approval No. 1041).