
Abstract
Background:
Hip arthroscopy after in situ fixation of a slipped capital femoral epiphysis (SCFE) is used to treat postoperative disability that develops from metaphyseal cam deformity after pinning. Short-term follow-up has demonstrated excellent outcomes in patients treated for SCFE with subsequent hip arthroscopy. Midterm follow-up of these patients has been sparse and rarely reported in the literature.
Purpose:
To evaluate the midterm clinical and functional outcomes of patients undergoing hip arthroscopy after SCFE in situ fixation.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients with SCFE who underwent subsequent hip arthroscopy for femoroacetabular impingement (FAI) were enrolled in a prospective database. Inclusion criteria were a primary diagnosis of residual post-SCFE deformity and subsequent surgical treatment for FAI >1 year before the start date of the study. Patients were excluded if they were unable to be contacted. Participants were sent a survey that included physical function (Patient-Reported Outcomes Measurement Information System [PROMIS]) and Likert-style questions assessing disability and satisfaction. Patient charts were retrospectively reviewed for patient characteristics, visual analog scale (VAS) pain scores, and a modified Harris Hip Score (mHHS) from the postfixation but prearthroscopy period.
Results:
Of the 63 patients receiving hip arthroscopy after treatment for SCFE, 41 patients met the inclusion criteria and 34 completed the midterm follow-up survey (54.0% response rate). The mean duration of follow-up was 6.17 years. Patient subjective outcomes demonstrated that 88.3% of patients reporting being satisfied or very satisfied with their surgical result. The mean preoperative baseline mHHS was 67.43, indicating poor functional status. The mean midterm follow-up PROMIS-PF T score for this cohort was 50.81, indicating a slight overall improvement for the study cohort’s functional status when compared with the general population. The mean VAS pain score at rest was 5.09 preoperatively and 1.91 at midterm follow-up. The mean postarthroscopy iHOT-12 score was 68.27 (SD, 28.58), indicating greater quality of life postoperatively, with 20 patients (59%) obtaining a Patient Acceptable Symptom State (PASS) and a revision rate of 15%.
Conclusion:
The results of the first midterm follow-up of patients undergoing hip arthroscopy after surgical pinning of SCFE demonstrate improved functional and clinical objective outcomes compared with preoperative scores. These patients demonstrated poor functional status preoperatively but average or above-average functional status at the midterm follow-up postoperatively. Additionally, 20 patients (58.8%) obtained a PASS and a revision rate of 15%.
Clinical Relevance:
Arthroscopic treatment of post-SCFE FAI reported at short-term follow-up persists into the midterm follow-up period with hip function equivalent to age-matched population norms.
Keywords
Slipped capital femoral epiphysis (SCFE) is a devastating hip injury that can lead to proximal femoral deformities. There is concern that the incidence of SCFE is increasing, partly because of the increased prevalence of childhood obesity and early maturation.10,18,22 The physeal injury associated with SCFE causes morphological changes to the proximal femur and increases the risk of chondrolysis and avascular necrosis. 22 Adolescents who experience an SCFE and undergo reduction and screw fixation have been shown to have decreased hip function and poor outcomes.11,22 Accordingly, treatment consists primarily of in situ screw fixation to stabilize the epiphysis. Despite adequate fixation, the femoral head position in a slipped epiphysis can predispose to the formation of a cam deformity and lead to femoroacetabular impingement (FAI) syndrome, which can contribute to hip pain in this patient population. 17
FAI is increasingly recognized as a cause of hip pain in adolescents and young adults, with cam-type impingement having consistently been associated with the development of osteoarthritis. 27 Hip arthroscopy for symptomatic impingement has been shown to improve pain, patient-reported outcomes (PROs), and function.8,10,16,23 Moreover, there is some evidence that restoring offset through reshaping the femoral head-neck junction and eliminating the impingement can alter the natural history of the hip and prevent the development of osteoarthritis. 2
Although there is some metaphyseal remodeling after an SCFE, the residual apex anterosuperior deformity may lead to the development of FAI. 17 The repetitive trauma from this impingement prompts chondrolabral damage, leading to hip pain and loss of function.5,26,29 Previous studies have shown that treatment of the post-SCFE deformity with a femoral osteochondroplasty, both acutely at the time of injury and in a delayed fashion when impingement symptoms arise, is successful at restoring head-neck offset.15,27 Previous work has additionally demonstrated improved hip function over the short term. 27
Hip arthroscopy for isolated FAI has been shown to provide improvements in pain and hip function that persist into the midterm. 10 While post-SCFE impingement may resemble typical FAI in symptoms and treatment, there are pathophysiological differences inherent to the former, including distinct effects on tilt angle, femoral head offset, and range of motion.17,21 While the presence of SCFE is known to raise acute concern for sequelae such as avascular necrosis, there is a paucity of literature investigating whether these biomechanical alterations affect longitudinal functional outcomes past the short-term interval among patients who choose to undergo hip arthroscopy.11,22 The purpose of this study was to quantify PROs, as well as the incidence of conversion to total hip arthroplasty (THA), at the midterm follow-up in a population of patients with SCFE treated with subsequent hip arthroscopy for FAI.
Methods
Study Design and Patient Inclusion
After IRB approval (IRB No. 00055341), all patients at a single tertiary care institution who had undergone surgical fixation for SCFE and subsequent hip arthroscopy for symptomatic FAI were recruited for this survey study. Patients included in this study underwent hip arthroscopy by the senior author (S.K.A.) between August 2008 and July 2020 and were identified using a query of the principal investigator’s (S.K.A.) database. Inclusion criteria were a primary diagnosis of residual post-SCFE deformity and subsequent surgical treatment for FAI >1 year before the start date of the study. Patients unable to be contacted were excluded from the study but were included in a calculation of the follow-up rate.
As part of our institution’s standard of care, patients routinely fill out a preoperative worksheet containing PRO measures, such as the modified Harris Hip Score (mHHS), Hip Outcome Score (HOS), and visual analog scale (VAS) for pain score. Routine preoperative Patient-Reported Outcomes Measurement Information System [PROMIS] scores were not collected. Patient charts were accessed using the institution’s electronic medical record and retrospectively reviewed for surgical and demographic information as well as their preoperative PRO scores from the period after pinning and before hip arthroscopy. The Southwick angle was determined from the frog-leg lateral radiograph. The angle between the line representing the axis of the femur and a line perpendicular to the line connecting the anterior and posterior epiphysis was measured. The operative side was subtracted from the nonoperative side to yield the Southwick angle. Southwick angles <30° were categorized as mild slips, angles of 30° to 50° were categorized as moderate slips, and angles >50° were categorized as severe slips.
Surgical Technique
The surgical technique consistently utilized throughout this study was based on previously published research. 15 Briefly, the patient was placed supine on a traction table (Smith & Nephew or Stryker). The hip was accessed as described in the literature and utilizing either an interportal or T-type capsulotomy. 2 Hardware was removed in cases of screw impingement. Labral repair was performed on a case-by-case basis if indicated. Subsequently, a femoral osteochondroplasty was performed on the impingement lesion and the femoral head was reshaped (Figure 1). Fluoroscopic evaluation and dynamic intraoperative testing were utilized to evaluate for the presence of residual impingement. Capsular repair was performed using 1 to 5 nonabsorbable sutures.
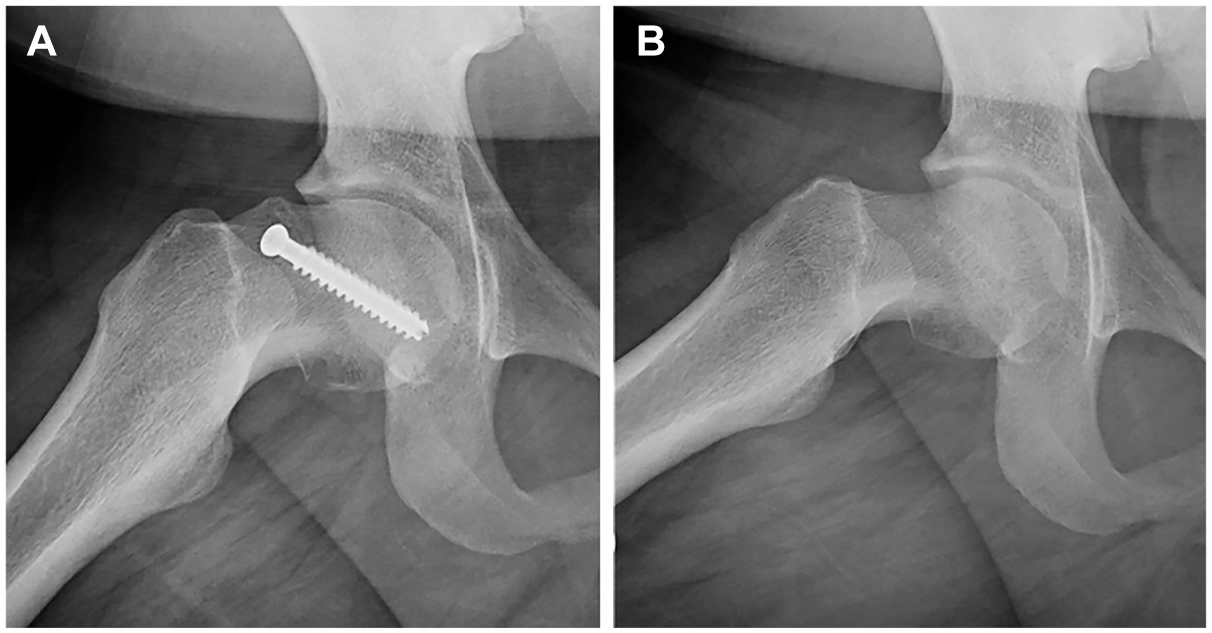
Frog-leg lateral radiographs obtained in a patient (A) treated with in situ fixation with subsequent cam morphology and (B) after arthroscopy osteochondroplasty.
After hip arthroscopy, patients underwent a physical therapy regimen with a primary focus on strength, conditioning, and restoration of range of motion. Patients were restricted to toe-touch weightbearing for the first 2 weeks and partial weightbearing with crutches for the following 2 weeks. Patients were given instructions to avoid hip external rotation and hyperextension for 6 weeks and, after this initial period, were encouraged to utilize the full range of motion of the hip. Patients returned to sport between 4 and 6 months on a case-by-case basis. Naproxen (500 mg, twice daily) for 2 to 3 weeks was given as prophylaxis for heterotopic ossification.
Survey Methodology
Patients were first contacted by mail, informing them of the study. Patients were subsequently contacted over the telephone and sent an email containing a link to the survey. If a patient could not be reached, contact was attempted an additional 2 times. All survey data were housed in an electronic data warehouse (REDCap) before exportation and analysis. The survey included a single assessment numeric evaluation (SANE) prompt, subjective Likert-style questions assessing disability and satisfaction, the VAS pain score, and PROMIS Physical Function (PF) and 12-item International Hip Outcome Tool (iHOT-12) questionnaires (Supplemental Appendix A). Crucially, because this retrospective study spanned a prolonged period, the PRO instruments used by the senior author changed over time; as a result, the preoperative and postoperative scores for this cohort vary.
Statistical Analysis
Descriptive statistics were utilized to analyze patient and survey data. Calculations were performed using SPSS Version 28 software (IBM Corp).
Results
Of the 63 patients identified in the initial database query, 22 (34.9%) were excluded due to a lack of working contact information. Of the 41 patients contacted, 1 participant (1.6%) declined enrollment and 6 (9.5%) were contacted but did not complete the survey. The final cohort consisted of 34 patients, accounting for 42 hip arthroscopies, for a follow-up rate of 54% (Figure 2). Patient characteristics are summarized in Table 1, with a mean follow-up time of 6.17 years (range, 1.66-13.13 years).

Flowchart used to determine study population.
Patient Characteristics of Study Population (N = 34) a
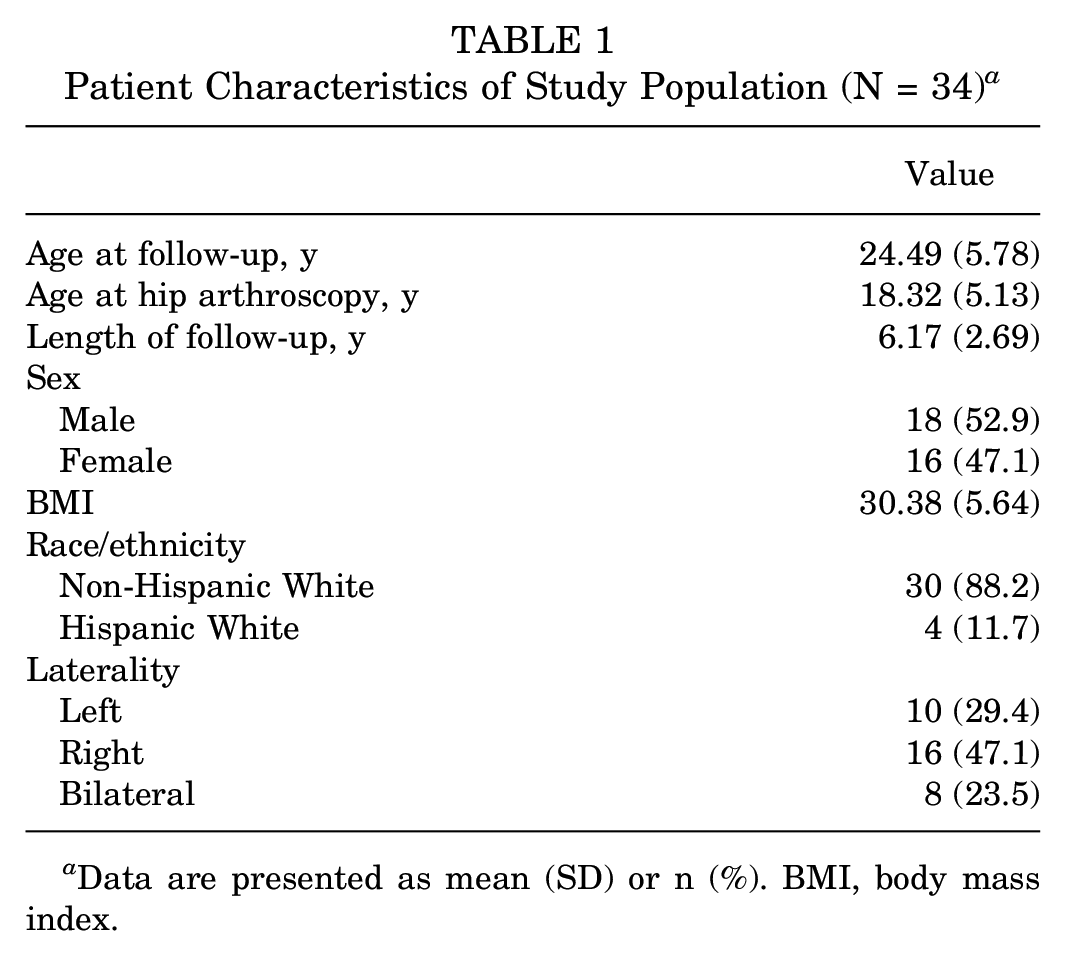
Data are presented as mean (SD) or n (%). BMI, body mass index.
Most hips underwent a concomitant labral repair (29; 69.0%) with acetabuloplasty (32; 76.2%) and utilized an interportal capsulotomy (41; 97.6%). Clinical characteristics are summarized in Table 2.
Clinical Characteristics of Study Population (N = 42) a

Data are presented as mean (SD) or n (%). LCEA, lateral center-edge angle.
Incomplete data for 2 hips.
Incomplete data for 1 hip.
The mean SANE score rating at final follow-up was 78.6% (SD, 19.8%) of normal. Almost all respondents (33/34) expressed satisfaction or neutrality toward the surgery, and 28 (82.4%) would undergo the surgery again, with 5 (14.7%) being neutral in this respect and 1 patient (2.9%) saying they would not. No patients (0%) reported undergoing a THA procedure, although 5 patients (11.9%) underwent a revision hip procedure during the interim: 4 revision hip arthroscopies and 1 rotational osteoplasty. Subjective information from the final follow-up survey can be found in Table 3.
12-Month Postoperative Survey Results: Subjective Measures a
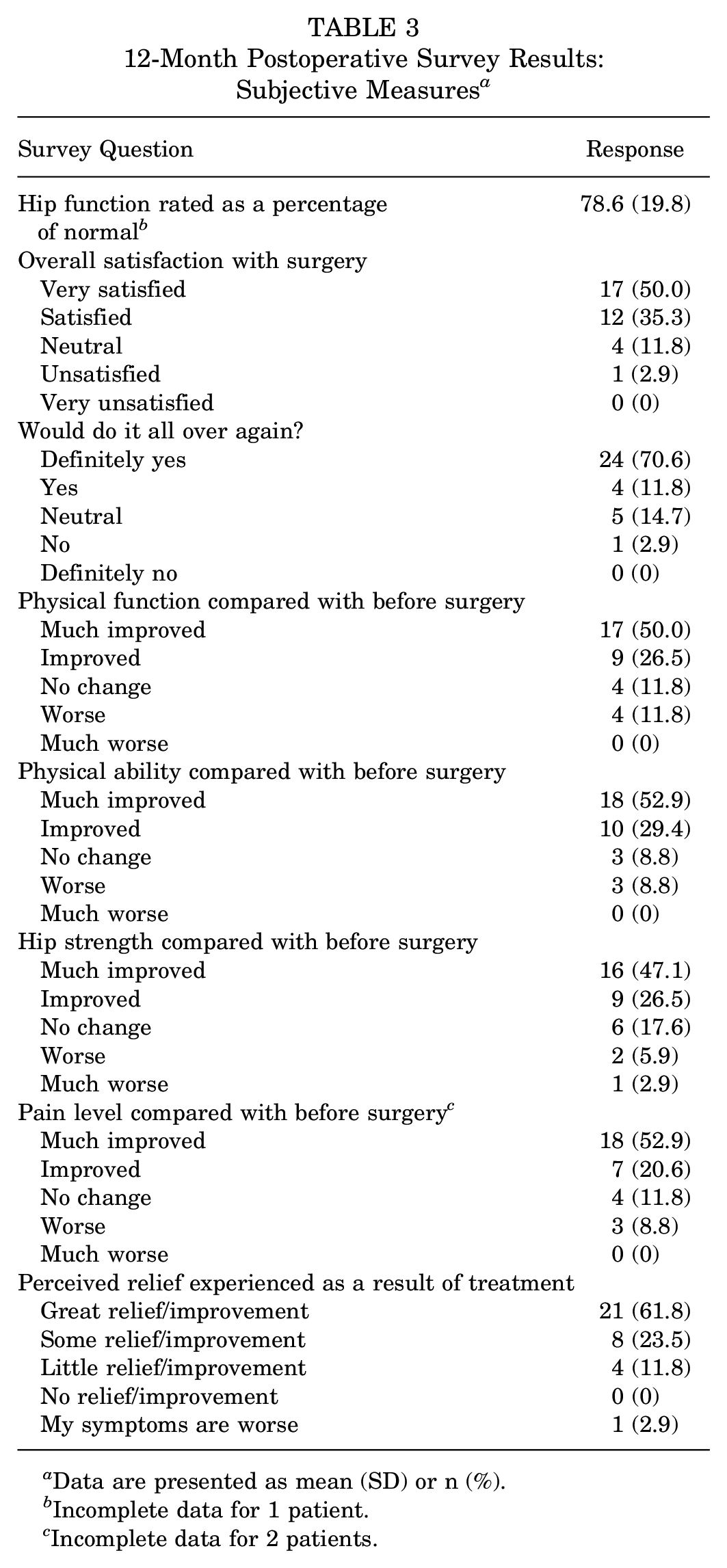
Data are presented as mean (SD) or n (%).
Incomplete data for 1 patient.
Incomplete data for 2 patients.
Preoperatively, the mean mHHS was found to be 67.43. The mean follow-up PROMIS-PF T score was 50.81 (SD, 10.74), indicating a slight overall improvement for the study cohort’s functional status when compared with the general population. 4 The mean prearthroscopy VAS pain score at rest was 5.09 (SD, 2.74), and 6.88 (SD, 2.25) during sports. After arthroscopy, the VAS pain score at rest was 1.91 (SD, 2.38), and 3.88 (SD, 2.92) during sports at midterm follow-up. The mean postarthroscopy iHOT-12 score was 68.27 (SD, 28.58), with 20 patients (58.8%) obtaining a Patient Acceptable Symptom State (PASS) (Table 4). 25
Patient-Reported Outcome Score Results a
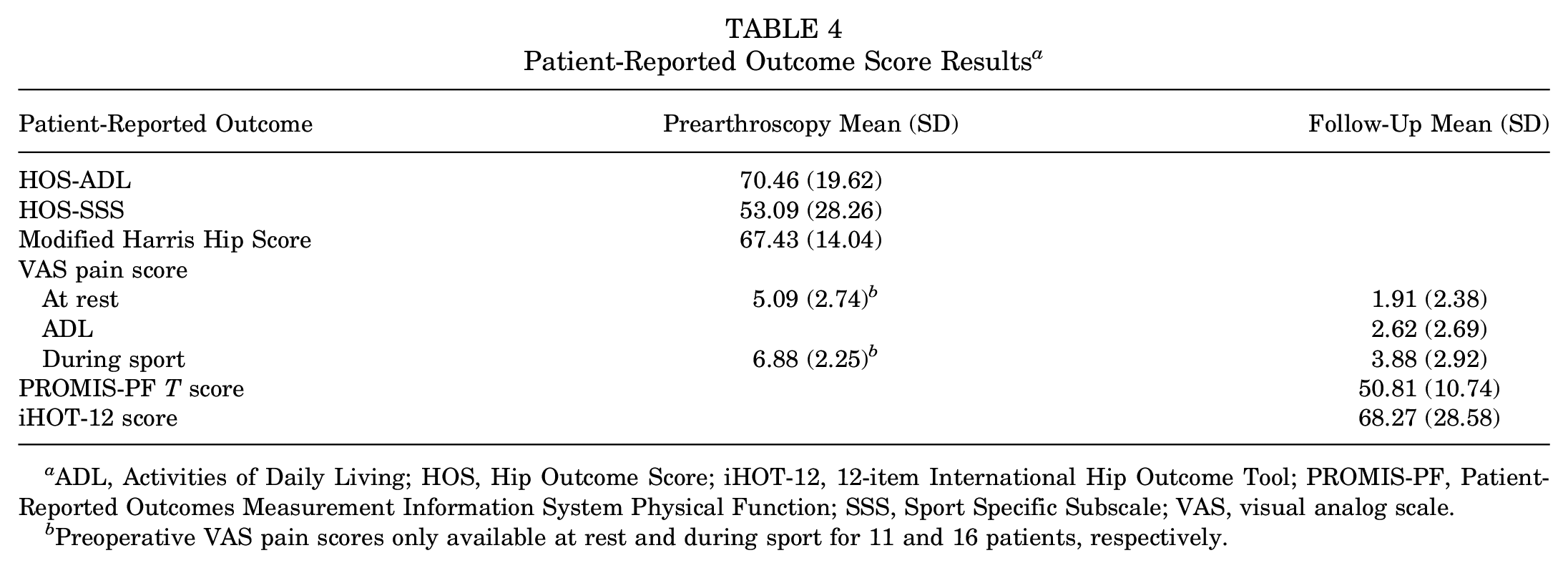
ADL, Activities of Daily Living; HOS, Hip Outcome Score; iHOT-12, 12-item International Hip Outcome Tool; PROMIS-PF, Patient-Reported Outcomes Measurement Information System Physical Function; SSS, Sport Specific Subscale; VAS, visual analog scale.
Preoperative VAS pain scores only available at rest and during sport for 11 and 16 patients, respectively.
Discussion
The purpose of this study was to quantify the midterm outcomes of hip arthroscopy and femoral osteochondroplasty in patients with FAI due to post-SCFE deformity after in situ percutaneous screw fixation. Our study population consisted of 34 patients with a mean follow-up of 6.17 years. We utilized several different metrics to assess the outcomes of patients at the midterm follow-up, overall demonstrating that arthroscopic labral repair and osteochondroplasty provide this patient population with improvement in pain, 60% PASS for iHOT-12, and a mean PROMIS-PF score of 50.
The midterm follow-up survey results demonstrate that most patients viewed their surgical result positively, with 82.4% of patients indicating that they would undergo the procedure again and no patients regretting their decision. Despite a revision rate of 15% in this patient cohort, the survey results consistently show improvements in subjective function, physical ability, hip strength, and pain relief from the surgery. While most patients achieved the PASS for iHOT-12, 40% of patients did not, and just less than one-half of the patients in this study reported postoperative PROMIS scores <50. However, the overall surgical satisfaction, reported in Likert-style format, was 85.3%, with patients reporting that the function of their affected hip was 78.6% of that of their normal hip. These results were further substantiated by standardized PRO measures. At the midterm follow-up, the mean PROMIS-PF score was equivalent to the functional status of the population norm (PROMIS-PF score of 50). At the final follow-up, no patients had undergone conversion to THA, further supporting the benefit of hip arthroscopy in this patient population.
Unstable SCFEs frequently have antecedent pain, indicating a more acute-on-chronic time course that may occur over 6 to 8 weeks.9,20 Many studies have reported both acetabular cartilage injury and labral tear at the time of initial presentation, and some have suggested that this may be due in part to the acute-on-chronic nature of this pathology resulting from deformity impingement.14,15 It is clear, however, that even mild SCFEs may result in FAI given the characteristics of the present study population.27-29 Current epidemiological studies of patients with SCFE suggest that the risk of avascular necrosis ranges from 15% to 50% for unstable slips. 19 These complicating factors have led to less confidence in the prognosis for patients after SCFE FAI, but our results demonstrate that the outcomes of hip arthroscopy in these patients are comparable to those of other FAI patients.
Several studies have reported midterm outcomes (PROs) for hip arthroscopy, regardless of the cause of FAI.1,3,6,8,13,16,23 The primary PRO metrics utilized in these studies were the mHHS and the HOS–Sport Specific Subscale. It is difficult to make direct comparisons to the present study because of the inconsistency in PRO metrics and reporting methods, but our results are consistent with the literature and show that hip arthroscopy provides substantial improvement in pain and physical function that persists into the midterm. It is worth noting that pain relief, in some cases, may be a result of hardware removal. In terms of patient satisfaction, it appears that the post-SCFE FAI population is on par with or above the general FAI population, with 85.3% of patients in the present study reporting satisfaction with their surgery, compared with 79.2% satisfaction at the midterm follow-up in the general FAI population, using the same Likert-style format. 25 Overall, the results of our study further contribute to the growing body of literature showing that hip arthroscopy for FAI, regardless of cause, provides substantial functional and pain benefits at the midterm follow-up. 9
Previous work by Wylie et al 27 has demonstrated significant improvements in function over the short term for patients after SCFE FAI treated with hip arthroscopy. This was further analyzed in a 2020 comparative investigation based on the severity and treatment modalities for patients after SCFE FAI, which found that moderate and severe deformities were more likely to be treated via an open procedure, versus arthroscopic treatment for milder slips. 29 At a mean follow-up of 4.3 years, both groups exhibited similar improvements in pain and function scores, although the 19 patients treated arthroscopically were noted to have slightly higher function at follow-up. 29 To our knowledge, the present study is the largest study to date to evaluate outcomes past the short term in this patient population. Only 1 previous study evaluating midterm outcomes in patients with SCFE treated with hip arthroscopy for FAI exists in the literature. Rahm et al 24 demonstrated good functional outcomes at midterm follow-up in a cohort of 11 patients treated for SCFE. Furthermore, Rahm et al reported on patients who were treated with prophylactic osteochondroplasty at a median of 10 days after in situ pinning, which differs significantly from the present study, in which only patients with symptoms were treated, with a mean time between pinning and osteochondroplasty of 5.36 years. Furthermore, the study by Rahm et al was limited to patients with mild slips (Southwick angle <30°), in contrast to the present study, which also included patients with moderate and severe slips.
Natural history studies investigating the consequences of SCFE and in situ pinning have shown that many patients do well in the long term. 19 There is debate as to whether prophylactic osteochondroplasty should be performed early, and our current treatment protocol is to allow patients to recover from their slip, as many patients do not require hip arthroscopy after SCFE pinning. Arthroscopic treatment is typically reserved for those with symptomatic impingement. In addition, screw impingement necessitating hardware removal is a common problem that occurred in the majority of the patients in the present study. By delaying arthroscopic osteochondroplasty, the surgeon is given the opportunity to perform a hardware removal at the time of the arthroscopy that would not be possible if the osteochondroplasty were to be performed shortly after pinning.
While avascular necrosis seems to be the main cause of THA in the post-SCFE population, degenerative osteoarthritis is the second most common cause.11,19 Long-term natural history studies of patients after SCFE estimate the 20-year risk of THA for secondary osteoarthritis to be 5%. 12 Although the exact rate remains unknown due to the variable time course, the mean age at the time of conversion to THA was 38 years, far younger than the mean age of patients undergoing THA for primary osteoarthritis, suggesting that the post-SCFE deformity does play a role.7,11 In the present study, no conversions to THA were reported, although this finding is inconclusive given the relatively young mean age at follow-up (24.49 years) among the included patients, along with the significant proportion lost to follow-up, as they would typically not be followed for avascular necrosis in the clinic in which this study was conducted. Unfortunately, we were unable to obtain imaging at the final follow-up to evaluate for radiographic signs of hip degeneration.
Limitations
The main limitation of this study is the lack of consistent outcome measures, which prevents a direct comparison of pre- and postoperative hip outcome scores. The orthopaedics department at the University of Utah has long advocated for the use of PRO measures to better assess the results of our surgeries. Early on, joint or subspecialty-specific scores were collected and recorded on paper, but later the department shifted to exclusively utilizing PROMIS and an electronic collection process, as it is thought to better capture the overall health of a patient and allows comparison with population norms. While this will be beneficial over the long run, this has limited our ability to provide direct comparisons to our preoperative scores. It is, however, reassuring that the results of this study indicate that patients are doing as well as their comparative norms. Being a survey-based study, our results are subject to the same limitations of all survey-based studies, namely, recall bias and selection bias. In our study, 34.9% of patients lacked a working email or telephone number in 2 separate electronic medical record systems, and the inability to contact these patients, although out of our control, certainly furthered the selection bias. Loss of follow-up could certainly affect our ability to identify patients who have not improved with hip arthroscopy or needed further surgical intervention. Furthermore, the present study was unable to include objective outcome measures along with the surveys, such as physical examination, strength testing, and radiographic examination. Additionally, as this study spans 12 years, variations in surgical technique may have occurred during this time period and could affect the outcomes. However, the femoral osteochondroplasty process remained relatively similar during this time. Lastly, the present study provides insight solely into how this patient cohort is doing at midterm follow-up and does not provide any direct comparison to similar patients who did not undergo hip arthroscopy or who underwent open treatment of the SCFE deformity. Although we compared our findings to those seen in the existing relevant literature, this lack of a propensity-matched control group increases the potential risk of unknown confounding variables affecting the results of the study. Ultimately, further research is needed to better understand the optimal treatment of these patients and whether these results persist into the long-term.
Conclusion
The results of the first midterm follow-up of patients undergoing hip arthroscopy after surgical pinning of SCFE demonstrate improved functional and clinical objective outcomes compared with preoperative scores. These patients demonstrated poor functional status preoperatively but average or above-average functional status at the midterm follow-up postoperatively. Additionally, 20 patients (58.8%) obtained a PASS and a revision rate of 15%. Arthroscopic treatment of post-SCFE FAI reported at short-term follow-up persists into the midterm follow-up period with hip function equivalent to age-matched population norms.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251342579 – Supplemental material for Improved Midterm Outcomes After Hip Arthroscopy for Femoroacetabular Impingement Syndrome in the Setting of a Previous Slipped Capital Femoral Epiphysis
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251342579 for Improved Midterm Outcomes After Hip Arthroscopy for Femoroacetabular Impingement Syndrome in the Setting of a Previous Slipped Capital Femoral Epiphysis by Adam H. Kantor, Allan K. Metz, Collin D.R. Hunter, Reece M. Rosenthal, Ameen Z. Khalil, Devin L. Froerer, Travis G. Maak and Stephen K. Aoki in The Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted January 14, 2025; accepted February 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.K.A. has received consulting fees from Stryker Corp. T.G.M. has received consulting fees from Arthrex Corp and education payments from Active Medical. A.H.K. has received hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The University of Utah (IRB No. 00055341).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.