
Abstract
Background:
Hip labral and chondral lesions are commonly found as co-occurring conditions in patients with abductor tendon tears. Concomitant hip arthroscopic surgery for the correction of intra-articular abnormalities and endoscopic abductor tendon repair has therefore emerged as a strategy to address these conditions simultaneously.
Purpose:
To systematically review the existing literature assessing clinical outcomes after endoscopic abductor tendon repair with concomitant hip arthroscopic surgery for the treatment of intra-articular abnormalities.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Under PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, the PubMed, CENTRAL, and Scopus databases were queried in May 2023 to conduct this systematic review using the keywords “hip arthroscopy,”“gluteal,”“abductor,”“gluteus,”“minimus,” and “medius.” Articles were included if they reported preoperative and postoperative patient-reported outcome measure (PROM) scores for patients undergoing endoscopic abductor tendon repair for gluteus medius and/or gluteus minimus tears with concomitant hip arthroscopic surgery for the treatment of labral tears and/or femoroacetabular impingement. We identified a total of 404 articles after our initial search. Title, author, publication date, study design, patient characteristics, preoperative radiographic findings (lateral center-edge angle, alpha angle, and Tönnis grade), concomitant surgical procedures performed, preoperative and postoperative PROM scores, measures of clinical benefit, and secondary surgery performed (revision arthroscopic surgery, revision abductor tendon repair, and conversion to total hip arthroplasty) were recorded. P values were extracted from the articles included in our review, all of which defined statistical significance as P < .05. We were unable to create forest plots for these data, given that no single PROM (preoperative and postoperative scores in means and standard deviations) was reported in ≥3 articles. This also prevented us from further analyzing heterogeneity. We calculated the total rate of secondary surgical procedures by dividing the instances of these events by the total number of patients across the 4 studies that included these outcome measures.
Results:
After duplicate articles were removed, 270 articles entered the abstract screening phase, and 11 full-text articles were reviewed. Overall, 5 articles were included in the systematic review. A total of 223 hips were included, with mean follow-up times ranging from 26 to 74 months. All studies reported a significant improvement (P < .05) on all reported PROMs from preoperative to latest postoperative time points. There were 2 studies that compared combined endoscopic abductor tendon repair and labral treatment with a matched group undergoing hip arthroscopic surgery alone and found no significant differences (P > .05) between groups. Among studies reporting secondary surgical procedures, there was 1 case (0.9%) of revision abductor tendon repair and 5 cases (4.3%) of conversion to total hip arthroplasty.
Conclusion:
Our systematic review demonstrated that patients who underwent concomitant endoscopic abductor tendon repair and hip arthroscopic surgery had significant improvements on PROMs with low rates of secondary surgery at a minimum 2-year follow-up. Longer-term studies are needed for us to understand concomitant treatment methods for multiple abnormalities in patients undergoing hip arthroscopic surgery in the future.
Chronic degenerative tears of the gluteus medius and minimus tendons are an increasingly well-recognized cause of greater trochanteric pain syndrome (GTPS) in part because of improved imaging modalities and other diagnostic techniques.15,18 Studies evaluating radiological findings in patients with GTPS have reported rates of abductor tendon tears of 28% to 45%, with some degree of abductor tendinopathy present in the majority of these patients.3,29 They are far more common in female patients and have a peak incidence in the fifth and sixth decades of life. 18 Patients typically have an insidious onset of lateral hip pain aggravated by weightbearing, and examination findings may include tenderness at the greater trochanter, weakness in hip abduction, and a Trendelenburg gait. 33 Magnetic resonance imaging can confirm the diagnosis and may demonstrate findings along a spectrum from tendinosis, to partial-thickness tears, to full-thickness tears with or without muscle atrophy and fatty degeneration.3,7 The initial management of abductor tendon abnormalities includes activity modification, physical therapy, nonsteroidal anti-inflammatory medications, and peritrochanteric corticosteroid or platelet-rich plasma injections.2,11,17,22
Surgical repair of abductor tendon tears, with either an open or endoscopic approach, is considered for cases refractory to nonoperative measures.6,25 While both of these approaches have been shown to improve pain and functional outcomes, there appears to be a lower postoperative complication rate with the minimally invasive endoscopic approach.1,6,20 In addition, the endoscopic approach lends itself to the simultaneous correction of peritrochanteric and intra-articular abnormalities. Meghpara et al 23 reported that among patients undergoing hip arthroscopic surgery for femoroacetabular impingement, 3.9% and 1.7% of patients had symptomatic and asymptomatic abductor tendon tears, respectively. Furthermore, a systematic review by Yee et al 35 found that among patients undergoing endoscopic abductor tendon repair, over 85% and 25% had labral and chondral lesions identified, respectively. Intra-articular abnormalities can be difficult to distinguish from abductor tendinopathy and other causes of GTPS and may contribute to lateral hip pain.28,35
There is currently a paucity of literature specifically evaluating the efficacy of combining hip arthroscopic surgery and endoscopic abductor tendon repair. The purpose of this study was to systematically review the existing literature assessing clinical outcomes after endoscopic abductor tendon repair with concomitant hip arthroscopic surgery for the treatment of intra-articular abnormalities. It was hypothesized that these patients would demonstrate significant improvements in patient-reported outcomes and low rates of secondary surgery at a minimum 2-year follow-up.
Methods
Literature Search
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed while conducting this study. The protocol for this review was registered in PROSPERO (CRD42023427206) before performing the literature search. PubMed, CENTRAL, and Scopus were queried in May 2023 from database inception. Search strategies for the databases are shown in Table 1. Using the Covidence screening tool (www.covidence.org; Veritas Health Innovation), 2 independent reviewers (J.G., P.F.M.) performed title and abstract screening. A full-text review was performed by 2 senior authors (S.S., A.E.J.) before final inclusion. A senior author (A.E.J.) resolved all conflicts between reviewers. Articles were included if they reported preoperative and postoperative patient-reported outcome measure (PROM) scores for patients undergoing endoscopic abductor tendon repair with concomitant hip arthroscopic surgery for the treatment of intra-articular abnormalities and were written in English. Animal studies, abstracts, biomechanical studies, case reports, opinion articles, review articles, technique articles, and articles that did not report postoperative outcomes were excluded. Studies comparing concomitant abductor tendon repair with hip arthroscopic surgery for the treatment of intra-articular abnormalities against a control group undergoing hip arthroscopic surgery alone underwent a qualitative subanalysis. P values were extracted from the articles included in our review, all of which defined statistical significance as P < .05.5,9,21,24,27 We were unable to create forest plots for these data, given that no single PROM (preoperative and postoperative scores in means and standard deviations) was reported in ≥3 articles. This also prevented us from further analyzing heterogeneity. We calculated the total rate of secondary surgical procedures (eg, revision abductor tendon repair, conversion to total hip arthroplasty [THA]) by dividing the instances of these events by the total number of patients across the 4 studies that included these outcome measures.
Database Search Strategies a

ab, abstract; ABS, abstract; KEY, keywords; kw, keywords; ti, title.
Quality Assessment
The Methodological Index for Non-Randomized Studies (MINORS) criteria were used to qualitatively assess all articles. 32 There were 2 independent authors (J.G., P.F.M.) who scored all articles, and conflicts were resolved by a senior author (S.S.).
Data Extraction
The following data were extracted: title, author, publication date, study design, patient characteristics, preoperative radiographic findings (lateral center-edge angle, alpha angle, and Tönnis grade), concomitant surgical procedures performed, preoperative and postoperative PROM scores, measures of clinical benefit, and secondary surgery performed (revision arthroscopic surgery, revision gluteal repair, and conversion to THA). The primary outcome was postoperative PROM scores; all other data were extracted if available. Data were collected and recorded in a premade Excel spreadsheet (Microsoft Office [Version 2011]; Microsoft) by 2 independent authors (S.M.P., T.K.), and conflicts in data extraction were resolved by a senior author (S.S.).
Results
Study Identification and Quality
After an initial search in PubMed, CENTRAL, and Scopus with the selected keywords, 404 studies were identified. After duplicates were removed, 270 studies were included for abstract screening. There were 11 studies selected for a full-text review. A total of 5 articles were included in the systematic review.5,9,21,24,27 Overall, 2 studies were level 4 case series,5,27 and 3 studies were level 3 cohort or comparative studies.9,21,24 The article selection process is detailed in Figure 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for article screening.
Study Characteristics
Table 2 lists the characteristics of the 5 studies included in the systematic review, including study period, MINORS score, sample size, sex, age, body mass index (BMI), and mean follow-up time. The study period ranged from 200821,24 to 2020. 21 A total of 223 hips were included between the 5 studies, with the mean follow-up time ranging from 26 9 to 74 24 months. The mean patient age ranged from 51 9 to 575,27 years. There were considerably more female (n = 207 [93%]) than male (n = 16 [7%]) patients in the study population. The mean BMI ranged from 27.7 24 to 28.8 21 kg/m2. The MINORS score ranged from 13 27 to 23. 9 Table 3 lists the preoperative radiographic measurements, intraoperative findings, and arthroscopic procedures performed.
Study Characteristics a

BMI, body mass index; F, female; LOE, level of evidence; M, male; MINORS, Methodological Index for Non-Randomized Studies.
Data are reported as mean, mean ± SD, or mean (range).
Preoperative Radiographic Measurements, Intraoperative Findings, and Arthroscopic Procedures a

Data are reported as n (%) or mean ± SD. ALAD, acetabular labrum articular disruption; AO, acetabular Outerbridge; FHO, femoral head Outerbridge; LCEA, lateral center-edge angle; NR, not reported.
Data missing for one patient with a partial-thickness tear.
Data missing for two patients with a partial-thickness tear.
43 patients met inclusion criteria, but only 37 patients were actually matched with controls.
PROM Scores
All studies reported scores for ≥1 PROMs, which are listed in Table 4. There were 3 studies9,24,27 that reported modified Harris Hip Score (mHHS) and Hip Outcome Score–Sports-Specific Subscale (HOS-SSS) scores, all of which found significant improvements from preoperatively to the latest follow-up. The Non-Arthritic Hip Score (NAHS) scores improved significantly in all cohorts for which they were reported.21,24,27 Horner et al 9 reported Hip Outcome Score–Activities of Daily Living (HOS-ADL) scores, which improved significantly from 51.7 ± 16.2 to 82.7 ± 15.6. Finally, all studies reported significant improvements in visual analog scale (VAS) pain scores at the latest time point.5,9,21,24,27 Of note, Chandrasekaran et al 5 displayed the preoperative and postoperative scores of 4 of 5 PROMs (mHHS, NAHS, HOS-ADL, HOS-SSS) graphically. The authors stated that all of these scores improved significantly from preoperative to all postoperative time points. 5
Preoperative and Latest Follow-up PROM Scores a
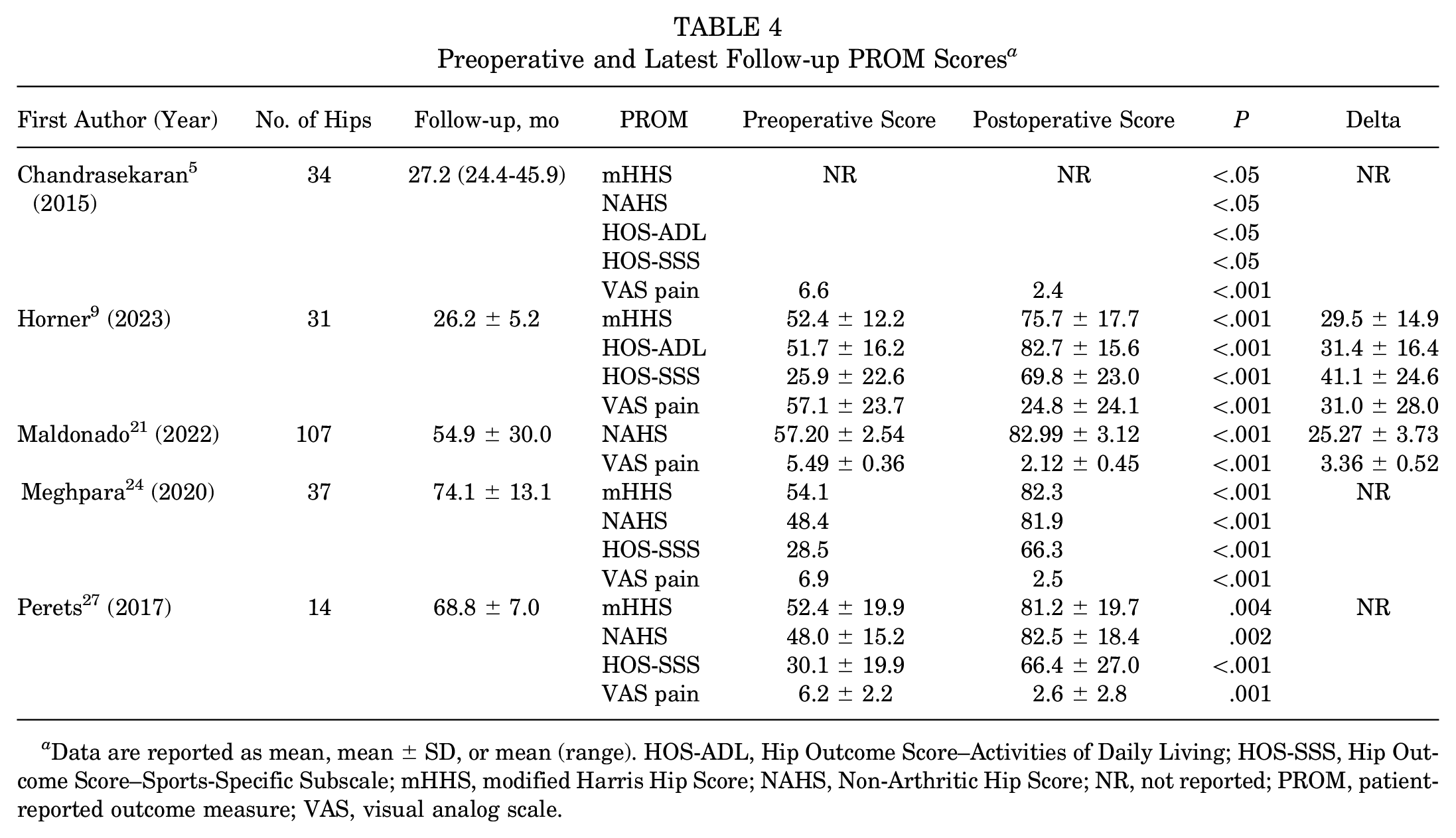
Data are reported as mean, mean ± SD, or mean (range). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; NR, not reported; PROM, patient-reported outcome measure; VAS, visual analog scale.
Achievement of Clinical Benefit
A total of 2 studies,9,24 comprising 68 hips, reported clinical psychometric thresholds including the minimal clinically important difference (MCID) and patient acceptable symptomatic state (PASS). Both studies reported greater than 70% of the cohort achieving the MCID for all PROMs. Meghpara et al 24 reported PASS achievement rates of 73.5%, 56.0%, and 67.6% for the mHHS, HOS-SSS, and International Hip Outcome Tool–12, respectively. Rates were lower in Horner et al’s 9 cohort at 40.7%, 50.0%, 40.9%, and 55.6% for the mHHS, HOS-ADL, HOS-SSS, and VAS pain, respectively. These findings are summarized in Table 5.
Rates of Achieving Measures of Clinical Benefit a

HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-12, International Hip Outcome Tool–12; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; PASS, patient acceptable symptomatic state; VAS, visual analog scale.
Data are reported as mean ± SD.
Secondary Surgical Procedures
Overall, 4 studies5,9,24,27 reported rates of secondary procedures, including revision abductor tendon repair, revision arthroscopic surgery, and conversion to THA. Meghpara et al 24 reported 1 case of revision abductor tendon repair at 32 months postoperatively. There were no secondary arthroscopic procedures reported. Conversion to THA occurred in 4 hips among Chandrasekaran et al’s 5 cohort and 1 hip in Perets et al’s 27 cohort. These findings are summarized in Table 6.
Secondary Surgical Procedures a

Data are reported as mean ± SD or No. THA, total hip arthroplasty.
Comparison With Control Groups
There were 2 studies9,24 that compared patients undergoing endoscopic gluteal repair with concomitant labral treatment to patients undergoing labral treatment alone. Horner et al 9 matched the main study group in a 1:3 ratio by sex, age, and BMI to patients who underwent isolated labral repair. They found that both groups experienced significant improvements in all PROM scores assessed. 9 In addition, there were no significant differences between groups in improvements in postoperative PROM scores, achievement rates of the MCID and PASS, or rates of revision hip arthroscopic surgery or conversion to THA. The authors noted a trend toward fewer cases of conversion to THA performed in the abductor tendon repair group (0.0%) compared with controls (4.4%), but this result did not reach statistical significance.
Meghpara et al 24 also included a control group of patients undergoing primary arthroscopic labral treatment alone. Whereas Horner et al 9 only included patients treated with labral repair, Meghpara et al’s 24 study consisted of any form of labral treatment, including debridement, reconstruction, and repair. They also utilized labral treatment type, acetabular Outerbridge grade, and femoral head Outerbridge grade as factors in the matching process, in addition to those used by Horner et al. 9 The authors reported that both groups demonstrated significant improvements from preoperative to latest follow-up time points on the mHHS, NAHS, HOS-SSS, and VAS pain. 24 Some notable differences were found between groups, including a significantly older mean age in the abductor tendon repair group. In addition, the abductor tendon repair group had significantly lower preoperative HOS-SSS scores and significantly higher preoperative VAS pain scores compared with controls. However, there were no significant differences between groups at the latest follow-up for all recorded PROM scores, and there were similar rates of achieving the MCID and PASS for all PROMs.
Comparison Between Abductor Tendon Repair Techniques
Chandrasekaran et al 5 performed a subanalysis of outcomes between partial-thickness tears (n = 17), which were repaired with a transtendinous technique, and full-thickness or near full-thickness tears (n = 17), which were repaired with a double-row suture bridge technique. There were no significant differences between treatment groups with respect to patient or other preoperative characteristics (other than the grade of gluteus medius tear), nor were there any significant differences in any PROM scores at the latest time point. There were 3 other studies that reported using the same repair techniques for partial- and full-thickness tears but did not explicitly compare the outcomes between groups.21,24,27 Finally, Horner et al 9 reported using a knotted single-row repair technique on all patients, regardless of the degree of tendon tear.
Discussion
The main findings of this systematic review were that (1) patients who underwent endoscopic abductor tendon repair with concomitant hip arthroscopic surgery for the treatment of intra-articular abnormalities demonstrated significant improvements (P < .05) on PROMs postoperatively, (2) outcomes were comparable with matched controls who underwent hip arthroscopic surgery alone without abductor tendon repair, and (3) there were low rates of secondary procedures including revision abductor tendon repair (0.9%) and conversion to THA (4.3%).
This review showed that primary endoscopic abductor tendon repair with simultaneous hip arthroscopic surgery resulted in improved PROM scores at time points from at least 2 years to over 5 years postoperatively. All 5 articles included in this review utilized multiple PROMs and found significantly improved scores for every PROM at the latest follow-up time point.5,9,21,24,27 Moreover, 2 studies reporting measures of clinical benefit found that over 70% of these patients achieved the MCID for all PROMs assessed.9,24 The results for achievement of the PASS were lower, particularly in Horner et al’s 9 study, which reported PASS achievement rates of 40.7% to 55.6% for the PROMs examined. This may be explained in part by the older mean ages of all groups included in this study relative to the mean age of a typical hip arthroscopic surgery cohort.4,26 Specifically, patients included in Horner at al’s 9 study exhibited several demographic risk factors for inferior outcomes after hip preservation surgery including older age (50.8 years), smoking status (22.6% of the cohort),13,14 concomitant low back pain (22.6% of the cohort), 19 psychiatric comorbidities (12.9% of the cohort), 30 and preoperative chronic hip pain for over 2 years (38.7% of the cohort). 16 As a result, the included cohort in their study consisted of patients with significant demographic factors for inferior outcomes after hip arthroscopic surgery and may have contributed to the lower rates of PASS achievement in this study. Interestingly, they found similar rates of PASS achievement in a matched group of patients undergoing isolated labral repair, indicating that demographic factors rather than the surgical procedure may have had an influence on outcomes. Overall, these findings are consistent with previous systematic reviews that suggest that both open and endoscopic approaches to abductor tendon repair result in improved clinically meaningful outcomes.1,6,20
The rates of secondary surgery among the included studies, including revision abductor tendon repair, revision hip arthroscopic surgery, and conversion to THA, were low. Among the 4 studies reporting secondary surgical procedures, comprising 116 hips, there were 5 cases (4.3%) of conversion to THA. Of these, 4 occurred in Chandrasekaran et al’s 5 study between 11 and 16 months after index surgery. The authors noted that this was likely caused by severe cartilage degeneration in these patients, given that all of them were found to have Outerbridge grade ≥3 changes in the acetabulum and/or femur intraoperatively. 5 The remaining case of conversion to THA occurred in Perets et al’s 27 cohort at 4.7 months after abductor tendon repair. Of note, these 2 studies had the oldest cohorts in this review (mean age ≥57 years), which is an age group that has been associated with worse outcomes after hip arthroscopic surgery.10,31,34 There were no secondary hip arthroscopic procedures reported in any of the included studies. Finally, there was a single case of revision abductor tendon repair in Meghpara et al’s 24 cohort, constituting a 2.7% revision rate in this particular study and a 0.9% total rate among the 4 studies in this review that reported secondary surgical procedures. These low revision rates are consistent with 2 previous systematic reviews investigating outcomes after endoscopic abductor tendon repair alone, which reported retear rates of 0% and 3.4%.1,20
A systematic review by Yee et al 35 previously demonstrated that there is a significant co-occurrence of intra-articular abnormalities and abductor tendon tears in patients with GTPS. The authors found that among patients undergoing endoscopic abductor tendon repair, over 85% and 25% had labral and chondral lesions identified, respectively. 35 The 2 studies included in the current review that compared simultaneous abductor tendon repair and labral treatment to labral treatment alone found no significant differences in improvements on PROMs postoperatively or achievement rates of the MCID and PASS between groups.9,24 While Horner et al 9 noticed a trend toward lower rates of secondary surgery in the abductor tendon repair group, including revision arthroscopic surgery and conversion to THA, this finding did not reach statistical significance.
Overall, these results suggest that endoscopic abductor tendon repair can be effectively paired with hip arthroscopic surgery for the treatment of concomitant abductor tendon tears and intra-articular abnormalities without compromising the therapeutic effect of hip arthroscopic surgery alone. However, given the high prevalence of labral tears in patients older than 50 years, 12 further studies are needed to identify which subset of patients with abductor tendon tears undergoing endoscopic repair is most likely to benefit from concomitant hip arthroscopic surgery and labral treatment. At present, as stated in an editorial by Domb and Curley, 8 this decision must be made on a case-by-case basis, guided by history, physical examination, and other diagnostic findings (eg, diagnostic injections) that suggest a primarily peritrochanteric versus intra-articular source of symptoms.
This systematic review has several strengths. First, the included studies reported multiple PROMs, which in turn increases the external validity of the results. Second, measures of clinical benefit were reported in 2 studies to qualitatively assess whether patients had successful outcomes after surgery. Third, the review included studies with mean follow-up times of at least 2 years and up to greater than 5 years postoperatively.
Limitations
There are also several limitations that should be acknowledged. First, the number of studies (n = 5) included in this review was relatively small. Second, 4 studies were conducted at the same institution, and there is therefore a risk of patient overlap between studies. Third, the article by Maldonado et al, 21 which accounted for 107 (48%) of the hips included in this review, did not report preoperative radiographic measurements or arthroscopic procedures performed. Fourth, the study periods ranged from 2008 to 2020, during which time surgical techniques may have changed or improved. Fifth, while 4 of 5 studies used consistent repair techniques for both partial- and full-thickness tears, Horner et al’s 9 study used an alternative method that may have influenced outcomes. Sixth, the overwhelming majority of the patients in the included studies were female, which may limit the generalizability of the findings to a cohort of male patients. Seventh, only 2 of the 5 studies included a control group with which to compare outcomes of the combined procedure. The control groups in these 2 studies included different intra-articular treatment methods, which may introduce heterogeneity. Eighth, we were unable to perform further statistical analyses (eg, forest plots) because of the heterogeneity of the PROMs used across the included articles. Finally, no studies included a cohort that underwent endoscopic gluteal repair without hip arthroscopic surgery.
Conclusion
Our systematic review demonstrated that patients who underwent concomitant endoscopic abductor tendon repair and hip arthroscopic surgery had significant improvements in PROM scores with low rates of secondary surgery at a minimum 2-year follow-up. Longer-term studies are needed for us to understand the concomitant treatment of multiple abnormalities in patients undergoing hip arthroscopic surgery in the future.
Footnotes
Final revision submitted February 8, 2025; accepted February 17, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.