
Abstract
Background:
Athletes who undergo an anterior cruciate ligament (ACL) reconstruction (ACLR) typically follow supervised rehabilitation before returning to sport. Return-to-sport (RTS) readiness is partially determined by RTS testing. It is not known how characteristics of the supervised rehabilitation episode of care relate to performance on RTS testing.
Purpose:
To compare high, average, and low performers on RTS testing among athletes after ACLR in regard to characteristics of their rehabilitation episode of care.
Study Design:
Case-control study; Level of evidence 3.
Methods:
Data from 262 athletes after ACLR (age 20.7 ± 6.7 years; 131 females) who underwent supervised rehabilitation and elective RTS testing were analyzed. Demographic data including the ACL Return-to-Sport Inventory (ACL-RSI) were gathered. RTS testing data included triple-hop symmetry, single-leg vertical jump symmetry, and an assessment of a repeated change-of-direction task for time, the Lower Extremity Functional Test. Athletes were classified as high or low performers if they were in the top (high performers) or bottom quartile (low performers) of at least 2 of the 3 performance measures. Episode of care characteristics included total supervised rehabilitation encounters, episode length, number of unique rehabilitation providers, and frequency of encounters in each quartile. Analyses of covariance with Bonferroni corrections were performed to assess between-group differences with age and sex as covariates.
Results:
Of the 262 athletes analyzed, 52 were classified as high performers and 46 were classified as low performers. Compared with high performers, low performers had a lower frequency of rehabilitation encounters in the third quartile (−0.39 visits per week; 95% CI, −0.60 to −0.18; P < .01) and fourth quartile (−0.34 visits per week; 95% CI, −0.54 to −0.14; P < .01). Compared with average performers, low performers had a lower frequency of rehabilitation encounters in the third quartile (−0.20 visits per week; 95% CI, −0.36 to −0.03; P = .04). The ACL-RSI score of the high performers was higher than that of average performers (+10.65; 95% CI, 4.17 to 17.12; P < .01) and low performers (+14.82; 95% CI, 6.70 to 22.95; P < .01).
Conclusion:
Athletes who performed well on RTS tests after ACLR had a significantly higher frequency of rehabilitation encounters during the second half of their rehabilitation episode. Supervised care during the later stages of rehabilitation may have contributed to the more favorable outcomes on RTS tests. Clinicians and patients should consider the timing and distribution of rehabilitation encounters when creating and modifying a plan of care.
Keywords
Athletes who undergo anterior cruciate ligament (ACL) reconstruction (ACLR) typically follow a rehabilitation program supervised by a physical therapist and/or athletic trainer. For athletes who wish to return to sport (RTS) after an ACLR, completion of supervised rehabilitation is associated with improved outcomes compared with unsupervised rehabilitation.11,24 Supervised rehabilitation for athletes after ACLR typically includes basic range of motion and strengthening in the earlier phases of rehabilitation. This is followed by the middle and later phases of rehabilitation, which typically begin around 4 months after surgery. The middle and later phases of rehabilitation have more emphasis on power, agility training, and conditioning.2,15 The middle phase of rehabilitation addresses impairments present after surgery, 4 whereas the later phase emphasizes preparing athletes for their sport. 3 The frequency and duration of supervised rehabilitation vary in published literature pertaining to ACLR rehabilitation.6,8 Incorporation of supervised rehabilitation in the later stages of recovery may confer additional benefits compared with discharging the athlete to a self-directed program8,10,20,32; however, supervised rehabilitation does not always occur in the real-world setting.6,8
RTS testing is often performed for athletes after ACLR to determine their readiness for returning to sport.2,5,15 RTS testing may include assessments of strength, power, and change-of-direction ability as well as other constructs specific to the athlete and their sport.5,26 Triple-hop testing and single-leg vertical jump testing are frequently used to assess muscular power and are correlated to strength.7,13,26,33 The Lower Extremity Functional Test (LEFT) is an example of a test used to assess change-of-direction ability. 25 Using multiple tests to better capture different constructs of athleticism may be superior to using any single test in isolation.17,26 Specific benchmarks or cut-offs for RTS tests are not clear.21,22 Performing well on RTS testing criteria is associated with improved reported outcomes12,19,30,37 and a lower rate of reinjury in some studies16,35; however, the results of other studies are mixed regarding the specific utility of RTS testing.1,22,23
Although evidence is available to support supervised rehabilitation throughout the entire recovery process for athletes after an ACLR, characteristics of the supervised rehabilitation needed for optimal recovery and RTS are not well established. It is not known how characteristics of the rehabilitation episode of care, such as the frequency, duration, or total number of rehabilitation encounters, may influence outcomes. The purpose of this study was to stratify athletes after ACLR who underwent RTS testing into high performers, low performers, and average performers and to compare the groups in regard to the characteristics of their supervised rehabilitation episode of care, including (1) total number of encounters, (2) episode length, (3) number of unique rehabilitation providers, (4) time between the last rehabilitation encounter and the RTS test, and (5) frequency of rehabilitation encounters in each quartile of the episode of care. Our hypothesis was that athletes who were high performers on RTS testing would have a greater number of rehabilitation encounters, a longer duration of episode length, a shorter time between rehabilitation and the RTS test, a lower number of unique rehabilitation providers, and a higher frequency of rehabilitation encounters.
Methods
Study Design
This was a retrospective cohort study of athletes who underwent ACLR surgery, associated supervised rehabilitation, and elective RTS testing at a single hospital-based rehabilitation system in the midwestern United States. Inclusion criteria included having a rehabilitation encounter related to an ACLR, age between 14 and 30 years, having completed RTS testing at our institution between December 2016 and July 2023, having completed elective RTS testing within 16 months of ACLR surgery, and having an episode length of at least 3 months. These inclusion criteria were implemented to allow representation of at least the minimum standards of care for rehabilitation after ACLR and to minimize the chances of missing data. Exclusion criteria included having <15 rehabilitation encounters associated with ACLR, evidence of a concomitant surgery beyond an isolated first-time ACLR besides a meniscectomy or lateral extra-articular tenodesis (identified through manual chart inspection), or incomplete documentation on RTS testing. Those with a concomitant surgery (including, but not limited to, meniscal repair and ACLR revision) were excluded because concomitant surgery would potentially influence outcomes and impair comparability. International Classification of Diseases, 10th Revision (ICD-10)–based database searches were performed, and potentially eligible cases were manually cross-referenced with RTS testing data. Before initiation of the study, the University of Michigan institutional review board approved this study (HUM00228060).
Athlete and Rehabilitation Characteristics
For athletes who passed the inclusion and exclusion criteria, the following demographic data were collected: age, sex, height, weight, surgical graft type, the time between surgery and the RTS test, and ACL Return-to-Sport Inventory (ACL-RSI) score. 9 The ACL-RSI is a 12-item questionnaire, scored 0 to 100, which assesses psychological readiness for those returning to sport from an ACL injury. 9 The rehabilitation characteristics collected included the total number of supervised rehabilitation encounters, the length of the episode of care (months), the number of unique rehabilitation providers (including physical therapists, physical therapist assistants, and athletic trainers), the time (days) between the last rehabilitation encounter and the RTS test, and the calculated frequency of rehabilitation encounters (visits per week) for each quartile of the episode of care. The episode of care was defined as the time between the first and last rehabilitation encounter. To identify the frequency of rehabilitation encounters for each quartile, the number of rehabilitation encounters in each quartile was divided by 25% of the total episode of care duration. This was converted to encounters per week for standardization and comparison purposes.
Return-to-Sport Testing
RTS testing was elective, and the timing was at the discretion of the rehabilitation provider and the orthopaedic surgeon. RTS testing was performed by trained rehabilitation providers within the rehabilitation system and included a dynamic warm-up followed by a battery of physical performance tests. The data extracted from RTS testing included 3 physical performance measures: the LEFT, the limb symmetry index (LSI) of the triple-hop test, and the LSI of the single-leg vertical jump. These tests were chosen because they represent different constructs related to athleticism and have high levels of reliability.13,25 The LEFT consists of the athlete performing a frequent change-of-direction task for time and assesses athletic constructs of change-of-direction ability and conditioning. 25 The LEFT set-up has 4 cones spaced equally apart on a level surface, and the athlete is required to perform 16 predefined change-of-direction tasks, which include forward running, backward running, and shuffling. 25 The triple-hop test is widely used in RTS testing and consists of the athlete hopping forward 3 times before sticking their landing on the same foot.5,26 The single-leg vertical jump has gained popularity in RTS testing recently because it is more specific and sensitive to deficits related to ACLR compared with traditional horizontal hop tests.7,13,14,29,34 This test consists of the athlete jumping vertically as high as possible on 1 leg, and the height attained is collected. The LSI is the ratio of the output of each test on the surgical and nonsurgical side, and this was calculated for both the triple-hop test and the single-leg vertical jump.
Statistical Analysis
Statistical analysis was performed using R Version 4.3.0 (R Core Team, 2023). Athletes were first categorized as high performers or low performers if their performance in at least 2 of the 3 physical performance measures assessed was in the highest (high performers) or lowest (low performers) quartile of the entire data set. This novel categorization of high performers and low performers was used in this study based on previous research demonstrating the construct validity of using multiple tests rather than single tests in isolation to identify RTS readiness.17,26 Athletes were categorized as average performers if they did not meet the classification of high or low performers. Basic descriptive statistics for demographic characteristics, episode of care, and RTS testing were collected, including means and standard deviations for all continuous variables. Demographic information was compared between groups with analyses of variance. Analyses of covariance with Bonferroni corrections were performed to assess the between-group differences in rehabilitation episode characteristics, with age and sex as covariates. Post hoc comparisons between groups were performed for significant findings. Statistical significance was defined as P < .05.
Results
A total of 262 athletes were included (Figure 1) in the analysis. Of these, 52 (19.8%) athletes were classified as high performers and 46 (17.6%) were classified as low performers. Descriptive statistics including demographic information of each group as well as the entire cohort are depicted in Table 1. RTS test results are depicted for each group in Table 2. Descriptive statistics of episode characteristics are depicted in Table 3. No significant differences were found between groups in height, weight, body mass index, or time since surgery. We noted a higher proportion of males in the high performers group (71%) compared with low performers (45%), average performers (44%), and the overall cohort (50%). The ACL-RSI score of the high performers was significantly higher than that of average performers (+10.65; 95% CI, 4.17 to 17.12; P < .01) and low performers (+14.82; 95% CI, 6.70 to 22.95; P < .01). Analyses of covariance with Bonferroni corrections revealed significant differences between the high performers and the low performers, with the low performers having a lower frequency of rehabilitation encounters during both the third (−0.39 visits per week; 95% CI, −0.60 to −0.18; P < .01) and fourth (−0.34 visits per week; 95% CI, −0.54 to −0.14; P < .01) quartiles of rehabilitation. A significant difference was found between the low performers and average performers, with the low performers having a lower frequency of rehabilitation encounters during the third quartile of rehabilitation (−0.20 visits per week; 95% CI, −0.36 to −0.03; P = .04). The frequency of visits for low, high, and average performers over each quartile is depicted in Figure 2. The differences between groups for visits per week during the first 2 quartiles were not statistically significant. No significant differences were found for the number of visits or number of unique rehabilitation providers between groups (Table 2).

Flowchart of participant selection. ACLR, anterior cruciate ligament reconstruction.
Descriptive Statistics of High, Low, and Average Performers on Return-to-Sport Testing After Anterior Cruciate Ligament Reconstruction a

Data are presented as n or mean ± SD. ACL-RSI, Anterior Cruciate Ligament Return-to-Sport Inventory; BMI, body mass index; NA, not applicable.
Return-to-Sport Test Results for High, Low, and Average Performers a
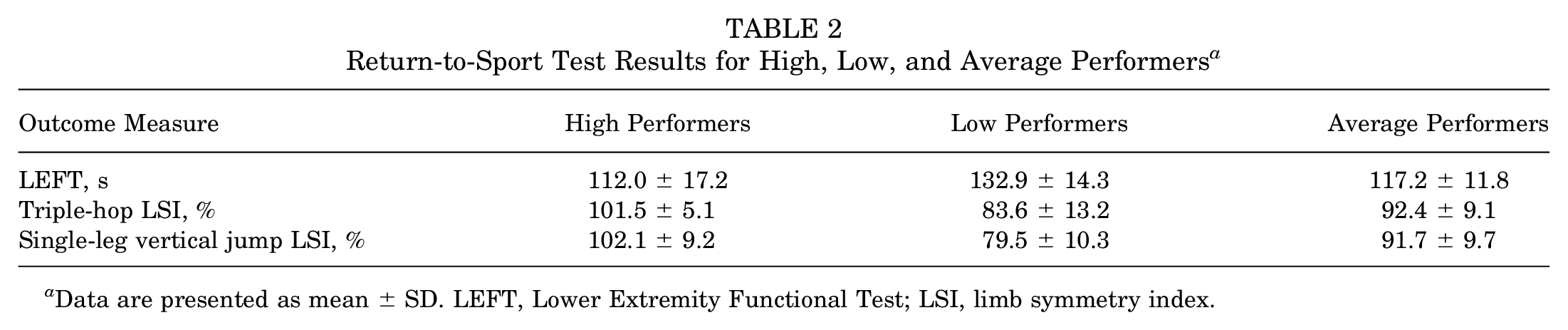
Data are presented as mean ± SD. LEFT, Lower Extremity Functional Test; LSI, limb symmetry index.
Episode Characteristics for High, Low, and Average Performers a
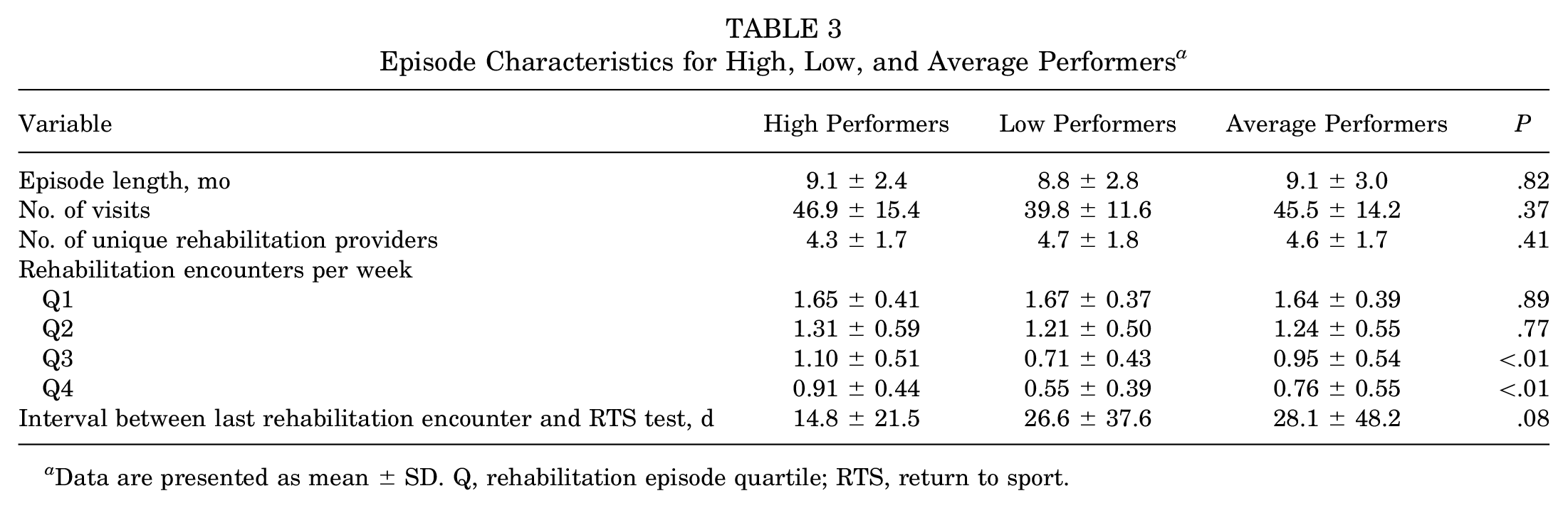
Data are presented as mean ± SD. Q, rehabilitation episode quartile; RTS, return to sport.
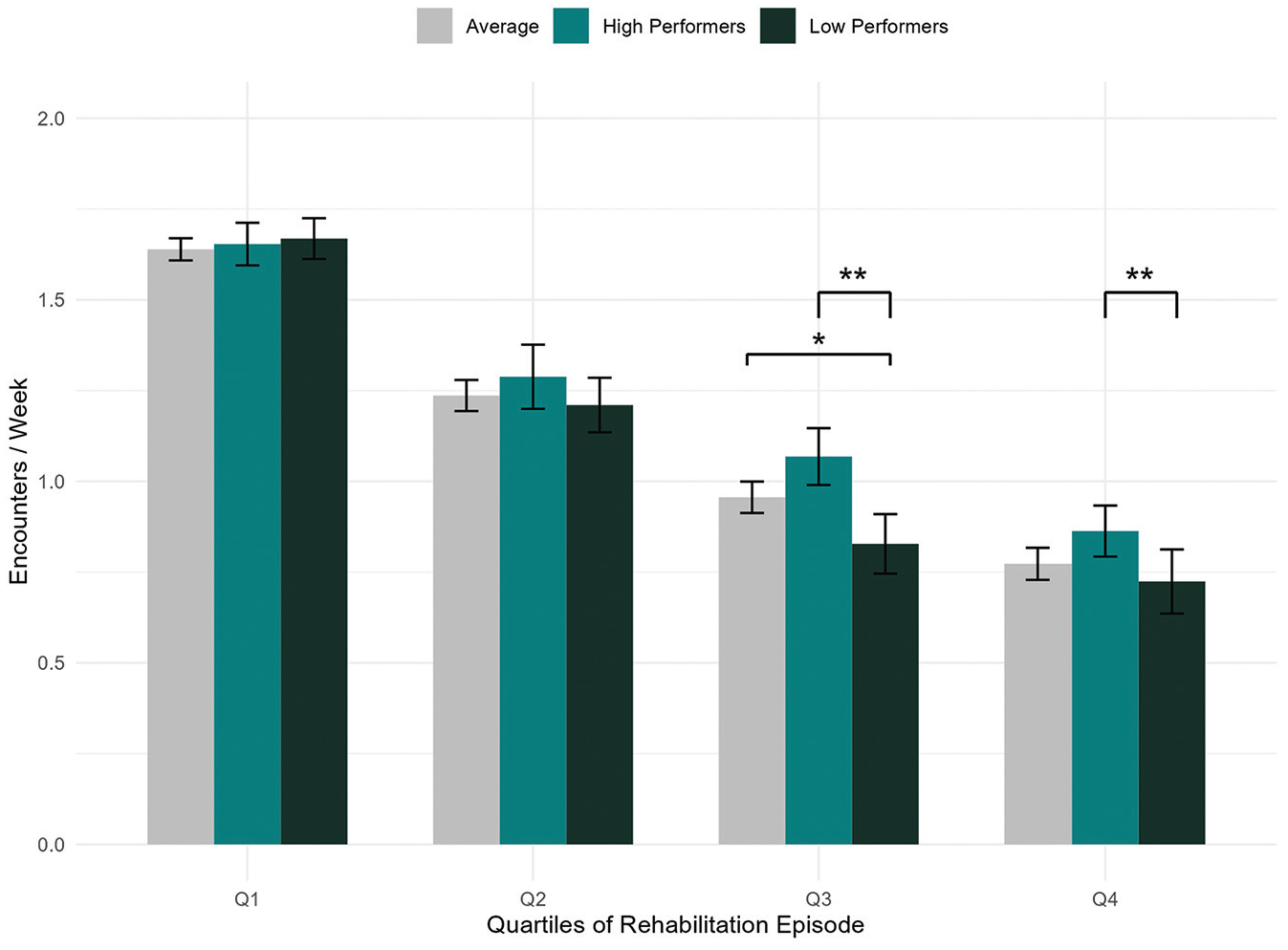
Frequency of supervised rehabilitation encounters over the episode of care for low, average, and high performers on return-to-sport tests after anterior cruciate ligament reconstruction in the third and fourth quartiles of the rehabilitation episode. *Significance <.05. **Significance <.01.
Discussion
The results of this study demonstrated a significantly higher frequency of rehabilitation encounters during the later stages (third and fourth quartiles of the episode of care) of rehabilitation of athletes who were classified as high performers on RTS testing compared with those who were classified as low performers. High performers on ACL RTS testing had 1.10 and 0.91 rehabilitation encounters per week in the third and fourth quartiles of their rehabilitation episode, respectively, compared with 0.71 and 0.55 for low performers (P < .01). Other variables, including the total number of rehabilitation visits, episode length, days between the last rehabilitation encounter and the RTS test, and number of unique rehabilitation providers, were not statistically different between groups.
Previous research suggests that supervised rehabilitation episodes that are of longer duration seem to result in superior outcomes compared with shorter ones for athletes recovering from ACLR.8,20,32 The difference in frequency of supervised rehabilitation encounters in the second half of the episode of care in high-performing athletes after ACLR compared with low-performing athletes is a novel finding of this study. The magnitude of this finding is highlighted by the unequal distribution of rehabilitation encounters skewed toward the early stages of rehabilitation, which is common in ACLR rehabilitation. 6 The content and focus of rehabilitation in the early and late stages of ACLR rehabilitation differ substantially. Earlier stages of ACLR rehabilitation typically focus on managing effusion, normalizing range of motion, restoring volitional quadriceps activity, and basic strengthening. 4 In contrast, later stages of rehabilitation for athletes after ACLR have an emphasis on high-load strength training, impact training, and agility. 3 The constructs of rehabilitation in later stages are notably similar to the RTS tests used in this study. One explanation for the findings of this study is that supervision and guidance for these constructs result in improved performance compared with self-directed or unsupervised rehabilitation. Surgeons and rehabilitation providers may wish to consider the frequency of supervised rehabilitation throughout the entire recovery process to maximize outcomes in athletes after ACLR. This is further emphasized by the lack of significant differences in the total number of rehabilitation encounters between groups found in this study and the trend toward a relationship between the time since the last rehabilitation encounter and the RTS test. Future prospective research assessing the relationship between the distribution of supervised rehabilitation as well as the quality of rehabilitation (such as incorporation of agility or impact training) will be of benefit.
It is unclear why the high performers in this study had a greater frequency of supervised rehabilitation encounters in the later stages of rehabilitation. Many factors can influence rehabilitation attendance, including socioeconomic factors; the goals, beliefs, and fears of the athlete; and the relationship the athlete has with the rehabilitation provider.27,28 We did not assess these variables and our study used a retrospective design, which dampens any suggestion of a causal relationship. The full scope of the relationship between athletes after ACLR, their situation (such as financial status, access to care, insurance limitations, psychological and social status), and the rehabilitation experience has with outcomes after surgery is not clear.
Athletes who were classified as high performers on RTS tests in this study had significantly higher ACL-RSI scores, signifying better psychological readiness for sport, compared with average and low performers. Previous research evaluating the relationship between RTS testing and psychological readiness is mixed.33,36,38 It is possible that the frequency of supervised rehabilitation during the later stages of rehabilitation influenced psychological readiness. Given the lack of a clear relationship between RTS testing and psychological readiness, it is possible that nonspecific factors of supervised rehabilitation, such as the relationship the athlete has with the rehabilitation provider, may positively influence outcomes in athletes after ACLR. 18 We did not directly assess such nonspecific factors, but they may be worthy of future consideration given the value of psychological readiness for predicting future function and reinjury. 9
The strengths of the study include a large sample size and use of multiple performance measures. However, the retrospective study design is a notable limitation. This precludes the ability to infer causal relationships and increases the risk of a selection bias favoring those who completed an elective RTS test. This study demonstrated a relationship between the frequency of supervised rehabilitation encounters in the later stages of rehabilitation and performance on RTS testing, but the actual rates of RTS, return to performance, and reinjury for the population studied are not known. Further, the test battery and categorization strategy used in this study rely heavily on the LSI of hop and jump testing. The test battery and categorization strategy notably do not include quadriceps strength assessment or standardized patient-reported outcomes, which carries limitations regarding assessment of RTS readiness. 31 The categorization of high, average, and low performers used in this study has not been validated in regard to long-term performance or health outcomes, further limiting the interpretation of the results in this study. All athletes in this study underwent supervised rehabilitation within a single hospital system in the United States. This enhances the consistency of care between athletes but may limit the generalizability of the findings to other settings or regions of the world. Finally, this study did not account for other variables that may influence outcomes, such as access to additional outside resources, financial status, and sporting level.
Conclusion
Athletes who performed well in RTS tests after ACLR had a significantly higher frequency of rehabilitation encounters during the second half of their rehabilitation episode. Supervised care during the later stages of rehabilitation may have contributed to more favorable outcomes on RTS tests. Clinicians and patients should consider the timing and distribution of rehabilitation encounters when creating and modifying a plan of care.
Footnotes
Acknowledgements
The authors acknowledge and appreciate the contributions of Darlene Yao, Tyler Bolley, and Jessica Kellum toward this project.
Final revision submitted January 7, 2025; accepted February 3, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Michigan Institutional Review Board (HUM00228060).