
Abstract
Background:
Descriptive parameters for the evaluation of the labrum’s appearance on magnetic resonance imaging (MRI) after capsulolabral repair are not well established.
Purpose:
To assess the morphology and structural appearance of the postoperative glenoid labrum on MRI in athletic patients with anterior glenohumeral instability.
Study Design:
Case series; Level of evidence, 4.
Methods:
This prospective study examined MRI scans of the involved shoulder in a population of 27 athletic patients with traumatic anterior instability before arthroscopic capsulolabral repair and at 3 and 6 months after surgery. The morphology, axial height, coronal height, axial angle, coronal angle, integrity, and homogeneity of repaired capsulolabral tissue were evaluated. The labrum was considered healed if it was integrated or intact (ie, if there was no discontinuity between the labrum and the glenoid). For each of these variables, a comparison was made between the MRI scans preoperatively and at 3 and 6 months after surgery to verify significant differences in these measures. Linear and logistic regression models were built to verify the associations between exposure variables and outcome variables. For all analyses, a significance level of .05 was used.
Results:
Each continuous outcome variable (ie, morphology, angle, and height) showed statistically significant differences across the 3 different MRI time points, indicating that we observed an increase in height and angle as well as an improvement in morphology throughout the follow-up period. Integrity was not significantly different on MRI between 3 and 6 months. Homogeneity was not significantly different between preoperative and 3-month MRI but significantly differed between preoperatively and 6 months postoperatively. The difference between postoperative and preoperative coronal height (increase in height) was associated with the occurrence of multiple dislocation episodes. Advanced age or multiple dislocations reduced the improvement in morphology. At 6 months, the integrity of the labrum on MRI was observed in all patients; however, 17 patients (63%) still had a heterogeneous labrum. Patients who underwent surgery within 90 days or those with a first dislocation episode had better integrity and homogeneity of labral tissue.
Conclusion:
There were statistically significant differences in the morphology, height, and angle of the labrum between the preoperative and postoperative periods in patients who underwent arthroscopic repair for glenohumeral instability. Although a 6-month MRI revealed labral integrity in all the athletes, 63% still had heterogeneous labral tissue.
Traumatic anterior shoulder instability is a common condition, especially in young athletes.13,17 The incidence of dislocations can reach 23 cases per 100,000 people per year and is most common in male and White patients. 16 The recurrence of shoulder instability is related to a younger age at the time of the first episode and the presence of associated bone lesions.14,15 Surgical treatment, when performed, has success rates close to 96%, and arthroscopic repair is the most commonly used approach today.4,6,18,19,24
Returning to physical activity is often allowed after 4 to 6 months, depending on demand and the type of activity.12,29 This decision is made after functional evaluations of the strength and range of motion of the shoulder joint. Although magnetic resonance imaging (MRI) is a validated method for analyzing labral morphology, it is not routinely used to examine the integrity of capsulolabral repair, unlike the use of computed tomography to assess bone consolidation after the surgical bone block technique for shoulder instability. 11 Few studies have assessed labral integrity and morphology on imaging in patients with anterior glenohumeral instability undergoing arthroscopic repair.13,27,28,30,31
The aim of the present study was to examine the morphology and appearance of the labrum on MRI preoperatively and at 3 and 6 months after arthroscopic capsulolabral repair for traumatic anterior glenohumeral instability in athletic patients. Changes in MRI findings and measured variables were examined for correlations with patient and injury characteristics within the population. We hypothesized that morphometric MRI analysis of arthroscopic capsulolabral repair would show progressive differences in the labrum between 3 and 6 months and that the labrum would be healed at 6 months.
Methods
Participants
This prospective clinical study was conducted with 46 patients with traumatic anterior instability who underwent surgery between January 2021 and December 2022. Overall, 27 patients met the inclusion criteria and comprised the study population for analysis (Figure 1).

Flowchart showing the number of patients included in the study.
The inclusion criteria were as follows: (1) traumatic anterior dislocation, (2) positive physical examination findings for anterior instability, and (3) anterior and inferior capsulolabral lesions on preoperative MRI. The exclusion criteria were as follows: (1) glenoid bone lesion >20%, (2) off-track lesion, (3) associated rotator cuff injury, (4) associated posterior labral lesion, (5) humeral avulsion of the glenohumeral ligament lesion, (6) multidirectional or posterior instability on a clinical evaluation, (7) generalized ligamentous laxity (Beighton score >4), 5 (8) advanced arthrosis (grade 2 or 3 according to the Samilson and Prieto classification), and (9) no agreement to participate in the study. The exclusion criteria applied after enrollment were associated injuries found intraoperatively (such as rotator cuff tears and posterior labral tears) and loss to follow-up.
All included patients were athletes, as defined according to Araújo and Scharhag. 3 The types of sport were categorized according to Allain et al 1 into neutral (without contact and throwing), collision/contact, and throwing sports. These athletes had the following characteristics: the mean age was 31.07 ± 8.42 years, 23 (85.19%) were male, 18 (66.67%) had right shoulder injuries, 13 (48.15%) had a duration of injury of up to 90 days, and 19 (70.37%) had multiple dislocation episodes. Regarding the type of sport and the level of competition, 10 athletes (37.04%) practiced throwing sports, 11 (40.74%) practiced contact sports, and 20 (74.07%) were amateurs (Figure 2). This study was approved by the ethics and research committee of our university (No. 46089221.7.0000.5505), and patients provided informed consent.

Distribution of sports practiced by athletes.
Surgical Procedure
All surgical procedures were performed by a single surgeon with general anesthesia and a brachial plexus interscalene block. In the lateral decubitus position, the arm was suspended in 45° of abduction with 3 kg of longitudinal traction. All patients were examined under anesthesia, as described by Ejnisman et al, 12 to observe inferior, anterior, and posterior translation. Surgery was performed arthroscopically with a 4 mm–diameter 30° arthroscope. One posterior portal and 2 anterior portals were formed. Double-loaded 3.0-mm knot-tying suture anchors were used (SutureTak; Arthrex). Anterior labral repair was performed after labral detachment and debridement of the anterior glenoid edge using a shaver blade through the anteroinferior portal while the arthroscope was positioned in the anterosuperior portal. The bioabsorbable anchors were placed at the 5:30, 4:00, and 3:00 clockface positions on the right side, and arthroscopic sliding knots were made (Figure 3).
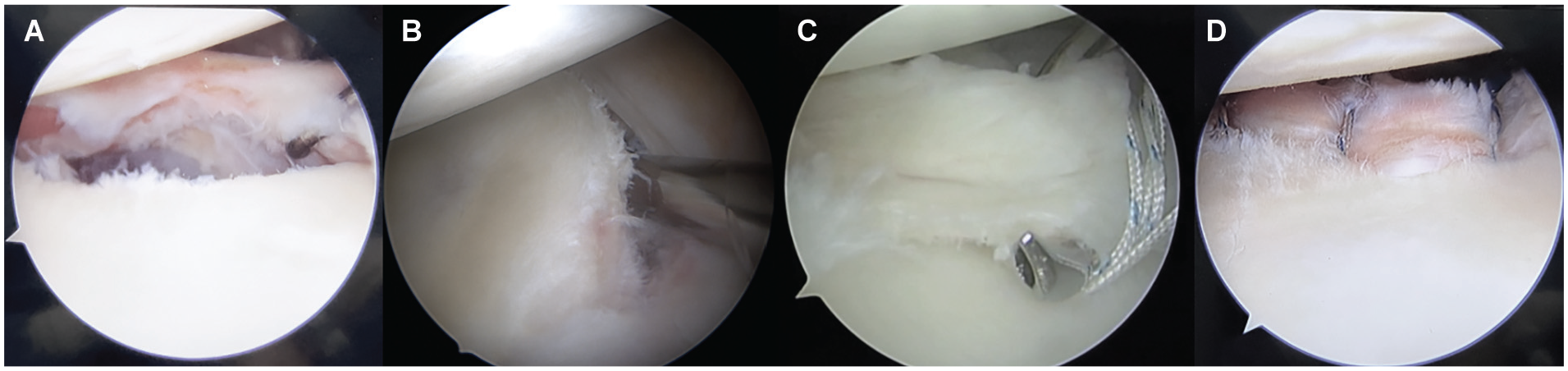
Intraoperative photographs of a left shoulder showing (A) a capsulolabral lesion; (B) labral detachment and scarring of the anterior glenoid rim, viewed from the anterosuperior portal; (C) passage of the suture passer through labral tissue; and (D) capsulolabral tissue repaired with stitches.
Postoperative Rehabilitation
After the procedure, the operated shoulder was placed in a simple sling for 6 weeks. Passive movements were initiated in the third week, avoiding abduction and lateral rotation >30° until the sixth week. Strengthening exercises were started at 10 weeks, and return to contact or collision sports was allowed only at 6 months. 26
Imaging Evaluation
MRI evaluations of the labrum were performed according to the established and validated protocol of Yoo et al. 30 A 1.5-T MRI scanner (Signa Explorer; GE HealthCare) with a dedicated coil for shoulder examinations was used in all patients. Images were obtained in 4 mm–thick slices with a 1-mm interval between slices. The arm was kept at the side of the trunk, and the shoulder was kept in neutral rotation with the thumb pointing upward. Axial transverse T2-weighted images and oblique coronal T2-weighted images were obtained. All measurements were performed on a picture archiving and communication system via the RadiAnt program.
The following were analyzed by MRI: morphology, axial height, coronal height, axial angle, and coronal angle. Labral morphology was measured in the same T2-weighted sequence and graded from 0 to 3 according to the descriptive validated method of Randelli et al 25 (Figure 4).

Randelli classification for labral morphology.
An additional 2 outcome variables were integrity and homogeneity, both of which were defined on the basis of morphology according to the Randelli classification. Integrity was defined as follows: the repair construct was considered intact (normal integrity) if the morphology grade was 0, 1, or 2; it was considered nonintact (altered integrity) if the grade was 3 or if there was discontinuity between the labrum and the glenoid (Figure 5). We considered a healed labrum as a labrum with integrity. Homogeneity was defined as a morphology grade of 0, and heterogeneity was defined as a morphology grade of 1, 2, or 3 (Figure 6).

Randelli classification. Intact labrum: grade 0, 1, or 2. Nonintact labrum: grade 3.

Randelli classification. Homogeneous labrum: grade 0. Heterogeneous labrum: grade 1, 2, or 3.
The parameters (morphology, height, and angle) were measured on axial and coronal oblique images at the anteroinferior portion of the glenoid, immediately above the lowest anchor, avoiding the site of the labrum where the suture was located to preclude being interpreted as a lesion. Height was defined as the distance (in mm) from the bottom of the glenoid to the top of the labrum’s tip (Figure 7). Angulation (slope) was defined as the angle formed by a tangential line drawn from the deepest portion of the glenoid (center of the glenoid) to the tip of the highest point of the labrum (Figure 8). Measurements were taken by an experienced musculoskeletal radiologist, who performed all examinations of the patients.
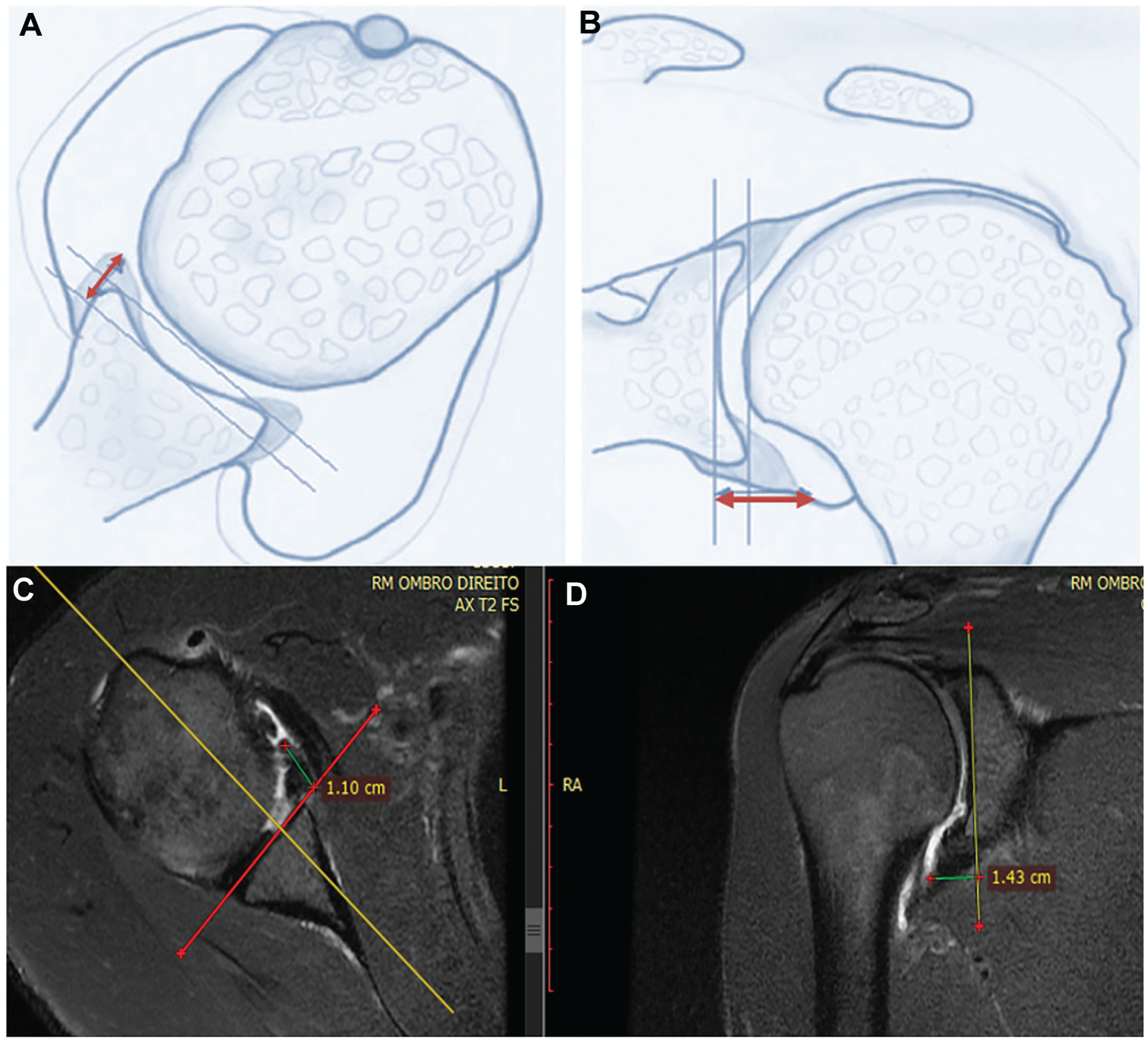
(A, B) Illustration of the method for measuring labral height on axial and coronal sections. (C, D) Magnetic resonance imaging of the method for measuring labral height on axial and coronal sections.

(A, B) Illustration of the method for measuring labral angle on axial and coronal sections. (C, D) Magnetic resonance imaging of the method for measuring labral angle on axial and coronal sections.
Statistical Analysis
A descriptive analysis of the data was performed for the exposure variables. Categorical data are expressed as absolute numbers and percentages, and continuous data are expressed as means ± standard deviations. For each outcome variable, a comparison was made between preoperative, 3-month, and 6-month MRI to assess whether there was a significant difference between the measures. The Shapiro-Wilk test revealed that these variables did not follow a normal distribution, which precluded the use of analysis of variance for mean comparisons. As an alternative, the Friedman test was used for continuous variables, and the Cochran test was used for the categorical variables of integrity and homogeneity.
A power analysis was performed using simulations. Clinically different results were considered changes of at least 2 mm for axial/coronal height, 5° for axial/coronal angle, and 1 point for morphology, as published in previous studies.30,31 The simulations used sample standard deviations, a sample size of 27, and a significance level of .05. For all outcomes, the estimated power was at least 0.8.
Regression models were constructed to verify associations between exposure variables and each outcome variable. Linear regression models were constructed for morphology, axial height, coronal height, axial angle, and coronal angle. Logistic regression models were constructed for integrity and homogeneity. The determination of relevant exposure variables for each outcome was made by adjusting all possible models and checking the one with the best score according to the Akaike information criterion. Assumptions such as multicollinearity, the existence of influential points, heteroscedasticity (for linear regression models), and the distribution of model residuals were verified in all regression models. No assumptions were violated. A significance level of .05 was set for all analyses.
Results
All patients underwent MRI preoperatively and at 3 and 6 months postoperatively. There were no reinjuries or the recurrence of instability during the 6-month postoperative period. Patient data are summarized in Table 1.
Patient Characteristics (n = 27)

Table 2 compares the MRI measurements obtained at the 3 study time points. There were significant differences between the preoperative, 3-month, and 6-month time points. At those time points, labral morphology on MRI according to the Randelli classification was 2.52 ± 0.58, 1.52 ± 0.58, and 0.70 ± 0.61, respectively. Preoperatively and at 3 and 6 months, the axial height was 8.23 ± 2.91, 9.72 ± 2.24, and 10.60 ± 2.86 mm, respectively. The preoperative, 3-month, and 6-month coronal height was 9.34 ± 2.36, 10.50 ± 2.06, and 11.40 ± 1.83 mm, respectively. The axial angle preoperatively and at 3 and 6 months was 26.30° ± 7.83°, 29.70° ± 7.00°, and 30.60° ± 7.26°, respectively, and the coronal angle was 24.10° ± 5.04°, 25.30° ± 3.94°, and 27.00° ± 3.36°, respectively. For all outcome variables, the differences were statistically significant over time (P < .05). Special attention should be given to the axial angle variable, as the P value was very close to .05.
Measurements of Outcome Variables a

Data are shown as mean ± SD.
The Friedman test.
For morphology, axial height, and coronal height, the measurements at all the time points differed from each other. There was no difference in the coronal angle and axial height between preoperatively and 3 months postoperatively. The axial angle did not differ over time; however, this variable had a P value very close to the limit of .05 (Table 3).
Differences in Measurements of Outcome Variables a
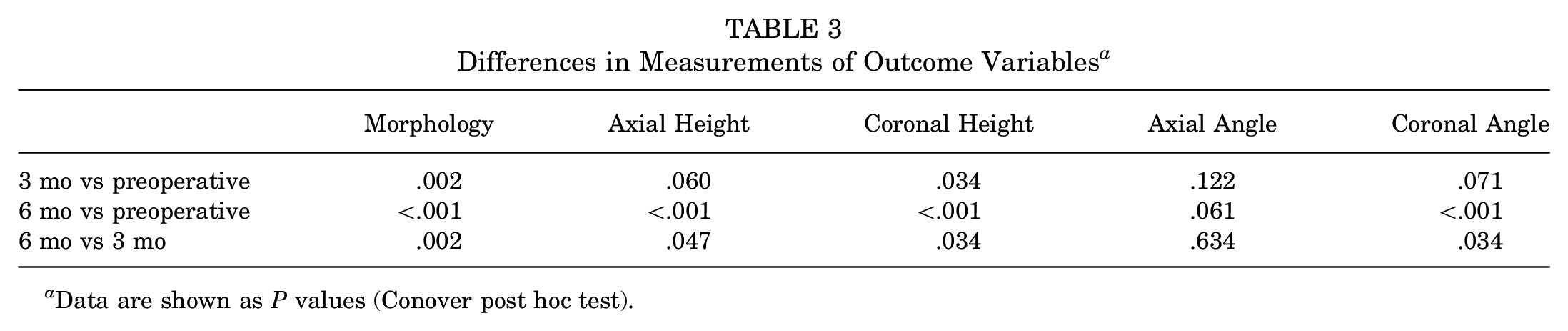
Data are shown as P values (Conover post hoc test).
Table 4 shows the results of the integrity and homogeneity variables at different time points. There were significant differences in both the proportion of patients with an intact (integrity) labrum and the proportion of patients with a homogeneous labrum. We also determined pairwise which time point(s) differed from the others (Table 5).
Integrity and Homogeneity Variables a

Data are shown as n (%).
The Cochran test.
Differences in Integrity and Homogeneity Variables a

Data are shown as P values (McNemar post hoc test).
For the integrity variable, there were no differences in the observed proportion of patients between 3 and 6 months postoperatively. For the homogeneity variable, there were no differences in the observed proportion of patients between preoperatively and 3 months, but there was a significant difference between preoperatively and 6 months postoperatively.
At 6 months, labral integrity was present in all patients, although 17 patients (63%) had a heterogeneous labrum (Figures 9-11). For each continuous outcome variable, a linear regression model was applied to examine for associations with the exposure variables. Axial height, coronal height, and axial angle had no relationship with any of the exposure variables. Associations between exposure variables and the preoperative to postoperative improvement in morphology were also analyzed. Multiple dislocations reduced the improvement in morphology (Table 6).
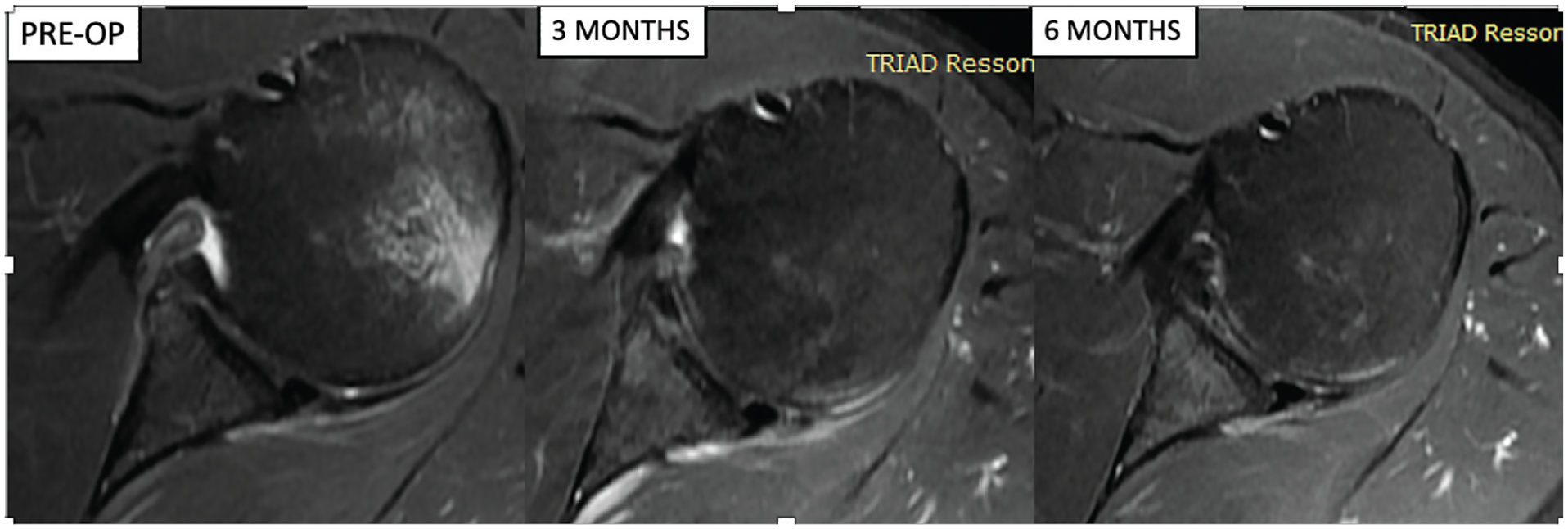
Axial magnetic resonance imaging showing a detached and nonintact labrum preoperatively, an intact and heterogeneous labrum (nodular hyperintensity; grade 1) at 3 months, and an intact and homogeneous labrum (grade 0) at 6 months.

Axial magnetic resonance imaging showing a detached and nonintact labrum preoperatively, an intact and heterogeneous labrum (linear hyperintensity; grade 2) at 3 months, and an intact and heterogeneous labrum (nodular hyperintensity; grade 1) at 6 months.

Axial magnetic resonance imaging showing a detached and nonintact labrum preoperatively, an intact and heterogeneous labrum (linear hyperintensity; grade 2) at 3 months, and an intact and homogeneous labrum (grade 0) at 6 months.
Regression Model for Difference in Morphology Between Preoperatively and 6 Months a

R2 = 0.3132.
The difference between preoperative and postoperative coronal height (increase in height) was associated with the occurrence of multiple dislocation episodes (Table 7). An increase in coronal height was associated with the occurrence of a single dislocation episode, indicating that patients who experienced a first dislocation episode tended to have a greater increase in coronal height at 6 months.
Regression Model for Difference in Coronal Height Between Preoperatively and 6 Months a

R2 = 0.11.
The preoperative coronal angle was associated with the time from injury to surgery and the occurrence of multiple dislocation episodes. The associations between exposure variables and the preoperative to postoperative improvement in the angle (labral slope) were analyzed. Patients treated within 90 days of the injury and those who did not practice contact sports had greater increases in the coronal angle.
Discussion
This prospective MRI study examined parameters with respect to labral morphology, height, angle, integrity, and homogeneity preoperatively and postoperatively in an athletic population with traumatic anterior shoulder instability, and we demonstrated that there were statistically significant differences in MRI measurements between these time frames. These differences were observed for variables such as morphology, axial height, coronal height, axial angle, coronal angle, homogeneity and integrity.
There was a progression in labral homogeneity at 6 months compared with 3 months. Although all patients in our study had integrity (healing) of capsulolabral tissue at 6 months, 63% still had a heterogeneous labrum; this characteristic was more predominant in patients with multiple dislocation episodes and those who underwent surgery more than 90 days after the trauma.
In our study, we observed that the preoperative coronal angle was associated with the time from injury to surgery and the occurrence of multiple dislocation episodes. An increase in the coronal angle was associated with the time from injury to surgery and the type of sport practiced. Patients who underwent surgery within 3 months and those with only one dislocation had a lower preoperative coronal angle. Perhaps those who seek surgery more quickly (within 90 days) are more likely to have more severe injuries and thus have a lower coronal angle. During the postoperative period, patients who underwent surgery within 90 days and those who did not practice contact sports had a greater increase in the coronal angle after labral repair.
Cohen et al 10 retrospectively evaluated graft consolidation in patients with anterior shoulder instability who underwent the Latarjet procedure. Bone resorption of the coracoid graft was present in at least 50% of the patients who underwent the Latarjet procedure, and the absence of significant preoperative glenoid bone loss was shown to be the only risk factor associated with severe graft osteolysis, even though this did not significantly influence the clinical outcome. Unlike techniques in which bone blocks are incorporated for stabilization, such as the Latarjet procedure, and computed tomography can be used to evaluate graft consolidation, there are no well-established imaging parameters for evaluating labral morphology and labrum healing in capsulolabral repair. Such parameters would provide objective factors to safely allow patients to return to their physical activities, especially professional athletes. In our study, labral density at 6 months was associated with the occurrence of multiple dislocation episodes. Patients with multiple dislocations were less likely to have a homogeneous labrum at 6 months after surgery. Although 6-month MRI revealed labral integrity in all the athletes, 63% still had a heterogeneous labrum. These data should be interpreted with caution when utilizing MRI for the evaluation of capsulolabral repair healing to avoid interpreting the injury as a new injury or the absence of labrum healing.
In our study, there was a statistically significant difference between all postoperative and preoperative measurements. An improvement in morphology was associated with age and the occurrence of a single dislocation. Generally, older age and lower preoperative morphology grades indicate less severe injuries; younger patients may be more prone to severe injuries. In the postoperative period, older age or multiple dislocations reduced the improvement in morphology, indicating that younger patients and/or those with only one dislocation tended to have greater improvement. Similarly, an increase in coronal height was associated with the occurrence of a single dislocation, indicating that patients with a first-time dislocation tended to have a greater increase in coronal height at 6 months. Yoo et al, 30 in their case-control study analyzing the parameters of glenoid labral morphology, compared preoperative, 6-week, and 6-month MRI scans of 3 groups of 21 shoulders: a group of patients treated arthroscopically for anterior glenohumeral instability who remained stable, another group of control patients, and another group of patients with a recurrence of instability after surgery. They reported improvements in parameters compared with preoperatively at 6 weeks after repair, which were maintained at 6 months. There was no difference in postoperative parameters between the stable group and the control group, but there was a significant difference in cases with a recurrence of instability. They concluded that restoration of the glenoid labrum’s position and height was related to surgical outcomes.
Stein et al 28 published a prospective study comparing the postoperative MRI results of 37 patients who underwent surgery for shoulder instability and the MRI results of 31 participants without a history of shoulder instability. The 2 groups had similar glenoid labral height and angle measurements, while glenoid labral morphology was worse in the presence of >4 dislocations. Multiple dislocations in the athletes in our study reduced the improvement in morphology, indicating that patients with only one dislocation tended to have greater improvement in labral morphology. Similarly, an increase in coronal height was associated with the occurrence of a single dislocation, indicating that patients with only one dislocation tended to have a greater increase in coronal height at 6 months.
Bock et al 7 published a retrospective series of 21 patients who underwent arthroscopic surgery for the correction of anterior glenohumeral instability and then bilateral shoulder MRI postoperatively to evaluate glenoid labrum healing. They reported that anterior and inferior glenoid labral height and angulation were equivalent between the operated shoulders and contralateral shoulders, but significant morphological and osteoarthritic changes were present in the operated shoulders, as were reduced clinical scores, compared with the nonoperated shoulders. Our follow-up time was too short to evaluate clinical or osteoarthritic results, but an improvement in morphology was associated with age. In the postoperative period, older patients in our study exhibited a reduced improvement in morphology.
Lobo et al, 23 in 51 patients undergoing arthroscopic treatment for anterior shoulder instability, analyzed whether there were differences in functional and imaging results according to the type of anchor (knotless or knotted) used. They concluded that the clinical, radiographic, and recurrence results were similar at 24 months of follow-up between the 2 groups. In our study, we only used knotted anchors and observed that measurements at 3 and 6 months for the analyzed parameters were significantly different from the preoperative measurements and that patients with a duration of injury of up to 90 days and those who did not practice contact sports tended to have a greater increase in the coronal angle.
Lee et al 21 evaluated 50 patients with anterior shoulder instability who underwent surgery and then computed arthrotomography at 3 and 12 months postoperatively. The group with postoperative apprehension had a greater capsular volume fraction than did the group without apprehension. The labral height measured by early and late computed arthrotomography was not significantly different between the 2 groups. In our study, we did not use MRI with contrast to avoid adverse events. When the labral height on 3- and 6-month MRI was evaluated, we observed a statistically significant difference from the preoperative value. However, labral height on the axial section showed no correlation with any exposure variable, whereas height on the coronal section was associated with the number of dislocation episodes, suggesting that patients with only one episode tended to have a greater increase in coronal height at 6 months probably because the mobility of the labrum at the time of surgery was still good or adhesion was less; thus, bumper formation was well executed, and the coronal height was able to be re-created.
Buckup et al 9 evaluated the clinical and radiographic results after repair of the anterior-inferior capsulolabral complex in patients with instability. One group received 2 knotless anchors, and the other group received 3 knotless anchors. Both groups underwent MRI after at least 1 year of follow-up on the operated shoulder and the contralateral shoulder. In the 2-anchor group, the height and angle were lower on the operated side than on the contralateral side compared with the 3-anchor group. However, both groups had good clinical and functional results, with a minimum follow-up of 2 years. In our study, we used knotted anchors, with a mean of 3.2 anchors per patient. We observed that patients who experienced fewer dislocation episodes had greater gains in labral height on 3- and 6-month MRI.
Our results revealed that the density of capsulolabral repair tissue was high on all 3-month MRI scans and in 63% of the 6-month MRI scans probably because this tissue was still immature. Some studies have assessed the MRI characteristics of anterior cruciate ligament (ACL) reconstruction in the knee and ligament reconstruction in the ankle using grafts. 9 Although these tissues have different healing processes, observations can be made regarding labral tissue. Animal studies have shown that lower graft signal intensity is correlated with greater strength and superior biomechanical properties of the reconstructed ligament. 2 A lower preoperative MRI signal intensity of the anterior talofibular ligament in the ankle is associated with better clinical outcomes, particularly a faster return to sport. While studies on ACL reconstruction have not demonstrated a correlation between graft maturity and clinical outcomes, understanding when the graft may be most fragile allows for the modification of rehabilitation exercises and even the return of these athletes to the field.8,20,22 As in ACL reconstruction, perhaps the heterogeneity of the labral tissue signal may be consistent with tissue that is still immature for a return to full physical activity; therefore, we must pay special attention to these athletes when we allow them to return to sport. The findings of this work will be useful for postoperative radiological evaluations, and notably, not all patients had a homogeneous labrum at 6 months postoperatively. This leads us to question whether these patients are truly ready to return to high-demand sport activities or if they may have higher rates of instability recurrence. A follow-up of these patients will be conducted to correlate long-term clinical outcomes (>5 years) with the results observed on MRI. Understanding the normal evolution of capsulolabral tissue is important; the MRI findings in our study can be used as a reference for radiologists to determine how capsulolabral tissue should appear at different time points after arthroscopic repair.
There are several limitations in our study. First, we did not evaluate clinical data such as functional scores, redislocation rates, or subluxation rates. Second, our follow-up period was too short to evaluate complications such as recurrence or arthritis. Despite these limitations, this was a prospective study with a specific population of athletes, and we evaluated data that have rarely been explored in previous studies, such as the type of sport, number of dislocation episodes, and characteristics of the glenoid labrum on MRI before and after arthroscopic labral repair.
Conclusion
In our study, we found a statistically significant improvement in the morphology, height, and angle of the glenoid labrum on MRI after arthroscopic labral repair for glenohumeral instability. Athletes who underwent surgery within 90 days or those with a single dislocation episode had better integrity and homogeneity of labral tissue. Compared with 3-month MRI, 6-month MRI showed a progressive improvement in labral homogeneity, and although 6-month MRI showed healing of the labrum in all athletes, 63% still had heterogeneous capsulolabral tissue.
Footnotes
Final revision submitted December 4, 2024; accepted January 3, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study was approved by the ethics and research committee of Federal University of São Paulo (No. 46089221.7.0000.5505).