
Abstract
Background:
Reduced absolute joint space width (JSW) has been shown to correlate with higher rates of total hip arthroplasty (THA) after hip arthroscopy.
Purpose:
To determine if quantitative differences in JSW between the operative and contralateral hips at the time of hip arthroscopy affect the risk of conversion to THA.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This retrospective analysis queried patients with preserved JSW (>2 mm) who underwent arthroscopic acetabular labral repair with minimum 5-year follow-up, performed by a single surgeon. Patients were grouped based on whether they received subsequent THA. Preoperative anteroposterior supine pelvic radiographs were obtained for each patient, and quantitative JSW measurements were performed at 3 fixed locations (10°, 30°, and 50° in a polar coordinate system, relative to the 0° line drawn from the center of the femoral head to the lateral edge of the acetabular roof). Measurements were obtained by an independent, blinded assessor in a semiautomated fashion, with intraclass correlation for this approach >0.8. JSW differences at each angle were calculated by subtracting the width in the operative hip from that of the nonoperative hip. Cox proportional hazards modeling identified predictors of THA conversion.
Results:
A total of 106 patients with mean follow-up of 8.23 ± 2.24 years were included; 21 (19.8%) converted to THA and 85 (80.2%) did not. THA patients had higher mean age (40.4 ± 13.1 years; P = .006), body mass index (27.2 ± 3.9 kg/m2; P = .02), Tönnis grade (90.5% ≥ grade 1; P < .001), and Outerbridge grade (90.5% grade 3-4; P = .01). THA patients had a significantly greater difference in JSW at 10° (0.494 ± 0.985 mm vs −0.064 ± 0.609 mm; P = .009), 30° (0.779 ± 0.839 mm vs 0.029 ± 0.507 mm; P < .001), and 50° (0.358 ± 0.832 mm vs −0.044 ± 0.527 mm; P = .045) compared with those not requiring THA. Adjusting for differences in JSW at all 3 locations in Cox regression, the 30° difference remained associated with conversion to THA (P < .001). In final modeling with age, sex, and Tönnis grade, greater JSW reductions at 30° were correlated with increased risk of THA (hazard ratio, 3.07; 95% CI, 1.75-5.38; P < .001).
Conclusion:
This study found that greater JSW reductions in the operative versus nonoperative hip were associated with increased risk of THA conversion. In conjunction with known predictors of failure after hip arthroscopy, preoperative JSW differences may be used as an adjunct to assess risk of early THA and counsel patients appropriately.
Keywords
Acetabular labral tears secondary to femoroacetabular impingement (FAI) cause reduced range of motion, hip and groin pain, stiffness, and reduced function and performance in active patients. 34 The bony lesions in FAI have been implicated as an important cause of early-onset osteoarthritis, adding support for surgical intervention.2,12,13 While some patients benefit from nonoperative management (ie, activity modification, physical therapy, nonsteroidal anti-inflammatory drugs or acetaminophen, and intra-articular corticosteroid injections),15,36 surgical intervention with hip arthroscopy is indicated for patients with labral tears secondary to FAI who fail to achieve adequate symptomatic relief, to address symptoms and halt progression of further degenerative changes.20,25,37 However, as the utilization of hip arthroscopy for acetabular labral tears secondary to FAI continues to rise,3,17 there remains a subset of patients who achieve limited benefit from hip preservation surgery and require early conversion to total hip arthroplasty (THA). 23 Thus, there is a need to reassess preoperative variables and patient-specific characteristics that may portend minimal clinical benefit or early failure after hip arthroscopy.
Previous studies have identified factors including older age,6,8,14 higher body mass index (BMI),6,43 decreased femoral version, 39 lower lateral center-edge angle (LCEA), 39 and more severe chondrolabral junction damage 6 as risk factors for conversion to THA after primary hip arthroscopy. Given the association between longstanding FAI and development of primary osteoarthritis,2,12,13 along with the universal availability of radiographs in preoperative evaluation of hip pain, radiographic signs of early degenerative changes represent the best studied predictors of long-term outcomes after hip arthroscopy.
Numerous studies have found higher Tönnis and Kellgren-Lawrence grade to be associated with greater risk of conversion to THA.4,6,10,11,18,20,44 However, these grading systems have been criticized due to their relative subjectivity and poor inter- and intrarater reliability.19,26,35,48 Furthermore, Philippon et al 33 have demonstrated that among Tönnis grade, Kellgren-Lawrence grade, and joint space narrowing, joint space narrowing most accurately predicts conversion to THA. Since this novel publication, 33 increased attention has been devoted to using joint space width (JSW) to predict outcomes after hip arthroscopy,7,21,33,40-42,46 with multiple studies associating reduced JSW at the time of hip arthroscopy (≤2 mm) with increased risk of and/or quicker conversion to THA.21,33,42,46 Of note, however, these studies have assessed absolute joint space narrowing in the operative hip (ie, ≤2 mm total width at a given location) and have found that significant reductions (≤2 mm) in width—representing severe degenerative changes (78% with Outerbridge grade 3 or 4 changes according to one study 42 )—are associated with greater risk of conversion to THA. No studies to date, however, have examined relative joint space narrowing in the operative hip with respect to that of the patient's nonoperative, asymptomatic hip (ie, the width in the nonoperative hip minus that in the operative hip). Furthermore, no single magnitude of joint space has been shown to necessarily correlate with clinical symptoms29,38; thus, a comparison of continuous JSW versus those in the asymptomatic, contralateral hip may provide more valuable information than a single binary cutoff value. Furthermore, assessment of relative joint space narrowing relative to the contralateral side could add particular value as a sign of early degenerative changes in patients with overall preserved absolute joint space (>2 mm) in their operative hip.
Thus, the purpose of the present study was to determine if quantitative differences in JSW between the operative and contralateral hips at the hip arthroscopy affect the risk of conversion to THA. We hypothesized that, even in the context of hips with preserved absolute JSW (ie, >2 mm), reduced preoperative JSW in the operative hip relative to the asymptomatic, nonoperative hip would predict early conversion to THA.
Methods
Study Design
This was a retrospective cohort study of patients who underwent primary hip arthroscopy for treatment of symptomatic acetabular labral tears secondary to FAI. All patients who underwent hip arthroscopy by a single, fellowship-trained surgeon (S.D.M.) between 2008 and 2016 were screened for study eligibility. Patient inclusion criteria were (1) age ≥18 years old; (2) primary hip arthroscopy with labral repair for the treatment of symptomatic acetabular labral tear; (3) adequate quality anteroposterior (AP) supine pelvic radiographs (ie, they included visualization of the entire pelvis including iliac crests, sacral and intervertebral foramina, sacroiliac joints, pubic and ischial rami, femoral necks, and greater/lesser trochanters with minimal distortion or rotation32,49); and (4) minimum 5-year follow-up. Exclusion criteria were (1) labral debridement or hip arthroscopy for indications other than an acetabular labral tear; (2) absolute JSW ≤2 mm in the operative hip on preoperative AP pelvic radiographs; (3) radiographic evidence of hip dysplasia (LCEA < 20°); (4) previous ipsilateral or contralateral hip surgery; (5) unavailable or poor-quality preoperative AP pelvic radiographs; (6) symptoms of bilateral hip pain on preoperative evaluation; and (7) previous hip conditions (eg, fracture, inflammatory arthropathy, Legg-Calve-Perthes disease, slipped capital femoral epiphysis, avascular necrosis, or pigmented villonodular synovitis) (Figure 1). Patients were then stratified into cohorts based on whether or not they received a subsequent THA.

CONSORT (Consolidated Standards of Reporting Trials) flow diagram detailing patient selection.
Study Population
During the study period, patients who presented to the clinic of the senior author (S.D.M.) with hip pain underwent a standardized preoperative evaluation, consisting of hip and pelvic radiographs (ie, AP pelvic, AP of affected hip, and Dunn lateral views) and physical examination with provocative testing of the labrum and assessment for impingement-related symptoms (eg, pain and/or limited range of motion with flexion, adduction, and internal rotation or flexion, abduction, and external rotation). 16 Patients with positive clinical and radiographic findings underwent magnetic resonance arthrography to evaluate labral pathology, coupled with a diagnostic and therapeutic intra-articular hip joint injection (ie, combined local anesthetic with a low-dose corticosteroid). 27 Finally, all patients trialed initial nonoperative management, including activity modification and formal physical therapy, for ≥3 months. Patients who failed to achieve adequate symptom and functional improvement from nonoperative management and consented to undergo hip arthroscopy were screened for inclusion in this study. 36 This study received institutional review board approval.
Data Collection
Eligible patients were invited to participate in the study through an online survey tracking various postoperative outcomes including subsequent THA. Retrospective chart review was performed for participating patients to collect demographic and descriptive data including age, sex, laterality, BMI, LCEA, alpha angle, Tönnis angle, type of FAI, and Tönnis grade. Intraoperative variables of interest were also collected, including Outerbridge grades of cartilage defect, Beck classification of transition zone cartilage injury, and concomitant arthroscopic procedures performed. 2
A computer-assisted, semiautomated method was employed to calculate quantitative JSW for each hip based on deidentified preoperative, supine AP pelvic radiographs obtained for each patient and analyzed in standard Digital Imaging and Communications in Medicine format.29,38 In brief, as has been previously described,29,38 to establish the reference point (0°), the reader placed a mark on a digital radiograph at the lateral edge of the acetabular roof, and the computer located the center of the femoral head. A line was then placed by the computer between these 2 points, as well as at 10°, 30°, and 50° medial to the reference line (Figure 2). The process was semiautomated, facilitated by software that delineated the femoral head and found the acetabular margin along each of the lines, with the assessor confirming each measurement and using a graphical user interface software tool to correct margins, if needed. All measurements were performed by a single, independent assessor blinded to other radiographic or clinical information; the methodology utilized has high intra-rater and interrater reliability (intraclass correlation coefficients [ICC] > 0.8), as has been previously described.29,38 Measurements were performed at 3 predefined fixed locations per hip, at 10°, 30°, and 50° in a polar coordinate system. Importantly, these locations lay within the sourcil and allowed for multiple comparisons that correlated with the superior weightbearing aspect of the acetabular dome. Differences in JSW at each predefined angle were calculated by subtracting the width (in mm) of each patient's operative hip from the measurement obtained from the nonoperative hip.

Quantitative joint space width measurements taken at 3 predefined locations (10°, 30°, and 50° in a polar coordinate system).
JSW measurements were also taken manually by a separate, blinded orthopaedic surgeon (N.J.C.) and JSW differences were calculated to determine interrater reliability of the semiautomated, previously validated approach relative a standard observer obtaining measurements manually at 10°, 30°, and 50° in a polar coordinate system. Interrater reliability between measurement approaches was assessed based on performing semiautomated versus manual measurements for JSW differences for all patients in the present cohort. Additionally, all preoperative radiographs were graded using the Tönnis classification system by a single observer (N.J.C.).
Abbreviated Surgical Technique
After the administration of general anesthesia, all patients were positioned supine on a hip distraction table (Smith & Nephew) with a well-padded perineal post. Intra-articular access was first established with the anterolateral portal using intra-articular fluid distention under fluoroscopic guidance to avoid iatrogenic damage to the labrum. 1 Next, under direct arthroscopic visualization, the anterior, midanterior, and Dienst portals were placed to complete the puncture capsulotomy approach that avoided disruption of the iliofemoral ligament.5,9 The hip arthroscopy technique utilized included use of intermittent traction, pulsed intra-articular lavage to maintain ambient intra-articular temperatures, and an emphasis on chondrolabral junction preservation.30,31,45,47
As clinically indicated, capsular elevation and acetabuloplasty were performed to address pincer deformities. 47 For labral pathology, “simple” repair was performed if adequate, healthy tissue was amenable to suture anchor fixation alone. 47 Conversely, labral augmentation via capsular autograft was employed if the labrum was irreparable (eg, insufficient tissue, advanced degeneration, or complex tears).24,30,31 After addressing pincer and labral lesions, traction was released to ensure restoration of the hip suction seal and confirm an in-round labral repair. As appropriate, cam deformities were resected via femoroplasty while the hip was flexed to 45°. Finally, a dynamic range of motion examination ensured restoration of the labral seal and adequacy of the femoroacetabular decompression and was followed by closure of all incisions.
Postoperative Rehabilitation
Postoperatively, all patients followed the same 5-step, patient-guided rehabilitation program. First, patients were permitted immediate weightbearing as tolerated using a flat-foot gait with crutches for the first 6 weeks; for the first 3 of these weeks, they were prescribed daily deep vein thrombosis prophylaxis (aspirin, 81 mg). At 6 weeks postoperatively, patients began using a stationary bicycle with minimal resistance. At 10 weeks, patients were cleared to begin using an elliptical trainer on low resistance or swimming (with or without a pull buoy) while avoiding intense flutter kicking. At 4 months, patients resumed light strengthening exercises, including short arc leg presses and hamstring curls. Finally, at 6 months postoperatively, patients were permitted to resume impact-loading activities, with high-pivoting activities at 9 to 12 months, as tolerated. 28
Statistical Analysis
Categorical characteristics were compared between cohorts using chi-square or Fisher's exact tests, as appropriate. A Shapiro-Wilk test was used to assess normality. Comparison of continuous variables was performed with independent samples t tests or Mann-Whitney U tests, as appropriate. Associations between continuous variables were assessed using Pearson correlation coefficient (r). Before performing Cox regression analyses, Schoenfeld residual tests were employed to assess the proportional hazards assumption. Both unadjusted (univariable) and adjusted (multivariable) survival analyses were performed using Cox proportional hazards models. Interrater reliability for JSW measurements between the semiautomated methodology and manual measurement was analyzed using the ICC. The following scale was used to classify measurement reliability: ICC < 0.5 (poor), 0.5 ≤ ICC < 0.75 (moderate), 0.75 ≤ ICC ≤ 0.90 (good), ICC > 0.90 (excellent). 22 All reported P values were 2-tailed, with level of significance set at α = .05. Statistical analyses were performed using SPSS Statistical Software Version 28 (IBM Corporation) and R Version 4.2.1 (R Foundation for Statistical Computing).
Results
Study Population
In total, 106 patients were included in the study. Of these, 21 (19.8%) patients converted to THA within the study period (Figure 1). Mean ± SD follow-up for the entire sample was 8.23 ± 2.24 years, with no difference in follow-up between cohorts (P = .53). Mean time to THA conversion was 4.66 ± 3.02 years. With regard to baseline demographics, patients in the THA cohort were significantly older (40.4 ± 13.1 vs 32.9 ± 9.0 years; P = .006) with higher BMI (27.2 ± 3.9 vs 25.0 ± 4.1 kg/m2; P = .02) (Table 1). There were no differences in patient sex or laterality of labral tear between cohorts (P > .05). On radiographic assessment, THA patients had higher Tönnis grades, particularly with more frequent Tönnis grade 2 hips (47.6% vs 9.4%; P < .001) and larger mean Tönnis angles (5.9°± 4.7° vs 3.1°± 4.3°; P = .02) (Table 1). No differences in LCEA, alpha angle, or FAI type were observed between cohorts (P > .05 for each).
Baseline Characteristics for Patients Undergoing Arthroscopic Labral Repair a

Data are reported as mean ± SD or No. of hips (%). JSW, joint space width; THA, total hip arthroplasty.
Statistically significant at P < .05 or adjusted standardized residual >2.
Intraoperative Findings
On intraoperative assessment, the THA cohort had significantly higher Outerbridge grades (P = .01), with a larger proportion of patients with grade 4 chondral defects (38.1% versus 8.2%). No other intraoperative characteristics differed between cohorts, including Beck classification of the chondrolabral junction, FAI procedures performed, other concomitant procedures performed, or presence of a chondral flap (Table 2).
Intraoperative Characteristics for Patients Undergoing Arthroscopic Labral Repair a

Data are presented as No. of hips (%). FAI, femoroacetabular impingement; THA, total hip arthroplasty.
Statistically significant at P < .05 or adjusted standardized residual >2.
JSW Analysis
There were significantly greater differences in JSW among THA patients at 10° (0.494 ± 0.985 mm vs −0.064 ± 0.609 mm; P = .009), 30° (0.779 ± 0.839 mm vs 0.029 ± 0.507 mm; P < .001), and 50° (0.358 ± 0.832 mm vs −0.044 ± 0.527 mm; P = .045) compared with those that did not undergo subsequent THA (Table 1). For the entire study sample, differences in JSW at 10°, 30°, and 50° were strongly correlated (P < .001 for each association) (Appendix Table A1). Upon adjusting for differences in JSW at all 3 locations (10°, 30°, and 50°), only the difference at 30° remained significantly correlated with conversion to THA (P = .001) (Appendix Table A2). Thus, the JSW difference at 30° was included in our final regression analysis. The ICC for JSW difference at 30° was 0.75, indicating good reliability between our semiautomated method and manual measurement for calculating JSW differences.
Preoperative variables included in our final Cox regression were selected on the basis of baseline differences between cohorts, previous literature, and expert opinion (S.D.M.) of key predictors of conversion to THA.4,14,33,42-44,46 In the multivariable Cox model adjusting for age, BMI, Tönnis grade, and JSW differences at 30° (Table 3), larger differences in JSW at 30° were independently associated with an increased risk of conversion to THA after arthroscopic labral repair (Hazard ratio, 3.07; 95% CI, 1.75-5.38; P < .001). Schoenfeld residual tests confirmed that the proportional hazards assumption was not violated for any individual variable or the global model (P > .05 for all). Unadjusted, univariable survival analyses revealed that increased age, higher BMI, higher Tönnis grade, and larger 30° JSW differences each increased a patient's risk of conversion to THA (P < .05 for all) (Appendix Table A3). In the adjusted analysis including all these variables, however, age became nonsignificant, and both BMI and Tönnis grade exhibited marginal statistical significance (.04 < P < .05), while 30° JSW difference remained highly significant (P < .001).
Results of Cox Multivariable Regression a
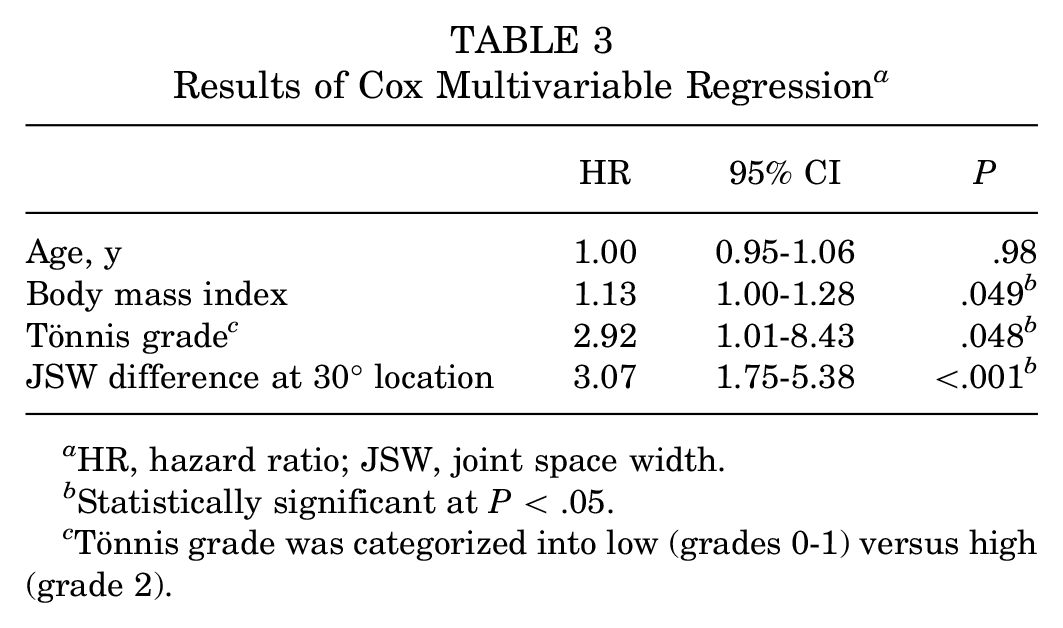
HR, hazard ratio; JSW, joint space width.
Statistically significant at P < .05.
Tönnis grade was categorized into low (grades 0-1) versus high (grade 2).
Discussion
Despite recent literature demonstrating the increased risk of early THA conversion in patients with absolute reductions in JSW at the time of hip arthroscopy,21,33,42,46 studies to date have not assessed the effect of relatively reduced JSW versus the contralateral hip. The first key finding of the present study was that patients who converted to THA had greater JSW reductions at 10°, 30°, and 50° relative to the contralateral hip than patients who did not convert to THA; after adjusting for differences in JSW at all 3 locations, the difference at 30° remained significantly associated with THA conversion. Second, in Cox multivariable regression with age, BMI, and Tönnis grade as covariates, JSW differences at 30° were significantly associated with subsequent conversion to THA at ≥5-year follow-up. These results suggest that, particularly for patients with preserved JSW in their operative hip, comparing JSW with the contralateral hip provides clinically useful information in stratifying risk of subsequent THA and augments other predictors of failure after hip arthroscopy.
The most notable finding of the present study was that patients who converted to THA at ≥5-year follow-up had significantly greater JSW reductions at 10°, 30°, and 50° versus the contralateral, nonoperative hip than did patients who did not convert to THA. Previous studies have demonstrated that reduced JSW at the time of hip arthroscopy is associated with increased risk of and/or quicker conversion to THA.21,33,42,46 In particular, Philippon et al 33 found radiographic JSW to be the most accurate osteoarthritis grading system to predict THA after hip arthroscopy, specifically describing absolute JSW ≤2 mm as a predictor of failure; subsequent studies from this group have shown JSW ≤2 mm to be associated with shorter THA-free survivorship (40 vs 88 months) 46 and that each millimeter of narrowing is associated with 2.5-times greater odds of THA conversion. 42 While these findings are valuable, patients with significantly reduced JSW (≤2 mm) generally have moderate to severe degenerative changes, with much greater odds of cartilage damage as indicated by Outerbridge grades 3 or 4 42 or Beck grades 3 or 4 21 and thus may not represent optimal hip arthroscopy candidates a priori. In contrast to previous studies, all patients in the present study had preserved JSW (>2 mm) in the operative hip. Comparing JSW measurements in the nonoperative, contralateral hip, we were able to identify relative JSW reductions in the operative hip that were associated with higher rates of conversion to THA. Moreover, in the absence of other radiographic predictors of early degenerative changes (ie, >2 mm joint space at all 3 locations and Tönnis grade < 2), 11 of 88 (12.5%) patients still converted to THA. Thus, these relative reductions in JSW may represent early signs of osteoarthritis before significant, absolute narrowing. Comparing JSW relative to the nonoperative hip before hip arthroscopy thus provides a patient-specific baseline and important prognostic information, suggesting that those patients with JSW reductions at 30° relative to the contralateral side have early degenerative changes and may be more likely to convert to THA. Thus, this metric may help to better identify patients who can achieve substantial benefit from arthroscopy versus those who are less likely to benefit and may be at higher risk of revision or conversion to THA, thereby better informing the shared decision-making process to pursue elective surgery.
This study found that in multivariable Cox regression, JSW differences at 30° were highly associated with subsequent conversion to THA at ≥5-year follow-up. Older age,6,8,14 higher BMI, 6 and higher Tönnis grade4,6,10,11,20,44 have been consistently associated with greater risk of conversion to THA after primary hip arthroscopy and thus are used for preoperative patient counseling, patient selection, and prediction of outcomes based on patient-specific characteristics after hip arthroscopy. The present study constructed a multivariable regression model with these established variables, as well as JSW differences at 30°, to assess relative predictive ability. We found that of these 4 variables, JSW differences at 30° were most significantly associated with conversion to THA with the greatest hazard ratio. BMI and Tönnis grade remained significant predictors, with age no longer being significant in the overall adjusted model, likely due to collinearity with Tönnis grade. 11 Thus, this modeling suggests that use of JSW differences provides another prognostic factor to augment known predictors of poor outcomes after hip arthroscopy; this may be helpful in guiding appropriate patient selection and informing patient expectations.
Limitations
While this study highlights novel findings, certain limitations of the present study should be noted. First, due to exclusion of patients not satisfying inclusion/exclusion criteria, our final analysis included a relatively smaller cohort of patients who converted to THA (106 of 345, or 31%, of eligible patients). Accordingly, our final Cox multivariate regression model incorporated the most impactful preoperative variables to avoid overfitting. As we were unable to collect data on patients who were excluded, we could not determine if selection bias existed. Second, our computer-assisted, semiautomated method provided JSW measurements at 3 discrete locations rather than continuous measurements spanning the entire joint. While the JSW difference at 30° was a significant predictor, future research should investigate differences in JSW across the entirety of the acetabular weightbearing dome. Third, these JSW differences relative to the contralateral hip can be small and perhaps not fully apparent to the naked eye without reliable measurement (the mean differences in JSW for patients who converted to THA were 0.494 mm at 10°, 0.779 mm at 30°, and 0.358 mm at 50°). However, previously defined thresholds for assessing absolute JSW have been at 1-mm intervals, 42 suggesting that our principal measurement point, JSW at 30° (mean difference of 0.779 mm), should be able to be appreciated with reliable measurement methodology. Relatedly, measurements were made on supine films; it is possible that measurements from a weightbearing position could produce different results. Finally and relatedly, our JSW measurements were all made with a computer-assisted, semiautomated method. While this method is objective, validated, and reliable,29,38 this approach may not be accessible to or preferred by all orthopaedic surgeons. However, we did assess interobserver reliability, comparing semiautomated measurements to manual measurements by an orthopaedic surgeon on AP pelvic radiographs, finding good interrater reliability between these systems (0.75), suggesting that manual measurements of JSW differences by orthopaedic surgeons and their teams are as valuable in assessing patient risk for subsequent conversion to THA.
Conclusion
This study found that greater JSW reductions in the operative versus nonoperative hip were associated with increased risk of THA conversion. In conjunction with known predictors of failure after hip arthroscopy, preoperative JSW differences may be used as an adjunct to assess risk of early THA and counsel patients appropriately.
Footnotes
Appendix
Results of Cox Univariable Regression a

| HR | 95% CI | P | |
|---|---|---|---|
| Age, y | 1.06 | 1.02-1.12 | .007 b |
| Body mass index, kg/m2 | 1.12 | 1.01-1.23 | .026 b |
| Tönnis grade c | 3.92 | 1.65-9.30 | .002 b |
| JSW difference at 30° location | 4.18 | 2.45-7.13 | <.001 b |
HR, hazard ratio; JSW, joint space width.
Statistically significant at P < .05.
Tönnis grade was categorized into low (grades 0-1) versus high (grade 2).
Final revision submitted December 24, 2024; accepted January 27, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: The Conine Family Fund for Joint Preservation provided research support for this study. S.D.M. has received support for education from Kairos Surgical and honoraria from Allergan. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Partners Human Research Committee (No. 2011P000053).