
Abstract
Background:
Chemically treated allografts (CTAs) have been developed with the goal of providing a graft that is fully sterilized while maintaining the structural integrity and biochemical properties of the graft without irradiation. Few studies have analyzed the complications and postoperative outcomes of CTA in medial patellofemoral ligament (MPFL) reconstruction.
Hypothesis:
The rate of complications and the outcomes of pediatric patients undergoing MPFL reconstruction would be similar between CTAs and low-dose irradiated allografts (IAs).
Study Design:
Cohort study; Level of evidence, 3
Methods:
The medical charts of a consecutive cohort of pediatric patients (aged 12-18 years) who underwent MPFL reconstruction at a single center from June 2011 to September 2022 with either 1- or 2-year follow-up were retrospectively reviewed. Patient characteristics, operative data, and postoperative data were collected in those without diagnosed collagen disorder or multiligament reconstruction. Without deliberate allocation, CTAs were overwhelmingly gracilis tendon allografts, whereas the majority of IAs were semitendinosus. Complications were recorded and included infection, redislocation, and reoperation. Patient-reported outcomes were collected including the Single Assessment Numeric Evaluation score, Kujala score, overall rating of treatment satisfaction, and pain score.
Results:
A total of 235 (114 CTA, 121 IA) patients had 1-year follow-up with no significant differences in complication rate noted between the cohorts (CTA: 6/114 [5.3%]; IA: 5/121 [4.1%]; P = .786). Of the entire group, 122 (60 CTA, 62 IA) patients had 2-year follow-up, with no significant differences in patient-reported outcomes between the CTA and IA cohorts at mean follow-ups of 35.9 and 38.3 months, respectively (P = .271). At a minimum 2-year follow-up, failure rates (defined as redislocation) were 5% (3/60) for the CTA group and 17.7% (11/62) for the IA group (P = .059). Reoperation rates (defined as redislocation requiring repeat operative intervention) were 5% (3/60) and 9.7% (6/62) for the CTA and IA cohorts, respectively (P = .433).
Conclusion:
CTA and IA for reconstruction of the MPFL in the pediatric patient demonstrate similarly low rates of complication, patellar redislocation, and need for revision surgery. Moreover, the outcomes appear to indicate that utilization of gracilis tendon CTA carries the same risk as low-dose semitendinosus IAs when managing children with MPFL reconstruction.
Allograft use in orthopaedic surgery is an acceptable and widely used tool in the setting of ligament reconstruction. Benefits of the utilization of allograft include lack of donor site morbidity, decreased surgical times, and smaller surgical incisions. 5 However, their use is not without risks, which include not only safety concerns but also potentially unknown outcomes regarding long-term stability and strength of the graft. One of the known risks and arguments against the use of allografts is the potential disease transmission. Specifically, there is a risk of transmission of diseases such as HIV, hepatitis B, hepatitis C, and bacterial infections. 14 According to Fishman et al, 3 transmission of disease has been reported in all graft types over the past 20 years with the exception of freeze-dried allografts. Sterilization is the process by which disease transmission is minimized. In orthopaedics, sterility of an allograft is achieved when the disinfection processes of a particular company result in no microorganisms present to a specified level of assurance, a level set by both the American Association of Tissue Banks and the Food and Drug Administration. 16
While the goal of sterility is to prevent disease transmission, the methods used in such processes are not without drawbacks. Processes designed to eradicate microorganisms must be weighed against the damage these processes impart to the strength of the graft. Irradiation, chemical sterilization, and various other preservation methods have been analyzed for their effect on graft strength. The results of these analyses demonstrate that high-dose irradiation, prolonged freezing, and chemical processing techniques may negatively affect the biomechanical properties of a graft. 8 While sterilization techniques can be either mechanical or chemical, novel sterilization processes involve a proprietary combination of both mechanical and chemical processes. Oscillating pressure and vacuum at low temperatures are used to penetrate and perfuse the tissue; blood and lipids are then subsequently removed with chemical agents. 6 Innovative combinations of techniques are proposed to preserve not only the biocompatibility and biomechanical properties of the graft but also the structural integrity.11,12
During the past 15 years, there have been various investigations and analyses undertaken to determine if the specific combination processing of chemically treated allografts (CTAs) has maintained the strength of the grafts while ensuring overall sterility. In their study of CTA in the use of anterior cruciate ligament reconstructions (ACLRs), Jones et al 6 found no difference in CTA when compared with untreated controls. Conversely, Tejwani et al 15 found CTA processing to be associated with a higher risk of clinical failure and need for subsequent revision surgery. Despite the increasing amount of data on the safety and strength of CTA in ACLR, currently, there are limited data analyzing the effectiveness of their use in other ligament reconstructions.
The purpose of this study was to analyze the complications and surgical outcomes of CTAs as compared with low-dose irradiated allografts (IAs) in the setting of medial patellofemoral ligament (MPFL) reconstruction in the pediatric population. The first aim was to identify and compare complication rates between the 2 cohorts. The second aim was to determine if there was any variation in clinical outcomes for the children being managed. Our hypothesis was that there would be no differences in complications or patient-reported outcomes between children managed with CTA or IA for their MPFL reconstructions.
Methods
An application for IRB review was submitted, and the study was determined to be exempt according to the local review board. We performed a retrospective review of the medical records of a consecutive cohort of pediatric patients who underwent MPFL reconstruction at a single center from June 2011 to September 2022. A query from our institution’s research informatics department was obtained utilizing Current Procedural Terminology (CPT) code 27427 for MPFL reconstruction. Inclusion criteria for the review specified patients aged 12 to 18 years at time of surgery who underwent MPFL reconstruction with either low-dose IAs (irradiation doses between 0.95 and 1.4 Mrad; AlloSource) or CTAs (Biocleanse; RTI Surgical) who did not undergo terminal radiation. Patients were excluded if found to be outside of the required age range, if they had a known collagen disorder(s), if they underwent multiple ligament reconstructions during the same operative procedure, or if they had <12 months of follow-up (unless associated with an early failure or complication) for the complication portion of the study. For the outcome portion of the study, a minimum 2 years of follow-up was the inclusion criterion for an assessment of patient-derived outcomes.
Our established institutional protocol for patient follow-up after this procedure is an in-person visit at the 1-year postoperative time point and a telephone call by the clinical team at the 2-year postoperative time point to revisit patient-reported outcomes and overall well-being related to the operative knee. These visits are monitored by our electronic medical record system that produces a weekly monitored report. If a patient misses the 1-year visit, then they are called by the clinical team (a clinical athletic trainer or care coordinator nurse) and invited to attend an in-person visit or, at a minimum, asked about complication metrics and, if the patient is available, patient-reported outcomes. At the 2-year mark, the clinical team (a clinical athletic trainer or medical trainee on service) will contact the family/patient by telephone to ask about outcome measures for clinical trending of surgical success. Each interval of time usually involves 2 or 3 attempts at variable times during the day and which day the attempt is made.
Cohort Selection
The initial query of the electronic health record system by CPT code yielded 1117 patients for review. On initial screening, 290 patients were excluded: 48 patients did not have an MPFL reconstruction, 59 patients underwent reconstruction with autograft, and 183 patients had an unknown or miscellaneous graft type. The remaining 827 cases were classified as having either an IA or CTA. A CONSORT (Consolidated Standards of Reporting Trials) flow diagram of inclusion is illustrated in Figure 1. An additional 705 patients were excluded from the CTA and IA cohorts because they met one of the previously specified exclusion criteria (outside of the required age range, if they had a known collagen disorder[s], if they underwent multiple ligament reconstructions during the same operative procedure, or if they had <12 months of follow-up). Of the 114 surgical cases that met inclusion criteria in the CTA cohort, 8 had bilateral surgery. Of the 121 surgical cases that met inclusion criteria in the IA cohort, 12 had bilateral surgery. One patient in the cohort had one knee with an MPFL reconstructed using CTA cohort, and the contralateral knee was reconstructed using IA. The cases that met a minimum 2-year follow-up included 60 in the CTA cohort and 62 in the IA cohort.

CONSORT (Consolidated Standards of Reporting Trials) diagram illustrating exclusion process. MPFL, medial patellofemoral ligament.
Treatment Protocol
Allografts were transported and stored at −80°F until the start of the case. Graft type chosen was based on surgeon preference. Indications for surgery included recurrent instability or loose body noted on imaging after a first-time dislocation. The surgical techniques of MPFL reconstruction were similar in that diagnostic arthroscopy was performed for any intra-articular pathology, and fixation of the graft on the femur was at the anatomic landmark of the Schöttle point with an interference screw construct. The fixation varied between cohorts in that the IA cohort was secured through a bone tunnel created at the superomedial quadrant of the patella, and the CTA cohort was secured with 2 interference screws on the patella (one for each single limb). Thus, the fixation for the IA cohort had the combined single limbs (not the doubled-over end) inserting into the femur, whereas the CTA cohort had the doubled-over portion of the graft secured to the femur (as the single limbs were attached to the patella). One surgeon was involved per technique. The rehabilitation protocol was the same for both groups.
Data Collection
Preoperative data, including sex, laterality, and age, were collected. Operative data, including graft type, duration of surgery, and concomitant procedures performed, were also collected. Postoperative outcome data collected for analysis included postoperative complications, documented failure (defined as redislocation, including those that did not require further surgery), symptoms of reported instability, reoperation (need for reoperation due to redislocation), any additional required surgery (including interventions related to complications), length of follow-up, and patient-reported outcomes. Patient-reported outcomes included the Single Assessment Numeric Evaluation (SANE) score, Kujala score, overall rating of treatment satisfaction, and pain score. The satisfaction score was on a scale of 0 to 10, with 0 being the least satisfied and 10 being the most satisfied. The pain score was on a scale of 0 to 10, with 0 representing no pain and 10 representing the most pain.
Statistical Analysis
Analysis in comparing variables between graft type groups was performed utilizing a generalized linear mixed model, using subject as a random factor, as multiple patients were represented with bilateral knees undergoing MPFL reconstruction. Two separate series of analyses were carried out: one utilizing any patient with a minimum of 12 months of follow-up and a second subanalysis of those within that cohort who met a minimum of 24 months of follow-up. Alpha was set at a P value <.05 to indicate significance. All analyses were performed utilizing SPSS Version 28 (IBM Corp).
Results
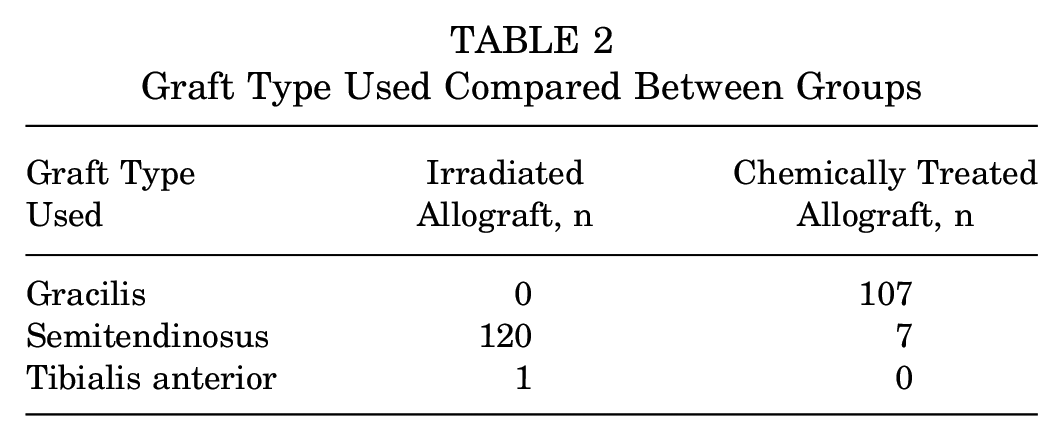
There was no significant difference between cohorts for age at time of surgery, sex, or laterality (Table 1). Surgical time was significantly less in the CTA cohort with a mean of 44.8 minutes (SE, 1.9 minutes) versus 67.6 minutes (SE, 1.9 minutes) in the IA cohort (P < .001) (Table 1). There was some variation in graft type between both cohorts (P = .001) (Table 2). Two surgeons performed the surgeries for this study, each with a preference for graft type. Secondary procedures were similar between cohorts: 49 of 114 (43%) patients with CTA underwent a secondary procedure for loose-body removal and/or chondroplasty, and 53 of 121 (44%) patients with IA underwent similar secondary procedures. Tibial tubercle and/or femoral osteotomies were another secondary procedure that some patients in the cohorts underwent: 24 of 114 (21%) patients with CTA and 15 of 121 (12%) patients with IA.
Comparison of Age at Time of Surgery, Sex, and Laterality Between Groups a

Bold P value indicates statistical significance.
Graft Type Used Compared Between Groups
No significant differences in complications were found between cohorts at a minimum of 12 months or 24 months (Tables 3 and 4). Rates of failure (defined as redislocation) in the cohort with a minimum of 24 months of follow-up approached significance (P = .059), with the CTA group yielding a 5% (3/60) rate of failure versus 17.7% (11/62) in the IA cohort. However, the rate of redislocation requiring a second surgery (represented as reoperation) was 5% in the CTA cohort versus 9.7% in the IA cohort, with a P value of 0.433 on the generalized linear mixed model (Table 4). No significant differences were observed on any subjective outcomes assessed for either 12- or 24-month follow-up (Tables 5 and 6).
Postoperative Outcomes for Cases With Minimum 1-Year Follow-up a

Data are given as n (%) unless otherwise indicated. Reoperation is defined as redislocation requiring revision surgery. Failure is defined as redislocation. Symptoms of instability are defined as shifting or subluxation of the kneecap without frank dislocation of the kneecap. Postoperative complications included events such as suture abscess, skin infection, or hardware removal.
Postoperative Outcomes for Cases With Minimum 2-Year Follow-up a

Data are given as n (%) unless otherwise indicated. Reoperation is defined as redislocation requiring revision surgery. Failure is defined as redislocation. Symptoms of instability are defined as shifting or subluxation of the kneecap without frank dislocation of the kneecap. Postoperative complications included events such as suture abscess, skin infection, or hardware removal.
Subjective Outcome Scores for All Patients With Minimum 1-Year Follow-up a

Data are given as mean ± SE. SANE, Single Assessment Numeric Evaluation.
Subjective Outcome Scores for All Patients With Minimum 2-Year Follow-up a

Data are given as mean ± SE. SANE, Single Assessment Numeric Evaluation.
Discussion
Our results suggest that CTA and IA may be utilized with similar rates of failure/redislocation or need for a second surgery. The results of this study mirror those of Jones et al 6 and Indelicato et al, 4 who demonstrated noninferiority of CTA grafts in adult populations undergoing ACLR. The results of this study signify that CTA use in MPFL reconstruction may be a reliable option for allograft choice without compromising sterility or allograft integrity, specifically in pediatric and adolescent populations undergoing patella-stabilizing procedures.
The benefits of the use of allograft for the reconstruction of ligamentous structures are numerous. Compared with autograft, their use can prevent donor site morbidity, decrease surgical time, and decrease surgical incisions. Of utmost importance, however, is obtaining sterility to prevent disease transmission. Sterilization techniques currently used include peracetic acid and ethanol soak, and pulsatile lavage with antibiotics. 8 In the process of sterilization, a company may also utilize terminal sterilization, in which a product is sterilized within its sterile barrier system. 8 Terminal sterility can be achieved through methods such as ethylene oxide or radiation; the choice of which may have an overall effect of the quality of the tissue.7,12 Biocleanse sterilization involves mechanical components applying oscillating positive and negative pressure along with chemical agents that remove pathogenic agents, blood, and lipids, followed by repeated rinsing. 12 The present study found no difference in the outcomes (complication rate or patient-reported outcomes) between the IA and CTA cohorts, supporting the hypothesis.
As newer techniques have been developed to achieve sterility, their success in guaranteeing sterility must not compromise the strength and integrity of the graft. As CTAs have become available for use, several studies have supported their noninferiority. Jones et al 6 analyzed the effect of CTA use in patellar tendon allograft in ACLR. They found no difference in preimplantation mechanical properties of CTAs compared with untreated controls. Similarly, long-term follow-up of CTA use in bone–patellar tendon–bone ACLR revealed no difference in clinical outcomes at the 2-year follow-up when compared with aseptic allografts. 4 With proven short-term and midterm results in ACLR, CTAs have also been utilized for Achilles tendon reconstructions. 2 In contrast, Tejwani et al 15 find that the use of CTA grafts and irradiation >1.8 Mrad may be linked to a higher risk of revision surgery needed in ACLR.
Although the present study demonstrated shorter surgical times for the CTA cohort compared with the IA cohort, the reason for this difference is not likely related to the graft choice. Although a decreased operative duration has been associated with fewer complications 1 and shorter surgeries can reduce costs through decreased time-dependent operating room fees, 13 the authors would not associate the use of CTAs during pediatric and adolescent MPFL reconstruction with the shorter surgical durations. Instead, it is most likely related to the slight variation in surgical technique.
The difference in graft type distribution among groups is notable but is best explained by surgeon preference (Table 2). Graft choice was not determined by any particular patient characteristic. Furthermore, Migliorini et al 10 showed that isolated MPFL reconstructions performed with semitendinosus grafts result in fewer revision surgeries, fewer redislocations, an increased range of motion postoperatively, and improved patient-reported outcome scores compared with gracilis tendon grafts. However, another meta-analysis demonstrated no difference in clinical outcomes or recurrence rate between semitendinosus or gracilis tendon grafts. 9 It is thus reasonable, as in this study, to use either tendon source based on surgeon comfort, preference, and experience with the graft.
Limitations
The limitations of this study are inherent to its retrospective nature, and the reduced pool of patients for analysis after criteria was applied, predominantly with the cohort of patients achieving 2-year follow-up. Limitations also include single-surgeon cohorts within each arm. Furthermore, this single-center study did not utilize randomization, and multiple surgeons were included in this study with minor variations in technique, thus potentially limiting the generalizability of the results.
Conclusion
This single-center comparison of CTA and IA for reconstruction of the MPFL in the pediatric patient demonstrated similarly low rates of complication, patellar redislocation, and need for revision surgery between the cohorts. There were no significant differences in complications or patient-reported outcomes in patients assessed at either 1-year or 2-year follow-up. However, a study evaluating intermediate-duration follow-up is required next to help determine the longer-term integrity of CTAs in this pediatric population. In the interim, the present results indicate that there is at least no difference in 2-year outcomes for these allograft options. Therefore, the provider should feel confident in the risk stratification and outcomes of both CTA and IA options, and perhaps even in the utilization of gracilis tendon allografts (at least in the form of CTA) when managing children with MPFL reconstruction.
Footnotes
Final revision submitted November 26, 2024; accepted December 30, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research grant funding to support this project was provided by RTI Surgical. E.W.E. is a board or committee member of Pediatric Orthopaedic Society of North America and has received support for education from Elevate Surgical CO, nonconsulting fees from Arthrex, and research support from RTI Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by University of California San Diego (No. 805705).