
Abstract
Background:
Graft selection can influence strength and patient-reported outcomes (PROs) in adults undergoing anterior cruciate ligament reconstruction (ACLR). Yet, there is a lack of high-quality evidence comparing these results in adolescents.
Purpose/Hypothesis:
The purpose of this study was to determine differences in quadriceps and hamstring strength and PROs between adolescents with bone–patellar tendon–bone (BPTB), quadriceps tendon (QT), and hamstring tendon (HT) autografts. It was hypothesized that patients with QT and BPTB grafts would have greater impairments in knee extension, patients with HT grafts would have greater impairments in knee flexion, but PROs would be similar between graft types.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 522 adolescents (mean age, 16.8 ± 1.8 years; 55% female) completed isokinetic knee strength testing at 60 deg/s, the International Knee Documentation Committee (IKDC) subjective knee form, the pediatric IKDC (Pedi-IKDC) subjective knee form, the Knee injury and Osteoarthritis Outcome Score (KOOS), and the Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scale at 7.8 ± 1.5 months after ACLR. Weight-normalized strength was compared via linear mixed-effects models, and PROs were compared between graft types with the Kruskal-Wallis test.
Results:
After controlling for age, sex, time since surgery, and assessment site, patients with BPTB grafts had 10.8% less quadriceps strength in the ACLR limb (P = .05) than patients with QT grafts and 20.4% less quadriceps strength (P < .001) than patients with HT grafts, while patients with HT grafts had 9.6% more quadriceps strength (P = .01) than patients with QT grafts. Patients with BPTB grafts had 3.1% more hamstring strength (P < .01) than patients with QT grafts and 7.0% more hamstring strength (P < .001) than patients with HT grafts. Patients with HT grafts had 10.8% less hamstring strength (P < .01) than patients with QT grafts. Patients with QT grafts had lower IKDC scores (–7.2%; P < .001) than patients with HT grafts and higher KOOS Sports scores (+4.5%; P < .001) than patients with BPTB grafts. Patients with HT grafts had higher IKDC scores (+5.4%; P < .001) and higher KOOS Sports scores (+5.1%; P < .01) than patients with BPTB grafts. There were no differences in ACL-RSI scores (P = .37).
Conclusion:
At 6 to 12 months after ACLR, patients with QT or BPTB grafts had worse normalized quadriceps strength but greater hamstring strength than patients with HT grafts. PROs were mixed, with no differences seen in ACL-RSI scores, but patients with HT grafts displayed greater self-reported function and a greater ability to participate in sport.
Adolescents who participate in sport experience anterior cruciate ligament (ACL) injuries at an alarming rate. 9 Over the last 2 decades, the growing number of ACL injuries among adolescent athletes has been linked to increased competitive sport participation and early sport specialization.10,27 ACL reconstruction (ACLR) remains the gold standard for the treatment of ACL injuries in the United States. Many patients return to sport within 1 year of an ACL injury, which is the primary goal for more than 80% of adolescent patients. 16 Numerous factors, including quadriceps strength, lower extremity function, and patient-reported psychological readiness for sport, have been recommended for consideration in clinical decision making for safe return to sport (RTS) in this population. 25 However, the role of graft source, especially given the recent increase in the use of quadriceps tendon (QT) autografts, has not been well established when evaluating physical and patient-reported measures utilized to determine readiness for RTS. Clinical decision-makers should understand how graft choice may influence outcomes of RTS assessments to inform their decisions based on individual patient needs.
Graft selection has been a debated topic for over 30 years. Despite a sizable body of literature comparing autograft options in adults after ACLR, there is no consensus on the optimal graft type in adolescents who desire to return to sport after surgery. 21 Multiple graft options are available for the management of adolescent ACL tears, and graft choice is dependent on many factors including patient anatomy, age, surgeon preference, rehabilitation outcomes, and expected level of sport participation.21,43 Compared with hamstring tendon (HT) autografts, bone–patellar tendon–bone (BPTB) autografts display quicker healing to bone tunnels, improved tensile strength, and decreased graft failure, while drawbacks include knee extensor weakness, anterior knee pain, and increased donor site morbidity. 3 HT autografts result in stronger knee extensor muscle strength and less donor site morbidity but often lead to persistent knee flexor weakness and an increased risk of reinjuries. 3
Recently, there has been an overall rise in the use of QT autografts because of lower rates of donor site morbidity than other graft types, less anterior knee pain, and similar patient-reported outcomes (PROs) and reinjury rates at 2 years compared with BPTB and HT autografts.14,26,32,36,45 The present literature on QT autografts is limited to small sample sizes in comparative studies, adult and mixed cohorts of patients, and differences in strength testing parameters such as isokinetic velocity, making it difficult to report outcomes from a large generalized adolescent population. 15 While the reinjury rates and anatomic benefits of each graft have been well examined, rehabilitation and PROs between grafts within the adolescent population have not been sufficiently evaluated in a large sample across multiple sites. 43 With the increased popularity of the use of QT autografts, there has not been a large multisite study in adolescent patients assessing how graft type affects knee extensor strength, patient-reported function, and psychological readiness as patients are preparing for RTS.26,37
Inadequate quadriceps and hamstring strength recovery is a concern after ACLR because of the association of decreased thigh muscle strength with an increased incidence of reinjuries, altered lower extremity biomechanics, diminished functional performance, and an increased risk of knee osteoarthritis.13,18,31,35 Many current protocols recommend between-limb symmetry of at least 90% for quadriceps and hamstring strength to begin a progression of RTS, although it is often reported that many patients display a limb symmetry between 70% and 80% at the time of RTS.18,29 The role of PROs is also important for RTS, patient satisfaction, and overall quality of life. For example, higher self-reported function and psychological readiness at 6 months after ACLR have been associated with 2.6 and 4 times greater odds, respectively, of returning to competitive sports at 1 year after ACLR. 42 If graft type affects factors such as strength and function that modify a patient's perception of his or her recovery, this may affect the patient's self-reported function, symptoms, and psychological readiness during the rehabilitation period after ACLR. Adolescent patients are likely to have far different daily demands or goals than adult patients.
Large studies of adolescent patients evaluating thigh muscle strength, patient-reported knee function, symptoms, and psychological readiness for sport after ACLR are needed to determine if graft source has a meaningful clinical effect on recovery while preparing for RTS. Therefore, the purpose of this study was to compare the outcomes of BPTB, QT, and HT grafts in a large adolescent cohort at 6 to 12 months after ACLR. We hypothesized that BPTB and QT grafts would lead to greater impairments in isokinetic knee extension, HT grafts would result in greater impairments in isokinetic knee flexion, and there would be similar PROs between graft types.
Methods
This was a multisite study including adolescent participants from 4 sites included in the ACL Reconstruction Rehabilitation Outcomes Workgroup's clinical outcomes registry. The purpose of the ACL Reconstruction Rehabilitation Outcomes Workgroup's registry is to combine data and resources from a geographically diverse consortium of researchers at affiliated universities, hospitals, and research sites to improve clinical decision-making and patient care after ACLR. Data were collected as part of separate prospective institutional review board–approved research studies (University of Virginia [HSR220225]) at each site, and a limited dataset from each site was then aggregated in an institutional review board–approved registry housed and managed by study team members at the University of Virginia (HSR230335).
Participants
Included patients underwent primary ACLR at 6 to 12 months before testing but had not yet been cleared for return to unrestricted sport participation. Participants were included if they were aged 12 to 21 years, completed strength testing, and completed at least 1 PRO measure included in our analysis. If participants underwent testing on >1 occasion during this time frame, only their most recent test results were included in analysis. We adopted this age range, as defined by the American Academy of Pediatrics, to allow for a wide range of patients. 1 Patients were excluded if they had a history of contralateral or ipsilateral knee surgery, a concomitant chondral injury, a surgical or postoperative complication that resulted in a second surgical procedure, or multiligament reconstruction at the time of ACLR. Patients were not excluded if they had a concomitant meniscal injury that was treated with partial meniscectomy or meniscal repair at the time of ACLR. Participants at all sites completed isokinetic quadriceps and hamstring strength testing as well as PRO measures as part of a battery of functional and strength tests at 6 to 12 months after primary ACLR. Rehabilitation protocols used at each site are summarized in the Appendix.
Quadriceps and Hamstring Muscle Strength
Peak quadriceps and hamstring strength were assessed by a licensed physical therapist or trained graduate sports medicine researcher using a Humac Norm (Computer Sports Medicine), Biodex System 3 (Biodex Medical Systems), or Biodex System 4 Pro (Biodex Medical Systems) isokinetic dynamometer. Comparisons between the Biodex and Humac dynamometers have shown good between-device agreement (intraclass correlation coefficient = 0.88-0.92). 8 Participants were seated at 90° of hip flexion, with their trunk and thigh secured with straps and the dynamometer's arm secured proximal to the ankle joint. The uninvolved limb was assessed first, followed by the ACLR limb. After warm-up repetitions, 5 consecutive trials were completed at 60 deg/s through a range of motion from 90° to 0° of knee flexion.2,19,41 Maximum peak torques (N·m) for knee extension and flexion were recorded. The peak torque was subsequently normalized to the participant's body weight (N·m/kg) and recorded for unilateral analysis. The limb symmetry index (LSI) was also calculated using the following equation for bilateral analysis:

PRO Measures
Knee Function, Pain, and Symptoms
Participants at the university-affiliated sites completed the International Knee Documentation Committee (IKDC) subjective knee form (n = 235), and participants at the hospital-affiliated sites completed the pediatric IKDC (Pedi-IKDC) subjective knee form (n = 266), to assess self-reported knee-related function for patients aged <18 years. 12 The Pedi-IKDC form was developed for use with 10- to 18-year-old patients and evaluates the same constructs as the adult IKDC form, with adequate psychometric properties and scores high correlated to adult IKDC scores.28,39 Participants also completed the Knee injury and Osteoarthritis Outcome Score (KOOS; n = 277) to evaluate self-reported pain (KOOS Pain), symptoms (KOOS Symptoms), activities of daily living (KOOS ADL), sports and recreation (KOOS Sports), and quality of life (KOOS QOL). 34
Psychological Readiness for RTS
Participants completed the ACL–Return to Sport after Injury (ACL-RSI) scale (n = 491) to assess psychological readiness for RTS. The ACL-RSI score has demonstrated a strong correlation with the IKDC score (R = 0.717) and has excellent internal consistency (Cronbach alpha = 0.959). 6
Statistical Analysis
Continuous variables by graft type were evaluated via 1-way analysis of variance, and categorical variables were evaluated via the chi-square test. Linear mixed-effects models were used to analyze weight-normalized strength testing results by graft type while including age, sex, time since surgery, and assessment site as covariates. As 1 group needed to be chosen as the reference group for each model, participants with QT grafts were used as the reference group in all models. Models were run for both the ACLR limbs and the uninvolved limbs. The outcome variables for the models were normalized peak torque of the ACLR limb, normalized peak torque of the uninvolved limb, and LSI for knee extension peak torque and knee flexion peak torque. Because of the nonnormal distribution of PRO data, PRO scores were compared via the Kruskal-Wallis test across graft types. The post hoc Dunn test was conducted for any significant findings from the Kruskal-Wallis test. Significance was set a priori at P≤ .05. Statistical analysis was conducted in Stata (Version 18.0; StataCorp). 38
Results
A total of 522 participants completed strength testing at 1 of 4 research sites. A breakdown of participants by research site can be found in Appendix Table A1. The number of patients who completed each PRO measure varied, and subsets of patients completed different PRO measures across all sites (IKDC form: n = 235; Pedi-IKDC form: n = 266; KOOS: n = 274-277 [varying by subscale]; ACL-RSI scale: n = 491). The HT group had a significantly greater distribution of female patients, while the BPTB group was significantly older. The QT group was significantly further out from surgery than the other groups. Full demographic information and strength testing results by graft type can be found in Table 1.
Patient Characteristics and Strength Data a

Data are presented as mean ± SD or n (%). ACLR, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone; HT, hamstring tendon; LSI, limb symmetry index; QT, quadriceps tendon.
Between-group differences were observed.
Knee Extension Strength Outcomes
Mean normalized strength data by graft type can be found in Figure 1. The overall model for normalized isokinetic knee extension strength of the ACLR limb at 60 deg/s was significant (P < .01), indicating a difference in knee extension strength across graft types. Sex was the only significant covariate, as male patients were stronger on average (P < .001). When controlling for age, sex, time since surgery, and assessment site, patients with BPTB grafts had 10.8% less knee extension strength than those with QT grafts (–0.17 N·m/kg; P = .05). Patients with HT grafts had 9.6% more knee extension strength than those with QT grafts (+0.15 N·m/kg; P = .01) and 20.4% more knee extension strength than those with BPTB grafts (+0.32 N·m/kg; P < .001). Among covariates, sex was the only significant predictor of knee extension strength (P < .001) for the ACLR and uninvolved limbs identified in the models. In addition to the models analyzing normalized strength metrics, the model analyzing LSI as the dependent variable was significant for knee extension strength (P < .001). Mean LSI data by graft type can be found in Figure 2. Age was the only significant covariate for limb symmetry, as older patients were less likely to be symmetrical (P < .001). When controlling for age, sex, time since surgery, and assessment site, patients with HT grafts had a 13.2% higher LSI for knee extension strength than patients with QT grafts and a 12.6% higher LSI for knee extension strength than patients with BPTB grafts (P < .001). Patients with QT grafts had a similar LSI for knee extension strength as patients with BPTB grafts (P = .14).

Between-group comparison of normalized isokinetic knee extension and knee flexion strength (N·m/kg).

Between-group comparison of limb symmetry index (LSI; %) for knee extension and knee flexion strength.
Knee Flexion Strength Outcomes
The model for normalized isokinetic knee flexion strength of the ACLR limb was also significant (P < .001), indicating a difference in knee flexion strength across graft types. On average, patients with HT grafts had 10.8% less knee flexion strength than those with QT grafts (–0.13 N·m/kg; P < .01) and 7.0% less knee flexion strength than those with BPTB grafts (–0.09 N·m/kg; P < .001). Patients with BPTB grafts had 3.1% more knee flexion strength than those with QT grafts (+0.04 N·m/kg; P < .01). Among covariates, sex was the only significant predictor of knee flexion strength (P < .001) identified in the models for the ACLR and uninvolved limbs, as male patients were stronger, on average. In addition to the models analyzing normalized strength metrics, the model analyzing LSI as the dependent variable was significant for knee flexion strength (P < .001). Patients with HT grafts had a 4.4% lower LSI for knee flexion strength than patients with QT grafts (P = .02) and a 10.8% lower LSI for knee flexion strength than patients with BPTB grafts (P < .001). Patients with BPTB grafts had a 6.5% higher LSI for knee flexion strength than patients with QT grafts (P = .02). Age, sex, and time since surgery were not significant predictors of the LSI for knee flexion strength in the mixed-effects model.
PRO Measure Scores
Among participants who completed PRO measures, there were significant differences across graft types for IKDC (P < .001) and KOOS Sports (P = .01) scores. Full PRO results can be found in Table 2. The post hoc Dunn test indicated that patients with QT grafts had lower IKDC scores than patients with HT grafts (–7.2%; P < .001) and higher KOOS Sports scores than patients with BPTB grafts (+4.5%; P < .001). Patients with HT grafts had higher IKDC scores (+5.4%; P < .001) and higher KOOS Sports scores than patients with BPTB grafts (+5.1%; P < .01). There were no differences in ACL-RSI scores by graft type (P = .37).
Patient-Reported Outcome Measure Scores a
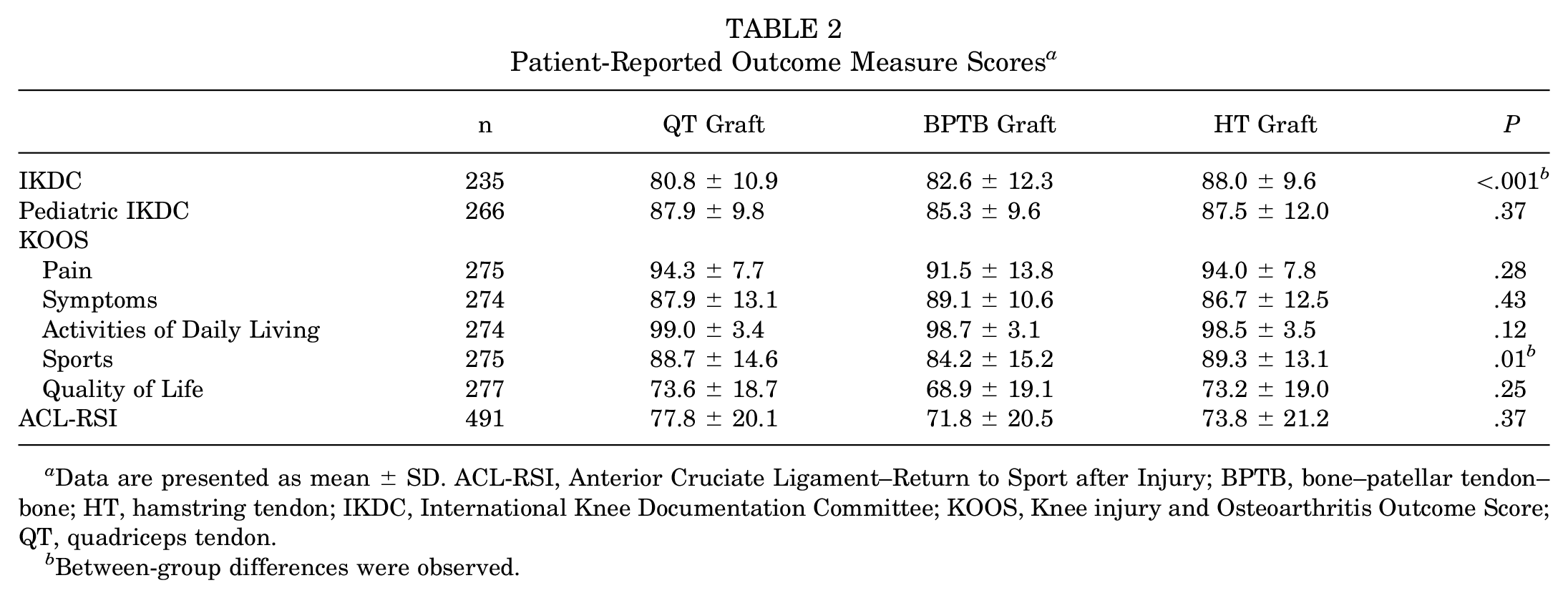
Data are presented as mean ± SD. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; BPTB, bone–patellar tendon–bone; HT, hamstring tendon; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QT, quadriceps tendon.
Between-group differences were observed.
Discussion
The primary finding of this study was that when accounting for age, sex, time since surgery, and assessment site, there were significant differences in isokinetic strength across graft types in adolescent patients at 7.8 months after ACLR. While these differences appear to be significant across the board without adjusting for age, sex, or time since surgery (Table 1), these patient-specific factors must be accounted for when attempting comparisons with each graft type. Strength results are presented without adjustment in Table 1 and Figures 1 and 2. Patients with QT or BPTB grafts had worse knee extension strength in the ACLR limb and a worse LSI for knee extension strength compared with patients with HT grafts; however, the mean LSI in all 3 groups fell below the established clinical cutoffs for acceptable knee extension symmetry for RTS (90%).18,29 Conversely, patients with HT grafts had worse knee flexion strength in the ACLR limb and a worse LSI for knee flexion strength compared to patients with QT or BPTB grafts. However, patients in all 3 groups had an LSI near or above previously established clinical cutoffs for knee flexion symmetry.18,29 Overall, it appears that strength in the muscle group from which the graft was extracted was negatively impacted during middle- to late-stage rehabilitation among adolescents after ACLR. This is especially important because it also coincides with the period of time in which patients are beginning the process of RTS.
There are multiple options of autografts for ACLR, and the risks and benefits must be weighed for their use in the adolescent population. One of the primary deficits hindering patient function after ACLR is persistent knee extensor weakness, which others have found to more negatively affect patients with QT grafts up to 2 years after the injury. 15 Restoring quadriceps strength has consistently been linked to lower reinjury rates, improved function, and a reduced risk of osteoarthritis.11,30,40,46 Regardless of the graft choice, restoring knee extension strength after ACLR is a primary focus of rehabilitation. Grafts harvested from the anterior knee were associated with larger deficits in knee extension strength, and patients with HT grafts had the highest relative isokinetic knee extension strength, which is likely because of the lack of disruption of the extensor mechanism. Similar to others, we found that knee extension strength in the QT group was significantly worse than that in the HT group, but somewhat unique to our findings was that the QT group had significantly greater normalized knee extension strength than the BPTB group when adjusting for age, sex, and time since surgery.7,15 While the unadjusted mean LSIs for knee extension strength in the BPTB and QT groups were different (Table 1), when controlling for age, sex, and time since surgery, the LSI was similar in these groups. It is also important to note that the BPTB group had stronger contralateral limbs than the QT group, which could lead to challenges in interpreting unadjusted LSIs across groups. While graft choice is a multifactorial decision, understanding the differences in presentation throughout recovery and the RTS process may allow clinicians to manage patient expectations or adjust rehabilitation practices in response. Continued longitudinal prospective studies are a necessity to further understand potential differences in the recovery trajectory in an adolescent sample.
Independent of graft type, age and time since surgery were not predictors of normalized knee extension or knee flexion strength in this population. This is important to note, given that this study included patients of various ages and ranged from 6 to 12 months after surgery. Our findings also indicated that regardless of graft type, male patients had higher normalized knee extension and flexion strength in both limbs but a similar LSI to female patients. These findings are similar to several recent studies that have highlighted sex differences in thigh muscle strength at a variety of time points after surgery among adults and adolescents undergoing ACLR.17,33 Developing a more robust understanding of age-, sex-, and graft source–specific patterns of strength recovery after ACLR may aid in setting more realistic goals for patients during rehabilitation while also allowing for more specific and targeted rehabilitation interventions.
PRO measures evaluating self-reported function and psychological readiness remain important tools to assist in determining the progression of RTS. Patients with HT grafts displayed the highest self-reported function on the IKDC form, and patients with HT grafts displayed the highest self-reported ability to participate in sport on the KOOS Sports subscale at 6 to 12 months after surgery. Previous studies have reported higher KOOS scores in patients with QT grafts compared with those with HT grafts and higher IKDC and KOOS scores in patients with HT grafts compared with those with BPTB grafts.5,20 Although patients with QT grafts displayed the highest ACL-RSI scores, there were no significant differences between graft types. The ACL-RSI score is strongly related to self-reported knee function. Previous work has established that scores <56 were associated with an increased risk of not returning to the preinjury level and that scores <76.7 were associated with an elevated risk of a second injury at 1 year.2,6,23,24 In the current study, participants with all graft types had ACL-RSI scores above the threshold associated with return to the preinjury level, but near or below the cutoff for secondary ACL injuries, at 7.8 months postoperatively. While a recent systematic review also explored differences in PROs by graft type, the mean age in reported studies was 27.3 years compared with our mean age of 16.8 years. 7 While the focus of this study on an adolescent population adds further context to a critical time point for the preparation of RTS, the differences in PROs between graft types may have limited clinical significance. Future work should determine the long-term effect of differences in perceived function and psychological readiness in adolescents and how it varies by graft type.
Limitations
An important distinction of this study is that our outcomes were focused on an adolescent population. While our statistical models of strength account for age, we only considered patients up to 21 years of age. Given the natural change in strength that comes with physical maturity and potential changes in goals or rehabilitation processes with older patients, it is important not to generalize these findings to patients of all ages after ACLR.4,22,44 Because of the nonnormal distribution of PRO data, our analyses of PROs did not account for factors beyond graft type. It is also important to note that these analyses focused on outcomes at a specific time point during the rehabilitation process and cannot be used to determine long-term outcomes after ACLR. In addition, although there were similarities between rehabilitation protocols, they were not identical, and differences between assessment sites were not investigated.
Conclusion
This study demonstrated differences in strength and PROs by graft type. Adolescent patients with QT or BPTB grafts had lower quadriceps strength but higher hamstring strength than patients with HT grafts at 6 to 12 months after surgery. Although most PROs showed no difference between graft types, graft type influenced patient-reported function and patient-perceived ability to participate in sport. Because of the nonnormal distribution of PRO data, our analyses of PROs did not account for factors beyond graft type. While graft selection is a multifactorial decision at the time of surgery, the effect of rehabilitative outcomes and reinjury rates after ACLR should continue to be explored in larger cohorts of patients. Future longitudinal analyses within multisite studies should be conducted on outcomes in adolescent patients after ACLR with various graft types.
Authors
Adam P. Weaver, PT, DPT (Connecticut Children's, Farmington, Connecticut, USA); Christopher M. Kuenze, PhD, ATC (University of Virginia, Charlottesville, Virginia, USA); Dylan Roman, PT, DPT (Connecticut Children's, Farmington, Connecticut, USA); Nicholas Giampetruzzi, PT, MS (Connecticut Children's, Farmington, Connecticut, USA); Meredith Link, PT, DPT, ATC, CSCS (Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania, USA); Alexa Martinez, DPT (Nicklaus Children's Hospital, Miami, Florida, USA); Kylee Rucinski, PhD, MHA (University of Missouri, Columbia, Missouri, USA); Natalie Kupperman, PhD, ATC (University of Virginia, Charlottesville, Virginia, USA); Lucy Phan, MS, CSCS (Arkansas Children's Hospital, Little Rock, Arkansas, USA); Victor V. Prati, DPT (Arkansas Children's Hospital, Little Rock, Arkansas, USA); Cody Walker, DAT, ATC, CSCS (Arkansas Children's Hospital, Little Rock, Arkansas, USA); Taylor Douthit, DPT (Children’s Health Andrews Institute, Plano, Texas, USA); Dhalston Cage, PT, DPT, MS (Children’s Health Andrews Institute, Plano, Texas, USA); John Abt, PhD (Children’s Health Andrews Institute, Plano, Texas, USA); Elliot Greenberg, DPT, PhD (Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania, USA); Theodore Ganley, MD (Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania, USA); Stephen LaPlante, MS, PT, ATC (Children’s Health Andrews Institute, Plano, Texas, USA); Lee Pace, MD (Children’s Health Andrews Institute, Plano, Texas, USA); Brooke Farmer, MS, ATC (Creighton University, Omaha, Nebraska, USA); Terry L. Grindstaff, PhD, PT, ATC (Creighton University, Omaha, Nebraska, USA); Lauren Butler, DPT (Florida International University, Miami, Florida, USA; Nicklaus Children's Hospital, Miami, Florida, USA); Edward Chang, MD (Inova Health System, Falls Church, Virginia, USA); Rachel Cherelstein, BS (Inova Health System, Falls Church, Virginia, USA); Corey D. Grozier, MS (Michigan State University, East Lansing, Michigan, USA); Matthew Harkey, PhD, ATC (Michigan State University, East Lansing, Michigan, USA); Arjun Parmar, BA (Michigan State University, East Lansing, Michigan, USA); Jacob Landers, DPT (Scottish Rite for Children, Dallas, Texas, USA); Sophia Ulman, PhD (Scottish Rite for Children, Dallas, Texas, USA); Chelsea Harrison, PTA (University of Missouri, Columbia, Missouri, USA); Steven DeFroda, MD (University of Missouri, Columbia, Missouri, USA); Richard Ma, MD (University of Missouri, Columbia, Missouri, USA); Elaine Reiche, ATC, CSCS (University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA); Caitlin Brinkman, MS, LAT, ATC (University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA); Tom Birchmeier, PhD, ATC, CSCS (University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA); Shelby Baez, PhD, ATC (University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA); Joseph M. Hart, PhD, ATC (University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA); Michelle Walaszek, PT, DPT, MS (University of Virginia, Charlottesville, Virginia, USA); Kevin Cross, PhD, ATC, PT (University of Virginia, Charlottesville, Virginia, USA); and Xavier Thompson, PhD, ATC (Louisiana State University, Baton Rouge, Louisiana, USA).
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251334143 – Supplemental material for Isokinetic Knee Strength and Patient-Reported Outcomes Differ Between Graft Types in Adolescents After Anterior Cruciate Ligament Reconstruction: A Multicenter Study
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251334143 for Isokinetic Knee Strength and Patient-Reported Outcomes Differ Between Graft Types in Adolescents After Anterior Cruciate Ligament Reconstruction: A Multicenter Study by Adam P. Weaver, Christopher M. Kuenze, Dylan Roman, Nicholas Giampetruzzi, Meredith Link, Alexa Martinez, Kylee Rucinski, Natalie Kupperman, Lucy Phan, Victor V. Prati, Cody Walker, Taylor Douthit, Dhalston Cage, John Abt, Elliot Greenberg, Theodore Ganley, Stephen LaPlante, Lee Pace, Brooke Farmer, Terry L. Grindstaff, Lauren Butler, Edward Chang, Rachel Cherelstein, Corey D. Grozier, Matthew Harkey, Arjun Parmar, Jacob Landers, Sophia Ulman, Chelsea Harrison, Steven DeFroda, Richard Ma, Elaine Reiche, Caitlin Brinkman, Tom Birchmeier, Shelby Baez, Joseph M. Hart, Michelle Walaszek, Kevin Cross and Xavier Thompson in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted October 29, 2024; accepted November 22, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.M.K. has received grants from Inova Health System and Nike. E.C. has received consulting fees from Avanos Medical and research support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Virginia (HSR230335).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.