
Abstract
Background:
The role of subscapularis tears in pseudoparesis in massive rotator cuff tears has been thoroughly investigated in the literature. However, further research is required to assess the effect of pseudoparesis on clinical outcomes in isolated subscapularis tear repair.
Purpose/Hypothesis:
The purpose of the present study was to compare the outcomes of patients with and without preoperative pseudoparesis after repair of isolated subscapularis tears at midterm follow-up. It was hypothesized that patients who underwent arthroscopic repair of isolated subscapularis tears would have satisfactory results regardless of the presence of preoperative pseudoparesis.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The study included 75 patients who underwent arthroscopic repair of isolated subscapularis tears between July 2014 and December 2019 and were evaluated at the final follow-up. Patients were classified into 2 groups based on the degree of preoperative active forward elevation (AFE), using a cutoff of 90° to define pseudoparesis: the nonpseudoparesis group (AFE, >90°; n = 49) and the pseudoparesis group (AFE, ≤90°; n = 26). The range of motion (ROM), visual analog scale score, University of California–Los Angeles shoulder rating scale (UCLA) score, Constant-Murley score (CMS), and Subjective Shoulder Value (SSV) were compared preoperatively and at the final follow-up.
Results:
The median duration of follow-up was 56 months (range, 48-108 months). At the preoperative assessment, active and passive forward elevation, active and passive internal rotation, and the CMS, UCLA score, and SSV were significantly lower in the pseudoparesis group (P < .05). For both groups, significant improvements were observed postoperatively in AFE, passive forward elevation, active internal rotation, passive internal rotation, and all functional outcome scores. There was no significant difference between the groups for both functional scores and ROM values in the postoperative measurements (P > .05). Also, a higher prevalence of pseudoparesis was observed with involvement of the inferior subscapularis tendon or Lafosse type 3 and 4 tears.
Conclusion:
The main finding of the present study is that satisfactory outcomes could be achieved after arthroscopic repair of isolated subscapularis tears, regardless of preoperative pseudoparesis.
Isolated tears of the subscapularis are uncommon, but because of the increased interest in subscapularis tears and shoulder arthroscopy over the last 2 decades, this pathology has been the subject of numerous studies. Although subscapularis tears occur in 27% to 49% of rotator cuff tears, isolated subscapularis tears are rare, with a prevalence of only 4.9% to 5.7%.1,3,13,17,21 Following the description of isolated subscapularis tears by Gerber and Krushell, 14 studies have demonstrated that satisfactory clinical outcomes could be achieved with both open and arthroscopic repair.8,11,23
One of the most important indicators of an adequate clinical outcome in rotator cuff repair is the restoration of the active shoulder range of motion (ROM) to as close to normal as possible. Especially in patients with pseudoparesis, active forward elevation (AFE) of the shoulder <90° in the presence of full passive forward elevation without any neurological deficit, achieving a normal ROM after repair provides substantial improvement.7,22,24 Studies evaluating the results of isolated subscapularis repair have reported that the AFE increases significantly from 100° to 174° preoperatively to 141° to 180° postoperatively.2,17,21,26,27 Kanatlı et al 16 reported on a patient group with an AFE <90° in cases of isolated subscapularis tears. The researchers noted that isolated subscapularis tears involving the tendon extending to the inferior part of the subscapularis have a higher likelihood of being associated with pseudoparesis.
Shoulder pseudoparalysis or pseudoparesis refers to a condition with limited AFE due to a rotator cuff injury without neurological impairment. Werner et al 25 recommended using the term “pseudoparesis” for AFE <90°, while Burks and Tashjian 4 suggested that “pseudoparalysis” is more accurate for AFE <45°. A review of conflicting definitions of the term reported that the most consistent definition of pseudoparesis is a massive rotator cuff tear with an active elevation <90°. 24 In this study, we adopted the term “pseudoparesis,” which is widely accepted in the literature, to describe AFE <90°. Limited information is reported in the literature on the relationship between subscapularis tears and pseudoparesis.
Studies have demonstrated that massive rotator cuff tears extending into the inferior half of the subscapularis tendon tend to be associated with pseudoparesis.5,9,10 Additionally, isolated subscapularis tears that extend into the inferior portion of the tendon are more likely to be linked with pseudoparesis. 16 While research has investigated the relationship between subscapularis tears associated with other rotator cuff pathologies and pseudoparesis, to the best of our knowledge, the relationship between isolated subscapularis tears and pseudoparesis has not been mentioned in clinical follow-up studies in the literature.
The aim of this study was to investigate the outcomes after arthroscopic repair of isolated subscapularis tears, with and without pseudoparesis. We hypothesized that patients who underwent arthroscopic repair of isolated subscapularis tears would have satisfactory outcomes regardless of the presence of preoperative pseudoparesis.
Methods
Participants and Study Design
The records of patients who were admitted to the institution with a diagnosis of rotator cuff tear and underwent arthroscopic surgery by the senior surgeon (U.K.) between July 2014 and December 2019 were retrospectively evaluated. Patients included in the study met the following criteria: (1) underwent isolated subscapularis tear repair without other rotator cuff pathologies, (2) experienced symptoms lasting for at least 6 months preoperatively, (3) had undergone a minimum of 3 months of physical therapy with no improvement preoperatively, (4) had a minimum follow-up period of 48 months postoperatively, and (5) had comprehensive and accessible data, including preoperative history, surgical video recordings, magnetic resonance imaging (MRI) scans, preoperative ROM measurements, and shoulder-specific scores (University of California–Los Angeles shoulder rating scale [UCLA] score, visual analog scale [VAS] score, Constant-Murley score [CMS], and Subjective Shoulder Value [SSV]). Patients with rotator cuff pathologies other than isolated subscapularis tears, acute injury, previous shoulder surgery or fracture, stiff shoulder, chronic and inflammatory arthritis, tumors, and missing data (preoperative examination information, MRI scans, and surgical video recordings) as well as patients lost to follow-up or who did not participate in the final follow-up assessment were excluded from the study. The patient selection process is shown in Figure 1.

STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flowchart demonstrating the patient selection process.
Preoperatively and postoperatively, all patients underwent a thorough physical examination, including shoulder passive and active ROM and rotator cuff–specific tests. The ROM assessments included flexion, abduction, internal rotation, and external rotation angles. Internal rotation was measured by positioning the hand on designated anatomic points: 0 (hand at the side of the thigh), 2 (hand behind the buttock), 4 (hand on the sacroiliac joint), 6 (hand on the waist), 8 (hand on the 12th thoracic vertebra), and 10 (hand at the interscapular level). External rotation was measured with the arm abducted to 0° at the side, using a goniometer. Pain intensity and functional status were assessed using the VAS score, UCLA score, CMS, and SSV. In patients with pseudoparesis, pain was eliminated by injection of local anesthetic to prevent the potential effect of pain on ROM. Using the Lafosse classification, the senior surgeon classified the subscapularis tears (types 1-4) and recorded the condition of the long head of the biceps tendon. 18 Subscapularis fatty degeneration was classified by the senior surgeon according to the Goutallier grading system by analyzing preoperative MRI scans. 15
The patients in the study group were initially classified into 2 categories based on the presence of pseudoparesis. Subsequently, the functional shoulder scores and ROM values of the patients in both groups were subjected to a comparative analysis. To mitigate the effects of selection bias, the tears were classified into 2 groups, superior subscapularis tears (Lafosse types 1 and 2) and inferior subscapularis tears (Lafosse types 3 and 4) based on the Lafosse classification system, and a subsequent subgroup analysis was conducted.
The study protocol was approved by the institutional review board (Decision E-77082166-604.01.02-835173, research code: 2023-1530) and adhered to the guidelines of the World Medical Association’s Declaration of Helsinki.
Surgical Procedures
All patients included in this study underwent surgical procedures performed by a single surgeon (U.K.). Patients were operated on in the semilateral decubitus position, with the glenoid fossa oriented parallel to the ground with the arm at 45° of abduction and 15° of flexion under 4.5 kg of longitudinal traction on a shoulder holder. All surgical procedures were performed with the patient under interscalene block with or without general anesthesia. To summarize, a standard diagnostic arthroscopy was performed with the scope in the posterior portal. Then, the anterior portal was used for instrument insertion and repair of the subscapularis tendon. Debridement involved identifying the lateral border of the subscapularis, visualizing the rolled edge anterior to the glenoid, and using a grasper tool for mobility testing. Soft tissue was removed from the insertion site of the anchor using a motorized shaver. Then, 1 or 2 double-loaded bioabsorbable anchors (Healix; DePuy Mitek) were placed in the footprint depending on the size of the tear, and the repair was completed by passing and knotting the sutures through the tendon. 19
Patients diagnosed with biceps pathology (tendinitis or instability) underwent either tenodesis or tenotomy, with the procedure selected considering the patient’s postoperative expectations. 12 Tenodesis was performed on patients concerned about postoperative deformity and residual pain, while tenotomy was performed on those concerned about longer rehabilitation durations and those experiencing severe pain in the existing bicipital groove.
Postoperative Rehabilitation and Final Follow-up
All patients underwent the same postoperative rehabilitation program. The affected arm was kept in a sling for 6 weeks after surgery. Circumduction exercises and passive external rotation to neutral and passive forward flexion were initiated on the first postoperative day. After 6 weeks, use of the orthosis was discontinued and active-assisted ROM exercises were started. Patients were prescribed a supervised, patient-specific rehabilitation program at 8 weeks. Strengthening exercises gradually progressed to daily activities after the third month.
Patients who met the inclusion criteria were invited for a final follow-up evaluation. During the examination, both passive and active ROM were evaluated using a goniometer by a physical therapist (I.H.A.). The physical examination, including the measurement of shoulder scores, was performed by the physician (A.A.). To minimize potential bias, the physical therapist and physician conducting the postoperative evaluations were blinded to both the study design and the patients’ preoperative conditions, ensuring that their assessments were not influenced by previous knowledge of the patients’ pseudoparalysis status.
Statistical Analysis
The data analysis was performed using SPSS Version 28 (IBM Corp). The Shapiro-Wilk test was used to assess the normality of the data. Because of the nonnormal distribution of the data, the Wilcoxon signed-rank test was applied for intragroup comparisons. The Mann-Whitney U test was used to compare preoperative and postoperative values between groups. Spearman rank-order correlation analysis was used to explore the relationships between clinical measurements and scores. For categorical data, chi-square and Fisher exact tests were used, as appropriate. The sample size of our study satisfied the minimum requirements established by our power analysis, ensuring that the study was adequately powered to detect statistically significant differences between the nonpseudoparesis and pseudoparesis groups.
Results
In total, 75 patients were included in the study: 49 in the nonpseudoparesis group and 26 in the pseudoparesis group. The mean patient age was 56.9 years (SD, 7.3 years; range, 43-68 years) in the nonpseudoparesis group and 55.4 years (SD, 7.4 years; range, 40-67 years) in the pseudoparesis group (P = .202). The group with pseudoparesis included 6 men and 20 women, while the nonpseudoparesis group consisted of 18 men and 31 women (P = .228). The median follow-up duration was 55 months (range, 48-108 months) in the nonpseudoparesis group and 60 months (range, 48-108 months) in the pseudoparesis group (P = .066). Moreover, there was no significant difference in the duration of preoperative symptoms between the 2 groups (P = .222) (Table 1).
Patient Characteristics a

Data are presented as % (n) or mean ± SD. Boldface P value indicates statistical significance.
Classified according to the Goutallier classification.
The Lafosse classification type was significantly higher in the pseudoparesis group than in the nonpseudoparesis group (P < .001). In 75% of patients in the pseudoparesis group, more than half of the subscapularis tendon (Lafosse types 3 and 4) was affected, whereas in the nonpseudoparesis group, more than half of the subscapularis tendon was affected in only 18% of the patients. There was no significant difference between the 2 groups in terms of subscapularis fatty degeneration (Goutallier classification) or biceps pathology (tendinitis or instability) (P = .508 and P = .943, respectively) (Table 1). Among the patients with biceps tendinitis, 4 patients in the pseudoparesis group underwent tenotomy and 4 underwent tenodesis, while 9 patients in the nonpseudoparesis group underwent tenotomy and 6 underwent tenodesis. In patients with instability, 1 patient in the pseudoparesis group underwent tenotomy and 2 underwent tenodesis, while 2 patients in the nonpseudoparesis group underwent tenotomy and 5 underwent tenodesis.
For both groups, when analyzed separately, significant improvements were observed postoperatively in AFE, passive forward elevation, active internal rotation, passive internal rotation, and other measurements, including VAS score, UCLA score, CMS, and SSV (P < .001) (Tables 2 and 3). However, no significant differences were found in active and passive external rotation (Table 2). At the preoperative assessment, significant differences were found between the 2 groups for all variables except active and passive external rotation and VAS score (Tables 2 and 3). However, there was no significant difference between the groups for both functional scores and ROM values in the postoperative measurements (Tables 2 and 3).
Active and Passive Range of Motion in Each Group a

Data are presented as mean ± SD. Boldface P values indicate statistical significance.
P values comparing intragroup preoperative with postoperative results.
P values comparing results between groups with and without pseudoparesis.
Functional Outcome Scores of Each Group a

Data are presented as mean ± SD. Boldface P values indicate statistical significance. CMS, Constant-Murley score; SSV, Subjective Shoulder Value; UCLA, University of California–Los Angeles shoulder rating scale; VAS, visual analog scale.
P values comparing intragroup preoperative with postoperative results.
P values comparing results between groups with and without pseudoparesis.
Subgroup Analyses
The clinical outcomes of patients with and without pseudoparesis were analyzed by classifying them into 2 subgroups based on the Lafosse classification: superior subscapularis tears (Lafosse types 1 and 2) and inferior subscapularis tears (Lafosse types 3 and 4) (Table 4). In the superior tear subgroup, evaluation of shoulder functional scores and ROM values in patients with pseudoparesis indicated significantly lower preoperative results compared with patients without pseudoparesis, except for external rotation and VAS scores, and in the postoperative period both groups achieved satisfactory outcomes (similar to the main groups) (Table 4). On examination of the inferior tear subgroup, it was observed that shoulder functional scores in both the preoperative and postoperative periods were similar to those observed in the superior tear subgroup and the main groups. With regard to ROM measurements, the relationship between pseudoparesis and nonpseudoparesis in patients with inferior tears was found to be similar to that in the main groups and the superior tear subgroup, with the exception of the values for preoperative internal and external rotation and postoperative AER.
Subgroup Analysis a
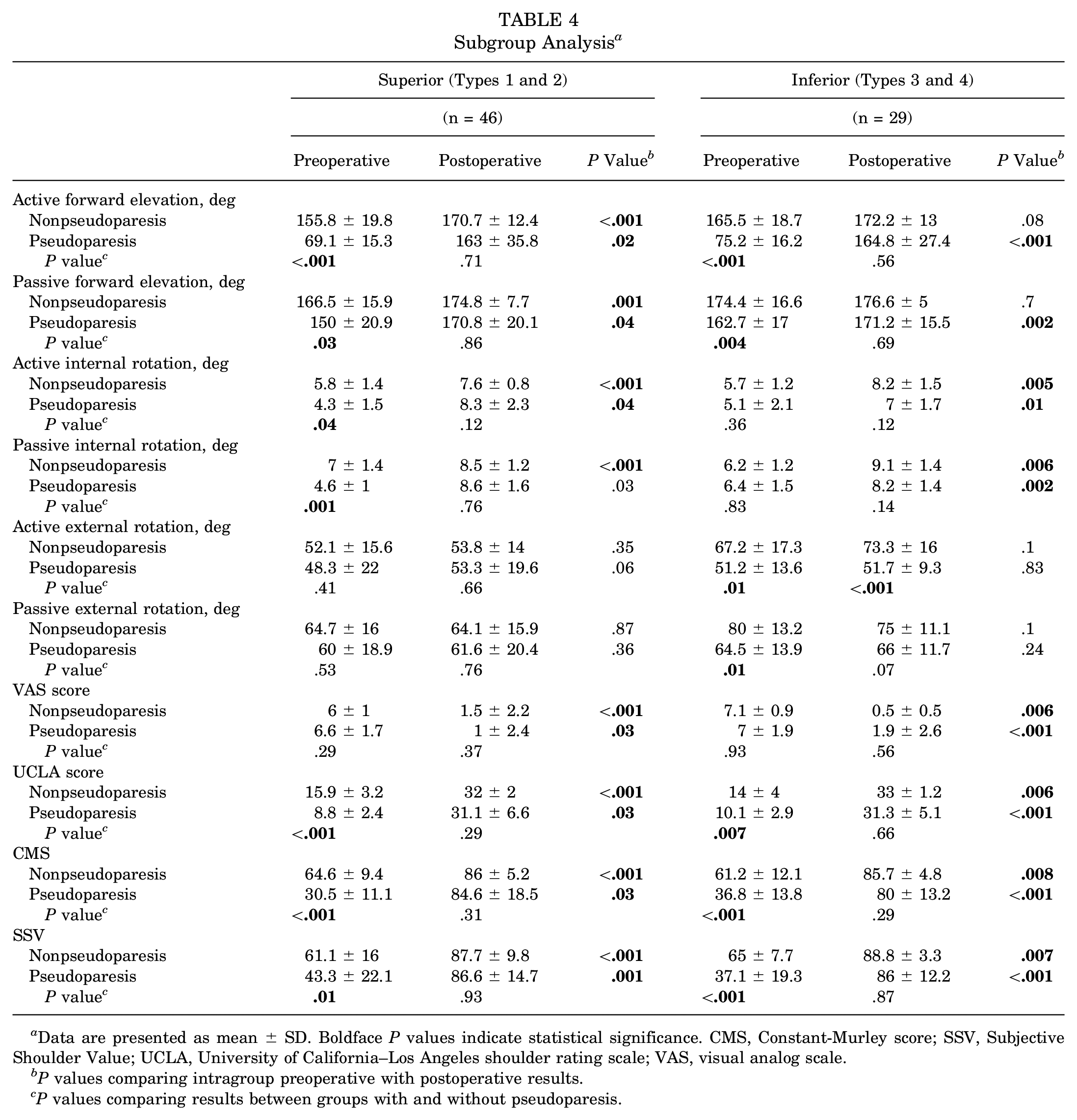
Data are presented as mean ± SD. Boldface P values indicate statistical significance. CMS, Constant-Murley score; SSV, Subjective Shoulder Value; UCLA, University of California–Los Angeles shoulder rating scale; VAS, visual analog scale.
P values comparing intragroup preoperative with postoperative results.
P values comparing results between groups with and without pseudoparesis.
Discussion
In this study, the effect of the presence of preoperative pseudoparesis on patient outcomes after the repair of isolated subscapularis tears was evaluated. The most important finding was that satisfactory results could be achieved after tendon repair in patients with isolated subscapularis tears, regardless of the presence of pseudoparesis.
Limited information is available in the literature regarding the effect of pseudoparesis on the outcomes of rotator cuff tear repair. Oh et al, 22 in their study of massive tears, revealed that patients in the pseudoparesis group had significantly better scores and ROM after repair than preoperatively. They reported that 76% of patients with preoperative pseudoparesis recovered, and there was no difference between patients with and without preoperative pseudoparesis in all scores after repair, except for the CMS and active elevation value. The reason for the lower CMS was indicated to be the lower postoperative abduction strength in the pseudoparesis group compared with the nonpseudoparesis group. In our study, because the postoperative abduction strength of patients with pseudoparesis was similar to that of patients without pseudoparesis, there was no significant difference between the 2 groups in terms of CMS. Oh et al 22 reported a 24% postoperative rate of persistent pseudoparesis in the pseudoparesis group; therefore, the postoperative active elevation value was lower in this group. In the present study, only 8% of patients with preoperative pseudoparesis had persistent pseudoparesis. As a result, postoperative active elevation was similar in both groups. The absence of any discernible difference in active elevation and CMS between the groups postoperatively is attributed to the fact that all the rotator cuff tendons except the subscapularis were intact in the patients in our study. In the present study, the degree of preoperative active internal rotation was significantly lower in the group of patients with pseudoparesis. The reason for the difference may be that the number of patients with more than half of the subscapularis tendon affected was significantly higher in the pseudoparesis group. This is because the middle and inferior parts of the subscapularis tendon have a greater role in internal rotation, and injury to these parts may result in more limited internal rotation. 20 Denard et al6,7 demonstrated that 90% to 95% of cases of pseudoparesis could be reversed with tear repair in patients with no previous surgical history, and favorable clinical outcomes were achieved in these patients. In the present study, most patients with pseudoparesis (92%) had a restored ROM and satisfactory functional results, in accordance with the literature. The main difference in our study is that the studies in the literature evaluated pseudoparesis in massive tears, whereas the present study evaluated pseudoparesis in isolated subscapularis tears.
The results of the subgroup analysis (Table 4) demonstrated that there was no statistically significant difference in the clinical outcomes of patients with and without pseudoparesis in ROM measurements and functional shoulder scores, except for postoperative active external rotation (AER) in the inferior tear subgroup. These findings are consistent with our results in the main groups (Tables 2 and 3). Although subgroup analysis typically provides results that are similar to those of the main groups, it should be noted that different outcomes are observed in the inferior tear subgroup with regard to preoperative internal and external rotation and postoperative AER values in relation to pseudoparesis and nonpseudoparesis. This discrepancy may be attributed to the insufficient sample size involved in our subgroup analysis. It is our contention that more extensive subgroup analyses with larger patient cohorts are required to achieve a more profound understanding of the effect of inferior isolated subscapularis tears and pseudoparesis on external and internal rotation.
Studies have reported that involvement of >50% of the subscapularis tendon is an important determinant of pseudoparesis in patients with massive chronic rotator cuff tears.5,9,10 Ernstbrunner et al 9 reported that the progression of subscapularis tears leads to a decrease in the anterior stabilization of the humeral head during abduction, which can result in pseudoparesis due to the loss of control over the center of rotation. Kanatlı et al 16 demonstrated a strong link between pseudoparesis and isolated subscapularis tears, especially when the tear involves the disruption of the tendon extending into the inferior portion of the subscapularis. Our study confirms previous findings that tears crossing half of the subscapularis tendon are predictive of the loss of AFE. However, we hold the opinion that further anatomic and mechanical studies should be conducted on the origin of pseudoparesis in patients with isolated subscapularis tears.
In addition to tears involving the inferior subscapularis, the pattern of the tear for massive rotator cuff tears is also important for the function of the shoulder. Tears do not affect the muscle in the same way in every tear pattern. 5 Muscle quality is also important for the function and reparability of the tendon. Ernstbrunner et al 10 reported that stage 3 fatty degeneration of >50% of the subscapularis in chronic massive rotator cuff tears was associated with AFE limitation. In this study, none of the participants had stage 3 or greater fatty degeneration, indicating that pseudoparesis could develop without significant fatty degeneration.
Limitations
This study has several limitations. An important shortcoming was the limited number of patients. A larger group of patients, especially in the pseudoparesis group, would allow the outcome analysis to be carried out more precisely in terms of the efficiency of the treatment and the role of other parameters involved. Another limitation is that the repaired subscapularis was not assessed using advanced imaging techniques such as ultrasound or MRI during the posttreatment period. The small number of patients in some subgroups did not allow statistical analysis owing to insufficient power, and we have been unable to provide an explanation for some of the ROM values observed in the inferior part of the subscapularis tear subgroup. The cause of the development of pseudoparesis in 6 patients despite the absence of a tear extending to the inferior subscapularis remains unclear. Further biomechanical investigation is required to elucidate the relationship between an isolated subscapularis tear and pseudoparesis.
Conclusion
In this study, we observed a higher prevalence of pseudoparesis with involvement of the inferior subscapularis tendon or Lafosse type 3 or 4 tears. The main finding was that satisfactory outcomes could be achieved after arthroscopic repair of isolated subscapularis tears, regardless of preoperative pseudoparesis.
Footnotes
Final revision submitted October 27, 2024; accepted November 27, 2024
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Gazi Universitesi Rektorlugu (2023-1530).