
Abstract
Background:
Bone-patellar tendon-bone (BTB) and hamstring tendon (HT) autografts are the most commonly utilized grafts for primary anterior cruciate ligament reconstruction (ACLR). While previous studies have compared outcomes using BTB and HT grafts for ACLR at short- and mid-term follow-ups, outcomes at long-term follow-ups remain unclear.
Purpose:
To perform a systematic review and meta-analysis of randomized controlled trials (RCTs) evaluating BTB versus HT autografts for primary ACLR at a minimum 10-year follow-up.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
A systematic review was performed in accordance with the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines by querying 5 databases from inception through May 2024 to identify level 1 and 2 RCTs evaluating outcomes of BTB versus HT autografts for primary ACLR at a minimum 10-year follow-up. A meta-analysis was performed using random-effects models with risk ratios (RRs) for discrete outcomes and mean differences (MDs) for continuous outcomes.
Results:
Six RCTs—consisting of 495 (BTB, n = 235; HT, n = 260) patients—were identified. The mean age at the follow-up was 41.3 ± 7.4 years, with men comprising 64% (n = 316/495) of patients. The mean final follow-up time was 14.6 ± 0.7 years (range, 10-17 years). No significant differences were observed in ACL graft rupture or revision rates (RR, 0.88; P = .70), contralateral ACL rupture rates (RR, 1.27; P = .46), Lysholm scores (MD, –1.27; P = .45), Tegner scores (MD, –0.01; P = .97), extension deficits (RR, 2.67; P = .23), or KT-1000 side-to-side differences (MD, –0.56; P = .10). There was a significantly greater risk of osteoarthritis (OA) progression in ACLR knees compared with the contralateral knee (RR, 3.64; P < .0001); however, there was no difference in OA progression between BTB and HT groups (RR, 1.01; P = .91).
Conclusion:
BTB and HT autografts for primary ACLR demonstrate similar outcomes and rates of OA progression at long-term follow-ups. Knees undergoing ACLR have a greater risk of OA progression compared with healthy contralateral knees.
Anterior cruciate ligament reconstruction (ACLR) is among the most common procedures performed in orthopaedic sports medicine, with rates continuing to rise annually in the United States. 32 Reconstruction of the ACL is generally recommended for patients sustaining an ACL injury with subsequent pain and instability to regain functional stability and enable return to sports (RTS). 41 Patients undergoing ACLR are reported to experience functional and clinically significant improvements with a low failure and complication rate.33,34
The most common grafts utilized during ACLR are the hamstring tendon (HT) and bone-patellar tendon-bone (BTB) autografts. The graft choice in ACLR is most often dependent on the surgeon’s preferences and the patient’s characteristics, with the BTB autograft often preferred in young athletes participating in pivoting activities. 4 Knees undergoing ACLR with a BTB autograft have demonstrated greater knee stability and a higher RTS rate. In addition, BTB autografts have traditionally been associated with more reliable bone-to-bone healing and osseointegration compared with soft-tissue grafts.13,23 However, previous studies have also shown an increased incidence of extension loss, articular cartilage degeneration, and donor site morbidity (ie, anterior knee pain and kneeling pain) in patients whose knees were reconstructed with a BTB autograft.9,27,49 While HT autografts remain a popular option because of lower donor site morbidity and improved cosmesis from the smaller incision, these grafts have also been associated with higher graft rupture rates, prolonged graft integration times, higher infection rates, and higher risk for tunnel enlargement.6,28 Although several studies have evaluated BTB and HT autografts at short- (1-4 years) and mid-term follow-ups (5-8 years), the long-term outcomes associated with these 2 graft options remain unclear. 37 Moreover, previous systematic reviews evaluating the long-term outcomes of ACLR have been limited, in part, to the inclusion of studies with lower levels of evidence.15,19
Examining the long-term outcomes after ACLR is relevant given the increasing frequency of this procedure, the desire by most patients to return to an active lifestyle even with increasing age, the risk for degenerative changes in the operative knee over time,8,10,11 the incidence of postoperative complications, graft viability, and the risk for revision surgery. This study aimed to perform a systematic review and meta-analysis of randomized controlled trials (RCTs) evaluating outcomes of BTB versus HT autografts for primary ACLR at a minimum 10-year follow-up. The authors hypothesized that BTB and HT autografts for ACLR would yield similar survivorship and clinical outcomes at long-term follow-ups, with comparable osteoarthritis (OA) progression rates.
Methods
Search Strategy
A systematic review was performed in accordance with the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta Analyses) guidelines. 36 A literature search was conducted by querying PubMed, MEDLINE, Scopus, the Cochrane Database for Systematic Reviews, and the Cochrane Central Register for Controlled Trials databases from inception through May 2024 to identify RCTs comparing BTB and HT autografts for primary ACLR at a minimum 10-year follow-up. The search included the following keywords combined with Boolean operators: “ACL,” “Anterior Cruciate Ligament,” “BTB,” “BPTB,” “Bone-patellar tendon-bone,” “Patellar tendon,” “HT,” “Hamstring,” “Semitendinosus,” “Gracilis,” “Autograft,” “Graft,” “Long-term,” “Mid-term,” “Follow-up,” “Outcomes,” “Osteoarthritis,” “Degenerative,” and “10-year.”
Eligibility Criteria
The inclusion criteria consisted of level 1 and 2 RCTs comparing BTB and HT autografts for primary ACLR, with a minimum 10-year follow-up. Each study had to be written in English (or with English-language translation) and reported on clinical and functional outcomes, as well as OA progression. The exclusion criteria consisted of previous systematic reviews and meta-analyses, non-English language studies, non-RCTs, studies with level of evidence 3 to 5, studies with <10-year follow-up, studies utilizing grafts other than BTB and HT, studies with overlapping patient datasets (the RCT with the most recent mean follow-up was retained), editorial commentaries, case reports, and review articles.
Two authors (V.G. and S.T.) independently performed a title and abstract screening followed by a full-text review to identify studies meeting the inclusion and exclusion criteria. A third independent author (D.M.K.) was designated to resolve any potential disagreements; however, no disagreements were encountered. The reference lists of all studies meeting the inclusion criteria were reviewed to ensure that all potential studies meeting these criteria were included.
Data Extraction
Data from the included studies was extracted and compiled into a Microsoft Excel spreadsheet Version 2403 (Microsoft). Study and patient characteristics from both BTB and HT groups were gathered and analyzed—including the number of patients, sex, age at surgery, age at follow-up, time between injury and surgery, and mean follow-up time. Similarly, all patient-reported outcome measures (PROMS), incidence of pain, side-to-side knee laxity, range of motion, RTS, complication rates, graft failures, reoperations (including revision ACLR), contralateral ACL rupture, and conversion to arthroplasty were recorded and analyzed. In addition, OA progression as well as functional outcomes (eg, single-leg hop test, Lachman test, and pivot shift) were evaluated and compared between groups. Osteoarthritic progression was defined as the presence of Kellgren-Lawrence (K-L) grades of ≥2 or International Knee Documentation Committee (IKDC) grades of C or D.
Statistical Analysis
Continuous variables were analyzed and pooled to report a population-weighted mean ± standard deviation. Discrete variables were reported as pooled proportions of the patient population analyzing the specific characteristic. Both the BTB and HT groups were further analyzed independently and compared, with the 2-sample t test of means utilized for continuous variables and the sample z test of proportions used for discrete variables.
When an outcome was reported in ≥3 studies, a meta-analysis was performed. Continuous variables were analyzed using mean differences (MDs) to compare the BTB and HT groups, while discrete variables were analyzed using risk ratios (RRs). If a study reported a median and range, it was converted to mean ± standard deviation using the Vassar Stats calculator. 21 Random effects models and forest plots were produced using Review Manager Version 5.4 (Cochrane). All forest plots included 95% CIs for MD and RR values as well as I 2 values to evaluate heterogeneity. The significance level was set at P < .05. OA progression was analyzed dichotomously, with the presence of significant OA defined as K-L grades of ≥2 or IKDC grades of C or D.35,40
Risk of Bias Assessment
The Cochrane Risk-of-Bias Tool for Randomized Trials (RoB 2) was used to assess study quality and risk of bias. 45 Two independent authors (V.G. and S.T.) performed an analysis with RoB 2 for studies that met the inclusion criteria. Any disagreements were resolved by a third author (D.M.K.).
Results
The initial literature search, performed on March 16, 2024, identified 3451 articles (Figure 1). After the removal of 1132 duplicates, 2319 articles underwent title and abstract screening. After the initial screening, 23 articles were identified for full-text screening, and 6 studies were included for further analysis.

A PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
Study and Patient Characteristics
Six RCTs, consisting of 495 patients, met the inclusion criteria (Table 1). A total of 235 patients underwent primary ACLR using BTB autografts, while 260 patients underwent ACLR with HT autografts. Men comprised 64% (n = 316/495) of all patients. The mean patient age at the time of surgery was 26.9 ± 7.8 years, and the mean patient age at the final follow-up was 41.3 ± 7.4 years. The mean time between injury and ACLR was 27.6 ± 39.4 months. The mean follow-up time was reported specifically in 4 studies,1,3,20,47 with a mean of 14.6 ± 0.7 years (range, 10-17 years). There were no significant differences in patients or study characteristics between the groups undergoing ACLR using a BTB versus an HT autograft (Table 2). As reported in 2 studies,3,26 the most common injury mechanism was during sporting activities—reported in 80% to 83% of patients.
Overview of Included Studies a

ACLR, anterior cruciate ligament reconstruction; AJSM, The American Journal of Sports Medicine; Arch Orthop Trauma Surg; Archives of Orthopaedic and Trauma Surgery; BTB, bone-patellar tendon-bone; F, female; HT, hamstring tendon; LOE, level of evidence; M, male; ST, semitendinosus.
Characteristics of BTB Versus HT Group a

Data are presented as % (n/N) or mean ± SD unless otherwise indicated. BTB, bone-patellar tendon-bone; HT, hamstring tendon.
Graft Rupture and Conversion to Revision ACLR
The rates of graft rupture and conversion to revision ACLR were reported in all 6 studies.1,3,20,26,43,47 Three studies reported graft rupture rates.3,26,47 Three studies reported the number of patients requiring revision ACLR but did not state whether there were additional patients with ACLR graft ruptures who did not undergo a revision ACLR.1,20,43 Random-effects models demonstrated no significant difference in graft rupture and revision rates comparing the BTB and HT groups (RR, 0.88 [95% CI, 0.44-1.74]; P = .70, I 2, 0%) (Figure 2).

Random-effects models demonstrating the risk ratio of graft rupture and conversion to revision ACLR rates between the BTB and HT groups. ACLR, anterior cruciate ligament reconstruction; BTB, bone-patellar tendon-bone; HT, hamstring tendon.
Contralateral ACLR Rupture
Five studies reported rates of contralateral ACL rupture.1,3,20,43,47 The random effects model demonstrated no significant difference in contralateral ACL rupture rates between the BTB and HT groups (RR, 1.27 [95% CI, 0.68-2.38]; P = .46, I 2, 0%) (Figure 3).

Random effects models demonstrating the risk ratio of contralateral ACL rupture between the BTB and HT groups. ACL, anterior cruciate ligament; BTB, bone-patellar tendon-bone; HT, hamstring tendon.
All 6 studies reported PROMS, with the most common scores being the Lysholm,3,20,26,43 the Tegner score,1,3,20,26 the IKDC,3,26,43,47 and the Knee Outcome and Osteoarthritis Score. 1 A meta-analysis was performed for postoperative Lysholm and Tegner scores. Random effects models demonstrated no significant difference in postoperative Lysholm scores between the BTB and HT groups (MD, –1.27 [95% CI, –4.58 to 2.04]; P = .45; I 2, 0%) (Figure 4). Similarly, no significant difference was found between BTB and HT groups in Tegner scores (MD, –0.01 [95% CI, –0.45 to 0.43]; P = .97; I 2, 0%) (Figure 5).

Random effects models demonstrating the mean difference in postoperative Lysholm scores between the BTB and HT groups. BTB, bone-patellar tendon-bone; HT, hamstring tendon.

Random effects models demonstrating the mean difference in postoperative Tegner scores between the BTB and HT groups. BTB, bone-patellar tendon-bone; HT, hamstring tendon.
OA Progression
OA progression was reported in all 6 studies.1,3,20,26,43,47 Four studies graded OA using the K-L grading scale,1,3,20,47 while the 2 remaining studies graded OA using the IKDC score 43 and the Sherman T score. 26 Random effects models demonstrated no significant differences in OA progression between the BTB and HT groups (RR, 1.01 [95% CI, 0.79-1.31]; P = .91; I 2, 30%) (Figure 6). However, significantly greater OA progression was seen in the knees undergoing ACLR (combined BTB and HT groups) compared with the contralateral knees (RR, 3.64 [95% CI, 2.05-6.48]; P < .0001; I 2, 70%) (Figure 7). One study reported OA risk factors, which included meniscus resection, a body mass index of ≥25 kg/m2 at a 2-year follow-up, a pivot shift grade of ≥1 at a 2-year follow-up, performance of manual labor at the time of injury, and injury to the medial meniscus. 1 Of note, Barenius et al 1 reported that 1 patient in the HT group underwent total knee arthroplasty (n = 1/66).

Random effects models demonstrating the risk ratio in OA progression in BTB and HT groups. BTB, bone-patellar tendon-bone; HT, hamstring tendon; OA, osteoarthritis.

Random effects models demonstrating a significantly greater risk for OA progression in knees undergoing ACLR compared with contralateral knees. ACLR, anterior cruciate ligament reconstruction; BTB, bone-patellar tendon-bone; HT, hamstring tendon; OA, osteoarthritis.
Functional Outcomes
Several functional outcomes were reported across studies—including the postoperative Lachman,3,26,43 postoperative pivot shift,3,43 range of motion,3,47 and single-leg hop test.3,20,26,43 Random effects models demonstrated no significant difference in the proportion of patients exhibiting an extension deficit at the follow-up (RR, 2.67 [95% CI, 0.53-13.41]; P = .23; I 2, 0%) (Figure 8). Postoperative knee laxity was reported in 5 studies using a KT-1000 knee arthrometer (MEDMetric) at 89 N 26 , 101 N 26 , 134 N,3,47 and maximum manual force.3,20,26,43 Random effects models demonstrated no significant difference in KT-1000 side-to-side differences at the maximum manual force between the BTB and HT groups (MD, –0.56 [95% CI, –1.22 to 0.10]; P = .10; I 2, 44%) (Figure 9).

Random effects models demonstrating the risk ratio in the proportion of knees with an extension deficit in the BTB and HT groups. BTB, bone-patellar tendon-bone; HT, hamstring tendon.

Random effects models demonstrating the mean difference in KT-1000 side-to-side differences at the maximum manual force in the BTB and HT groups. BTB, bone-patellar tendon-bone; HT, hamstring tendon.
Study Quality Assessment
All studies possessed an unclear risk of bias for bias due to missing outcomes (D3), while there was little concern for risk of bias in the randomization process (D1), or deviations from the intended intervention (D2). Overall, 3 studies1,3,26 showed little concern for the risk of bias, while 3 studies20,43,47 had an unclear risk of bias (Figure 10).
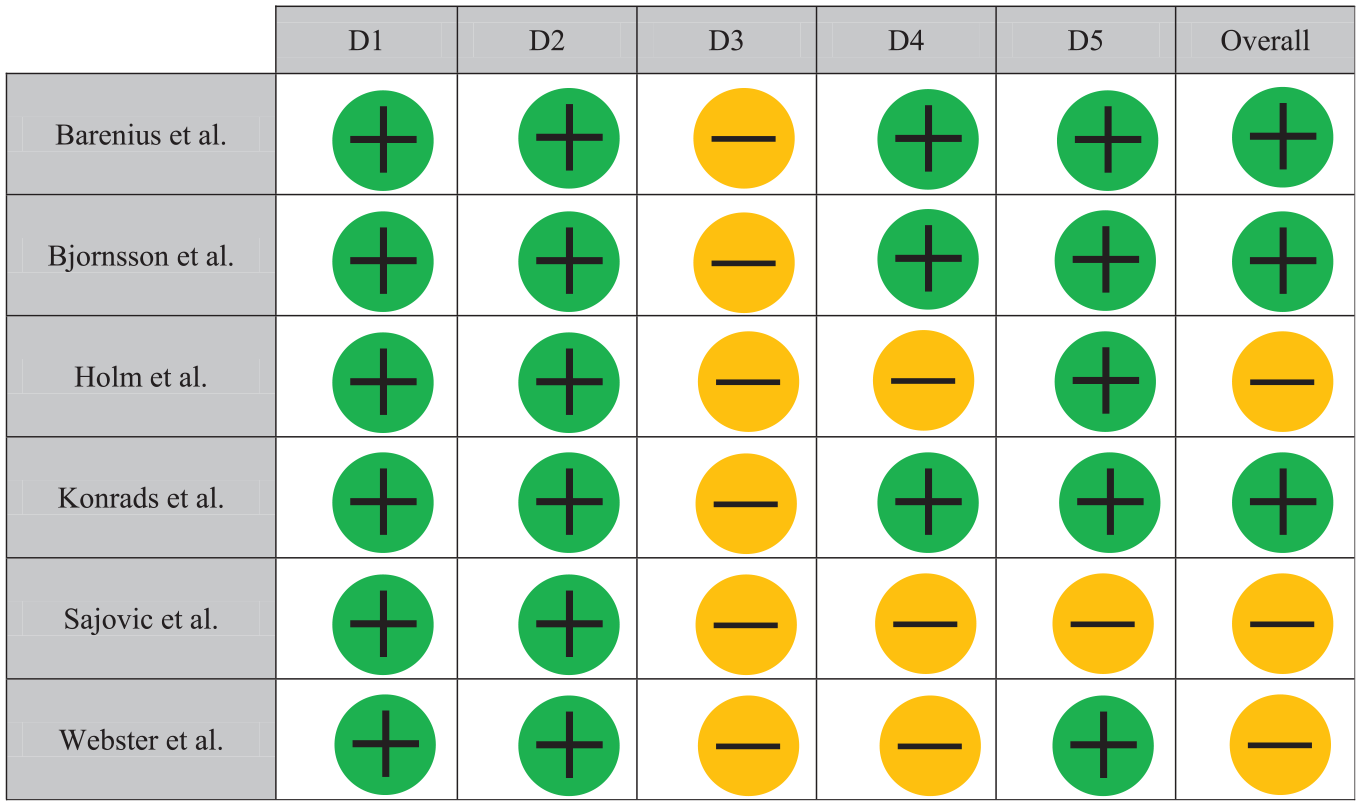
Cochrane Risk-of-Bias Tool for Randomized Trials assessment.
Discussion
The primary findings from this investigation were that data from level 1 and 2 RCTs evaluating patients undergoing ACLR using BTB versus HT autografts for primary ACLR report comparable graft rupture and revision rates, clinical and functional outcomes, as well as OA progression at a minimum 10-year follow-up. Knees undergoing ACLR had significantly greater rates of OA progression at long-term follow-ups when compared with the contralateral knee.
The development of degenerative changes, leading to OA, is a common sequela after ACL injury. 30 At 10 to 20 years after ACL injury, up to 50% of patients have been reported to develop symptomatic OA in the knee—a potentially devasting consequence given the young patient population typically experiencing ACL injury. 30 Development of early-onset OA after ACL injury often has multiple causes, including the ACL injury itself, concomitant and subsequent meniscus and cartilage damage, as well as abnormal gait mechanics after ACLR.7,12,25 In this study, the meta-analysis revealed an RR of 3.5 for OA progression in knees undergoing ACLR compared with the contralateral knee. Previous studies have reported similar findings at long-term follow-ups after ACLR.19,48 A meta-analysis by Grassi et al 19 evaluated patients undergoing ACLR at a minimum 20-year follow-up and reported signs of OA in 73% of knees, with a relative risk for the presence of OA development of 2.8 when compared with the contralateral knee. Similarly, Webster and Hewett 48 reported an odds ratio of 7.7 for the development of OA after ACLR. Although previous work by Roe et al 42 have noted degenerative changes in those knees undergoing ACLR with BTB autografts, there was no significant difference in OA progression between the BTB and HT groups. Therefore, it appears that concomitant injuries sustained during the original ACL injury (as well as additional factors such as time to surgery) may be more predictive of the development of degenerative changes as opposed to graft choice. Moreover, conversion to arthroplasty was an outcome that was only reported in 1 study. 1 Grassi et al 19 reported that 1.1% of patients underwent total knee arthroscopy (TKA) at a minimum 20-year follow-up after ACLR. Given the mean follow-up of 14.6 years in our study, a longer follow-up time is likely necessary to better investigate the true rate of conversion to TKA after ACLR.
No significant differences between groups were found in patients undergoing BTB versus HT tendon autograft reconstruction. Several studies have reported lower graft failure with the use of BTB grafts compared with HT grafts, typically those with follow-ups of <5 years.29,44,46 At a mean 14.6-year follow-up, our study revealed no significant differences in graft rupture or conversion to a revision ACL rate. A 2016 systematic review by Poehling-Monoghan et al 39 evaluated long-term outcomes of BTB and HT autografts, with 12 studies and 953 patients meeting their inclusion criteria. At a mean follow-up of 8.96 years, no studies reported significant differences in failure rates between the BTB and HT groups. Further studies are necessary to evaluate patient- and injury-specific risk factors associated with each graft type that may be predictive of graft failure. The authors hypothesized that the differences noted at short- and mid-term follow-ups between BTB and HT graft options would disappear at long-term follow-ups due to continued graft incorporation, harvest site healing, and postoperative rehabilitation, enabling restoration of lower extremity strength and muscle endurance.
The graft choice in ACLR is largely dependent on surgeons’ recommendations. 4 Numerous cross-sectional studies have reported a growing preference for BTB autografts, particularly among surgeons who are in academic practices, have surgical volumes, and are fellowship-trained in sports medicine.4,22 Advantages of BTB autografts over HT autografts include lower graft failure rates, faster graft incorporation due to bone-to-bone healing, greater RTS rates, and lower HT weakness and posterior knee pain.6,13,16 Moreover, studies evaluating patients after ACLR who underwent second-look arthroscopy have found that BTB autografts demonstrate superior graft morphology and maturation compared with HT autografts.18,31 However, HT autografts remain a viable graft choice, particularly in skeletally immature patients and athletes participating in sports that do not rely heavily on HT muscle strength. 6 While this meta-analysis did not find any significant clinical or functional differences between the BTB and HT groups after a mean follow-up of 14.6 years, further research is necessary to identify those factors most associated with outcomes for ACL autografts to better individualize graft selection based on patient and injury characteristics.
Limitations
This study has several limitations, including the small number of studies identified, secondary to the strict inclusion/exclusion criteria. Moreover, heterogeneous reporting of outcomes was seen across studies, a common limitation inherent to the performance of any systematic review. Several studies removed graft failure and contralateral ACLR ruptures from the respective trials. Although attempts were made to reconcile and include these patients in the final analysis, variable and inconsistent reporting may have led to the exclusion of these patients from the analysis. Moreover, certain outcomes—such as anterior knee pain, kneeling pain, reoperation rate, and complications—were not able to be analyzed and included within the meta-analysis because of the heterogeneity in reporting. Additional variables affecting the results of graft choice could not be stratified and analyzed— including the effect of sex-based and age-based differences, as well as preinjury activity levels. The percentage of patients able to return to their preinjury level of sport and/or work was not analyzed, because of variable and unclear reporting of the activity level at a follow-up of >10 years among studies. In addition, we could not account for the incidence of concomitant meniscal and cartilage injuries, which may have influenced outcomes such as OA progression.
No differences in patients or study characteristics were noted between the BTB and HT groups. However, several outcomes may be influenced by effect modification and confounding variables. Although no differences in long-term results were found in the BTB and HT groups, the vast majority of patients treated in both groups were men, with previous studies reporting female patients undergoing ACLR to possess greater knee laxity and graft rupture rates with HT autografts compared with BTB autografts, relative to their male counterparts.5,38 Moreover, the mean time between ACLR injury and surgery in this study was 27.6 months. Previous investigations have reported a higher rate of patients requiring meniscectomies, greater OA progression, and a poorer likelihood of achieving clinically significant outcomes when ACLR is delayed 6 to 24 months after injury.17,24 Finally, the mean patient age at the time of surgery in this study was 26.9 years, and studies have reported that graft choice in ACLR may have a greater influence on young, active patients, with BTB autografts yielding lower failure rates compared with HT autografts in patients <25 years.2,14 While alternative ACLR grafts are available—including quadriceps tendon autograft and allograft options—our analysis was limited to BTB and HT autografts because of the limited number of studies, with long-term follow-ups examining the use of quadriceps tendons and allografts during ACLR.
Conclusion
BTB and HT autografts for primary ACLR demonstrate similar outcomes and rates of OA progression at long-term follow-ups. Knees undergoing ACLR have a greater risk of OA progression compared with healthy contralateral knees.
Footnotes
Final revision submitted October 17, 2024; accepted November 22, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.V.S. has received speaking and faculty, education, and hospitality payments from Arthrex; education and hospitality payments from Elite Orthopaedics; and hospitality payments from Medical Business Services. M.J.M. has received consulting, faculty, speaking, and hospitality payments from Arthrex; education payments from Elite Orthopaedics; consulting and hospitality payments from Heron Therapeutics; and consulting and hospitality payments from Pacira Pharmaceuticals. R.H.B. has received support for education and hospitality payments from Elite Orthopaedics. D.M.K. has received support for education from Smith & Nephew, Elite Orthopedics, and Medwest Associates; hospitality payments from Arthrex, Encore Media, Stryker, and Smith & Nephew; honoraria from Encore Medical; and a grant from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.