
Abstract
Background:
The capacity of an unrepaired joint capsule to heal after primary hip arthroscopic surgery in patients with femoroacetabular impingement syndrome (FAIS) remains uncertain. The factors that may contribute to nonhealing of the joint capsule are yet to be elucidated.
Purpose:
To report the healing rate of the unrepaired joint capsule after primary hip arthroscopic surgery and to identify factors that may contribute to nonhealing.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Data collected between August 2015 and October 2023 were reviewed. Patients with FAIS aged 18 to 65 years who underwent hip arthroscopic surgery without capsule repair and had a minimum 6-month follow-up were included. Patient demographic data were collected including age at the time of surgery, sex, body mass index, laterality of the affected hip, follow-up duration, FAIS type, and intraoperative procedures. Capsule thickness was measured on preoperative magnetic resonance imaging. The status of capsule healing was evaluated on magnetic resonance imaging at least 6 months after surgery. The correlation between an unhealed capsule and various clinical factors was also evaluated.
Results:
A total of 64 patients (66 hips) were included for analysis (48 hips in the healed group and 18 hips in the unhealed group). Age (44.50 ± 11.36 vs 38.44 ± 10.52 years, respectively; P = .045) and preoperative anterior capsule thickness (3.02 ± 0.87 vs 3.64 ± 1.01 mm, respectively; P = .025) were significantly different between the unhealed and healed groups. Other patient characteristics did not significantly differ between the groups. Higher age (ρ = −0.247; P = .045) and thinner anterior capsule (ρ = 0.276; P = .025) were associated with unhealed capsules. Receiver operating characteristic curve analysis showed that the optimal cut-off value for anterior capsule thickness to discriminate between healed and unhealed capsules was 3.35 mm, with a sensitivity and specificity of 0.667 and 0.667, respectively. The optimal cut-off value for age was 43 years, with a sensitivity and specificity of 0.667 and 0.604, respectively.
Conclusion:
At a minimum 6-month follow-up, 27.2% of patients with FAIS who underwent primary arthroscopic surgery had unhealed anterior hip capsules. Both higher age and lower preoperative anterior hip capsule thickness may affect capsule healing in patients with FAIS who undergo primary arthroscopic surgery without capsule repair.
Hip arthroscopic surgery is increasingly becoming the preferred treatment method for hip diseases including femoroacetabular impingement syndrome (FAIS).3,8 Common capsulotomy techniques include interportal and T-portal capsulotomy, both of which damage the iliofemoral ligament, an important stabilizer of the hip. However, owing to the relative stability of the hip joint, capsule repair is not routinely performed in patients with FAIS during hip arthroscopic surgery.
Numerous studies have confirmed that good to excellent clinical outcomes can be achieved even without repairing the joint capsule.2,5 However, others have emphasized the importance of capsule repair. In a recent meta-analysis of 36 studies comprising 5132 hips, capsule repair was associated with significantly superior postoperative patient-reported outcomes. 11
The underlying theoretical reason is that the unrepaired capsule does not heal after surgery, which may affect the stability of the hip joint and further affect clinical outcomes. Gao et al 6 evaluated 194 patients with FAIS who underwent capsule repair during arthroscopic surgery and found that those with an unhealed capsule exhibited worse postoperative clinical outcomes than those with a healed capsule.
In addition, hip capsule thickness has long been a focal point of interest for researchers.9,17,19 Although several studies have explored the relationship between capsule thickness and stability or clinical outcomes,9,17,19 it is still unknown whether capsule thickness affects capsule healing when the capsule is not repaired during hip arthroscopic surgery.
The capacity of the unrepaired joint capsule to heal after primary hip arthroscopic surgery in patients with FAIS remains uncertain. The factors that may contribute to nonhealing of the joint capsule are yet to be elucidated. Therefore, this study aimed to determine whether hip capsule thickness affects capsule healing in patients whose capsule is not repaired during hip arthroscopic surgery. We also explored factors associated with capsule healing in this clinical setting. We hypothesized that a thinner hip capsule would be associated with nonhealing.
Methods
Participants
This study was approved by the institutional review board of our hospital. Written consent was obtained from all participants. All patients with FAIS who underwent arthroscopic surgery between August 2015 and October 2023 were invited to participate. FAIS was diagnosed based on the criteria of the Warwick Agreement. 7
The inclusion criteria were (1) a diagnosis of FAIS and (2) a follow-up ≥6 months. The exclusion criteria were (1) a lateral center-edge angle (LCEA) <25°; (2) Tonnis grade >1; (3) Legg-Calvé-Perthes disease, slipped capital femoral epiphysis, or avascular necrosis; (4) previous ipsilateral hip injuries or surgery; and (5) a lack of magnetic resonance imaging (MRI) at last follow-up. Patient demographic data were collected including age at the time of surgery, sex, body mass index (BMI), laterality of the affected hip, follow-up duration, FAIS type, Tonnis angle, alpha angle, LCEA, and intraoperative procedures.
Surgical Technique
All procedures were performed by an experienced sports medicine specialist. Under general anesthesia, the patient lay supine on a traction bed with both lower limbs simultaneously under traction. The affected hip joint was externally abducted by 20°, internally rotated by 20°, and flexed by 10°. A perineal column was used to protect the perineal area. Guidance was provided by C-arm fluoroscopy. Successful traction was confirmed by opening the hip joint gap by at least 10 mm and observing the appearance of a “vacuum sign.” Standard disinfection and draping protocols were followed. The procedure began with fluoroscopic localization of the anterolateral portal, midanterior portal, and anterior portal using a 70° arthroscope. An arthroscopic cannula was used for portal management. Interportal capsulotomy was performed for all patients with an arthroscopic electrothermal device between the anterolateral portal and midanterior portal (approximately from 10 o’clock to 3 o’clock). Acetabuloplasty was performed according to the intraoperative findings. The decision to use absorbable anchors (Arthrex) to repair the damaged acetabular labrum (typically 2-4 anchors with a diameter of 3.0 mm) was based on the severity of the labral injury. After confirming the stability of the repaired labrum, traction was released, the hip was flexed at 45°, and femoral osteoplasty was performed according to the intraoperative findings. The joint capsule was not repaired intraoperatively. Hemostasis was carefully achieved, and the skin incision was closed.
Postoperative Rehabilitation
All patients adhered to a standard postoperative rehabilitation protocol, which involved initiating the use of crutches and mobility on postoperative day 2. Partial weightbearing commenced at 2 weeks after surgery, and full weightbearing was allowed at 6 weeks. The recovery process was stratified into 3 phases. Phase 1 (0-6 weeks) focused on limited range of motion (ROM) exercises. Progressive passive, assisted active, and active ROM exercises were performed within the patient’s comfort level. However, in the first 4 weeks, patients were not allowed to flex the hip >90°, extend the hip >0°, or externally or internally rotate the hip >10°. In phase 2 (6-12 weeks), patients were allowed to increase ROM in all directions as tolerated and instructed to activate all key hip muscles to build up endurance and strength of the core and lower extremity muscles; the aim was to facilitate the restoration of daily activities such as normal gait, stair climbing, and sitting. In phase 3 (12-24 weeks), specific hip ROM, strength, and flexibility exercises were performed as needed. Patients were also encouraged to gradually return to performing various types of aerobic exercises. Sport-specific exercises and drills such as jumping, cutting, deceleration, and acceleration were introduced as needed.
Evaluation of Anterior Capsule Thickness (ACT) and Healing Status on MRI
Patients underwent 3.0-T MRI of the hip (uMR790; United Imaging) before and after surgery in the supine position. Scans included a fat-suppressed turbo spin echo (TSE) proton density (PD)–weighted sequence in the axial plane, a TSE T1-weighted sequence in the axial plane, a fat-suppressed TSE PD-weighted sequence in the oblique coronal plane, and a fat-suppressed TSE PD-weighted sequence in the oblique sagittal plane. Slice thickness was set at 2 mm for all sequences.
The iliofemoral ligament is the most significant pericapsular ligament 12 and is located adjacent to the anterior capsule, the primary site for conventional capsulotomy. 4 Consequently, the anterior capsule has become the primary measurement site.1,16 -18 Preoperative ACT was measured on the PD-weighted sequence in the oblique sagittal plane through the anterior inferior iliac spine at the site of routine capsulotomy. A capsular defect was defined as any visual disruption in the iliofemoral ligament in the zone of capsulotomy or the appearance of communication between the joint and the iliopsoas bursa (Figure 1). 18

(A) Measurement of anterior capsule thickness. (B) Example of an unhealed anterior capsule. The purple circle indicates the head of the femur. The purple square indicates the acetabulum. The purple arrow indicates a capsular defect.
There were 2 fellowship-trained sports physicians (L.-Y.S. and Q.-R.L.) who independently reviewed and analyzed the MRI scans in a random order to assess capsule thickness and healing status. Interrater reliability was calculated. In addition, L.-Y.S. assessed the scans 2 times with a 1-week interval to calculate intrarater reliability. In cases of discordant interpretations of healing status, the senior surgeon (H.-Y.L.) made the final determination. All readers were blinded to the clinical data.
Statistical Analysis
The threshold for statistical significance was set at .05 for all analyses. The Shapiro-Wilk test was performed to identify normally distributed data. The F test was used to ascertain whether the compared datasets exhibited equal variances. For categorical data with 2 categories, comparisons were performed using the chi-square test or Fisher exact test. For continuous variables, comparisons were performed using the 2-tailed t test or Mann-Whitney U test as appropriate. The association between the presence of an unhealed capsule and various clinical factors was examined using the Spearman rank correlation coefficient. Interrater and intrarater reliability were assessed using the Cohen kappa and the intraclass correlation coefficient, respectively. Values <0.40 were classified as poor reliability, 0.40-0.59 as fair, 0.60-0.75 as good, and >0.75 as excellent. Receiver operating characteristic (ROC) curve analysis was used to explore the cut-off value. All calculations were conducted using SPSS software (Version 29.0; IBM). Excel (Microsoft) was used for all data analyses.
Results
Patient Characteristics
As shown in Figure 2, of the 275 patients meeting the inclusion criteria, 64 patients (66 hips) were included for analysis, with 48 hips allocated to the healed group and 18 hips allocated to the unhealed group. Table 1 provides a detailed comparison of the participants’ characteristics. There were no significant differences between the 2 groups in BMI, sex, follow-up duration, laterality of the affected hip, preoperative alpha angle, preoperative LCEA, preoperative Tonnis angle, FAIS type, preoperative Tonnis grade, arthroscopic procedures, and presence of a labral tear (all P > .05). Age (44.50 ± 11.36 vs 38.44 ± 10.52 years, respectively; P = .045) and preoperative ACT (3.02 ± 0.87 vs 3.64 ± 1.01 mm, respectively; P = .025) were significantly different between the unhealed and healed groups.

Study flowchart. FAIS, femoroacetabular impingement syndrome.
Participant Characteristics a

Data are shown as mean ± SD (range), No., or n (%). ACT, anterior capsule thickness; BMI, body mass index; FAIS, femoroacetabular impingement syndrome; LCEA, lateral center-edge angle.
P < .05.
Unhealed Capsule
Capsular defects were present in 18 hips (27.2%). Higher age (ρ = −0.247; P = .045) and lower ACT (ρ = 0.276; P = .025) were associated with unhealed capsules. There were no significant correlations between an unhealed capsule and BMI, follow-up duration, preoperative alpha angle, preoperative LCEA, or preoperative Tonnis angle (all P > .05) (Table 2). Intraobserver and interobserver reliability of capsule thickness measurements and healing status assessments were high (Table 3).
Correlation Between Unhealed Capsule and Clinical Factors a
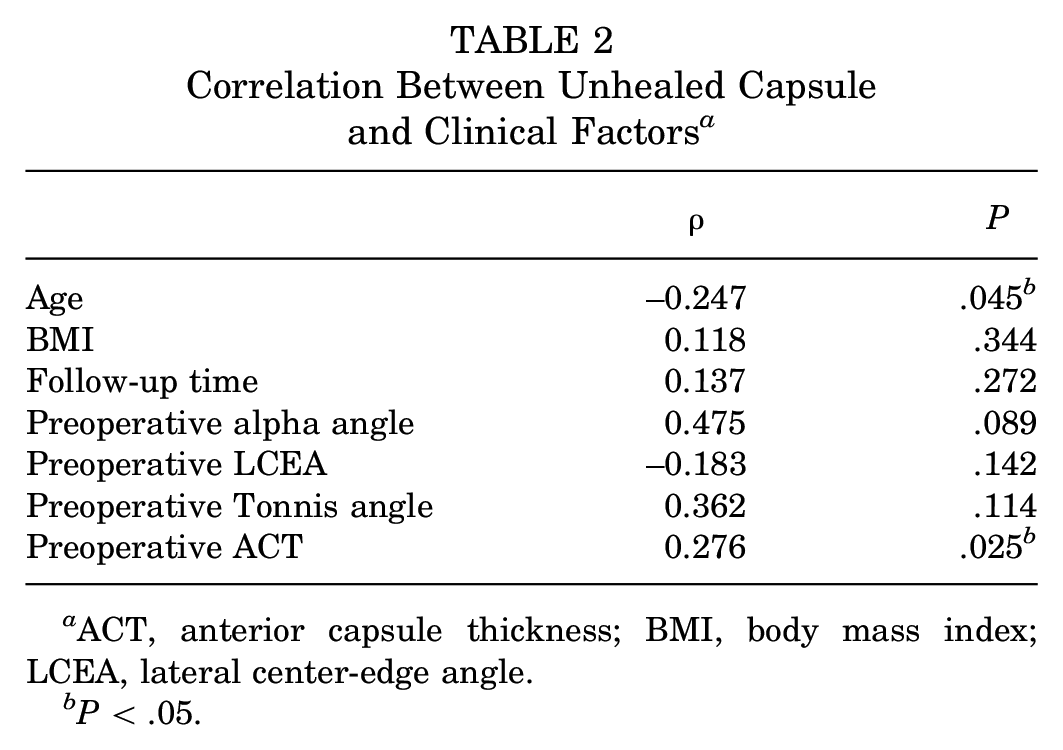
ACT, anterior capsule thickness; BMI, body mass index; LCEA, lateral center-edge angle.
P < .05.
Intraclass Correlation Coefficients for Capsule Thickness Measurements and Healing Status Assessments

ROC Curve Analysis
ROC curve analysis showed that the optimal ACT cut-off value to discriminate between healed and unhealed capsules was 3.35 mm, with a sensitivity and specificity of 0.667 and 0.667, respectively. The optimal age cut-off value was 43 years, with a sensitivity and specificity of 0.667 and 0.604, respectively (Figure 3).

(A) Receiver operating characteristic curve analysis of anterior capsule thickness and age to discriminate between healed and unhealed capsules. (B) Output of analysis, with the largest area under the curve as an indication of predictive power. The optimal cut-off value is the level with the highest combination of sensitivity and specificity.
Discussion
The main finding in the current study was that at a minimum of 6 months of follow-up, 27.2% of patients with FAIS who underwent primary arthroscopic surgery had unhealed anterior hip capsules. Additionally, both higher age and lower preoperative anterior hip capsule thickness may affect capsule healing in patients with FAIS undergoing primary arthroscopic surgery without capsule repair.
Gao et al 6 evaluated 194 patients with FAIS who underwent capsule repair during arthroscopic surgery and found that 17 (8.8%) had a capsular defect on coronal MRI at a minimum of 6 months of follow-up. In addition, Weber et al 15 evaluated 39 patients with FAIS who underwent interportal capsulotomy with routine capsular closure during arthroscopic surgery and found that 92.5% of the repaired hip capsules remained closed at more than 1 year of follow-up. Additionally, Li et al 10 reported that 3 of the 10 patients in their study who underwent interportal capsulotomy without capsule repair were healed at 6 months after surgery, while 7 were not.
In our case series, 27.2% of the patients exhibited nonunion of the joint capsule. There are several reasons that this rate is higher in our study than in previous ones. First, in our study cohort, all interportal capsulotomy sites were not repaired. Therefore, these were more likely to be unhealed, as seen in the study of Li et al. 10 Second, the MRI section thickness in our study was able to identify capsular defects more precisely: we used a 2-mm thickness, while Strickland et al 14 used 3.5 mm.
Several previous studies have explored whether capsule repair affects joint capsule healing. Yang et al 18 examined 74 patients with borderline developmental dysplasia of the hip (37 in the repair group and 37 in the no repair group) and found that the healing rate was higher in the repair group (91.9% vs 73.0%, respectively; P = .032). However, Strickland et al 14 evaluated 15 patients with FAIS (30 hips) who underwent simultaneous bilateral hip arthroscopic surgery with unilateral capsule repair. Coronal MRI showed that all capsules healed, regardless of repair, during a 2-year follow-up period.
In addition, the method of capsulotomy may influence capsule healing. Li et al 10 found that 7 of 10 patients who underwent interportal capsulotomy were unhealed at 6-month follow-up; however, among 23 patients with FAIS who underwent periportal capsulotomy without capsular closure, all had a healed capsule at 6 months after surgery.
Not repairing the joint capsule does not seem to indicate that the capsule will not heal. In addition, most of the capsule remains closed after some time postoperatively. Therefore, it is important to look for factors that may contribute to nonhealing of the hip joint when the joint capsule is not sutured.
Based on our study, higher age and lower preoperative ACT may affect capsule healing in patients with FAIS who undergo primary arthroscopic surgery without capsule repair. The optimal ACT and age cut-off values were 3.35 mm and 43 years, respectively. Theoretically, a thicker joint capsule represents more contact area and is easier to heal. In addition, younger patients have a faster metabolism and a higher likelihood of healing.
Hip capsule thickness is receiving increasing attention from researchers, especially ACT. Studies have identified several factors associated with a thinner joint capsule, including female sex, 1 capsular laxity, 13 increased femoral torsion angle, 17 and elevated neck-shaft angle. 19 It is surprising that a thinner joint capsule always seems to be present in patients with joint instability or microinstability. Instability or microinstability may also be an important factor that influences capsule healing.
Although the need for capsule repair after arthroscopic surgery remains controversial, an increasing number of studies seem to support capsular suturing. Looney et al 11 conducted a meta-analysis that showed that capsule repair is associated with significantly superior patient-reported outcomes. In addition, postoperative clinical outcomes are worse in patients with unhealed capsules than healed capsules in both patients with FAIS 6 and patients with borderline developmental dysplasia of the hip. Our study also found a relatively higher unhealed rate in patients who did not undergo capsule repair. These results indicate the importance of capsule repair, especially in patients with a thinner preoperative anterior capsule and higher age.
Limitations
This study had several limitations. First, it was retrospective in design, which almost certainly introduced a degree of selection bias. Second, the sample size was relatively small. Third, the time points of follow-up MRI were different, and the integrity and thickness of the capsule may be different at different time points. However, a previous study has shown that the capsule will heal within 6 months. 15
Conclusion
Unhealed anterior hip capsules were present in 27.2% of patients with FAIS who underwent primary arthroscopic surgery without capsule repair and had a minimum 6-month follow-up. Both higher age and lower preoperative anterior hip capsule thickness may affect capsule healing in patients with FAIS who undergo primary arthroscopic surgery without capsule repair.
Footnotes
Final revision submitted August 29, 2024; accepted November 22, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a grant from the National Key Research and Development Program of China (2020YFC20070405 [to H.-Y.L.]). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Huashan Hospital Affiliated to Fudan University Institutional Review Board (2020).