
Abstract
Background:
Current anterior cruciate ligament (ACL) injury prevention programs focus on integrating the athlete’s cognitive and motor skills. A few studies examine the effectiveness of different types of attentional instructions on motor learning.
Purpose:
To investigate the acute and first-week effects of combined focus of attention and video instructions given to female athletes with dynamic knee valgus (DKV) and landing technique.
Study Design:
Controlled laboratory study.
Methods:
A total of 30 athletes were randomized to (1) a verbal combined focus–instructed group (VFIG) (n = 10), (2) a video-instructed group (VIG) (n = 10), and (3) a control group (CG) (n = 10). DKV was assessed with frontal plane projection angle (FPPA) during the single-leg squat test, and landing technique was assessed with the Landing Error Scoring System (LESS) during drop vertical jump (DVJ) task. After pre-FPPA and pre-LESS values were recorded, 2 training blocks that contained 10 repetitions of the DVJ task in each were completed with group-specific instructions, and posttest measurements were taken immediately afterward and a week after as a retention test. Parametric tests were utilized due to the normal distribution of numerical descriptive features. Independent-sample t tests compared numerical features between groups, chi-square tests assessed categorical features, and mixed-order analysis of variance evaluated variables based on retention times, with Bonferroni correction applied and a significance threshold set at P < .05.
Results:
Statistical improvement occurred in both VFIG and VIG intragroup FPPA assessment at posttest and retention test (respectively, P < .001; P < .001; P < .01). In the intergroup evaluation, FPPA showed superior improvement in VFIG at the posttest and retention test (P = .001; P < .01). In the intragroup evaluation, there was a statistical improvement in LESS values in both VFIG and VIG, at the posttest and retention test (respectively, P = .04; P < .001; P < .05), and VIG had superior improvement in the intragroup evaluation compared with VFIG. There was no statistically significant difference between LESS values in the intergroup evaluation (for all, P > .05). There was no significant difference in the CG tests (for all, P > .05).
Conclusion:
Our study demonstrated that while both types of instructions were effective in improving knee valgus and landing technique, verbal combined focus instructions were superior in improving valgus. Future long-term studies will help in the understanding of the prevention of ACL injuries in female athletes.
Clinical Relevance:
Considering that female athletes have a higher risk of ACL injury due to higher DKV values than men, the authors believe that combined verbal and video instructions are important in reducing the knee valgus value and improving the landing technique, thus possibly reducing the injury rate.
Registration:
NCT06424886 (ClinicalTrials.gov identifier).
Sports that require landing and rapid changes of direction after jumping, such as football, basketball, and volleyball, are associated with anterior cruciate ligament (ACL) injuries. 7 Approximately 70% of ACL injuries occur during noncontact landing on 1 leg. 30 The landing phase after a jump is important as it is the moment that 31% of injuries occur 7 because it causes high ground-reaction force and increased knee valgus.19,24 The risk of injury is particularly high in female athletes <20 years of age, with a rate of 63%.8,14
The jump landing task has been widely used as a screening method to assess ACL injury risk.1,25 Kinetic and kinematic parameters associated with ACL injury risk are assumed to be an effective way to identify at-risk athletes when evaluated during jump landing tasks. 1
Current rehabilitation approaches target motor learning as well as the updating of traditional rehabilitation programs to prevent faulty movement patterns. 4 Recently, the importance of adding cognition and motor learning principles to injury prevention programs has been underlined.5,28,38 A variant within the cognitive approach is the external focus of attention (EFA) and the internal focus of attention (IFA). In EFA, the athlete’s attention is directed to objects or environments external to the human body (eg, “stand on 1 leg and slowly bend your knee while keeping your knee over your foot”). In IFA, attention is directed directly to the movements (“stand on 1 leg and reach slowly toward the cone with your knee while bending your knee”). 5 Although the difference in these instructions may seem small, EFA has resulted in better performance, retention (maintenance of acquired skill), transfer of the gained motor ability from one type of movement to another, and greater movement automaticity.10,12,37,39 On the other hand, IFA resulted in better conscious control of the body, 34 movement acuity, and muscle activity. 15
Although current injury prevention programs include interventions to provide motor skills using clear instructions, such as EFA or IFA, and visual feedback regarding desired landing positions,4,39 there are a limited number that aim to correct lower extremity alignment form and use verbal instructions,2,37 and study results are not consistent.2,20,32,35,37 Because most sports are complex and consist of multiple different movement patterns, athletes need to adopt many focusing tips. In addition to the need for athletes to switch between EFA and IFA, it is also supported that they should adopt both focus types at the same time. 17 However, to our knowledge, there is no study related to the combined use of EFA and IFA instructions in the current literature.
The use of visual instructions in ACL injury prevention programs has also been shown to be effective.3,5,16 Instructions for participants to simply imitate the expert in the video, without pointing to specific body parts, have been seen as an effective method of promoting motor learning and retention by improving embodied cognition targeting the whole body.5,36 Therefore, ACL injury prevention programs can be expanded to include modern technology such as video with expert learning to investigate the effects of video feedback on motor learning and retention. 5
The main purpose of our study is to investigate the acute and first-week effects of combined (EFA and IFA) instructed verbal training and video-instructed visual training given to semiprofessional female athletes with dynamic knee valgus (DKV) on frontal plane projection angle (FPPA) and landing technique. We hypothesized that the verbal combined focus–instructed group (VFIG) would have a superior improvement in DKV while the video-instructed group (VIG) would have a superior improvement in landing technique.
Methods
General Design
Our study has a randomized, controlled, single-blind, prospective design and was conducted between January 15, 2024, and June 12, 2024. Evaluations of the participants were made at Caferağa Sports Hall. Before the study began, ethics committee approval was obtained from Istanbul Medipol University Non-Interventional Clinical Research Ethics, and the protocol to be applied was recorded in and registered at the National Library of Medicine Clinical Trial Registration and Results System (NCT06424886). Before including the participants in the study, all participants were asked to read and sign the informed consent form.
A total of 30 healthy female athletes were included in the study. Participants were randomized into groups by drawing a sealed envelope from a closed box with the group names written on a piece of paper within each envelope. The study groups were the VFIG (n = 10), VIG (n = 10), and control group (CG) (n = 10). Landing Error Scoring System (LESS) and FPPA evaluations were completed before and immediately after the intervention. Additionally, the same evaluations were repeated a week later as a retention test. The CONSORT (Consolidated Standards of Reporting Trials) flow diagram of the study is shown in Figure 1. The evaluations were made by a blinded assessor (P.P.) to the groups.

CONSORT (Consolidated Standards of Reporting Trials) flowchart of the study FPPA, frontal plane projection angle; LESS, Landing Error Scoring System.
A pilot study was conducted with 10 participants to ensure the consistency and reliability of the assessor. After the participants were evaluated at the beginning of the week, they were reevaluated within the same week without any change in their condition. In the evaluation of intraclass correlation coefficients (ICCs) for the pilot study, confidence intervals <0.40 were “weak,” 0.40 to 0.59 were “moderate,” 0.60 to 0.74 were “good,” and 0.75 to 1.00 were “very good.” 9 Intrarater hand reliability was determined as 0.888 and 0.988 for FPPA and LESS, respectively. Pilot study values are summarized in Table 1.
Intrarater Reliability of Measurements a
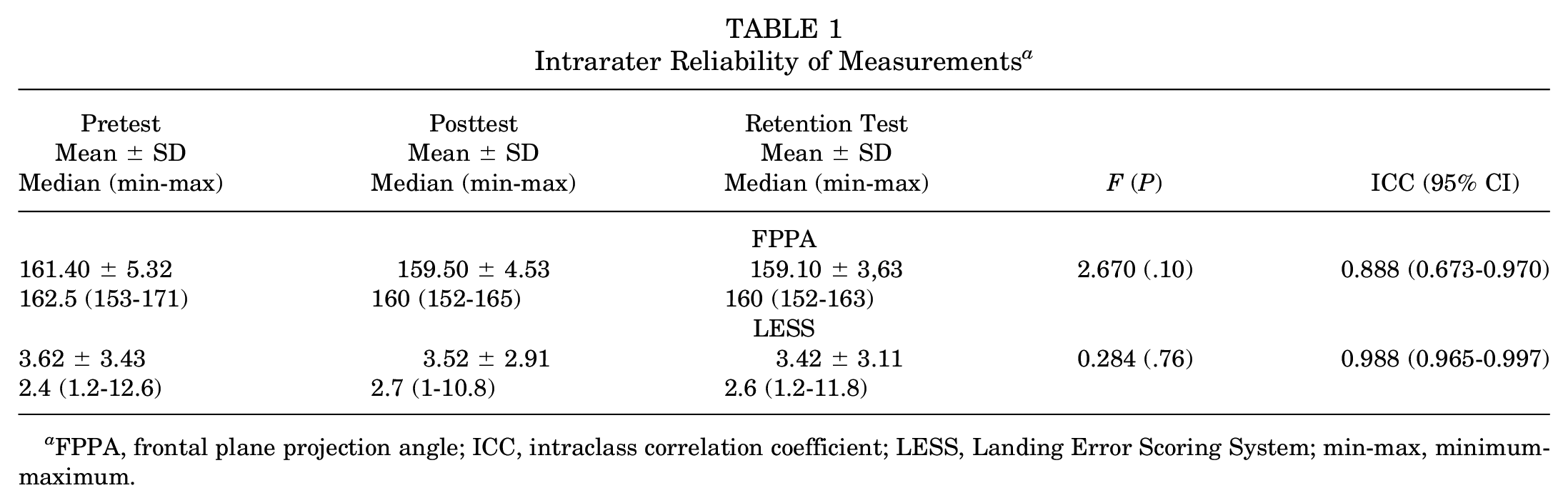
FPPA, frontal plane projection angle; ICC, intraclass correlation coefficient; LESS, Landing Error Scoring System; min-max, minimum-maximum.
Participants
The study included 18- to 24-year-old female second-league basketball and volleyball athletes with body mass index between 18.5 and 25 kg/m2, a frontal plane projection angle >10° during the single-leg squat test, 27 and no experience of trunk and extremity injuries in the past 6 months. Low back pain, congenital musculoskeletal anomaly, visual, auditory, vestibular, or neurological disorders, 13 along with pregnancy, malignancy, and metabolic diseases experienced in the past years were excluded.
The sample size of the study was calculated using the G Power program (Version 3.1.9.7) with an effect size value of 0.8, 95% power, and .05 type 1 error, accepting the change value of the LESS results in the study conducted by Welling et al 36 in 2016 as reference. The number of participants required was calculated as 30, with 10 participants in each group.
Assessments
Participants were asked to complete a demographic data form before the study began. The participant’s age, height, weight, and dominant extremity information were recorded.
Frontal Plane Projection Angle
The reliability of 2-dimensional FPPA measurement in individuals with DKV is very high (ICC, 0.918). 22 FPPA measurement was adapted from the study protocol of Pisirici and Sakul 27 in 2024. While squatting on the leg included in the study, the participant was asked to squat up to 60°, without support and loss of balance. The recording was made for 5 consecutive measurements. Without causing fatigue, the participant’s “mean squat repetition” was accepted as the third measurement. Reference points to measure FPPA in the pelvic segment were determined as spina iliaca anterior superior (SIAS) on both sides. The midpoint of the patella was determined by drawing a straight line along the thigh from the SIAS, and the midpoint of the ankle was determined as the reference point by drawing a straight line from the midpoint of the patella. The FPPA degree was calculated by subtracting the angle value between the femoral and tibial segments, measured from the medial side of the knee, from 360°. FPPA of ≥195° was considered pathological. 27 FPPA measurement was evaluated with the Spark Motion Pro mobile motion analysis system during the single-leg squat test. 29 The FPPA measurement is shown in Figure 2.

Frontal plane projection angle (FPPA) measurement. (A) Reference points for FPPA measurement in the pelvic segment were determined as spina iliaca anterior superior (SIAS) on the included side. The midpoint of the patella was determined by drawing a straight line from SIAS through the thigh, and the midpoint of the ankle was determined as the reference point by drawing a straight line from the midpoint of the patella. (B) The athlete performed a 60° squat on the leg included in the study. (C) The FPPA degree was calculated by subtracting the angle value between the femoral and tibial segments measured from the medial side of the knee from 360°.
Landing Error Scoring System
LESS is a field assessment tool to detect errors in potentially high-risk movement patterns during the landing technique. The LESS has been shown to have concurrent validity and good interrater reliability. 26 LESS measurements were adapted from the study protocol of Welling et al in 2016. 36 The frontal and sagittal plane views of each participant were simultaneously recorded with 2 standard video cameras during the vertical jump, and a total of 17 items were evaluated by replaying the video. According to the score, the participant’s jumping technique was classified as excellent (≤4), good (>4 to ≤5), average (>5 to ≤6), and poor (>6). 36 All participants were initially given a general description of how the drop vertical jump (DVJ) task was performed. The DVJ was adapted from the study protocol of Padua et al in 2009. 26 During the general task training, it was emphasized that the participants should jump from the 30–cm high box and, immediately after landing, jump as high and forward as possible, maintaining the final landing stance for 5 seconds. Participants were allowed to perform 3 trials to get used to the DVJ task. The DVJ task is shown in Figure 3.

Drop vertical jump task. (A, B, C) The athlete jumped horizontally from a 30–cm high box to a target point 50% of her height away. (D, E) The athlete jumped again for maximal vertical jump immediately after landing.
Interventions
Before the study was conducted, an expert video was created to be used for VIG. The expert video is a record of an athlete who is optimally performing the DVJ in accordance with the instructions. Participants were initially given a general description of how the DVJ task was performed. The performed DVJ task was evaluated with LESS, and each athlete’s pretest LESS score and pretest FPPA values were recorded. After the pretest, participants were given instructions specific to their group. The VFIG was given combined focus-of-attention instructions such as “focus on how hard you push yourself off the ground after the jump and how quickly you straighten your knees during this push,” in which EFA and IFA directions were given simultaneously. The VIG was shown an expert video on the screen and was instructed to “perform the DVJ as close to the performance you see in the video.” The instructions given were used separately in previous studies on motor learning and attention focus, and the study results proved that the instructions were effective on performance.6,36 The CG was not given any instructions. After receiving specific instructions for their groups, the participants performed 2 training blocks (TB1, TB2) containing 10 repeated DVJs. Training blocks were adapted from the protocol of Welling et al in 2016. 36 During the training blocks, a 30-second rest break was given after each DVJ task, and a 5-minute rest break was given between TB1 and TB2. In each training block, participants’ instructions were repeated after 5 repetitions of DVJ. While VFIG and VIG participants were given feedback after the training blocks, no feedback was given to the CG. Feedback consisted of the real-time LESS mistakes of the DVJ. After TB2, participants were allowed to rest sufficiently. For the final test evaluation, participants were asked to perform the DVJ task 5 times without being given any instructions or feedback. Posttest FPPA and posttest LESS measurements were recorded. Retention testing was performed after 1 week to check whether the possible difference between groups could be attributed to motor learning principles rather than just motor performance. In the retention test, participants were asked to perform the DVJ task 5 more times. Participants were not given any feedback or instructions for this task. 6 Follow-up FPPA and follow-up LESS scores were recorded during retention testing.
Statistical Analysis
The data were evaluated in the statistical package program SPSS Statistics Standard Concurrent User Version 26 (IBM Corp). Descriptive statistics are shown as mean with standard deviation, and median with minimum-maximum values. Normal distribution of the data of numerical variables was evaluated with the Shapiro-Wilk normality test. Parametric tests were used because numerical descriptive features and variables were normally distributed. Independent-sample t test was used to compare numerical descriptive features of the patients between groups, and chi-square tests (Pearson chi-square/Fisher exact test) were used to compare categorical descriptive features between groups. Mixed-order analysis of variance was used to compare variables in groups according to retention times. In the analysis, Bonferroni correction was applied to compare the main effects. A P value of <.05 was considered statistically significant.
Results
Participants’ demographic characteristics, baseline FPPA, and LESS values were found similar. The general age, weight, height, and body mass index data of the participants were 19 years, 58.27 ± 7.40 kg, 168.43 ± 6.44 cm, and 20.51 ± 2.31 kg/m2, respectively. All baseline values are summarized in Table 2. Participants with right-side dominance were distributed as VFIG (n = 7), VIG (n = 7), and CG (n = 6).
Comparison of Baseline Values of Participants According to Groups a

Values are presented as mean ± SD unless otherwise indicated. BMI, body mass index; CG, control group; FPPA; frontal plane projection angle; LESS, Landing Error Scoring System; VFIG, verbal combined focus–instructed group; VIG, video-instructed group.
Frontal Plan Projection Angle
Statistical improvement occurred in both VFIG and VIG intragroup FPPA assessment at posttest and retention test (respectively, P < .001; P < .001; P < .001). However, there was no statistically significant difference in the FPPA values of the CG (P = .31; P > .05). In the intergroup evaluation, posttest and retention test FPPA values of the VFIG were statistically superior to the results of the VIG (VFIG: F = 47.899, P < .001, η2 = 0.787; VIG: F = 26.711, P < .001, η2 = 0.673), but there was no significant change in the CG (P = .61; P > .05). The results of FPPA values and changes according to groups are given in Table 3 and Figure 2.
Comparison of FPPA Measurements According to Groups at Follow-up Times a

Values are presented as mean ± SD unless otherwise indicated. Sections highlighted in bold are statistically significant (P < .05). CG, control group; FPPA, frontal plane projection angle; VFIG, verbal combined focus–instructed group; VIG, video-instructed group.
Comparison between groups.
Comparison within groups.
Landing Error Scoring System
In the intragroup evaluation, there was a statistical improvement in LESS values in both VFIG and VIG, at the posttest and retention test (respectively, P = .04; P < .001; P < .05). However, there was no statistically significant difference in the CG (P = .90; P > .05). In the intragroup evaluation, the change in LESS value in VIG (F = 16.509; P < .001; η2 = 0.559) was statistically superior compared with the change in VFIG (F = 3.842; P = .04; η2 = 0.228). There was no statistically significant difference between LESS values in the intergroup evaluation (for all, P > .05). The results of LESS values and changes according to group are given in Table 4 and Figure 3.
Comparison of LESS Measurements According to Groups at Follow-up Times a

Values are presented as mean ± SD unless otherwise indicated. Bold values are statistically significant (P < .05). LESS, Landing Error Scoring System; VFIG, verbal combined focus–instructed group; VIG, video-instructed group.
Comparison within groups.
Comparison between groups.
Discussion
The present study examined the effects of combined focus of attention (EFA and IFA) instructions and video instructions on DKV and landing technique on motor learning in the acute period and at the end of the first week in semiprofessional female athletes. The most important findings of the present study were that both VIG and VFIG had significant improvement in FPPA, but VFIG training had a superior improvement in DKV. In the LESS evaluation, it was determined that the VIG showed superior improvement compared with the VFIG in intragroup evaluation although the groups were not statistically superior to each other. Our results did not support the “video instructions will have a superior improvement in landing technique” hypothesis.
Frontal Plane Projection Angle
Verbal instructions can be used in training and exercises to shape a particular movement. 39 It has been suggested that IFA instructions have superior effects on specific muscle activation compared with EFA and when the goal is to increase muscle activation, IFA, the so-called “mind-muscle connection,” should be adopted. 32 EFA instructions also seem to improve athletes’ performance, but improvement is suboptimal for hypertrophic adaptations. 21 Additionally, in the lower extremities, both IFA and EFA instructions have been shown to trigger higher muscle activation compared with baseline, especially in targeted focal areas, and support the conscious control effect when targeting certain points during movement. 20 Literature results seem contradictory in triggering muscle activation, and many studies are showing that IFA instructions are not superior to EFA in improving movement form. 2,20,35 Vidal et al 35 examined the effect of attentional focus instructions on jumping patterns. It has been confirmed that IFA instructions targeting knee extension for the long jump create a better knee-ankle movement pattern by encouraging greater use of knee movement compared with nonspecific EFA instructions. However, there was no statistically significant difference in jumping performance results between groups. Similarly, Almonroeder et al 2 examined the effect of IFA and EFA instructions on the load on the patellofemoral joint during squatting. In the results, they found that the stress and load on the patellofemoral joint decreased after both IFA and EFA verbal instructions. It has been determined that verbal instructions can affect squat mechanics, which may reduce patellofemoral joint loading, but it cannot be concluded which type of focus is superior. 2 Current literature raises curiosity about how IFA and EFA instructions will yield results when they are combined. As a result of our study, DKV showed significant improvement in the VFIG participants. The improvement continued in the retention test. Because our study is the first study using the combined focus of attention instructions, our findings cannot be compared with the literature.
The use of visual instructions produces beneficial results, as it promotes automaticity and permanence of learning with a visual component and therefore helps health/sports professionals to spend less time and investment. 4 Barrios et al 3 investigated the effectiveness of gait retraining using real-time visual feedback on dynamic knee alignment. They found a significant reduction in knee adduction moment via hip internal rotation in individuals who received real-time visual feedback on FPPA while walking on a treadmill. Similarly, Grooms et al 16 investigated the effect of stroboscopic visual feedback on landing mechanics. Their results showed that visuomotor training affected motor control of landing after the jump by increasing hip-knee extension and ankle dorsiflexion and decreasing knee valgus. In our results, the DKV values of the VIG participants showed a significant improvement compared with the beginning, and this improvement continued significantly in the retention test. Our study findings are in line with the results of previous studies that found visual instructions an effective method to promote motor learning.
Verbal attention focus and visual training have been shown to have positive results in improving movement form, but to our knowledge, there are a limited number of studies comparing these 2 techniques with each other. Benjaminse et al 4 investigated the effects of visually instructed EFA and verbally instructed IFA on peak knee joint load during the unexpected sidestep cutting task (sudden change of direction after a side step) in male and female athletes. According to the study results, the difference between the verbal and visual feedback techniques was observed only in the visual EFA group. However, this study was not methodologically similar to ours. Our study is the first to compare video instructions containing the optimal movement pattern with combined verbal instructions. Our study contributes to the literature in this aspect. In our results, an improvement in FPPA was observed in both groups in the intragroup evaluation, and the improvement was sustained in the retention test. In the intergroup evaluations, the results of the VFIG were found to be statistically superior compared with the VIG. It was determined that the combined use of IFA and EFA instructions was effective in bringing the knee to the desired position and made a greater difference in supporting motor learning than the VIG.
Landing Error Scoring System
The difference between EFA and IFA is slight, but this difference allows athletes to adapt more freely to the changing environment and achieve more successful adaptation. 12 Dalvandpour et al 11 examined the changing DVJ task kinematics in professional football players who received neuromuscular training with EFA and IFA instructions. As a result of the study, it was concluded that EFA-instructed training significantly improved sagittal plane hip and knee mechanics compared with IFA. 10 However, there are also results showing that EFA and IFA instructions given after the jump are not superior to each other, showing that both have a positive effect on the alignment of the lower extremity after the jump. 37 However, no study has been found examining the kinetic and kinematic effects of combined IFA and EFA instructions on landing after DVJ performance. In our study results, VFIG had an improvement in the LESS posttest and retention test results. To the best of our knowledge, because our study is the first study in the literature examining the effect of combined attention focus instruction on landing mechanics, our results cannot be compared with the literature.
It was observed that athletes who practiced with video instructions made a more successful transition between observing and practicing, achieved a meaningful transfer, and improved their landing pattern after the jump.6,36 Benjaminse et al 6 investigated the effects of verbal EFA, verbal IFA, and visual video instruction training used during a jump landing task on lower extremity kinematics and kinetics during a sidestep cutting task. The results showed that the EFA and video instruction groups were more successful in skill transfer. Additionally, the study found that women in the visual instruction group exhibited a softer landing technique and achieved a lower LESS score. 6 Similarly, Welling et al 36 compared the effects of different types of verbal and visual instructions on landing jump technique and jump performance. According to study findings, women in both the EFA and the visual training groups and men in the visual training group significantly improved their LESS scores over time, while maintaining their performance 1 week later. In our results, a statistically significant improvement was seen in both verbal and visual groups in the intragroup evaluation, and this improvement continued at the end of the first week. However, the groups were not found to be superior to each other. Considering that, to our knowledge, there has been no previous study in which combined focus of attention instructions were used together, our results are compatible with the existing literature. Although the groups did not have any superiority over each other, the change in the visual group was significantly higher than that in the verbal group. We interpret the reason for the higher change in the visual instructions as follows: Studies have shown that jumping and performing a secondary task that requires attention at the same time negatively affects landing mechanics and causes an increase in ACL load.1,2,11,23 The reason for the lower performances obtained here can be shown as the capacity model of attention.31,33 If the focus of attention is divided by visual and auditory information given simultaneously, processing of sensory information becomes difficult and a decrease in performance is observed. 18 In our study, VFIG participants divided the focus of attention into 2 by receiving a combination of both IFA and EFA instructions. Based on the capacity of the attention model, athletes’ simultaneous processing of input from 2 different focal points resulted in a statistically significant increase in their performance, but as expected, no superiority was found in the VIG. On the basis of these findings, we see that learning through observation and practice as well as verbal combined attention focus instructions is a powerful tool and that we have obtained findings that will expand the framework of existing rehabilitation programs. However, there is a need for more studies in this field in the literature.
Both combined verbal and video instructions provide the athlete with the correct kinematics through motor learning during the landing-after-DVJ task and encourage automaticity and permanence in the brain. Considering that female athletes have a higher risk of ACL injury due to their higher DKV value compared with men, we think that video and combined verbal instructions are important in reducing the knee valgus value and improving the landing technique, thus reducing the injury rate.
To our knowledge, this study is the first research to compare video instructions using a combination of verbal EFA and IFA instructions. While both types of instructions were effective in improving knee valgus and landing technique, verbal combined focus instructions were found to be superior in improving valgus.
Limitations
Our study is not without limitations. A limitation of the LESS score is that all identified movement errors are grouped into a single overall score, which may include any combination of individual-specific movement errors. It could not be evaluated precisely which subcomponent of LESS resulted from the existing improvement. Another limitation of our study is that our follow-up measurements were not evaluated after a long period.
Conclusion
Our study demonstrated that while both types of instructions were effective in improving knee valgus and landing technique, verbal combined focus instructions were superior in improving valgus. In light of this, our results suggest that using both verbal and video instructions is crucial for reducing knee valgus and enhancing landing technique, which may help reduce the injury rate.
Footnotes
Acknowledgements
The authors thank physical therapist Oktay Şenozan for contributing to the study.
Final revision submitted November 8, 2024; accepted November 14, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Istanbul Medipol Universitesi (E-10840098-202.3.02-643).