
Abstract
Background:
Anatomic labral repair is paramount when restoring the hip suction sealing mechanism in femoroacetabular impingement syndrome (FAIS) surgery. All-suture knotless tensionable anchors have been recently proposed as an alternative; however, data are scarce.
Purpose:
To report patient-reported outcome measure (PROM) scores at a minimum 2-year follow-up for patients who underwent primary hip arthroscopic surgery with labral repair using an all-suture knotless tensionable anchor with the controlled-tension anatomic technique in the setting of FAIS.
Study Design:
Case series; Level of evidence, 4.
Methods:
Data were prospectively collected, and patients who underwent primary hip arthroscopic surgery for the treatment of FAIS and labral tears using an all-suture knotless tensionable anchor with the controlled-tension anatomic technique between April 2019 and February 2021 were included. Patients were excluded if they had previous ipsilateral hip conditions or surgery, Tönnis grade >1, or workers’ compensation insurance. Baseline and minimum 2-year follow-up scores for the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), Hip Outcome Score–Sport-Specific Subscale (HOS-SSS), visual analog scale (VAS) for pain, International Hip Outcome Tool–12 (iHOT-12), and patient satisfaction were collected. Rates of achieving the minimal clinically important difference (MCID), the Patient Acceptable Symptomatic State (PASS), and the maximum outcome improvement (MOI) as well as the rate of secondary procedures were reported. Survivorship was defined as no conversion to total hip arthroplasty.
Results:
A total of 200 patients (200 hips) were included for analysis with a minimum 2-year follow-up. There were 141 female (70.5%) and 59 male (29.5%) patients with a mean age and mean body mass index of 33.3 ± 13.5 years and 24.5 ± 4.8 kg/m2, respectively. A significant improvement on all PROMs from baseline to a minimum 2-year follow-up was reported (P < .05). The cohort demonstrated high rates of achieving the MCID for the mHHS (91.0%), NAHS (92.0%), HOS-SSS (93.5%), and VAS (92.5%); high rates of achieving the PASS for the mHHS (80.5%), NAHS (73.0%), and HOS-SSS (77.0%); and high rates of achieving the MOI for the NAHS (74.5%) and HOS-SSS (76.5%), with 95.5% of patients achieving the MCID or PASS for at least 1 metric. The survivorship rate at a minimum 2-year follow-up was 97.5%, and 4.0% of patients underwent subsequent revision hip arthroscopic surgery at a mean of 31.4 months.
Conclusion:
At a minimum 2-year follow-up, patients who underwent primary hip arthroscopic surgery for FAIS with labral tears using an all-suture knotless tensionable anchor demonstrated a significant improvement on all the PROMs examined. Moreover, high achievement rates of the MCID, PASS, and MOI were reported. Based on this prospective analysis, labral repair using an all-suture knotless tensionable anchor seems to be a safe and valid option.
Keywords
Hip arthroscopic surgery is currently the standard of care for the management of arthroscopically accessible femoroacetabular impingement syndrome (FAIS) and labral tears. 19 A labral tear is one of the most common intraoperative findings in FAIS surgery, 23 and labral repair is the preferred surgical method, particularly over debridement. 14 Superior outcomes and less risk of conversion to total hip arthroplasty have been reported at midterm to long-term follow-up after labral repair compared with debridement.7,16,29 In fact, labral repair is part of arthroscopic FAIS surgery in almost 80% of cases. 41
Acetabular labral repair can be performed with different types of suture anchors. Benca et al 1 compared hard-body knotless versus knotted anchors and reported similar biomechanical properties for both options. Safran et al 35 compared different versions of hard-body knotless anchors and found that knotless anchors tended to fail by suture pullout from the anchor; however, they also suggested that the stiffness of these anchors would guarantee that minimal displacement of the labral repair construct would take place under physiological loads. In vivo, when comparing hard-body knotless to knotted anchors for arthroscopic acetabular labral repair, Rhee et al 33 reported similar and comparable outcomes at 2-year follow-up. Maldonado et al 22 also reported a significant improvement on patient-reported outcome measures (PROMs) at a minimum 2-year follow-up using hard-body knotless anchors with the controlled-tension anatomic technique in primary hip arthroscopic surgery for FAIS. Compared with hard-body anchors, all-suture knotless tensionable anchors are smaller in diameter, providing bone preservation advantages with less risk of acetabular subchondral or intra-articular penetration.37,40 Favorable short-term outcomes have been reported after labral repair with knotted all-suture anchors,3,5 and in shoulder surgery, arthroscopic soft Bankart repair using all-suture knotless anchors has been proven to be an effective and safe option. 32 Nonetheless, there are scarce clinical data reporting outcomes for all-suture knotless tensionable anchors in hip arthroscopic surgery.
The purpose of the present study was to report PROM scores at a minimum 2-year follow-up for patients who underwent primary hip arthroscopic surgery with labral repair using the 1.8-mm Hip FiberTak (KHFT; Arthrex) with the controlled-tension anatomic technique in the setting of FAIS. It was hypothesized that significant improvements on all the PROMs examined and high achievement rates of the minimal clinically important difference (MCID), the Patient Acceptable Symptomatic State (PASS), and the maximum outcome improvement (MOI) would be obtained at a minimum 2-year follow-up.
Methods
All patients included in this study participated in the American Hip Institute Hip Preservation Registry and provided informed consent. The present study represents a unique analysis. This study was performed in accordance with ethical standards of the 1964 Declaration of Helsinki and with relevant regulations of the United States Health Insurance Portability and Accountability Act. Institutional review board approval was received for the study protocol.
Patient Selection
Institutional data from April 2019 to February 2021 were prospectively collected. A total of 200 consecutive patients who underwent primary hip arthroscopic surgery for FAIS and labral tears by the senior surgeon (B.G.D.) using the KHFT with a minimum 2-year follow-up were included. Exclusion criteria were if they had previous ipsilateral hip conditions such as avascular necrosis, Legg-Calve-Perthes disease, slipped capital femoral epiphysis, Ehlers-Danlos syndrome, pigmented villonodular synovitis, and inflammatory disease or had previous ipsilateral hip surgery; had Tönnis grade >1; had workers’ compensation insurance; were unwilling to be part of the study; underwent labral repair with a different type of anchor; and underwent labral reconstruction, labral augmentation, or selective debridement. 25
Clinical Examination and Imaging
Before surgery, all patients underwent a physical examination that assessed range of motion and signs of FAIS, as indicated by positive lateral, anterior, and posterior impingement test results, performed by the senior surgeon (B.G.D.). 19 Additionally, all patients underwent preoperative radiographic imaging, including a 45° Dunn view, false profile view, and anteroposterior pelvic view in the upright and supine positions. 4 For assessing acetabular coverage, the anterior center-edge angle was measured on the false profile view according to the method described by Lequesne and de Seze 17 , and the lateral center-edge angle was measured on the anteroposterior pelvic view in the supine position according to the method described by Wiberg 4 and later modified by Ogata et al. 31 The alpha angle was measured on the 45° Dunn view, and an alpha angle >55° was defined as a cam-type deformity. 6 The degree of osteoarthritis was assessed using the Tönnis classification system. 38 Magnetic resonance imaging (1.5 T) was performed to determine the presence of labral tears.
Surgical Indications
A detailed patient history, physical examination, and radiographic analysis were collectively utilized preoperatively by the senior surgeon (B.G.D.) to evaluate appropriate candidates for hip arthroscopic surgery. Before being recommended for surgery, all patients reported pain that interfered with activities of daily living for a minimum of 3 months and that did not improve with nonoperative treatment, including activity modification, nonsteroidal anti-inflammatory drugs, physical therapy, intra-articular ultrasound-guided injections, and rest. 10 Patients with persistent hip pain and disability, despite nonoperative treatment, were indicated for surgery.
Surgical Technique
Hip arthroscopic procedures were carried out utilizing the anterolateral, midanterior, and distal anterolateral accessory portals with the patient in a modified supine position. 26 Interportal capsulotomy was performed for all the patients. 13 A diagnostic arthroscopic examination was conducted in every instance to evaluate the joint's condition. Labral tears were graded using the Seldes classification system. 36 The chondrolabral junction was assessed using the acetabular labrum articular disruption (ALAD) classification system. 39 The extent of acetabular and femoral cartilage damage was categorized using the Outerbridge classification system. 2
The treatment decision for labral tears was based on the senior surgeon's (B.G.D.) opinion and expertise. 8 When labral repair was the alternative selected, acetabular capsular elevation and preplanned acetabular rim trimming were performed without detaching the labrum. 21 Labral tears underwent repair utilizing the KHFT with the controlled-tension anatomic technique described by Maldonado et al 22 (Figure 1).
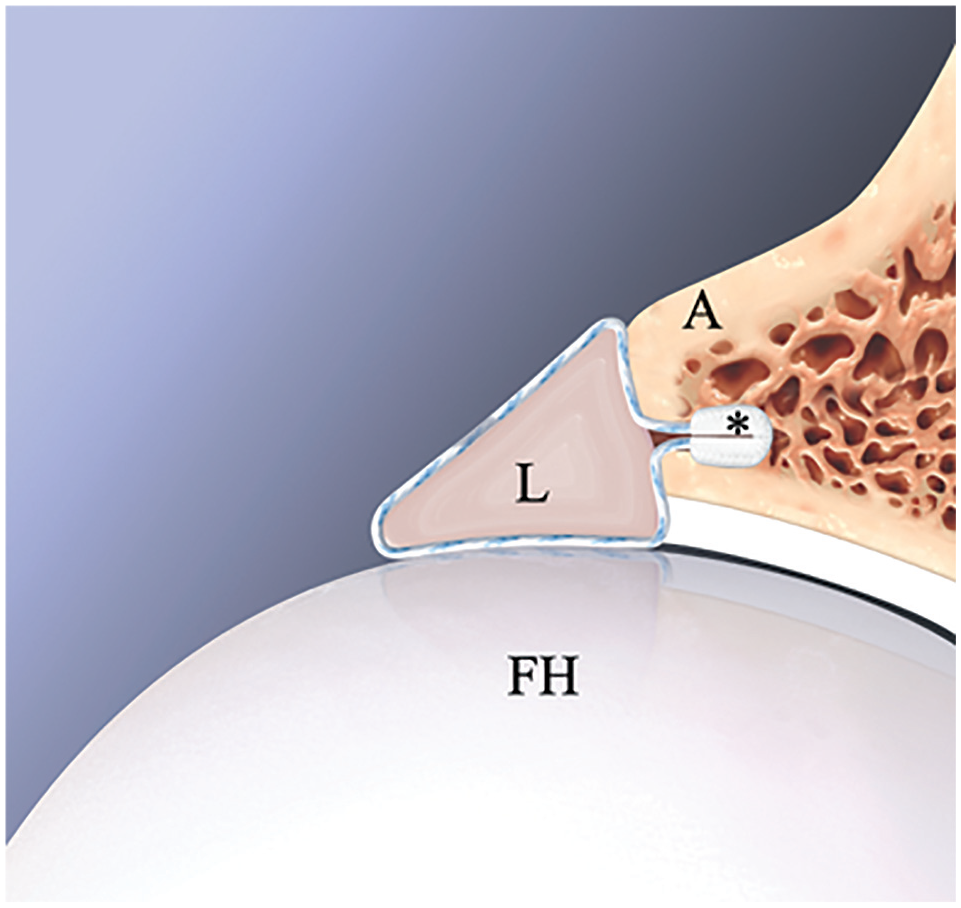
Sagittal view illustration of labral repair using the 1.8-mm Hip FiberTak (*; Arthrex). The all-suture knotless anchor was placed in the acetabular rim (A) as close as possible to the subchondral bone. After applying appropriate tension using the controlled-tension anatomic technique, the anatomy of the labrum (L) was preserved, and excellent contact between the labrum and femoral head (FH) was achieved, restoring the suction sealing mechanism.
KHFTs were placed from the most anteromedial aspect to the most posterolateral aspect of the labral tear. Looped repair was routinely performed (Figure 2). Tension was applied to the repair construct as needed using the tensionable mechanism until anatomic labral compression was achieved. 22 After all intra-articular work was performed, hip traction was released, and restoration of the labral seal was confirmed in all cases by releasing hip traction and obtaining perfect contact between the repaired labrum and femoral head (Figure 2).

Intraoperative images of a right hip viewed from the distal anterolateral accessory portal with a 70° arthroscope. (A) The right hip is placed under traction, and labral repair using a circumferential looped technique was performed using three 1.8-mm Hip FiberTak anchors (Arthrex). (B) Traction was released, and restoration of the hip suction seal was observed. A, acetabulum; C, capsule; FH, femoral head; L, labrum; *, 12-o’clock position.
Spherical femoroplasty using a bur was performed under fluoroscopic guidance. 27 All patients underwent capsular closure unless otherwise indicated by insufficient capsular tissue.
Rehabilitation Protocol
Postoperatively, patients were advised by the senior surgeon (B.G.D.) to follow individualized rehabilitation programs based on the surgical procedures performed intraoperatively. Patients were instructed to ambulate using crutches and to continue using a hip brace for the first 2 weeks postoperatively. Additionally, patients were recommended to ride a stationary bicycle or use a continuous passive motion machine daily for the first 8 weeks postoperatively before transitioning to a dedicated 5-stage physical therapy program specific to the patient's surgical procedures. Finally, patients were advised to take naproxen 500 mg twice daily for 6 weeks postoperatively to minimize the risk of heterotopic ossification. Aspirin 81 mg twice daily for 2 weeks postoperatively was indicated for deep vein thrombosis prophylaxis.
Patient-Reported Outcome Measures
All patients completed questionnaires preoperatively and postoperatively at a minimum 2-year follow-up. The PROMs included the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), Hip Outcome Score–Sport-Specific Subscale (HOS-SSS), and visual analog scale (VAS) for pain. In addition, the latest follow-up scores for the International Hip Outcome Tool–12 (iHOT-12) and patient satisfaction were also reported.
The rate of patients who achieved the MCID using the method described by Norman et al, 30 the PASS, 22 and the MOI were recorded. 24 Secondary procedures were reported, and survivorship was defined as no conversion to total hip arthroplasty. The calculated thresholds of achieving the MCID were 6.8 for the mHHS, 7.7 for the NAHS, 9.7 for the HOS-SSS, and 1.0 for the VAS. 30 The thresholds of achieving the PASS for the mHHS, NAHS, HOS-SSS, and VAS were 74.0, 85.6, 75.0, and 2.16, respectively. 12 The thresholds of achieving the MOI for the mHHS, NAHS, HOS-SSS, and VAS were 54.8, 52.5, 44.6, and 55.5, respectively. 24
Statistical Analysis
A 2-tailed t test or its nonparametric equivalent was used to analyze continuous data, and the chi-square test or Fisher exact test was used to assess categorical data. The F test and Shapiro-Wilk test were used to determine variance equality and normality. All statistical analyses were conducted using Excel with the Real Statistics Add-In package (Microsoft) or RStudio (Version 4.1.2; Posit). A P value <.05 was set as the statistical significance threshold for analysis.
Results
Patient Characteristics and Radiographic Measurements
A total of 200 patients (200 hips) met the inclusion criteria (100% follow-up). Detailed patient data are shown in Table 1. Radiographic data are presented in Table 2.
Patient Characteristics a

Data are presented as n (%) or mean ± SD (range).
Radiographic Measurements a

Data are presented as n (%) or mean ± SD.
Intraoperative Findings
There were 75 Seldes type I labral tears (37.5%), 38 Seldes type II labral tears (19.0%), and 87 Seldes combined type I and II labral tears (43.5%). Detailed intraoperative data are summarized in Table 3.
Intraoperative Findings a

Data are presented as n (%). ALAD, acetabular labrum articular disruption.
Surgical Procedures
The mean number of KHFTs required per case was 4.32 ± 0.83 (range, 1-7). Capsular closure was performed in 193 patients (96.5%). All the patients underwent femoroplasty, and 189 (94.5%) underwent acetabuloplasty. Detailed data on surgical procedures are presented in Table 4.
Surgical Procedures a
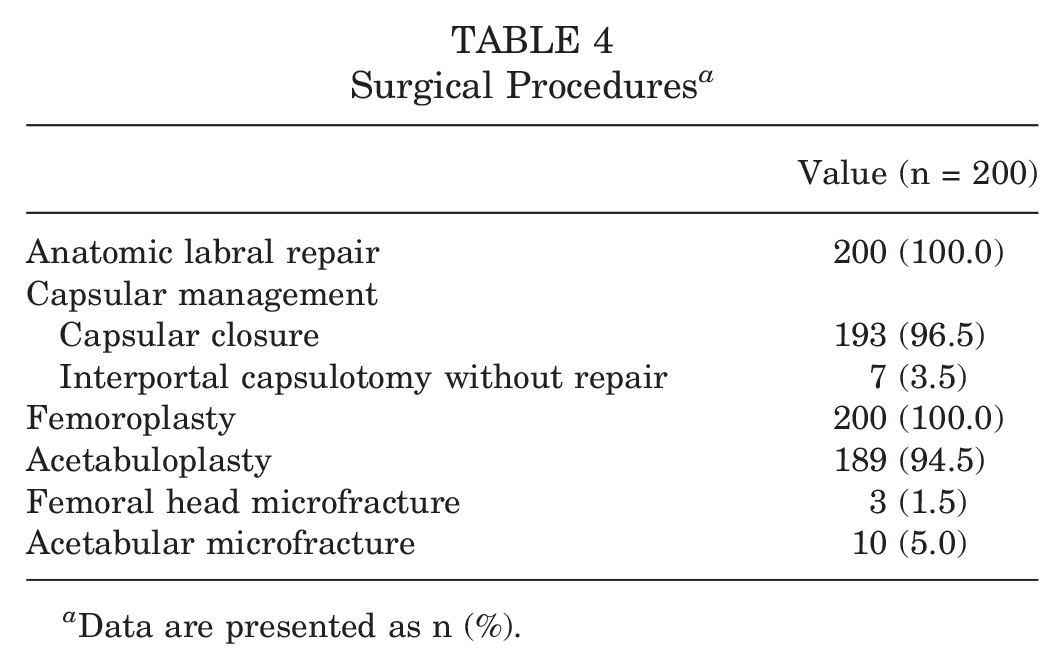
Data are presented as n (%).
PROM Scores
At a minimum 2-year follow-up, patients demonstrated a significant improvement (P < .05) on the mHHS, NAHS, HOS-SSS, VAS for pain, and iHOT-12 from preoperatively. Additionally, patients exhibited favorable patient satisfaction scores at the latest follow-up, with a mean score of 8.1. A complete summary of PROM scores is found in Table 5 and Figures 3 and 4.
Patient-Reported Outcome Measure Scores a

Data are presented as mean ± SD (95% CI). Boldface indicates a statistically significant difference (P < .05). HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale.

Preoperative and postoperative patient-reported outcome measure scores. Data are reported as means. *A statistically significant difference (P < .05). HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score.

Preoperative and postoperative visual analog scale (VAS) and patient satisfaction scores. Data are reported as means.
High achievement rates of the MCID and PASS were reported, with 95.0% of patients achieving the MCID for at least 1 metric, 86.5% of patients achieving the PASS for at least 1 metric, and 95.5% of patients achieving either the MCID or PASS for at least 1 metric at the most recent follow-up. A full summary of clinimetric data is presented in Table 6.
Clinical Benefit Measures a

Data are presented as n (%). HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; MOI, maximum outcome improvement; NAHS, Non-Arthritic Hip Score; PASS, Patient Acceptable Symptomatic State; VAS, visual analog scale.
Secondary Procedures
The arthroplasty-free survivorship rate at a minimum 2-year follow-up for patients in the cohort was 97.5%. There were 8 hips (4.0%) that underwent revision hip arthroscopic surgery at a mean of 31.4 months postoperatively. Data regarding secondary surgery are presented in Table 7. The Kaplan-Meier survivorship curve is illustrated in Figure 5. Intraoperative procedures performed during revision hip arthroscopic surgery are presented in Table 8. Intraoperative findings regarding ALAD and Outerbridge grades in patients requiring conversion to total hip arthroplasty are presented in Table 9.
Secondary Procedures a

Data are presented as n (%) unless otherwise indicated. THA, total hip arthroplasty.

Kaplan-Meier survivorship curve.
Intraoperative Procedures Performed During Revision Hip Arthroscopic Surgery a
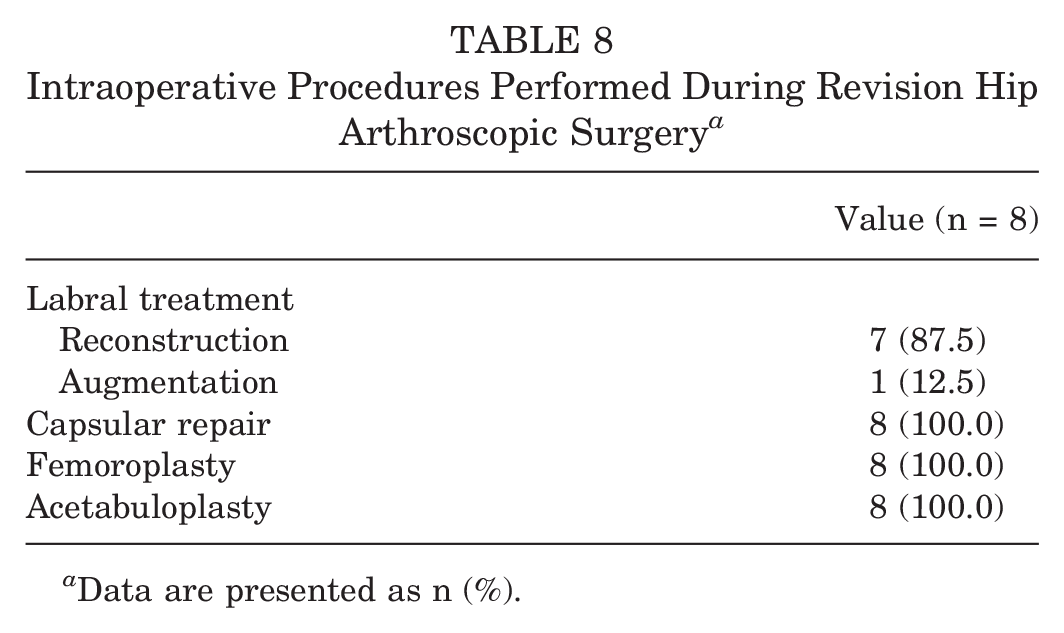
Data are presented as n (%).
Intraoperative Findings of Patients Converting to Total Hip Arthroplasty a

ALAD, acetabular labrum articular disruption.
Discussion
The main finding of this study is that using KHFTs for primary labral repair in the setting of FAIS was safe and yielded statistically significant improvements on several PROMs and excellent clinical results, with high achievement rates of the MCID and PASS and a survivorship rate of 97.5%, at a minimum 2-year follow-up.
In general, knotless technology has the potential advantage of less time-consuming acetabular labral repair, and the abrasive effect of knots is no longer part of the equation.9,15,37 The KHFT has characteristics worthy of mention. It is a 1.8-mm U-shaped polyester anchor, and the deployment mechanism works by compressing the sleeve against the tip of the anchor inserter instead of against the acetabular cortical bone, making it theoretically less dependent on bone density. 40 Nevertheless, it is critical to pull on the KHFT's sutures after deploying them to diminish the risk of pullout. 34
Clinical outcomes using all-suture knotted anchors for arthroscopic acetabular labral repair have been published. In a case series that included 24 patients (13 male and 11 female) with a mean age of 29.42 years, Di Benedetto et al 5 reported a significant improvement on several PROMs at a minimum 1-year follow-up using 1.4-mm polyester all-suture knotted anchors. After 434 consecutive hip arthroscopic procedures with labral repair using 1.8-mm polyester all-suture knotted anchors, Byrd et al 3 reported an overall pullout failure rate of 1.6%, supporting the use of all-suture anchors for hip labral repair. Anecdotally, pullout failure has been an extremely infrequent event using the KHFT in our experience.
Data on the KHFT for labral repair during hip arthroscopic surgery are scarce. Nonetheless, biomechanical and clinical evidence from shoulder surgery is available. In a cadaveric study, Lacheta et al 15 demonstrated that Bankart repair using the KHFT had comparable values of ultimate load, first failure load, and stiffness compared with the 1.8-mm all-suture knotted version. Similar results were reported by LeVasseur et al 18 ; however, they demonstrated that with the controlled-tension anatomic technique, retensioning was possible, achieving improvements in labral-capsular construct tension. After arthroscopic soft Bankart repair using the KHFT described in the current investigation, Pearce et al 32 reported significant improvements on PROMs and high patient satisfaction in a case series that included 31 active patients (8 female and 23 male) with a mean age of 29 years at a minimum 2-year follow-up. After labral repair using hard-body knotless anchors with the controlled-tension anatomic technique, Maldonado et al 22 reported a significant improvement on several PROMs at a minimum 2-year follow-up in a cohort that included 309 hips prospectively analyzed. In the present study, labral retears and residual bony impingement were found to be the reasons for revision hip arthroscopic surgery. During second-look procedures, labral tissue degeneration but no failure of the KHFT itself was encountered, and labral reconstruction/augmentation using the same all-suture anchor technology was performed. 34
This study has several strengths. This is one of the few investigations of a prospective analysis with the use of the KHFT for primary labral repair in the context of FAIS with a minimum 2-year follow-up. The prospective data collection limited the risk of selection and recall biases. The validity and generalizability of the results were increased by using multiple validated, functional hip outcome tools specific to nonarthritic hips. Moreover, psychometric tools such as the MCID, PASS, and MOI were utilized with the goal of providing clinical significance to the results presented. 12
Limitations
Limitations of the present study need to be acknowledged. This is a case series study; therefore, there was no control group to compare the presented results. Further, with the data presented, we cannot conclude that the KHFT is superior to other types of knotless or knotted anchor designs. 20 Pullout failure is possible with all-suture anchor technology; although this event is rare, data on this were not recorded in the database. This study included data from a single high-volume hip preservation institution, and results may not be reproducible.11,28 There was a minimum follow-up of 2 years; a longer follow-up time is mandatory to determine the results’ durability. The PROM scores of the patients who underwent secondary surgery were considered endpoint outcomes and were not included in PROM analysis.
Conclusion
At a minimum 2-year follow-up, patients who underwent primary hip arthroscopic surgery for FAIS with labral repair using the KHFT demonstrated a significant improvement on all the PROMs examined. Moreover, high achievement rates of the MCID, PASS, and MOI were reported. Based on this prospective analysis, acetabular labral repair using the KHFT seems to be a safe and valid option.
Footnotes
Final revision submitted November 5, 2024; accepted November 14, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by Arthrex (IIRA-01156). D.R.M. has had ownership interests in the American Hip Institute and affiliates, North Shore Surgical Suites, and Munster Specialty Surgery Center; research support from Arthrex, Stryker, Smith & Nephew, and Ossur; consulting fees from Arthrex, Medacta, Stryker, and SI-Bone Inc; has received educational support from Arthrex, Stryker; speaking fees from Arthrex; travel and lodging from Arthrex and Stryker; food and beverage from Arthrex, DJO Global, Medacta, Stryker, Zimmer Biomet, DePuy Synthes Sales, Medtronic, Trice Medical, Medwest Associates, SI-Bone Inc, Xiros Inc, Intellijoint Surgical Inc, Electronic Waveform Lab Inc; royalties from Arthrex, DJO Global, Medacta, Orthomerica; patents with Arthrex, Orthomerica, and DJO Global. D.R.M. is Director of Hip Preservation at St. Alexius Medical Center and a board member for the American Hip Institute Research Foundation, AANA Learning Center Committee, the Journal of Hip Preservation Surgery, Arthroscopy: The Journal of Arthroscopic and Related Surgery, AOSSM Research Committee, and ISHA Executive Board. B.G.D. has had ownership interests in the American Hip Institute, Hinsdale Orthopaedics, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center; has received research support from Arthrex, the Kauffman Foundation, and Stryker; has received consulting fees from Adventist Hinsdale Hospital, Arthrex, Medacta, and Stryker; has received educational support from Arthrex, Breg, Medacta, and Medwest Associates; has received speaking fees from Arthrex; has received honoraria from Medacta; has received travel and lodging from Arthrex, Medacta, and Stryker; has received food and beverage from Arthrex, Medacta, Stryker, DJO Global, and Zimmer Biomet; and has received royalties from Amplitude, Arthrex, DJO Global, Medacta, Stryker, and Orthomerica. B.G.D. is also the Medical Director of Hip Preservation at St Alexius Medical Center and a board member of the American Hip Institute Research Foundation, the Arthroscopy Association of North America Learning Center Committee, the Journal of Hip Preservation Surgery, and Arthroscopy: The Journal of Arthroscopic and Related Surgery. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from WCG (20242189).