
Abstract
Background:
The role of forearm rotation at the time of ulnar collateral ligament (UCL) reconstruction (UCLR) graft tensioning is poorly understood.
Purpose:
To compare postoperative medial elbow joint gapping in cadaveric elbows after UCLR graft tensioning with the forearm in supination versus pronation.
Study Design:
Descriptive laboratory study.
Methods:
A total of 18 full-arm human specimens were stripped of soft tissue except elbow ligamentous and capsular structures. Elbows with an intact, native ligament were tested for medial elbow gapping during valgus stress at 30°, 60°, and 90° with the forearm in neutral, maximal supination, and maximal pronation. Joint gapping was determined with a 3-dimensional motion capture system and calibrated digitized points on the ulna and humerus. The UCL was transected, and reconstruction was performed using a standard docking technique. Elbows were randomized to full supination or pronation at the time of final graft tensioning, and medial elbow joint gapping was again measured for the same positions and same technique. Analysis of variance test was used to compare differences in native and postoperative medial elbow joint gapping (P < .05).
Results:
The position of forearm rotation did not affect the amount of medial elbow joint gapping during valgus stress at all tested elbow flexion angles with an intact, native UCL. The position of forearm rotation during UCL graft tensioning also did not affect postoperative medial elbow joint gapping during valgus stress at all tested elbow flexion angles.
Conclusion:
Forearm rotation with an intact UCL and at the time of UCL graft tensioning did not affect the amount of medial elbow joint gapping during valgus torque.
The anterior bundle of the ulnar collateral ligament (UCL) is the primary static valgus restraint of the elbow joint.6,23 Certain athletic movements, such as throwing a baseball, can increase the risk of UCL injury due to the large, repetitive valgus force generated during the overhead throwing motion with near supraphysiologic loads experienced on the athlete’s medial elbow during a pitch.1,23 On average, a professional baseball pitcher generates 7600 deg/s rotational velocity with elbow varus torque approaching 75 to 80 Nm.12,22
The role of forearm rotation (supination and pronation) is an important concept in the biomechanics of throwing a baseball. Some pitches, such as the slider and the curveball, often require supination throughout the release point while other pitches, such as certain fastballs and the changeup, require pronation. Various biomechanical studies using motion analysis from infrared cameras and retroreflective markers have found minimal difference between elbow torque created by fastballs, curveballs, and slider pitches.10,11 Specifically, Escamilla et al 10 suggested that a changeup is the least forceful pitch on the elbow, mostly due to the generalized decreased speed of the kinetic chain during its execution, resulting in favorable arm kinetics. Currently, it is poorly understood if these different positions of forearm pronation or supination during a valgus load affect the amount of medial elbow joint gapping or UCL strain.
Furthermore, the rate of UCL injuries continue to rise in both amateur and professional baseball pitchers.4,8,9,13,16,18,24 Consequently, more athletes are undergoing UCL surgeries, specifically UCL reconstruction (UCLR) or repair with internal brace (Arthrex) augmentation.4,8,9,13,16,18,24 Regardless of UCLR technique, there are multiple factors that the surgeon must consider when tensioning the UCL graft or internal brace. The amount of elbow flexion, the use of varus force, and the type and amount of forearm supination or pronation are important factors that may influence the tension of the UCL graft postoperatively. As a general principle, most ligament reconstruction grafts are tensioned with the joint in the opposite position of the resisted force on the graft. Therefore, most elbow surgeons agree on placing the elbow around 30° to 60° of elbow flexion along with a varus force at the time of UCL graft tensioning. However, it is less understood what position of forearm rotation best reduces the medial elbow joint in the setting of isolated UCL insufficiency surgery.
The effect of supination and pronation at the time of final graft tensioning during UCLR has not been quantified. It is currently unknown which forearm position, if any, results in the least amount of elbow joint gapping postoperatively. Therefore, it is controversial which forearm position is ideal during UCLR graft tensioning. Pomianowski et al 15 showed that forearm pronation increased varus and valgus laxity in a cadaveric biomechanical model regardless of the status of the UCL. Consequently, many surgeons prefer tensioning a UCLR graft during maximal supination with the belief that this maximally reduces the medial elbow joint space, allowing for a maximally taut graft.5,20 However, others advocate for placing the arm in the neutral position or even a pronated position to prevent overconstraint of the medial elbow. 3 A biomechanical, cadaveric model comparing UCL graft tensioning in both supination and pronation would help provide clarity for optimal position of the forearm during UCLR graft tensioning.
Therefore, the objectives of the current study were the following: (1) to determine if placing the forearm in maximal supination or pronation affects the amount of elbow joint gapping with a native, intact UCL during valgus load and (2) to determine if placing the forearm in supination or pronation at the time of UCLR graft tensioning results in a change in postoperative medial elbow joint gapping during valgus load. We hypothesized that (1) medial elbow joint gapping would be larger when the forearm was in maximal pronation with an intact, native UCL and that (2) tightening the UCL graft in maximal pronation would result in larger postoperative medial elbow joint gapping relative to the intact UCL state during postoperative valgus testing.
Methods
Biomechanical Setup
The current study received institutional review board exemption, as cadaveric specimens were deidentified prior to procurement. Eighteen fresh-frozen full-arm human specimens (male, aged 27-65 years) were stripped of soft tissue leaving only the elbow ligamentous and capsular structures intact. The humerus was placed in a clamp such that the axis connecting the epicondyles was perpendicular to the floor and the forearm was free to move. The medial side of the elbow joint was facing upward. Retroreflective markers were attached to both the humerus and the ulna just outside the native UCL footprint and anticipated UCLR surgical site. Throughout testing, a 3-dimensional motion capture system (Motion Analysis Corporation) using Eagle-IV cameras at 4 megapixel and 60 Hz (Eagle Eye Networks, Inc) was used to record the position of the markers and thus record the position of the humerus and ulna with an accuracy of 0.1 mm. The 0.1-mm accuracy was based on calibration of the motion capture system, which was performed at the beginning of each testing session. Medial joint gapping was determined by digitizing a point on either side of the joint and calculating the distance between these points for all test configurations (Figure 1).
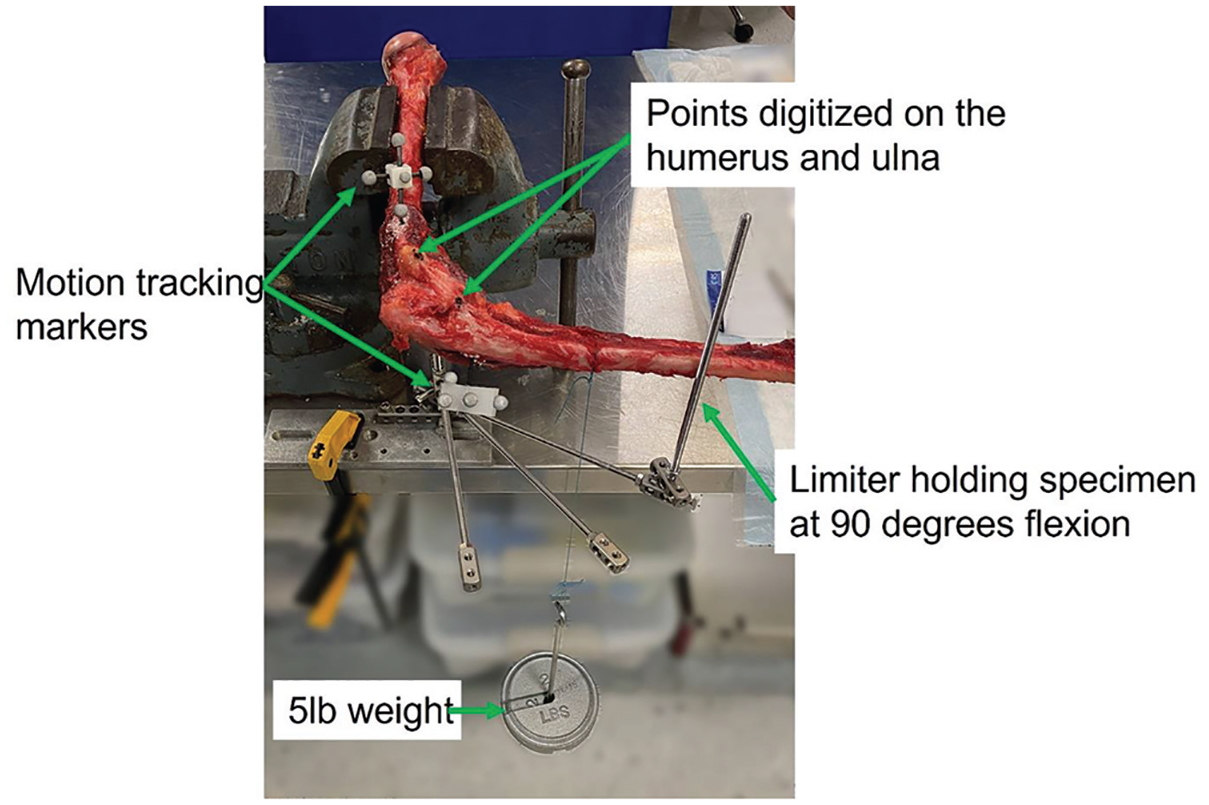
Picture of setup for native and reconstructed elbow ulnar collateral ligament valgus stress testing.
Native UCL Testing
All specimens were statically tested at 30°, 60°, and 90° of elbow flexion with the forearm in full pronation, full supination, and neutral in a loaded and unloaded configuration. To set forearm position, a screw was inserted into the distal radius, and a spring scale was connected to this screw such that the hook was against the bone. Full supination and full pronation were determined by applying 0.91 kg of force to the distal radius with the spring scale to rotate the forearm into the desired testing position. A pin was then placed across the radial and ulnar styloids to hold the forearm in that position. Neutral position was pinned with the axis through the radial styloid parallel to the floor. Valgus load was applied by hanging a 2.27 kg weight on the ulna 13 cm from the joint line to produce an approximately 3-Nm valgus torque (22.2 N × 0.13 m = 2.9 N·m).
UCLR Testing
After intact testing, the UCL was transected. Specimens were not tested for medial elbow joint gapping after UCL transection because medial elbow joint gapping in the intact UCL state was chosen as the comparison point for postoperative medial joint line gapping between the various forearm positions during graft tensioning. An ipsilateral flexor carpi radialis (FCR) tendon autograft was used to reconstruct the UCL following the standard docking technique (Figure 2). 17 This was performed by creating 2 converging 3.5-mm ulnar tunnels centered around the ulnar crest 6 mm from the elbow joint line followed by a single, 4.5-mm medial epicondylar tunnel at the UCL isometric insertion point with 2 docking tunnels that were created with a 2.0-mm drill bit. The FCR tendon was sized to 3.5 mm for all specimens, and a curved curette was used to enlarge the ulnar tunnels to accept the graft. The FCR tendon autograft was chosen to ensure that the same muscle tendon was used for all specimens, as the presence of a palmaris longus tendon can be variable. After passage of the graft through the ulnar tunnels, a 2-tailed graft was created by passing a set of #1 Ethibond sutures (Ethicon) through each docking tunnel. The graft was sized to the appropriate length prior to final docking to ensure maximal graft tension. At the time of graft tensioning, all specimens were placed in 45° of elbow flexion with a varus force and randomized to either full supination or full pronation. Each graft was secured by tying the docking sutures over a bone bridge along the proximal aspect of the medial epicondyle. Specimens were randomized for supination versus pronation position during tensioning and securing of the graft. Valgus testing was then repeated as outlined above for the native ligament.
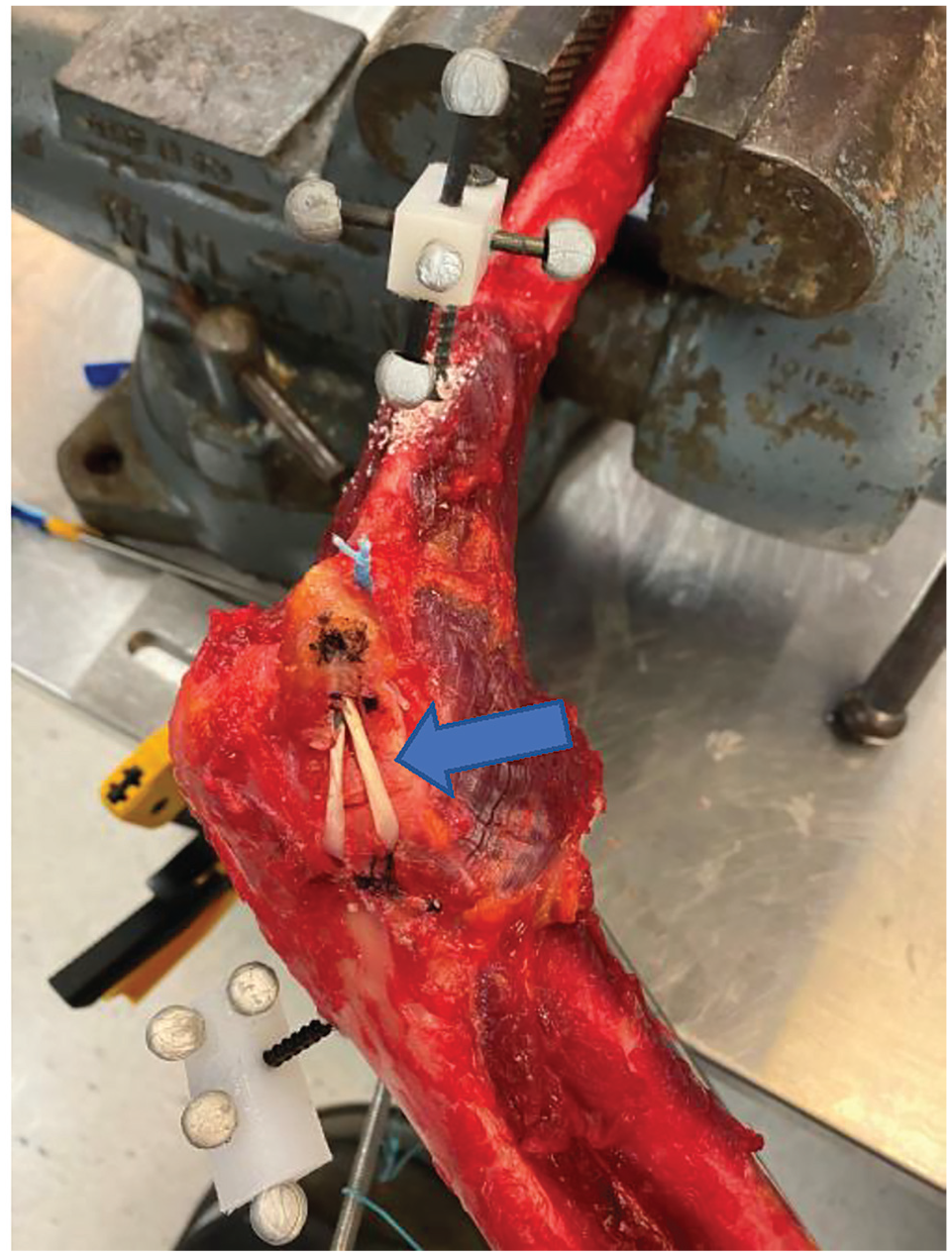
Picture of a reconstructed elbow ulnar collateral ligament using a standard docking technique, resulting in a 2-tailed graft (blue arrow).
Outcome Measures
For all intact and reconstructed testing, the order of forearm rotation and the amount of elbow flexion (30°, 60°, 90°) was randomized. All specimen configurations were first tested unloaded and then with load added. Medial joint gapping was calculated as the distance between the digitized point on the humerus and the digitized point on the ulna with load minus the distance without load for all test conditions. Change in gap was calculated as the medial joint gapping after reconstruction minus the intact, native value.
Statistical Analysis
Two-way repeated measures analysis of variance (ANOVA) was used to assess the effect of forearm position on medial gapping with the UCL intact. Groups were compared between the loaded (ie, valgus stress test) and unloaded state. Factors were position of the forearm during testing and elbow flexion angle. Additionally, 2-way repeated-measures ANOVA was also used to determine the effect of forearm position during UCLR graft tightening on the change in postoperative medial elbow joint gapping. The values of medial elbow joint gapping during valgus stress test with the native UCL were compared with the postoperative values of medial elbow joint gapping after UCLR in the various forearm positions. Forearm position during UCL graft tightening and preoperative testing were the investigated factors. Postreconstruction ANOVAs were repeated for each elbow flexion angle. Significance for all tests was set as P < .05.
Results
The forearm test position (ie, supination, pronation, or neutral) did not significantly affect the medial elbow gapping with the intact, native UCL at any degrees of elbow flexion (30°, P = .82; 60°, P = .36; 90°, P = .57) (Figure 3).

Mean medial joint gapping with an intact ulnar collateral ligament. No statistical differences were found due to forearm position or elbow joint angle (P > .05 for all comparisons).
Forearm position (ie, maximal supination or maximal pronation) at the time of UCLR graft tensioning did not result in a significant change in the medial joint gap relative to the intact state at 30°, 60°, or 90° of elbow flexion (Figure 4).
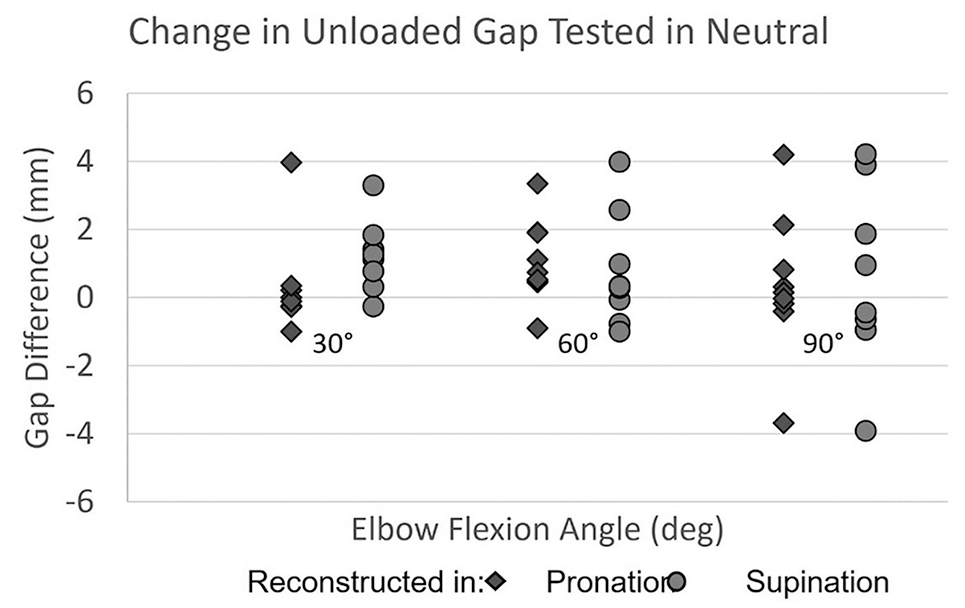
The unloaded gap after reconstruction minus that with the ulnar collateral ligament intact. No significant difference was found regardless of elbow joint angle (P > .05 for all comparisons).
Forearm position at the time of UCLR graft tensioning also did not result in a significant change in the medial joint gapping of the reconstructed UCL at 30°, 60°, or 90° of elbow flexion regardless of postoperative forearm testing position (neutral, supination, or pronation) (Figure 5).
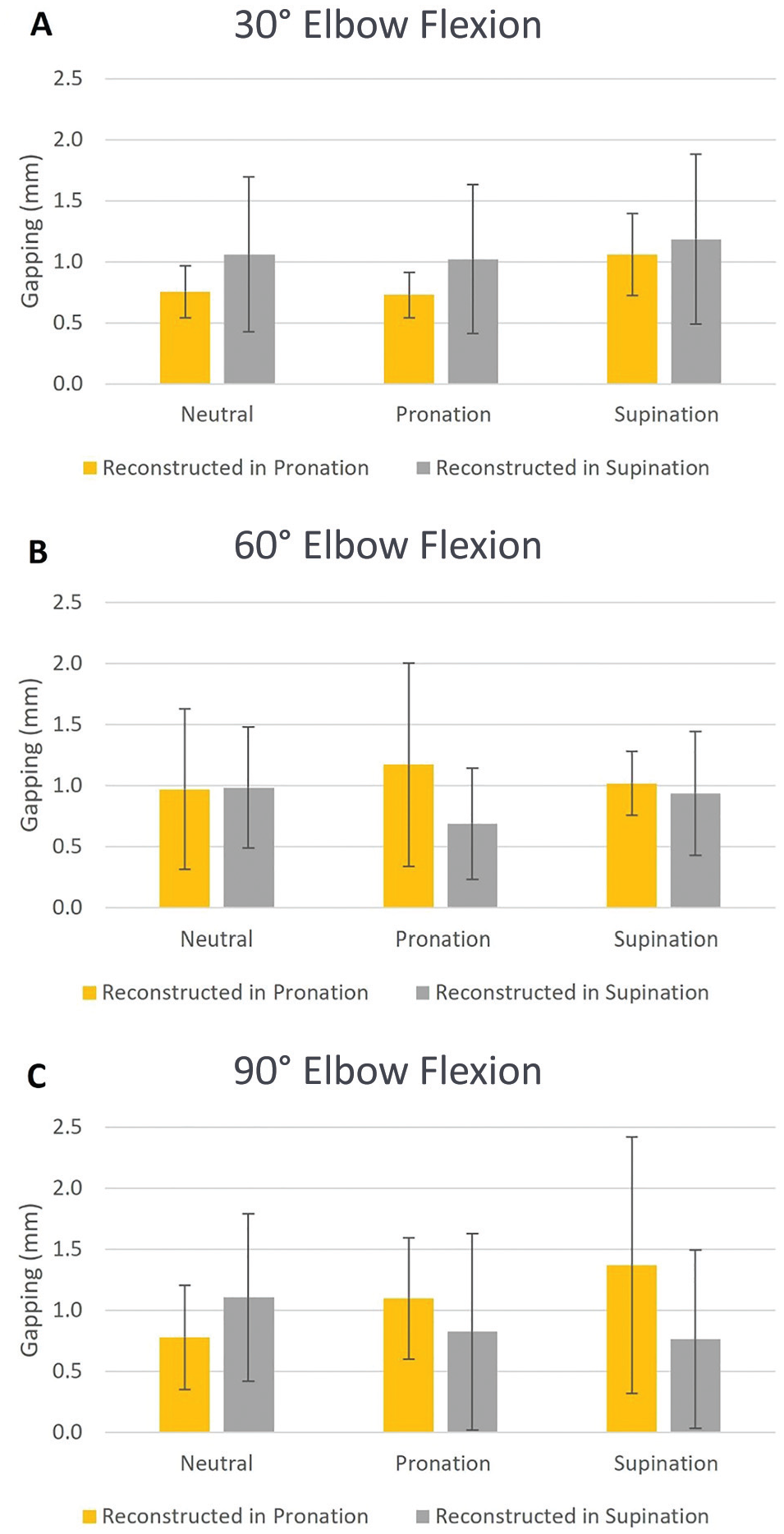
Medial joint gapping with a reconstructed ulnar collateral ligament is not significantly different regardless of forearm positioning during graft tensioning regardless of test position or elbow flexion angle (P > .05 for all comparisons).
Discussion
There were multiple important findings in the current study. First, the position of forearm rotation did not affect the amount of medial elbow joint gapping during valgus load at fixed positions of flexion with an intact, native UCL. This suggests that the native UCL is equally efficacious at maintaining reduction of the medial elbow joint regardless of forearm rotation. Second, the position of forearm rotation at the time of UCLR graft tensioning did not affect the amount of postoperative medial elbow joint gapping at various degrees of elbow flexion and forearm rotation. These findings appear to suggest that the position of forearm rotation at the time of graft tensioning during UCLR may not influence postoperative medial elbow joint reduction or subsequent medial joint gapping during valgus stress. These findings support any forearm rotation at the time of UCLR graft tensioning.
For any ligament reconstruction surgery, it is paramount to achieve an accurate joint reduction without overconstraining or underconstraining the joint. An overconstrained joint may lead to increased joint contact forces and possible stiffness with subsequent degenerative joint disease, while an underconstrained joint may lead to persistent joint laxity. In general, when a ligament reconstruction graft is secured, most surgeons prefer to place the joint in the opposite position of the forces that the ligament graft will resist in order to achieve a maximally taut graft.
The position of forearm rotation is of particular interest for sports surgeons as they examine and operate on the elbow joint. In general, elbow pronation has been demonstrated to increase both varus and valgus laxity regardless of the UCL integrity after a lateral approach to the elbow in a posterolateral instability model. 15 Laxity was further increased with the combination of forearm pronation and UCL insufficiency, suggesting that pronation further exacerbates valgus instability in the setting of UCL injury. We suggest that static valgus testing should be performed in pronation to allow for maximal exacerbation of valgus stress. These findings also advocate for placing the arm in supination during UCL graft tensioning. Similarly, Seiber et al 21 investigated the role of forearm rotation on elbow stability after sequential sectioning of elbow ligaments and muscle groups. 21 They found that the UCL had twice as much of an effect on valgus stability and that the medial musculature was most effective in providing stability in supination. The medial elbow musculature stabilized the elbow more during forearm supination even in the setting of a deficient UCL, suggesting that the musculature is an important secondary stabilizer of the medial elbow, especially with forearm supination.
While posterolateral instability is more commonly studied because of its higher frequency after elbow trauma, isolated UCL insufficiency is the most common form of ligamentous injury in overhead throwing athletes. Therefore, understanding the biomechanical effects of UCL instability and UCL surgery is paramount for restoring appropriate joint stability in these high-demand athletes. Safran et al 19 examined the effect of forearm rotation on valgus laxity with sequential UCL sectioning and found that valgus laxity was greatest with the forearm in neutral rotation. Another biomechanical study by Armstrong et al 2 demonstrated that after transection of the UCL, the elbow was more stable in supination during passive flexion but more stable in pronation during rotatory instability testing. These findings led the authors to conclude that the elbow is more stable in supination in the setting of UCL insufficiency, which appears to justify the belief that the elbow should be held in supination at the time of graft tensioning in order to achieve maximal joint reduction.
However, the findings of the current study call into question this reasoning since postoperative medial joint gapping was similar regardless of forearm rotation at the time of UCL graft tensioning. There may be a few reasons for this finding. First, it is possible that the elbow joint is minimally susceptible to large differences in joint gapping based on forearm rotation since it is a relatively small joint. Second, the presence of a varus force at the time of graft tensioning may minimize or altogether reduce the influence of forearm rotation on medial elbow joint gapping. It is also possible that an isometric and sufficiently tight UCL graft appropriately reduces the joint regardless of forearm rotation. Since the elbow joint is a relatively smaller joint, it may not be as susceptible to changes in elbow position at the time of UCL graft tensioning. Additionally, the special relationship between the distal humerus and ulna may not be particularly influenced by forearm rotation since the radius rotates around the ulna. Last, it is likely that biomechanical results in a posterolateral instability model are not directly applicable to isolated UCL insufficiency. During UCL surgery, all other elbow joint structures are presumably intact, whereas posterolateral instability often includes damage to other elbow structures in addition to the lateral UCL (LUCL) (eg, anterior capsule and possibly the UCL). Therefore, it is possible that this may also minimize any changes to medial elbow joint gapping despite forearm rotation in an isolated UCL insufficiency model.
Limitations
There are multiple limitations of the current study. While the cadaveric model allowed for consistent testing within and between specimens, it is unknown if this model accurately simulates clinical valgus stress during the pitching motion. The use of 3 N·m is below the physiologic amount of valgus torque during the act of baseball pitching, but this value has been used in other biomechanical studies.7,14 The current model necessitated stripping all muscles from the specimens, but these muscles have been shown to influence valgus stability, especially the medial flexor pronator muscles. Additionally, isometry was not able to be confirmed for the specimens. However, the insertion sites of the native UCL were readily visualized since all other soft tissues were stripped, yet it is unknown if there were isometric differences between specimens that could alter the results. Furthermore, gapping in the sectioned state was not performed. Last, a power analysis was also not performed.
Conclusion
In the current cadaveric biomechanical model, forearm rotation did not affect medial elbow joint gapping with an intact, native UCL. Additionally, securing the UCLR graft in full forearm pronation or supination did not affect postoperative medial elbow joint gapping. Further studies are needed to validate these findings and help elucidate if other surgical factors can influence postoperative medial elbow joint gapping after UCLR.
Footnotes
Final revision submitted October 21, 2024; accepted November 11, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.S.S. has received hospitality payments from Arthrex and Stryker; consulting fees from Medacta USA; education payments from Medwest Associates, Smith & Nephew, and Arthrex; and a grant from Arthrex. C.D.L. has received hospitality payments from Smith & Nephew, Vericel Corporation, and Arthrex; consulting fees from RTI Surgical; and education payments from Great Lakes Orthopedics, Arthrex, and Smith & Nephew. J.B.C. has received hospitality payments from Medtronic and Surgalign Spine Technologies, consulting fees from Surgalign Spine Technologies, and education payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Hospital for Special Surgery (No. 2016-0071).