
Abstract
Background:
Anterior cruciate ligament (ACL) injury prevention programs address quality of movement to identify and correct high-risk movement patterns. However, return-to-play decisions after ACL reconstruction (ACLR) are often based on non–sport related quantitative measures such as isokinetic tests, jump testing, and/or time from surgery, with 6 to 9 months a common expectation for progressing to sport-specific training and return to play.
Purpose:
To identify the presence in each limb of movement patterns associated with ACL injury in athletes 6 months post-ACLR using a quality-of-movement assessment.
Study Design:
Cross-sectional study; Level of evidence: 3.
Methods:
A quality-of-movement assessment including 10 dynamic tasks progressing from double- to single-limb and vertical to horizontal movements was administered to 148 athletes at 6 months after ACLR. Tasks were viewed live from the frontal and sagittal planes by a physical therapist and certified strength and conditioning specialist. Movements were evaluated for strategy, depth, alignment, symmetry, and control. The proportion of patients exhibiting faulty movement patterns for each task was assessed in the involved and uninvolved leg and between sex, meniscal injury status, and age. To examine the differences in age, patients were divided into age groups based on their age at the time of surgery (<14 years, 14-18, 19-25, 26-34, and ≥35 years).
Results:
Mean time of testing was 6.4 months after ACLR. All patients exhibited faulty movement patterns for ≥1 task on the involved leg. On the involved leg, the proportion of patients demonstrating faulty movement patterns for a task ranged from 52% to 95%. Forward stepdown (P < .001), single-leg squat (P = .03), side-to-side jump (P = .03), and hop to opposite (P = .04) demonstrated higher frequency of faulty movement patterns in the involved versus the uninvolved leg. Rates of faulty movement patterns were not different between sex or meniscal injury status. Single-leg stance on the involved leg (P = .05) and single-leg bridge (uninvolved leg) (P = .02) differed between age groups.
Conclusion:
Athletes demonstrated multiple faulty movement patterns that have been associated with both initial and second noncontact ACL injury. Faulty movement patterns were evident in tasks as simple as single-leg stance. The rates of faulty movement were similar in both male and female patients, as well as in the involved and uninvolved limb.
Anterior cruciate ligament (ACL) injuries have been identified as the single largest problem in orthopedic sports medicine. 48 ACL reconstruction (ACLR) is the standard of care for injured athletes who wish to return to their previous level of play.36,39 The incidence of ACL injury and ACLR have both been shown to increase over recent years. 50 In the United States alone, 200,000 primary ACLR are performed annually. 47 Historically, an athlete who underwent ACLR typically expected to return to play (RTP) at his/her previous level at 6 months after surgery, 4 an expectation that was consistent with the RTP time frames documented by the orthopaedic community.4,20,46 Current research, however, has shown that this time frame is not realistic.3,9,38 Several studies have highlighted the low rate of athletes who RTP and the high rate of subsequent ACL injury.3,43,44,49 In a meta-analysis, Ardern 2 reported that only 1 in 3 athletes returns to the previous level of play and 1 in 2 returns to competition. In addition, athletes who RTP after ACLR are vulnerable to sustaining a second ACL tear occurring on either their ipsilateral or their contralateral limb; second injuries have been reported in 8% to 30% of athletes who RTP at any time point after ACLR.28,30,49 Laboute and colleagues 33 reported that if an athlete returns to one's sport within the first 7 months, there is a 3-fold increase in reinjury. Furthermore, athletes evaluated for 2 years after ACLR were found to have as much as a 15 times higher risk of suffering a second injury.43,44 Nonetheless, athletes are initiating return to sport-specific activities—for example, running, jumping, and cutting drills—at 6 months postoperatively.
The rationale for ACL injury prevention programs is to address an athlete's quality of movement during sport-specific tasks for the purpose of identifying and modifying movement patterns known to put an athlete at risk for ACL injury. In contrast, RTP decisions after ACLR are often based on non–sport related quantitative measures such as isokinetic tests, clinical diagnostic tests (ie, Lachman test), single-leg (SL) hop tests, and/or time from surgery.5,20,46 The athlete is often deemed ready to return when he or she achieves an 85% to 90% limb symmetry index (LSI) with various performance measures. 1 Recent studies question the usefulness of the LSI as a tool in RTP decision making.19,34,40,56,60 Bilateral strength deficits exist after ACLR; thus, LSI may overestimate function by failing to account for the decrease in muscle strength in the uninvolved leg.51,56 Postoperative ACL rehabilitation guidelines have largely promoted early RTP by focusing on reducing pain and swelling and restoring range of motion, strength, and neuromuscular control while protecting the “new” ACL. These postoperative protocols/guidelines all indicate that based on quantitative measures such as those previously mentioned, the athlete will be ready to initiate sport-specific training by 6 months postsurgery.1,10,58 In a systematic review of factors used to determine readiness to return to unrestricted activity after ACLR, 4 time from surgery was used as an RTP criterion in 60% of the 264 studies, 40% failed to report any criteria, and only 13% included any measurable objective criteria that an athlete had to achieve before clearance to RTP. In a survey of 271 experienced surgeons, 46 RTP criteria included a variety of clinical measures (81% Lachman test, 60% pivot-shift test, 45% anterior drawer test, 78% knee range of motion, 15% instrumented anterior laxity measurement, 3% magnetic resonance imaging) and quantitative measures such as SL hop tests and measures of strength and proprioception. The importance of adding quality of movement to the RTP decision-making process has only recently surfaced,16,37,57 and recent systematic reviews and consensus statements advocate the inclusion of measures of strength, hop tests, and video analysis of quality of movement.16,17,55
Although the exact mechanism of noncontact ACL injury is not well-understood, it appears to be the result of a combined loading pattern of reduced hip and knee flexion angles, 26 increased knee valgus 26 and internal rotation of the femur on the tibia, and high quadriceps activity unbalanced by the hamstrings.6,27,29,31,35,59 Paterno and colleagues 45 identified specific movement patterns that were highly predictive risk factors for incurring a second ACL injury in athletes returning to full activity. In their study, they found that the risk of second injury was increased 2-fold in athletes who demonstrated deficits in postural stability on the involved limb, 3-fold in those who demonstrated a side-to-side difference in sagittal plane knee moment at initial contact or greater frontal plane knee motion during landing, and 8-fold in those demonstrating decreased hip external rotator moment during the initial 10% of landing. 45 These movement patterns are consistent with those known to predict primary ACL injury, yet are rarely used to inform the RTP decision-making process.
Considering the documented high risk of sustaining a second injury when returning to play after ACLR, we developed a quality of movement assessment (QMA) to identify the presence of such risky movement patterns in athletes after ACLR and demonstrated the reliability of the QMA. The purpose of this study was to identify the presence of movement patterns in both the involved and the uninvolved limbs associated with ACL injury in athletes 6 months after ACLR using the QMA.
Methods
Participants
A clinical database was searched to identify patients who had a QMA at the outpatient sports rehabilitation center of our institution between January 2013 and September 2014 using a retrospective cross-sectional study design. Patients who had a QMA performed 5 to 7 months after ACLR were included in the study. Only the first eligible QMA was included in the analysis for patients with multiple assessments during this time frame (Figure 1). All patients had undergone ACLR at our institution, a hospital specializing in the treatment of orthopaedic and rheumatological conditions, and were referred for a QMA by the patient's surgeon. The patients came to our institution for surgery from a wide geographical area and received rehabilitation from a local provider. There were 235 patients who had a primary ACLR, without revision or multiligament injury. Of those, 80 patients were excluded because their first QMA was performed outside the inclusion time frame (mean ± SD, 6 ± 1 months from surgery), and 7 were excluded because the timing of their QMA was unknown. A total of 148 participants were eligible for inclusion into our study. Approval from our institutional review board was obtained before study commencement.

Flow diagram for study population. ACLR, anterior cruciate ligament reconstruction; DOS, date of service; M, months; QMA, quality of movement assessment.
Procedures
The QMA included up to 10 tasks, which progressed from double- to single-limb, static to dynamic, and vertical to horizontal tasks. Not all patients performed all 10 tasks; the examiners were allowed to end the assessment at any point if the patient was unable to perform a given task or the examiner felt it was not safe to perform the task.
Tasks ranged from double-leg movements such as squats and jumps to similar movements on a single leg. Both a physical therapist and a certified strength and conditioning specialist guided the patient through the task sequence and observed each task in the frontal and sagittal planes. The assessment evaluated movement strategy, depth, alignment, symmetry, and control. The presence or absence of pain was noted for all movements (Table 1).
Quality of Movement Assessment Tasks

Performance was recorded as optimal or faulty on a checklist for each task and each limb. Faulty movement strategy referred to the athlete's initiating the movement with the knees first and/or continuing to drive the movement with the knee, or where the knees flexed beyond the toes (Figure 2). Depth of movement was rated as faulty if the athlete demonstrated limited knee and hip flexion angles during tasks as indicated by not achieving thighs parallel to floor for the double-leg squat or 60° of knee flexion for jumping and SL tasks. Alignment was rated as faulty if the patient was not able to maintain the trunk, hip, knee, and foot in a single line and level hips in the frontal plane and/or if the trunk and shins were not parallel in the sagittal plane during the task. Asymmetry, described as a shift biased toward either lower extremity, was assessed during double-limb movements. Control was defined as the athlete's ability to maintain one's center of mass within the base of support without being wobbly at any joint during SL tasks and was first assessed during the SL stance. Thus, lack of control referred to the individual's inability to control the rate or direction of movement. The inability to demonstrate smooth, coordinated kinetic linking in a task or to sustain a static position in good alignment for the requisite period of time also indicated lack of control.

Hip versus knee strategy for performing a squat.
Athletes were asked about pain when performing each movement, as pain would influence their movement patterns. If the athlete reported pain or if the examiner determined that an athlete should not perform a movement due to exhibiting faulty movements on a previously less demanding task, then the assessment was abbreviated. The examiner then rated each task as “faulty” or “optimal” based on the evaluation of movement characteristics as described above and patient-reported pain with the task. Several examples of faulty movement are depicted in Table 2.
Examples of Faulty Movement

Statistical Analysis
Study data were collected via paper forms and later transferred to the Research Electronic Data Capture (REDCap) electronic data capture tool.24,25 Descriptive statistics of the study population included reporting of means and standard deviations for continuous variables and frequencies and percentages for discrete variables. Chi-square tests were used to evaluate any potential differences in performance of each exercise between involved and uninvolved legs (Chi-square tests were used to assess differences in exercise performance between involved and uninvolved limbs; Fisher's exact test was used when assumptions for the chi-square test were not met). Additional analyses included comparison of faulty movement between patient sex, meniscal injury status, and age within the involved and uninvolved leg. To examine the differences in age, patients were divided into age groups based on their age at the time of surgery (<14, 14-18, 19-25, 26-34, and ≥35 years). All analyses were performed using SAS Version 9.3 (SAS Inc) with statistical significance defined as P < .05.
Results
From January 2013 to September 2014, a total of 148 patients who had undergone primary ACLR were evaluated using the QMA. All patients had their ACLR between May 2012 and March 2014 and were 5 to 7 months postsurgery. The mean ± SD age of the study population was 19.3 ± 8.3 years (range, 9.5-53.1 years). Females comprised 55% of the study population, while injury side was evenly distributed between left (50%) and right (50%) sides. Concomitant meniscal injury was found in 59 patients (42%). All participants completed ≥5 of the QMA tasks. As tasks were not completed if the patient was unable to perform the task or the examiner felt it was not safe for the patient to perform the task, only 29% of patients completed all 10 tasks. Full description of patient characteristics and task completion rates can be found in Table 3.
Demographic and Clinical Characteristics of Study Population (N = 148) a

Data are shown as Mean ± SD or N (%). ACLR, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone; N, number; QMA, quality of movement assessment; SD, standard deviation.
Overall Performance Between Involved and Uninvolved Leg
Patient performance on the QMA was different between the involved and uninvolved leg depending on the task (Figure 3). The proportion of patients demonstrating faulty movement patterns for a task on the involved leg (among the tasks completed) ranged from 52% to 95%, with a mean of 83% among tasks. The proportion of patients with faulty movement patterns on the uninvolved side ranged from 45% to 92%, with an overall mean of 76%. A significantly higher proportion of faulty tasks was observed in forward stepdown (P < .001), SL squat (P = .03), side-to-side jump (P = .03), and hop to opposite (P = .04) on the involved as compared with the uninvolved legs.
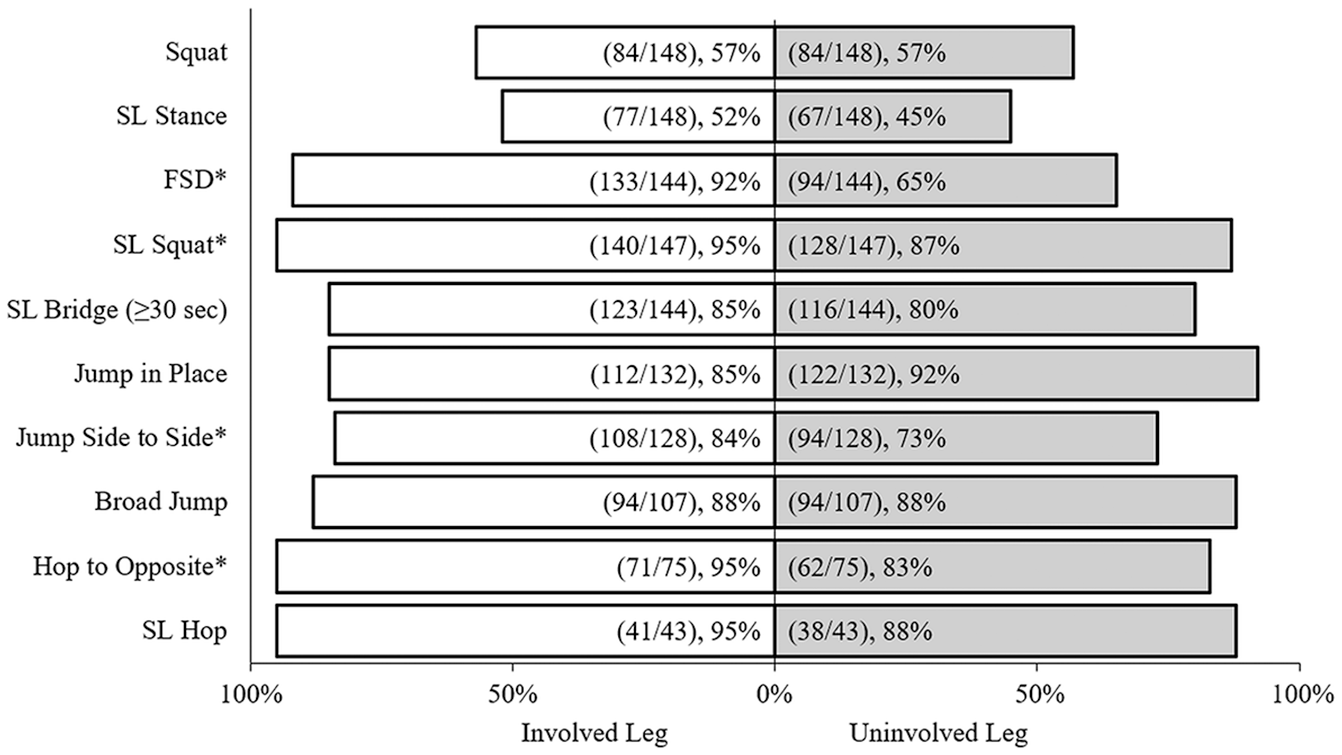
Percentage of faulty movement in all completed tasks, involved versus uninvolved leg. *Indicates statistically significant difference between involved and uninvolved leg (P≤ .05). FSD, forward stepdown; SL, single leg.
Faulty Movement Between Sex, Meniscal Injury, and Age Group
No statistical differences in performance were found between male and female patients on either the involved or the uninvolved leg (Figure 4). Similarly, no performance differences were found between patients with and without meniscal injury on either leg (Figure 5). No differences were found among age groups on either side for most tasks (Table 4). However, in the involved leg, there was a significant difference overall in SL stance among age groups (P = .05). Post hoc comparisons found that percentage of faulty movements in patients aged 19 to 25 years (22%) was lowest among all age groups and significantly lower compared with patients aged 14 to 18 years (55%; P = .02), 26-34 (60%; P = .046), and ≥35 years (75%; P = .008) for the SL stance on the involved leg. On the uninvolved leg, there was a significant difference overall in SL bridge (P = .02). During the SL bridge, patients ≥35 years (50%) had significantly lower faulty movements compared with all other age groups (<14: 91%, P = .01; 14-18: 80%, P = .02; and 26-34: 100%, P = .02).
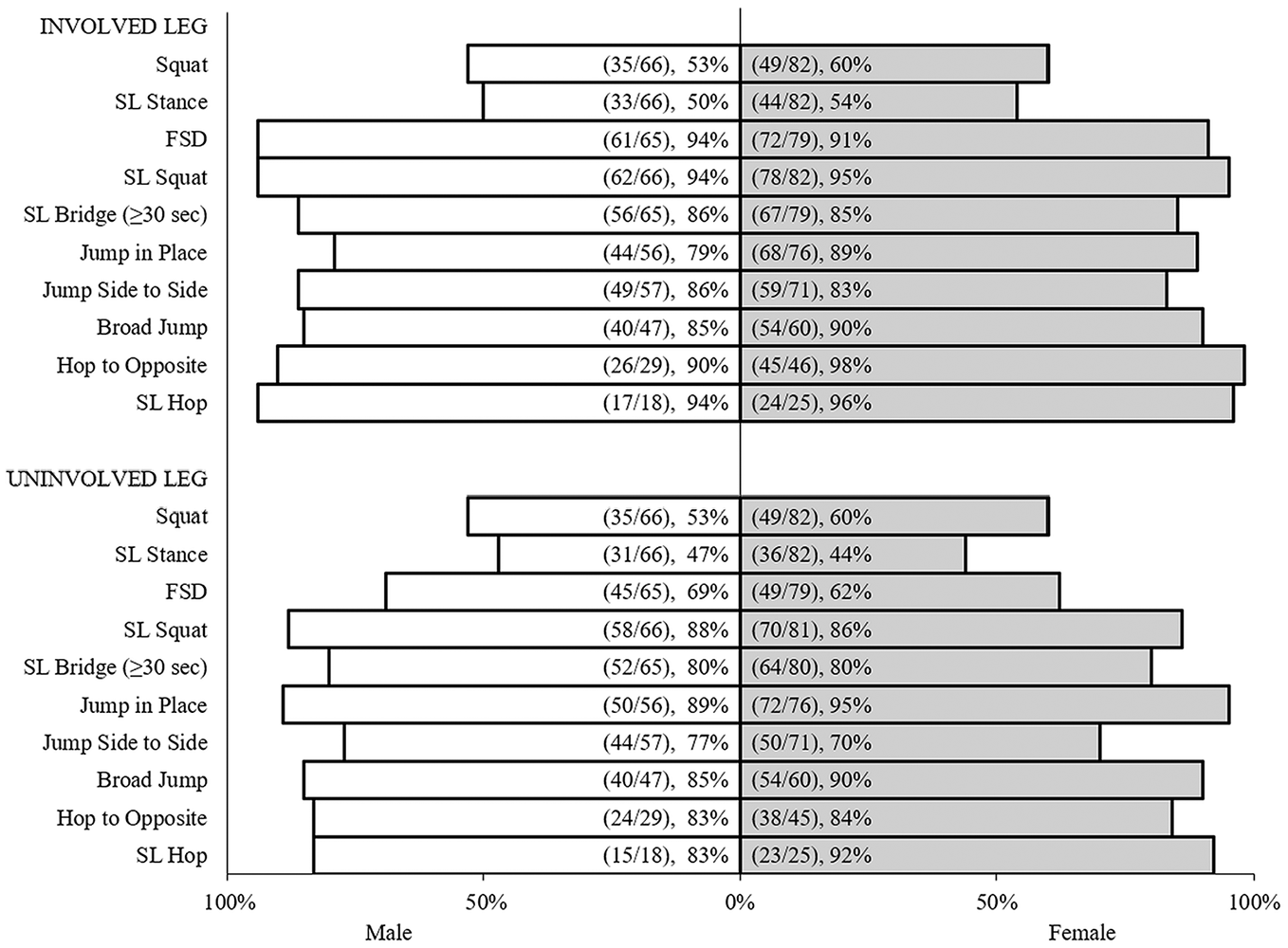
Percentage of faulty movement by sex in the involved and uninvolved leg. FSD, forward stepdown; SL, single leg.
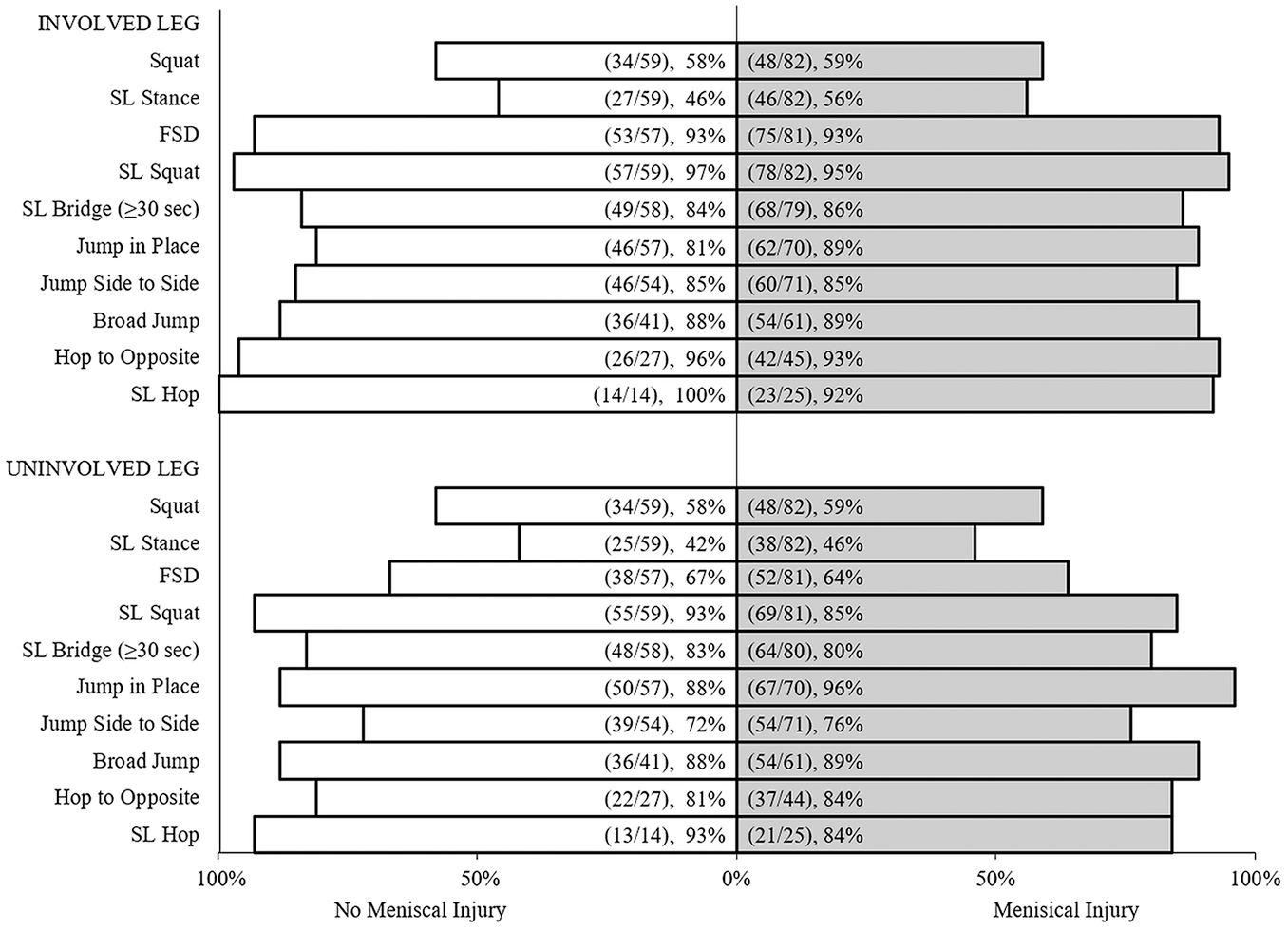
Percentage of faulty movement by meniscal pathology in the involved and uninvolved leg. FSD, forward stepdown; SL, single leg.
Frequency of Faulty Movement in Involved and Uninvolved Leg by Age Group a

Data are presented as (n/N) %, where n is the number of patients exhibiting a faulty movement pattern, N is the number of patients in that age group that performed the movement, and % represents the corresponding percentage.
Discussion
Our results, after reviewing the QMA in athletes after ACLR, indicate that deficits in quality of movement are present 6 months postoperatively, a time when many athletes are progressing to sport-specific training and planning their RTP. Depending on the task, 52% to 95% of patients demonstrated faulty movement on the involved side; patients were only slightly better on the uninvolved side with 45% to 92% demonstrating faulty movement. As many of the faulty movement patterns identified during QMA testing are the same movement patterns known to put the athlete at risk for both primary and second ACL tears,26,27,45 the high prevalence of faulty movement on both sides suggests high risk for reinjury for the involved side and future injury on the uninvolved side. It is possible that these deficits might not be identified on conventional quantitative measures used in standard RTP decision making.
Time from surgery, restoration of joint range of motion, and a negative Lachman test are the most commonly cited criteria by surgeons when determining readiness to RTP.4,46 Other commonly cited criteria are quantitative measures such as isokinetic testing or hop tests for distance. While these quantitative measures are valuable tools in the RTP decision-making process, their purpose is not to identify movement patterns that have been associated with increased risk of both primary and second ACL injury. In the systematic review of measurement procedures after ACLR, Engelen-van Melick and colleagues 16 concluded that qualitative measures, in addition to the assortment of quantitative measures available, would complete the picture when determining readiness for unrestricted activity after ACLR. This conclusion has been supported by others,14,17,22,23,53,55,57 encouraging clinicians to implement functional testing before allowing athletes to RTP.
The evidence suggests that it takes longer than 6 months to restore neuromuscular control and correct faulty movement patterns after ACLR. Sensory and motor deficits in ACL-reconstructed knees have been reported to persist for 12 to 30 months postoperatively while altered joint kinematics have been documented to persist for 12 months.8,13,18,42,52 These deficits may contribute to movement patterns that have been associated with an increased risk of ACL injury. It is also possible that these deficits may amplify preexisting faulty movement patterns that contributed to the primary ACL injury. Since our cohort represented athletes who had already been injured, the prevalence of faulty movement patterns is not surprising. While the greatest percentage of faulty movements were noted in single-limb movements, faulty movement patterns were also highly prevalent in double-limb movements. Nagelli and Hewett 41 have called for young athletes to delay their return to competitive sport until 2 years after ACLR. This recommendation was based on findings from their review that the risk of reinjury is highest within the first 2 years and that knee health recovers to baseline levels only after that time. There is a growing consensus that a more robust battery of measures combined with a more gradual RTP is warranted in light of the high rate of reinjury and relatively low rate of successful RTP.3,15,20,23,53,55
The equal presence of faulty movement patterns in the involved and uninvolved limb supports the possibility that these movement patterns contribute to the initial injury and remain a risk factor for subsequent injury. The only movement patterns in which the involved limb demonstrated significantly more at-risk movement patterns were the forward stepdown, the SL squat, the side-to-side jump, and hop to opposite. The forward stepdown requires specific eccentric quadriceps control, and the disparity between involved and uninvolved may reflect the relative deficit in quadriceps strength that persists at 6 months postsurgery. The forward stepdown and SL squat require the ability to decelerate over a planted leg. The side-to-side jump begins to assess deceleration in a more dynamic, yet controlled environment. Hop to opposite progresses this challenge to control deceleration and shear forces upon landing. Since ACL injuries are predominantly noncontact in origin and occur during deceleration (landing from a jump or cutting),7,12,32 the inability to maintain optimal alignment during relatively simple deceleration tasks is a significant concern when considering readiness to RTP. The similarity in faulty movement patterns seen in the involved versus uninvolved limbs should also bring into question the use of the LSI in RTP decision making. Using the uninvolved limb as the standard for comparison may not be appropriate if this limb is demonstrating movement patterns associated with risk of ACL injury,34,56 and the presence of faulty movement patterns in the uninvolved limb speaks to the high rate of contralateral ACL injury after returning to sport. Asymmetry is the most common deficit noted during double-legged tasks, whereby loss of alignment is the most common during SL tasks. When asymmetrical, the athlete shifts more weight onto the uninvolved limb yet displays faulty movement patterns on that limb as well. Webster and Hewett 54 have also cited this pattern as a possible explanation for the increased risk in contralateral injury. These findings were present whether or not patients had meniscal pathology and across a range of age groups.
Strengths and Limitations
A strength of this study was the wide variety of surgeons, surgical protocols, and rehabilitation protocols received from a wide geographical area. Despite the heterogeneous sample, the results were uniform in the striking prevalence of faulty movement patterns displayed in common sport-specific movements regardless of sex, age, or concomitant injury. Our previously published study 21 utilizing the QMA in skeletally immature athletes (10-15 years of age) also showed that faulty movement patterns existed in a younger population. In particular, no skeletally immature athlete could perform a 2-legged squat without some degree of compensation at 6 months. 38
A limitation of the study is the lack of inclusion of an uninjured group and validation of observed deficits against the gold standard of 3-dimensional motion capture. However, the criteria by which movements were deemed faulty have been validated in another study. 11 These movement patterns are commonly used to identify “at risk” athletes in primary ACL injury prevention programs. While this is a retrospective analysis of previously collected data from 2013 to 2014, these data form the basis of a larger ongoing study. Clinically, we continue to see a higher proportion of faulty movement patterns in athletes after ACLR. In addition, the QMA was conducted based on a referral from the patient's surgeon; this may limit the potential generalizability to all patients after ACLR. Future research will focus on establishing the internal and external validity of the QMA, determining whether qualitative measures are predictive of an athlete's successful return to preinjury levels of play, and ascertaining whether correlations exist between quantitative and qualitative measures.
Another limitation is the lack of control of the rehabilitation protocol these patients received at clinics close to their homes. As patients came to our institution from a wide geographical area, we did not provide all the rehabilitation at our institution. That said, the high prevalence of faulty movement patterns regardless of rehabilitation protocol is notable. Future studies would be useful to identify which, if any, rehabilitation protocols lead to better movement quality.
Conclusion
The results of this study demonstrated that bilateral faulty movement patterns exist in ACLR athletes 5 to 7 months after surgery. A shift in the mindset of the orthopaedic community is warranted to modify rehabilitation guidelines toward the incorporation of a QMA, correction of potentially risky movement patterns, and modification of suggested timing of full RTP to provide athletes, parents, and coaches with realistic expectations of readiness for RTP.
Footnotes
Acknowledgements
The authors thank Liz Selvaggio for her help with data entry, Huong Do for her assistance with data analysis, and Gwen Weinstock-Zlotnick for her patience, guidance, and support in this project.
Final revision submitted September 23, 2024; accepted November 25, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: With grant support provided to his institution, Mr. Nguyen was supported in part by funds from the Clinical Translational Science Center (CTSC), National Center for Advancing Translational Sciences (NCATS) grant #UL1-RR024996. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding source NCATS based in Rockville, MD. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approved granted by Hospital for Special Surgery (2015-287 and 14029).