
Abstract
Background:
Transphyseal techniques are the most commonly used for anterior cruciate ligament (ACL) reconstruction in children. To mitigate the risk of growth disturbance, the tunnels should be positioned as vertically and centrally as possible in relation to the physis, potentially compromising the anatomic orientation of the graft and, therefore, its isometry. A graft rupture is frequent in this age group. Even though all-epiphyseal techniques have not clearly demonstrated better isometry, the authors propose an epiphyseal technique that aims for favorable anatomy, and therefore isometry, while avoiding physeal damage in young children with ACL ruptures.
Purpose:
To present the results of a modified all-epiphyseal technique in prepubertal patients, evaluating knee function, graft survival, and joint and growth protection.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 74 skeletally immature patients with a traumatic ACL rupture underwent a physeal preserving technique using a semitendinosus-gracilis tendon graft fixed with intra-epiphyseal resorbable interference screws in the femur and tibia, along with associated minimal notchplasty. Preoperative, intraoperative, and postoperative assessments included clinical knee stability and meniscal status, magnetic resonance imaging, isometry measurements, comparative laximetry measurements with stress radiography using the Lerat method, full-length standing radiography, measurements of the axes of the lower limbs, Tegner and Lysholm scores, and patient satisfaction.
Results:
From 2004 to 2014, a total of 74 patients met our inclusion criteria and were followed up for a mean of 4.1 years (range, 2-7 years). Of these patients, 91.9% had an excellent/good postoperative Lysholm score, with similar preoperative and postoperative Tegner activity scores. Intraoperative isometry showed an intratunnel graft excursion <3 mm during extension in 95.9% of cases. Abnormal clinical laxity was observed in 4.1% at final follow-up, with an improvement in side-to-side laxity of 4.8 mm. There were 3 patients who experienced graft failure, with the salvage procedure employing a transphyseal technique in 1 patient. Meniscal tears occurred in 27.0%, with concomitant repair yielding a healing rate of 87.5%. No physeal alterations were observed, except for a tendency toward subtle overgrowth in the affected limb. Also, 90.5% of patients were satisfied or very satisfied with the outcome.
Conclusion:
The proposed all-epiphyseal technique in skeletally immature patients demonstrated excellent overall results with a low incidence of reruptures and meniscal degeneration, without relevant alterations related to growth.
Greater participation of children in competitive sports has led to an increase in acute anterior cruciate ligament (ACL) injuries, now comprising 2% to 5% of all ACL ruptures, although they remain rare in children <9 years.3,73 The nonoperative management of an ACL tear in a child is not recommended in cases of knee instability, meniscal or chondral injuries, or high physical activity levels because of functional impairments and a high risk of premature joint degeneration. Consequently, there has been a growing trend toward surgical interventions, as ACL reconstruction improves knee function and reduces the risk of intra-articular injuries.**
High rerupture rates in pediatric ACL reconstruction are concerning, but data on this issue are limited and heterogeneous compared with adults.20,38,79 Transphyseal techniques are commonly used, even in prepubertal patients, 2 but drilling tunnels through the physis poses the risk of growth disturbance. †† Smaller tunnel diameters and more vertically oriented tunnels are employed to reduce the physeal injury risk, although this may alter the graft’s anatomy.5,17,34,42
The objective of this study was to describe an all-epiphyseal surgical technique in prepubertal patients using a semitendinosus-gracilis tendon graft and intra-epiphyseal resorbable interference screw (RIS) fixation. Knee function, graft survival, and joint and growth protection after surgery were evaluated. Our hypothesis was that this intra-epiphyseal technique would provide favorable anatomy-isometry, which, when combined with minimal notchplasty, would protect the graft, resulting in favorable outcomes with a low risk of physeal damage.
Methods
Patients provided informed consent in accordance with the Declaration of Helsinki guidelines for biomedical research involving human participants. Institutional review board approval was obtained.
A prospective cohort study was conducted between 2004 and 2014 on 160 children and adolescents undergoing pediatric ACL reconstruction for an ACL rupture. Exclusion criteria included tibial eminence avulsions and the use of a different technique from the one described herein. Overall, 60 patients were excluded: 14 for tibial eminence fractures and 46 for undergoing alternative surgical techniques, including the Clocheville, transphyseal, all-inside, and extra-articular techniques.
Inclusion criteria included patients with an ACL rupture using the all-epiphyseal technique described herein, a maximum bone age of 13.5 years in boys and 11.5 years in girls using left-hand radiography, 31 a maximum maturity rating of Tanner stage 3, 76 a partial or complete ACL rupture (confirmed via magnetic resonance imaging [MRI]) with abnormal clinical laxity (anterior drawer or Lachman grade 3 and/or soft endpoint and/or pivot shift 70 ) and/or a concomitant meniscal and/or chondral injury, and a minimum follow-up of 2 years with completed growth. Of the remaining 100 patients, 26 did not meet the inclusion criteria because of insufficient follow-up or loss of follow-up or not reaching skeletal maturity, leaving 74 patients for analysis (Figure 1).

Flowchart showing the initial number of patients considered and the final number after applying inclusion and exclusion criteria. F, female; FU, follow-up; M, male.
Clinical variables recorded preoperatively and at the end of follow-up included laxity graded on 4 levels: 0 (normal), no difference on the Lachman or pivot-shift test; 1 (optimal), anterior drawer or Lachman grade 1 with a hard endpoint; 2 (suboptimal), anterior drawer or Lachman grade 2 with a hard endpoint; and 3 (abnormal), anterior drawer or Lachman grade 3 with a soft endpoint or pivot shift. The assessment of meniscal status included the Apley and Steinman II tests. 30
Radiological variables recorded preoperatively and at the end of follow-up included MRI findings of the affected knee; the difference in lower limb length by full-length standing radiography; and measurements of the tibiofemoral axes such as the lateral distal femoral angle, medial proximal tibial angle, sagittal distal femoral angle (sagittal femoral axis to Blumensaat line), and tibial slope. 80 Additionally, comparative laximetry measurements were performed using the Lerat method, 49 calculating differential anterior translation in the medial compartment of the knee using dynamic radiography during the anterior drawer test, with a load on the thigh proportional to the child’s weight. Normal values range from 2 to 5 mm.
Functional testing included the Tegner activity score both before the injury and at the end of follow-up as well as the Lysholm score preoperatively and at the end of follow-up.52,77 The patient’s final satisfaction was assessed using a 4-point ordinal Likert scale (0, very dissatisfied; 1, dissatisfied; 2, satisfied; and 3, very satisfied).
Surgical Technique
The technique that we employed is a modification of Anderson’s 6 arthroscopic method using a folded autologous semitendinosus-gracilis tendon graft to create a 4-strand hamstring tendon autograft. Traction loops were tied at both ends of the tendons, and a traction thread was used at the fold for ascending the graft. The folded portion of the graft was secured in the femoral epiphyseal tunnel using an RIS (FH Orthopedics). Another RIS was used to fix the ends at the tibial epiphyseal tunnel. Positioning was done with thigh support and an image amplifier to provide a precise profile of the knee (Figure 2).

Patient positioning.
An arthroscopic examination was performed through standard anteromedial working and anterolateral viewing portals. The diagnosis of an ACL tear was confirmed. The residual ACL was removed, and any excess soft tissue in the tibial and femoral footprints was cleared. Minimal notchplasty (2 mm) was performed, limited to the medial border of the lateral condyle to avoid damage to the physis. Any unstable meniscal lesions found were repaired. Femoral and tibial tunneling was performed transepiphyseally from outside to inside as follows: The sharp-ended femoral ACL guide was placed at the intra-articular femoral point, located fluoroscopically midway between the Blumensaat line and the posterior border of the lateral condyle, as close as possible to the physis but ensuring a minimum 2-mm distance between the physis and the upper edge of the tunnel. Drilling of the tunnel was guided by a wire inserted through the ACL guide from the lateral epicondyle to the intra-articular point, ensuring that the wire remained at a safe distance from the physis. The sharp-ended tibial ACL guide was positioned anterior to the posterior cruciate ligament, and the wire was directed obliquely at about 40° from medial to the anterior tibial tuberosity to the tibial footprint of the ACL on the tibial plateau. Tunneling was performed under profile image control, maintaining a minimum distance of 2 mm between the lower tunnel edge and the physis while preserving as much of the tibial bony roof as possible (Figure 3).

(A) Placement of the intra-articular femoral anterior cruciate ligament (ACL) guide in strict profile view (with the posterior borders of both condyles overlapping). (B) Out-in positioning of the femoral guide wire before tunneling. (C) Placement of the intra-articular tibial ACL guide and the tibial guide wire before drilling.
Using intratunnel visualization, we ensured the preservation of the growth plate, and then, the graft was ascended from distal (tibial tunnel) to proximal (femoral tunnel) (Figure 4). Fixation was performed as follows (Figures 5 and 6): Initially, the graft was fixed to the femur with an RIS positioned on the tunnel’s wall far from the physis, compressing the graft against the bone adjacent to the physis, so that the graft is positioned between the physis and the screw. Isometry was assessed by determining how many millimeters the graft moved into the tibial tunnel during extension, indicating that it would elongate intra-articularly. 41 If this excursion measured <3 mm, the graft was fixed in the tibial tunnel by another RIS in a neutral knee position; if it measured ≥3 mm, the graft was considered to have unfavorable isometry and was fixed in a near-extension position to prevent graft tension stress during extension. Any potential conflict with the notch was evaluated, and notchplasty was extended if necessary. The redundant distal graft was sutured to the sartorius fascia.

(A) Intratunnel verification of growth plate integrity. (B) Ascent of the graft. (C) Final result after fixation.

Magnetic resonance imaging showing correct positioning of the resorbable interference screw (RIS). (A) Tibial epiphyseal positioning midway between the physis and the articular surface. (B) Femoral epiphyseal positioning near the distal femoral physis.

Radiography at 1 year after intra-epiphyseal anterior cruciate ligament (ACL) reconstruction in an 11-year-old boy, illustrating tunnel orientation and positioning of the resorbable interference screw (RIS).
Statistical Analysis
For descriptive analysis, continuous variables were summarized as means with standard deviations and medians, while categorical variables were presented as absolute numbers with percentages. Univariate analysis was conducted to explore associations between variables and functional and satisfaction scores. Inferential comparisons of quantitative variables were carried out using the Student t test for unpaired data with normal distributions and the Mann-Whitney U test for variables that did not follow a normal distribution. All statistical analyses were performed using the statistical software package SPSS (Version 24; IBM).
Results
Patient Characteristics
All 74 patients eligible for analysis underwent surgery within 6 months after the trauma. Baseline patient characteristics are summarized in Table 1. The mean duration of follow-up was 4.1 years (range, 2-7 years). All patients had an ACL rupture confirmed during arthroscopic surgery, with 9 cases (12.2%) being partial ruptures, of which the fibers were preserved in 5 cases. Compared with the group with complete ACL ruptures, there were no differences in quantitative or categorical variables.
Baseline Characteristics of Patients (n = 74) a

ACL, anterior cruciate ligament.
Intraoperative Findings
Intraoperative results are summarized in Table 2. Of the 20 meniscal tears (27.0%) found during arthroscopic surgery, 14 (70.0%) involved the lateral meniscus. Of these 20 meniscal tears, 16 (80.0%) were repaired, among which 2 cases (12.5%) failed over the course of follow-up. Additionally, there were 4 new meniscal tears (5.4%; 3 lateral/1 medial). All 6 of these latter tears were repaired during follow-up. No meniscectomy was undertaken.
Intraoperative Findings (n = 74)

Minimal notchplasty (2 mm) was performed in 67 patients (90.5%), with 7 cases (9.5%) requiring an increase to ≥3 mm. The mean diameter of the bone tunnels was 7.3 mm (range, 6-9 mm) for both the femur and tibia. Isometry revealed a mean graft excursion of 1.1 mm (range, 1-4 mm), with 3 cases (4.1%) having a value ≥3 mm. In 1 case, there was a femoral physis injury during tunneling, but no growth disturbance occurred afterward (Figure 7). There were 7 cases (9.5%) with a screw-related incident: 3 femoral and 1 tibial screw breakage and 3 unstable tibial fixation. Of the 3 cases of unstable tibial fixation, 2 were treated intraoperatively with additional fixation using tibial metaphyseal stapling. The graft survival rate was 95.9% (Figure 8), with 3 cases of failure observed.

Epiphyseal-side injury of the distal femoral physis after tunneling. The patient exhibited no clinical consequences.

(A) Complete anterior cruciate ligament (ACL) rupture in a 12-year-old boy. (B) Adequate maturation and anatomic orientation of the graft at 2-year follow-up.
Clinical Outcomes
Table 3 summarizes the preoperative and postoperative clinical and functional results. The mean side-to-side laxity (with the Lerat method) improved from a mean of 7.6 mm (range, 6 to 12 mm) preoperatively to 2.8 mm (range, −6 to 10 mm) at follow-up, with 4 cases (5.4%) having a final laxity ≥6 mm (including the 3 cases of failure). Comparative clinical laxity was deemed symmetrical in 41 patients (55.4%), with type 2 (suboptimal) laxity observed in 6 cases (8.1%) and residual type 3 (abnormal) laxity noted in 3 cases (4.1%) (all failures).
Clinical and Functional Outcomes a

Data are presented as mean ± SD or n (%).
Among the 74 patients, 68 (91.9%) had an excellent/good postoperative Lysholm score, while 2 were rated as fair and 4 as poor. This score improved from a mean of 60.9 (range, 31-85) preoperatively to 94.5 (range, 43-100) at follow-up. The mean Tegner activity score after surgery was 5.4 (range, 2-10), similar to that found before the trauma. The mean time to return to sports was 8 months (range, 6-11 months). No clinical differences were observed regarding patient sex. Of the 74 patients, 67 (90.5%) reported being satisfied or very satisfied with the outcome (Table 4). Considering the 7 cases of dissatisfaction as poor outcomes (including the 3 cases of graft failure, 1 case of septic arthritis, 1 case of screw breakage, and 2 cases with meniscal-related issues), we concluded that the success rate was 90.5%.
Patient Satisfaction (n = 74)

Radiological Outcomes
Radiological results comparing the operated and contralateral limbs are summarized in Table 5. No axial deviation was observed in either the coronal or sagittal plane compared with the contralateral limb (Figure 9). No patient showed clinical or radiological signs of a physeal injury. A mean overgrowth in the operated limb of 6.5 mm (range, −2 to 18 mm) was observed, with 9 cases (12.2%) having >10 mm, none of which required treatment. No radiological differences were observed regarding patient sex.
Radiological Outcomes a

Data are presented as mean ± SD.
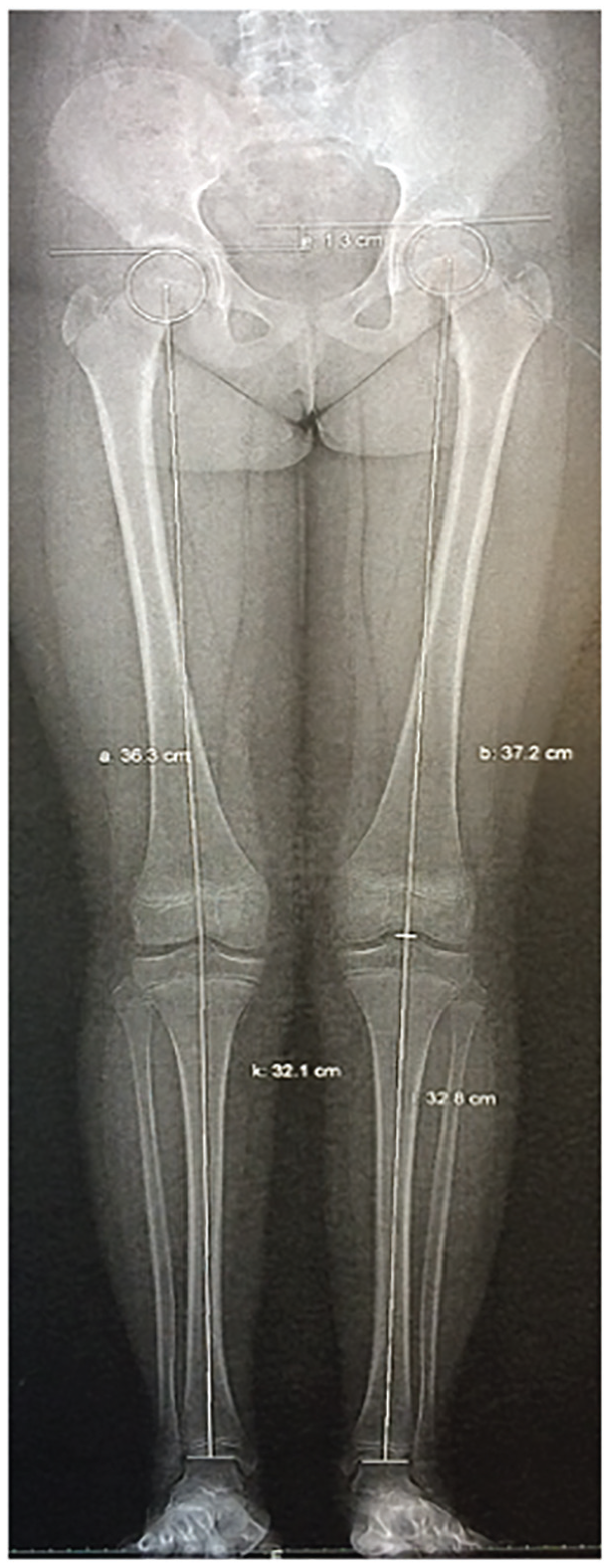
Symmetrical bone axes at 2 years after anterior cruciate ligament (ACL) reconstruction, with a 1.3-cm limb length discrepancy attributed to lengthening of the repaired limb (femur and tibia).
Complications
There were 17 cases (23.0%) with intraoperative or follow-up complications. A total of 3 graft failures (4.1%) were recorded. Among them, 2 underwent arthroscopic procedures. In one case, the graft appeared loosened with anterior impingement, which was treated by arthroscopic release and a failed attempt of retensioning using radiofrequency. In the other case, the graft ruptured, warranting a salvage procedure employing a transphyseal technique at 19 months after primary reconstruction.
One case (1.4%) developed septic arthritis that was treated by early arthroscopic surgery, with the graft ultimately preserved. Also, 6 patients (8.1%) had meniscal lesions (4 new lesions and 2 failures of repaired tears) that were repaired. Of these 6 cases, 5 (83.3%) healed, except for the occurrence of a new bucket-handle tear in the medial meniscus, with a good clinical outcome at 7 years of follow-up.
Further, there were 7 cases (9.5%) with a screw-related incident. Comparing this group of patients to the group without screw-related incidents, there were no differences in the analyzed quantitative or categorical variables (Figure 10). This should be interpreted with caution because of the small sample size of the group with screw-related incidents.

An 11-year-old boy presenting with tibial screw breakage.
On the other hand, 9 second-look procedures (12.2%) were performed, revealing narrowing of the notch in 1 case of a graft rupture. In the other 8 arthroscopic procedures (1 of the 3 graft failures, 1 septic arthritis, and 6 meniscal lesions), no signs of hypertrophy or a narrow notch were observed. No differences were found in complications regarding patient sex.
Discussion
In the current study, ACL reconstruction yielded excellent functional outcomes, with a mean final Lysholm score of 94.5 and a mean final Tegner score comparable with that before the injury. Knee stability was achieved, with only 4 cases of comparative laxity ≥6 mm (including the 3 failures), 3 cases of abnormal laxity (all failures), and 6 cases of suboptimal laxity (with good outcomes). Importantly, there were no relevant growth-related complications.
Studies on such patients have indicated a higher risk of developing meniscal and chondral lesions without ACL reconstruction. This risk increases with unstable episodes and delayed surgery, resulting in a 4-fold increase in the risk of meniscal lesions and a 3-fold increase in their severity when surgery is delayed by 12 weeks. ‡‡
In our series, 27.0% of arthroscopic procedures revealed meniscal lesions, 70.0% of which were in the lateral meniscus, yielding an odds ratio of 2.3 for lateral meniscal lesions. Comparing with previous studies is complex because of heterogeneity, but it contrasts with an approximately 70% incidence and an odds ratio of 1.5 reported in previous studies.7,21 The younger age of our cohort might have influenced these findings. Of these lesions, 80.0% were repaired, with an 87.5% healing rate and a 5.4% incidence of new injuries during the follow-up period (4 cases), which were effectively repaired in 3 cases. These results parallel those of isolated pediatric meniscal repair in stable knees, emphasizing the value of concurrent meniscal repair with knee stabilization.1,8,10,46,51
Graft survival is a critical concern, particularly in pediatric patients in whom rates of graft reruptures exceed those seen in adults.12,20,27,29,65,79 Dekker et al 20 observed a 19% rerupture rate among 85 pediatric athletes, with early return to sports identified as a significant predictor. Similarly, a large multicenter prospective study 29 found a 9% rerupture rate in patients with still-open physes over the first 2 postoperative years compared with 2.8% in adults. Paradoxically, the maturation time of a semitendinosus-gracilis tendon graft appears to be longer in children than in adults. 68 These findings suggest delaying high-risk athletic activities for at least 1 year. In our series, the mean time to return to preinjury sports was 8 months (range, 6-11 months), with no apparent effect on outcomes.
Studies on transphyseal techniques using a 4-strand hamstring tendon autograft have indicated that it elongates and thins with growth.11,13 The small size of the graft has been cited as a key factor for reruptures, with a graft width threshold of 8 mm suggested as a risk factor.53,56 However, recent comparative research involving 992 patients, with a mean age of 17.7 years, has contradicted this idea, as patients with a graft width <8 mm did not show a higher rerupture rate. 64
In our series, the graft survival rate was notably 95.9%. The small mean diameter of the graft (7.3 mm) did not seem to significantly affect the final outcomes. Additionally, if graft thinning is proportional to elongation caused by the growth of the intermediate physis, this risk is theoretically minimized with the intra-epiphyseal technique because there is no physis between the 2 graft ends.
Transphyseal and over-the-top (OTT) ACL reconstruction techniques are commonly used in the pediatric population. To mitigate the risk of growth disturbance, the tunnels should be narrow and be positioned as vertically and centrally as possible in relation to the physis. §§ This verticalization can be accentuated by the centrifugal migration of metaphyseal fixation with growth, potentially affecting the graft’s isometry and thereby increasing the risk of ruptures. Epiphyseal techniques may maintain better intra-articular anatomy, 17 potentially improving isometry and rotational control. In a meta-analysis by Frosch et al, 27 a lower rupture rate was observed with physeal sparing techniques compared with transphyseal techniques (1.4% vs 4.2%, respectively), although this finding lacked confirmation in subsequent studies.67,69 Objective intraoperative evaluations of graft isometry in this population are lacking in published literature. In our series, isometry showed a mean graft excursion of 1.1 mm, indicating good intraoperative isometry, with 3 cases with ≥3 mm progressing well.
One anatomic risk factor for graft failure, well documented in adults, 82 is the presence of a narrow notch, which in turn is associated with a smaller ACL size. 14 In their comparative study in children, Freychet et al 26 demonstrated that pediatric ACL ruptures are associated with a decreased notch width index, while Kocher et al 44 observed that the notch width index in the pediatric population was less in knees with ACL tears than in knees with tibial eminence avulsions.
The utility of notchplasty in adults is debated, 57 with concerns about the recurrence of notch narrowing. 4 Increased anterior tibial translation and a negative biomechanical effect due to an altered femoral insertion point have been credited for this.39,55 Our systematic use of notchplasty may be justified by increased notch narrowness associated with an ACL rupture in the pediatric population, given that is often quite challenging to determine intraoperatively whether the notch is narrow. We did not observe signs of hypertrophy or a narrow notch during the 8 second-look procedures in which the graft was in place, suggesting that, in these cases, there was no recurrence or hypertrophy of the notch. In contrast, narrowing of the notch was found during arthroscopic surgery for a failed graft.
Our surgical technique, based on Anderson’s 6 method, incorporates a different fixation approach using an intra-epiphyseal RIS. Some of its theoretical advantages include rigid fixation 59 and a reduction of certain risks associated with suspensory techniques: graft elongation with potential ruptures and a trampoline effect resulting from excessive pressure on the bone and physis surrounding the tunnel because of the relatively unloaded area overlying it. 48 While studies in adults have tended to favor suspensory fixation for graft incorporation and ligamentization and to minimize the risk of tunnel widening, 19 Lubowitz et al’s 50 prospective randomized study found no significant clinical or radiographic differences between fixation methods for all-inside ACL reconstruction using an allograft.
One weakness of the technique described here is the limited “safe space” available for tunneling (Figures 4 and 5) in which the risk of physeal involvement by proximity is added to the theoretical fragilization of the roof of the tibial epiphysis being increased by pressure from the interference screw. Indeed, one of our patients experienced a cartilaginous injury of the femoral physis, without clinical consequences.
RIS fixation is not without issues. In the group of 7 cases with fixation-related problems, we found slight but significant increased side-to-side clinical laxity, without complications, at follow-up. An alternative to consider is to use a PEEK (polyether ether ketone) screw in which its elastic modulus could decrease the risk of breakage. 25
A physeal injury is the most feared outcome in children undergoing ACL reconstruction. Tunneling in the vicinity of the physis18,27 carries risks in an area with high growth potential. Chotel et al 15 classified growth anomalies into 3 types: type A, indicating arrested growth within the physeal bridge; type B, indicating overgrowth secondary to physeal hyperstimulation; and type C, indicating decelerated growth secondary to a tenodesis effect of an overstressed graft.17,23 Type A is more closely associated with the transphyseal and OTT techniques than with epiphyseal techniques in which, although physeal involvement by proximity is theoretically possible, 48 less angular deformity has been observed in experimental models. 17
Physeal alterations may result with transphyseal techniques from direct damage to the physis through the tunnel. The threshold for problematic involvement appears to be in the range of 7% to 9% of the physeal surface, typically below a diameter of 9 mm in practice. This diameter increases as the growth plate is traversed more obliquely. These alterations can also result from the interposition of the material or bone in the physis, or perichondral damage at the OTT level, leading to lower limb length discrepancy and/or angular deformity. These risks can be minimized by making narrow tunnels as vertical as possible and using tendon filling as well as avoiding overtensioning of the graft. ∥∥
Systematic reviews have revealed no clear correlation between the risk of axial deviation and limb length discrepancy with transphyseal techniques,18,27,69 but this should be applied with caution. Yoo et al, 81 in their MRI study, revealed focal physeal disruption in 11.6% of cases, but no case exhibited clinical consequences. Small bone bridges have been observed at the edges of transphyseal tunnels, even when filled with a tendon graft. 71 Although the risk of growth disturbance is greater in patients with more residual growth potential, these bridges fracture easily when the growth potential is strong; thus, the risk of epiphysiodesis is, paradoxically, more important in adolescents in whom residual growth should have little capacity to break them. 16
On the other hand, type B overgrowth can be associated with epiphyseal techniques via stimulation of the physeal plate as well as with the transphyseal and OTT or “over-the-front” techniques, the latter by vicariant stimulation of the periosteum adjacent to the physis, thereby potentially triggering asymmetrical growth, analogous to posttraumatic tibial valgus (Cozen phenomenon).15,43,79,83
In our series, no axial deviation was observed. A mean overgrowth in the repaired limb of 6.5 mm (range, −2 to 18 mm) was noted, with 12.2% of the cases exhibiting >10 mm of overgrowth. We hypothesize that the presence of material in the epiphysis enhances metabolic activity, stimulating growth at the corresponding germinal layer of the physis. This effect is greater than if the graft is present alone, and is globally and symmetrically distributed, not limited to the graft side, causing such a discrepancy to both bones without deviation.
In comparison to the transphyseal and OTT techniques, the risk of a Cozen-like effect is minimal when the metaphysis remains untouched. Similar to Wall et al, 79 we avoided deperiostization when removing the graft from its tibial insertion, thereby minimizing, even more, this risk.
Limitations
Although our study is one of the largest prospective series of skeletally immature patients treated by a single surgeon, it is not without limitations. While Lysholm and Tegner scores are commonly used in studies on pediatric sports injuries, we recognize their lack of validation in this age group. We did not consider the International Knee Documentation Committee subjective functional assessment because of the absence of a pediatric equivalent at the time of the study. The Hospital for Special Surgery Pediatric Functional Activity Brief Scale, 24 which is validated in pediatric patients and is likely the most adapted test today, was not available at the time.
Conclusion
ACL reconstruction in children improves knee function, allows physical activity, and reduces the risk of intra-articular injuries during episodes of instability. Our technique yielded good results, including a low incidence of reruptures, which might be attributed to factors such as good anatomic positioning, isometry monitoring, rigid fixation, and consistent minimal notchplasty. Importantly, this procedure avoided direct physeal damage, preventing axis alterations. Overall, we consider this ACL reconstruction technique to be effective and safe, recommending its use for patients with an open physis and unstable knee after an ACL rupture.
Footnotes
Acknowledgements
The authors thank Jérôme Sales de Gauzy for his outstanding professionalism and for always inspiring them to think rationally, free from noise and biases, and helping them become better scientists and people. They give gratitude to Pedro Doménech for his valuable and unwavering support, sharing his vast knowledge, particularly in statistical matters. They are also grateful to Mikel Sánchez, a leader in the field, for his guidance and insights into many aspects of this work and for which he has contributed so much to the international scientific community. They also thank Francisco Soldado, a brilliant thinker and unique surgeon, for always providing a wealth of innovative ideas and to Carlos Barrios for his invaluable help in key aspects of the structure and development of this article.
Final revision submitted August 15, 2024; accepted September 17, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from ComitéÉtico de Investigación con medicamentos de HM Hospitales (HM05-13).